
Fluorescence Image-Guided Surgery for Thyroid Cancer: Utility for Preventing Hypoparathyroidism

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
1.1. Contrast-Enhanced Fluorescence and Autofluorescence
1.2. Postoperative Hypoparathyroidism
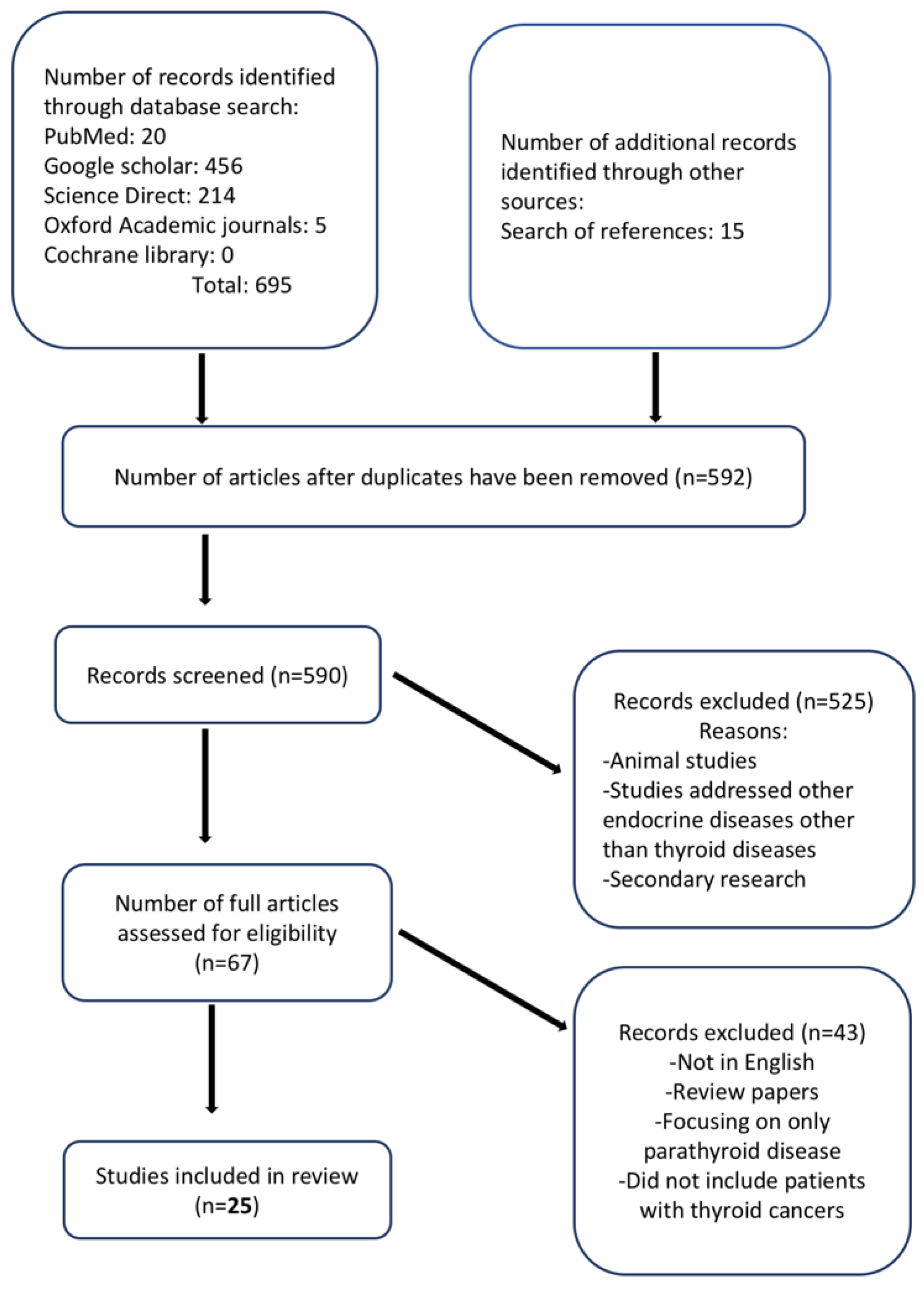
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Methodological Quality Assessment
3. Results
3.1. Data Extraction
3.2. Methodological Quality of Included Studies
3.3. Type of Fluorescence (Exogenous or Autofluorescence)
3.4. Parathyroid Gland Visualization and Preservation
3.5. Postoperative Serum Parathyroid Hormone
3.6. Effects on the Autotransplantation Rate
3.7. Postoperative Serum Calcium
3.8. Additional Duration of Surgery
3.9. Complications Related to Technique
3.10. Cost
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pellegriti, G.; Frasca, F.; Regalbuto, C.; Squatrito, S.; Vigneri, R. Worldwide increasing incidence of thyroid cancer: Update on epidemiology and risk factors. J. Cancer Epidemiol. 2013, 2013, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, L.; Wang, Y.; Sun, X.; Li, H.; Geng, X.; Ge, M.; Zhu, Y. Thyroid cancer: Trends in incidence, mortality and clinical-pathological patterns in Zhejiang Province, Southeast China. BMC Cancer 2018, 18, 291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deng, Y.; Li, H.; Wang, M.; Li, N.; Tian, T.; Wu, Y.; Xu, P.; Yang, S.; Zhai, Z.; Zhou, L.; et al. Global burden of thyroid cancer from 1990 to 2017. JAMA Netw. Open 2020, 3, e208759. [Google Scholar] [CrossRef]
- Links, T.P.; van Tol, K.M.; Jager, P.L.; Plukker, J.T.M.; Piers, D.A.; Boezen, H.M.; Dullaart, R.P.F.; de Vries, E.G.E.; Sluiter, W.J. Life expectancy in differentiated thyroid cancer: A novel approach to survival analysis. Endocr. Relat. Cancer 2005, 12, 273–280. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.S.; Nam, K.-H.; Chung, W.Y.; Chang, H.-S.; Park, C.S. Postoperative complications of thyroid cancer in a single center experience. J. Korean Med. Sci. 2010, 25, 541–545. [Google Scholar] [CrossRef] [Green Version]
- Medas, F.; Canu, G.L.; Erdas, E.; Giorgio, P. Intraoperative neuromonitoring in thyroid surgery. In Knowledges on Thyroid Cancer; Canu, G.L., Ed.; IntechOpen: Rijeka, Croatia, 2019; Chapter 6; ISBN 978-1-78923-984-3. [Google Scholar]
- Bai, B.; Chen, W. Protective effects of intraoperative nerve monitoring (IONM) for recurrent laryngeal nerve injury in thyroidectomy: Meta-analysis. Sci. Rep. 2018, 8, 7761. [Google Scholar] [CrossRef] [PubMed]
- Alander, J.T.; Kaartinen, I.; Laakso, A.; Pätilä, T.; Spillmann, T.; Tuchin, V.V.; Venermo, M.; Välisuo, P. A Review of indocyanine green fluorescent imaging in surgery. Int. J. Biomed. Imaging 2012, 2012, 940585. [Google Scholar] [CrossRef] [PubMed]
- Seeliger, B.; Alesina, P.F.; Walz, M.K.; Pop, R.; Charles, A.-L.; Geny, B.; Messaddeq, N.; Kontogeorgos, G.; Mascagni, P.; Seyller, E.; et al. Intraoperative imaging for remnant viability assessment in bilateral posterior retroperitoneoscopic partial adrenalectomy in an experimental model. Br. J. Surg. 2020, 107, 1780–1790. [Google Scholar] [CrossRef] [PubMed]
- Demarchi, M.S.; Karenovics, W.; Bédat, B.; Triponez, F. Intraoperative autofluorescence and indocyanine green angiography for the detection and preservation of parathyroid glands. JCM 2020, 9, 830. [Google Scholar] [CrossRef] [Green Version]
- De Boer, E.; Harlaar, N.J.; Taruttis, A.; Nagengast, W.B.; Rosenthal, E.L.; Ntziachristos, V.; Van Dam, G.M. Optical innovations in surgery. Br. J. Surg. 2015, 102, 56–72. [Google Scholar] [CrossRef]
- Mascagni, P.; Longo, F.; Barberio, M.; Seeliger, B.; Agnus, V.; Saccomandi, P.; Hostettler, A.; Marescaux, J.; Diana, M. New intraoperative imaging technologies: Innovating the surgeon’s eye toward surgical precision. J. Surg. Oncol. 2018, 118, 265–282. [Google Scholar] [CrossRef] [PubMed]
- Solórzano, C.C.; Thomas, G.; Baregamian, N.; Mahadevan-Jansen, A. Detecting the near infrared autofluorescence of the human parathyroid: Hype or opportunity? Ann. Surg. 2019. [Google Scholar] [CrossRef] [PubMed]
- Weissleder, R.; Pittet, M.J. Imaging in the era of molecular oncology. Nature 2008, 452, 580–589. [Google Scholar] [CrossRef] [Green Version]
- Seeliger, B.; Walz, M.K.; Alesina, P.F.; Agnus, V.; Pop, R.; Barberio, M.; Saadi, A.; Worreth, M.; Marescaux, J.; Diana, M. Fluorescence-enabled assessment of adrenal gland localization and perfusion in posterior retroperitoneoscopic adrenal surgery in a preclinical model. Surg. Endosc. 2020, 34, 1401–1411. [Google Scholar] [CrossRef] [PubMed]
- Sajedi, S.; Sabet, H.; Choi, H.S. Intraoperative biophotonic imaging systems for image-guided interventions. Nanophotonics 2018, 8, 99–116. [Google Scholar] [CrossRef] [PubMed]
- Van Manen, L.; Handgraaf, H.J.M.; Diana, M.; Dijkstra, J.; Ishizawa, T.; Vahrmeijer, A.L.; Mieog, J.S.D. A practical guide for the use of indocyanine green and methylene blue in fluorescence-guided abdominal surgery. J. Surg. Oncol. 2018, 118, 283–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kahramangil, B.; Kose, E.; Berber, E. Characterization of fluorescence patterns exhibited by different adrenal tumors: Determining the indications for indocyanine green use in adrenalectomy. Surgery 2018, 164, 972–977. [Google Scholar] [CrossRef] [PubMed]
- Fanaropoulou, N.M.; Chorti, A.; Markakis, M.; Papaioannou, M.; Michalopoulos, A.; Papavramidis, T. The use of indocyanine green in endocrine surgery of the neck: A systematic review. Medicine 2019, 98, e14765. [Google Scholar] [CrossRef] [PubMed]
- Solórzano, C.C.; Thomas, G.; Berber, E.; Wang, T.S.; Randolph, G.W.; Duh, Q.-Y.; Triponez, F. Current state of intraoperative use of near infrared fluorescence for parathyroid identification and preservation. Surgery 2021, 169, 868–878. [Google Scholar] [CrossRef] [PubMed]
- Barth, C.W.; Gibbs, S. Fluorescence image-guided surgery: A perspective on contrast agent development. In Molecular-Guided Surgery: Molecules, Devices, and Applications VI; SPIE: Bellingham, WA, USA, 2020. [Google Scholar]
- Orosco, R.K.; Tsien, R.Y.; Nguyen, Q.T. Fluorescence imaging in surgery. IEEE Rev. Biomed. Eng. 2013, 6, 178–187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van den Bos, J.; Al-Taher, M.; Schols, R.M.; van Kuijk, S.; Bouvy, N.D.; Stassen, L.P.S. Near-infrared fluorescence imaging for real-time intraoperative guidance in anastomotic colorectal surgery: A systematic review of literature. J. Laparoendosc. Adv. Surg. Tech. 2018, 28, 157–167. [Google Scholar] [CrossRef] [PubMed]
- Vutskits, L.; Briner, A.; Klauser, P.; Gascon, E.; Dayer, A.G.; Kiss, J.Z.; Muller, D.; Licker, M.J.; Morel, D.R. Adverse effects of methylene blue on the central nervous system. Anesthesiology 2008, 108, 684–692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Croce, A.C.; Bottiroli, G. Autofluorescence spectroscopy and imaging: A tool for biomedical research and diagnosis. Eur. J. Histochem. EJH 2014, 58, 2461. [Google Scholar] [CrossRef] [Green Version]
- Das, K.; Stone, N.; Kendall, C.; Fowler, C.; Christie-Brown, J. Raman spectroscopy of parathyroid tissue pathology. Lasers Med. Sci. 2006, 21, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Paras, C.; Keller, M.; White, L.; Phay, J.; Mahadevan-Jansen, A. Near-infrared autofluorescence for the detection of parathyroid glands. J. Biomed. Opt. 2011, 16, 067012. [Google Scholar] [CrossRef]
- McWade, M.A.; Paras, C.; White, L.M.; Phay, J.E.; Solórzano, C.C.; Broome, J.T.; Mahadevan-Jansen, A. Label-free intraoperative parathyroid localization with near-infrared autofluorescence imaging. J. Clin. Endocrinol. Metab. 2014, 99, 4574–4580. [Google Scholar] [CrossRef] [PubMed]
- Di Marco, A.N.; Palazzo, F.F. Near-infrared autofluorescence in thyroid and parathyroid surgery. Gland Surg. 2020, 9, S136–S146. [Google Scholar] [CrossRef]
- DSouza, A.V.; Lin, H.; Henderson, E.R.; Samkoe, K.S.; Pogue, B.W. Review of fluorescence guided surgery systems: Identification of key performance capabilities beyond indocyanine green imaging. J. Biomed. Opt. 2016, 21, 080901. [Google Scholar] [CrossRef] [PubMed]
- Chahardahmasumi, E.; Salehidoost, R.; Amini, M.; Aminorroaya, A.; Rezvanian, H.; Kachooei, A.; Iraj, B.; Nazem, M.; Kolahdoozan, M. Assessment of the early and late complication after thyroidectomy. Adv. Biomed. Res. 2019, 8, 14. [Google Scholar] [CrossRef] [PubMed]
- Tuttle, M.R. Differentiated Thyroid Cancer: Overview of Management. 2021. Available online: https://www.uptodate.com/contents/differentiated-thyroid-cancer-overview-of-management (accessed on 4 January 2021).
- Van Beek, D.-J.; Almquist, M.; Bergenfelz, A.O.; Musholt, T.J.; Nordenström, E. Complications after medullary thyroid carcinoma surgery: Multicentre study of the SQRTPA and EUROCRINE® databases. Br. J. Surg. 2020. [Google Scholar] [CrossRef]
- Edafe, O.; Antakia, R.; Laskar, N.; Uttley, L.; Balasubramanian, S.P. Systematic review and meta-analysis of predictors of post-thyroidectomy hypocalcaemia. Br. J. Surg. 2014, 101, 307–320. [Google Scholar] [CrossRef] [PubMed]
- McMullen, C.; Rocke, D.; Freeman, J. Complications of bilateral neck dissection in thyroid cancer from a single high-volume center. JAMA Otolaryngol. Head Neck Surg. 2017, 143, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Ritter, K.; Elfenbein, D.; Schneider, D.F.; Chen, H.; Sippel, R.S. Hypoparathyroidism after total thyroidectomy: Incidence and resolution. J. Surg. Res. 2015, 197, 348–353. [Google Scholar] [CrossRef] [Green Version]
- Khan, A.A.; Clarke, B.; Rejnmark, L.; Brandi, M.L. Hypoparathyroidism in pregnancy: Review and evidence-based recommendations for management. Eur. J. Endocrinol. 2019, 180, R37–R44. [Google Scholar] [CrossRef] [Green Version]
- Hicks, G.; George, R.; Sywak, M. Short and long-term impact of parathyroid autotransplantation on parathyroid function after total thyroidectomy. Gland Surg. 2017, 6 (Suppl. 1), S75–S85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almquist, M.; Ivarsson, K.; Nordenström, E.; Bergenfelz, A. Mortality in patients with permanent hypoparathyroidism after total thyroidectomy. Br. J. Surg. 2018, 105, 1313–1318. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Kim, S.W.; Song, S.H.; Lee, H.S.; Noh, W.J.; Oak, C.; Ahn, Y.C.; Lee, K.D. Intraoperative real-time localization of normal parathyroid glands with autofluorescence imaging. J. Clin. Endocrinol. Metab. 2016, 101, 4646–4652. [Google Scholar] [CrossRef] [Green Version]
- McWade, M.A.; Thomas, G.; Nguyen, J.Q.; Sanders, M.E.; Solórzano, C.C.; Mahadevan-Jansen, A. Enhancing parathyroid gland visualization using a near infrared fluorescence-based overlay imaging system. J. Am. Coll. Surg. 2019, 228, 730–743. [Google Scholar] [CrossRef]
- Jin, H.; Dong, Q.; He, Z.; Fan, J.; Liao, K.; Cui, M. Application of a fluorescence imaging system with indocyanine green to protect the parathyroid gland intraoperatively and to predict postoperative parathyroidism. Adv. Ther. 2018, 35, 2167–2175. [Google Scholar] [CrossRef] [PubMed]
- Benmiloud, F.; Godiris-Petit, G.; Gras, R.; Gillot, J.-C.; Turrin, N.; Penaranda, G.; Noullet, S.; Chéreau, N.; Gaudart, J.; Chiche, L.; et al. Association of autofluorescence-based detection of the parathyroid glands during total thyroidectomy with postoperative hypocalcemia risk: Results of the PARAFLUO multicenter randomized clinical trial. JAMA Surg. 2020, 155, 106. [Google Scholar] [CrossRef] [PubMed]
- Kose, E.; Rudin, A.V.; Kahramangil, B.; Moore, E.; Aydin, H.; Donmez, M.; Krishnamurthy, V.; Siperstein, A.; Berber, E. Autofluorescence imaging of parathyroid glands: An assessment of potential indications. Surgery 2020, 167, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Enny, L.; Ramakant, P.; Singh, K.R.; Rana, C.; Garg, S.; Mishra, A.K. Efficacy of fluorescein green dye in assessing intra-operative parathyroid gland vascularity and predicting post-thyroidectomy hypocalcaemia—A novel prospective cohort study. Indian J. Endocrinol. Metab. 2020, 24, 446. [Google Scholar] [PubMed]
- Razavi, A.C.; Ibraheem, K.; Haddad, A.; Saparova, L.; Shalaby, H.; Abdelgawad, M.; Kandil, E. Efficacy of indocyanine green fluorescence in predicting parathyroid vascularization during thyroid surgery. Head Neck 2019, 41, 3276–3281. [Google Scholar] [CrossRef] [PubMed]
- Rudin, A.V.; McKenzie, T.J.; Thompson, G.B.; Farley, D.R.; Lyden, M.L. Evaluation of parathyroid glands with indocyanine green fluorescence angiography after thyroidectomy. World J. Surg. 2019, 43, 1538–1543. [Google Scholar] [CrossRef]
- Van den Bos, J.; van Kooten, L.; Engelen, S.M.E.; Lubbers, T.; Stassen, L.P.S.; Bouvy, N.D. Feasibility of indocyanine green fluorescence imaging for intraoperative identification of parathyroid glands during thyroid surgery. Head Neck 2019, 41, 340–348. [Google Scholar] [CrossRef] [PubMed]
- Falco, J.; Dip, F.; Quadri, P.; de la Fuente, M.; Prunello, M.; Rosenthal, R.J. Increased identification of parathyroid glands using near infrared light during thyroid and parathyroid surgery. Surg. Endosc. 2017, 31, 3737–3742. [Google Scholar] [CrossRef] [PubMed]
- Lang, B.H.-H.; Wong, C.K.H.; Hung, H.T.; Wong, K.P.; Mak, K.L.; Au, K.B. Indocyanine green fluorescence angiography for quantitative evaluation of in situ parathyroid gland perfusion and function after total thyroidectomy. Surgery 2017, 161, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Serra, C.; Canudo, A.; Silveira, L. Intraoperative identification of parathyroid glands by autofluorescence on total thyroidectomy—Does it really reduces post-operative hypocalcemia? Surg. Pract. Sci. 2020, 2, 100011. [Google Scholar] [CrossRef]
- Lerchenberger, M.; Al Arabi, N.; Gallwas, J.K.S.; Stepp, H.; Hallfeldt, K.K.J.; Ladurner, R. Intraoperative near-infrared autofluorescence and indocyanine green imaging to identify parathyroid glands: A comparison. Int. J. Endocrinol. 2019, 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Leeuw, F.; Breuskin, I.; Abbaci, M.; Casiraghi, O.; Mirghani, H.; Lakhdar, A.B.; Laplace-Builhé, C.; Hartl, D. Intraoperative near-infrared imaging for parathyroid gland identification by auto-fluorescence: A feasibility study. World J. Surg. 2016, 40, 2131–2138. [Google Scholar] [CrossRef] [PubMed]
- Llorente, P.M.; Martínez, J.M.F.; Barrasa, A.G. Intraoperative parathyroid hormone measurement vs indocyanine green angiography of parathyroid glands in prediction of early postthyroidectomy hypocalcemia. JAMA Surg. 2020, 155, 84–85. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.W.; Lee, H.S.; Ahn, Y.C.; Park, C.W.; Jeon, S.W.; Kim, C.H.; Ko, J.B.; Oak, C.; Kim, Y.; Lee, K.D. Near-infrared autofluorescence image-guided parathyroid gland mapping in thyroidectomy. J. Am. Coll. Surg. 2018, 226, 165–172. [Google Scholar] [CrossRef]
- Ladurner, R.; Al Arabi, N.; Guendogar, U.; Hallfeldt, K.; Stepp, H.; Gallwas, J. Near-infrared autofluorescence imaging to detect parathyroid glands in thyroid surgery. Ann. R. Coll. Surg. Engl. 2018, 100, 33–36. [Google Scholar] [CrossRef]
- Ladurner, R.; Lerchenberger, M.; Al Arabi, N.; Gallwas, J.K.S.; Stepp, H.; Hallfeldt, K.K.J. Parathyroid autofluorescence—How does it affect parathyroid and thyroid surgery? A 5 year experience. Molecules 2019, 24, 2560. [Google Scholar] [CrossRef] [Green Version]
- Vidal Fortuny, J.; Belfontali, V.; Sadowski, S.M.; Karenovics, W.; Guigard, S.; Triponez, F. Parathyroid gland angiography with indocyanine green fluorescence to predict parathyroid function after thyroid surgery. Br. J. Surg. 2016, 103, 537–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vidal Fortuny, J.; Sadowski, S.M.; Belfontali, V.; Guigard, S.; Poncet, A.; Ris, F.; Karenovics, W.; Triponez, F. Randomized clinical trial of intraoperative parathyroid gland angiography with indocyanine green fluorescence predicting parathyroid function after thyroid surgery. Br. J. Surg. 2018, 105, 350–357. [Google Scholar] [CrossRef] [Green Version]
- Dip, F.; Falco, J.; Verna, S.; Prunello, M.; Loccisano, M.; Quadri, P.; White, K.; Rosenthal, R. Randomized controlled trial comparing white light with near-infrared autofluorescence for parathyroid gland identification during total thyroidectomy. J. Am. Coll. Surg. 2019, 228, 744–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaidi, N.; Bucak, E.; Yazici, P.; Soundararajan, S.; Okoh, A.; Yigitbas, H.; Dural, C.; Berber, E. The feasibility of indocyanine green fluorescence imaging for identifying and assessing the perfusion of parathyroid glands during total thyroidectomy. J. Surg. Oncol. 2016, 113, 775–778. [Google Scholar] [CrossRef]
- Kim, Y.S.; Erten, O.; Kahramangil, B.; Aydin, H.; Donmez, M.; Berber, E. The impact of near infrared fluorescence imaging on parathyroid function after total thyroidectomy. J. Surg. Oncol. 2020. [Google Scholar] [CrossRef]
- Jin, H.; Cui, M. Research on intra-operative indocyanine green angiography of the parathyroid for predicting postoperative hypoparathyroidism: A noninferior randomized controlled trial. Endocr. Pract. 2020, 26, 1469–1476. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Kim, S.W.; Kang, P.; Choi, J.; Lee, H.S.; Park, S.Y.; Kim, Y.; Ahn, Y.-C.; Lee, K.D. Near-infrared autofluorescence imaging may reduce temporary hypoparathyroidism in patients undergoing total thyroidectomy and central neck dissection. Thyroid 2021. [Google Scholar] [CrossRef] [PubMed]
- Kose, E.; Kahramangil, B.; Aydin, H.; Donmez, M.; Berber, E. Heterogeneous and low-intensity parathyroid autofluorescence: Patterns suggesting hyperfunction at parathyroid exploration. Surgery 2019, 165, 431–437. [Google Scholar] [CrossRef] [PubMed]
- DiMarco, A.; Chotalia, R.; Bloxham, R.; McIntyre, C.; Tolley, N.; Palazzo, F.F. Does fluoroscopy prevent inadvertent parathyroidectomy in thyroid surgery? Ann. R. Coll. Surg. Engl. 2019, 101, 508–513. [Google Scholar] [CrossRef] [PubMed]
- Bellier, A.; Wazne, Y.; Chollier, T.; Sturm, N.; Chaffanjon, P. Spare parathyroid glands during thyroid surgery with perioperative autofluorescence imaging: A diagnostic study. World J. Surg. 2021. [Google Scholar] [CrossRef] [PubMed]
- Benmiloud, F.; Rebaudet, S.; Varoquaux, A.; Penaranda, G.; Bannier, M.; Denizot, A. Impact of autofluorescence-based identification of parathyroids during total thyroidectomy on postoperative hypocalcemia: A before and after controlled study. Surgery 2018, 163, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.W.; Lee, H.S.; Lee, K.D. Intraoperative real-time localization of parathyroid gland with near infrared fluorescence imaging. Gland Surg. 2017, 6, 516–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudin, A.V.; Berber, E. Impact of fluorescence and autofluorescence on surgical strategy in benign and malignant neck endocrine diseases. Best Pract. Res. Clin. Endocrinol. Metab. 2019, 33, 101311. [Google Scholar] [CrossRef] [PubMed]
- Jin, H.; Dong, Q.; He, Z.; Fan, J.; Liao, K.; Cui, M. Research on indocyanine green angiography for predicting postoperative hypoparathyroidism. Clin. Endocrinol. 2019, 90, 487–493. [Google Scholar] [CrossRef]
- Lütken, C.D.; Achiam, M.P.; Osterkamp, J.; Svendsen, M.B.; Nerup, N. Quantification of fluorescence angiography: Toward a reliable intraoperative assessment of tissue perfusion—A narrative review. Langenbecks Arch. Surg. 2021, 406, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Meira, J.; Marques, M.L.; Falcão-Reis, F.; Rebelo Gomes, E.; Carneiro, Â. Immediate reactions to fluorescein and indocyanine green in retinal angiography: Review of literature and proposal for patient’s evaluation. Clin. Ophthalmol. 2020, 14, 171–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorente-Poch, L.; Sancho, J.J.; Ruiz, S.; Sitges-Serra, A. Importance of In Situ preservation of parathyroid glands during total thyroidectomy. Br. J. Surg. 2015, 102. [Google Scholar] [CrossRef]
- Baiocchi, G.L.; Diana, M.; Boni, L. Indocyanine green-based fluorescence imaging in visceral and hepatobiliary and pancreatic surgery: State of the art and future directions. World J. Gastroenterol. 2018, 24, 2921–2930. [Google Scholar] [CrossRef] [PubMed]
- Badii, B.; Staderini, F.; Foppa, C.; Tofani, L.; Skalamera, I.; Fiorenza, G.; Qirici, E.; Cianchi, F.; Perigli, G. Cost-benefit analysis of the intraoperative parathyroid hormone assay in primary hyperparathyroidism: Cost-benefit analysis of intraoperative PTH assay. Head Neck 2017, 39, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Thomas, G.; McWade, M.A.; Paras, C.; Mannoh, E.A.; Sanders, M.E.; White, L.M.; Broome, J.T.; Phay, J.E.; Baregamian, N.; Solórzano, C.C.; et al. Developing a clinical prototype to guide surgeons for intraoperative label-free identification of parathyroid glands in real time. Thyroid 2018, 28, 1517–1531. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| s/n | Study | Number of Patients | Age (Years) * | Study Design | Indication for Surgery | Type of Surgery |
|---|---|---|---|---|---|---|
| 1 | (Jin et al., 2018) [44] | 26 | 49.6 ± 14.7 | Prospective cohort study | Thyroid cancer (23%) Benign thyroid disease (77%) | Open total thyroidectomy |
| 2 | (Benmiloud et al., 2020) [45] | 241 | 53.6 ± 13.6 | Prospective multicenter RCT | Thyroid cancer 56 (23.2%) Benign thyroid disease 185 (76.8%) | Open total thyroidectomy |
| 3 | (Kose et al., 2020) [46] | 310 patients; 173 underwent thyroid surgery | 55.6 ± 15.2 | Prospective clinical study | Thyroid cancer 39 (13%) Benign thyroid nodule/multinodular goiter 115 (37%) Hyperthyroidism 19 (6%) Hyperparathyroidism 137 (44%) | Open total thyroidectomy 139 (45%) Thyroid lobectomy 34 (11%) Parathyroidectomy 137 (44%) |
| 4 | (Enny et al., 2020) [47] | 72 | 39.2 ± 11.9 | Prospective cohort study | Thyroid cancer 14 (18%) Benign thyroid disease 58 (69%) | Open total thyroidectomy |
| 5 | (Razavi et al., 2019) [48] | 111 43—ICG 68—conventional | ICG: 50.51 ± 1.98 Conventional: 51.56 ± 1.46 | Retrospective case–control study | ICG: Thyroid cancer (36.8%) Benign conditions (45.1%) Conventional: Thyroid cancer (34.9%) Benign conditions (44.6%) | Laparoscopic total or completion thyroidectomy |
| 6 | (McWade et al., 2019) [43] | 30 | Range: 32–70 | Prospective clinical study | Thyroid diseases including cancer 12 (40%) Parathyroid diseases 15 (50%) Both 3 (10%) | Open thyroidectomy and parathyroidectomy |
| 7 | (Rudin et al., 2019) [49] | 210 86—ICG 124—conventional | ICG: 47 Control: 49 | Retrospective case–control study | ICG: Thyroid cancer (56%) Benign conditions (44%) Control: Thyroid cancer (65%) Benign conditions (35%) | Open total/near-total thyroidectomy |
| 8 | (van den Bos et al., 2019) [50] | 30 surgeries in 26 patients | 56.3 ± 16 | Prospective clinical study | Suspected thyroid cancer 17 (56.7%) Proven thyroid cancer 7 (23.3%) Benign thyroid disease 6 (20.0%) | Open total thyroidectomy, completion thyroidectomy, and hemithyroidectomy |
| 9 | (Falco et al., 2017) [51] | 74 | 48.4 ± 13.5 | Retrospective clinical study | Thyroid cancer 35 (47%) Goiter 23 (31%) Primary hyperparathyroidism 13 (18%) Hyperthyroidism 3 (4%) | Not stated |
| 10 | (Lang et al., 2017) [52] | 94 | 54.5 ± 15.0 | Prospective clinical study | Thyroid cancer 12 (17.1%) Benign pathology 38 (54.3%) Graves’ disease/toxic goiter 15 (21.4%) Indeterminate cytology 5 (7.1%) | Open total thyroidectomy |
| 11 | (Serra et al., 2020) [53] | 105 45—study 65—control | Study group: 61.4 ± 15.5 Control: 61.6 ± 12.1 | Prospective case–control study | Study: Malignant 20 (33.3%) Benign 40 (66.7%) Control: Malignant 8 (17.8%) Benign 37 (82.2%) | Open total thyroidectomy |
| 12 | (Lerchenberger et al., 2019) [54] | 50 | 47.2 | Prospective clinical study | Thyroid cancer 12 Benign thyroid disease 16 Parathyroidectomy 17 | Open total thyroidectomy, hemithyroidectomy, and parathyroidectomy |
| 13 | (De Leeuw et al., 2016) [55] | 35 | 40.9 | Prospective clinical study | Benign and malignant thyroid diseases | Open total thyroidectomy, hemithyroidectomy, and parathyroidectomy |
| 14 | (Llorente et al., 2020) [56] | 50 | 52 ± 12.9 | Prospective cohort study | Thyroid cancer (70%) Multinodular goiter (26%) Graves’ disease (4%) | Open total thyroidectomy |
| 15 | (S. W. Kim et al., 2016) [42] | 8 | Range: 34–73 | Prospective clinical study | Papillary thyroid cancer | Open total thyroidectomy and hemithyroidectomy |
| 16 | (S. W. Kim et al., 2018) [57] | 38 | Not stated | Prospective clinical study | Papillary thyroid cancer | Open total thyroidectomy (44.7%) Unilateral lobectomy (55.3%) |
| 17 | (R. Ladurner et al., 2018) [58] | 21 | Not stated | Prospective clinical study | Thyroid diseases including thyroid cancer | Open thyroidectomy |
| 18 | (Roland Ladurner et al., 2019) [59] | 117 | 49.9 Range: 19–81 | Prospective clinical study | Thyroid cancer (21.3%) Thyroid benign (42.7%) Parathyroid disease (35.9%) | Total thyroidectomy, partial thyroidectomy, and parathyroidectomy |
| 19 | (Vidal Fortuny et al., 2016) [60] | 36 | 49.8 ± 15.7 | Prospective clinical study | Thyroid cancer (22.2%) Benign thyroid diseases (77.8%) | Total thyroidectomy |
| 20 | (Vidal Fortuny et al., 2018) [61] | 196 | Not stated | Prospective RCT | Study group: Malignancy 30 (41%) Benign 40 (59%) Control: Malignancy 17 (23%) Benign 56 (77%) | Completion thyroidectomy and total thyroidectomy |
| 21 | (Dip et al., 2019) [62] | 170 | 47.3 ± 13.6 | Prospective RCT | Thyroid cancer (48.2%) Benign conditions (51.8%) | Total thyroidectomy |
| 22 | (Zaidi et al., 2016) [63] | 27 | 43.9 ± 1.0 | Prospective feasibility study | Thyroid cancer (37.0%) Multinodular (48.2%) Graves’ disease (14.8%) | Total thyroidectomy, completion thyroidectomy, and hemithyroidectomy |
| 23 | (Y. S. Kim et al., 2020) [64] | 300 100—study 200—control | Study: 51.6 ± 15.2 Control: 50.2 ± 15.5 | Retrospective case–control study | Thyroid cancer (55.3%) Benign thyroid disease (44.7%) | Total thyroidectomy |
| 24 | (Jin & Cui, 2020) [65] | 56 28—test group 28—control group | 42.68 ± 11.70 | Randomized control trial | Study group: Malignancy 9 (32.1%) Benign thyroid disease 19 (67.9%) Control: Malignancy 9 (32.1%) Benign thyroid disease 19 (67.9%) | Total thyroidectomy |
| 25 | (D. H. Kim et al., 2021) [66] | 542 261—NIRAF group 281—control group | NIRAF group: 51.30 ± 12.44 Control group: 52.83 ± 10.92 | Retrospective study with historical control | All thyroid cancer patients | Total thyroidectomy with unilateral or bilateral central neck dissection |
| Study | A | B | C | D | E | F | G | H | I | J | K | L | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (Jin et al., 2018) [44] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | X | X | X | X | 14/16 |
| (Benmiloud et al., 2020) [45] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 22/24 |
| (Kose et al., 2020) [46] | 2 | 2 | 2 | 2 | 2 | 0 | 0 | 0 | X | X | X | X | 10/16 |
| (Enny et al., 2020) [47] | 2 | 2 | 2 | 1 | 2 | 1 | 0 | 0 | X | X | X | X | 10/16 |
| (Razavi et al., 2019) [48] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 22/24 |
| (McWade et al., 2019) [43] | 2 | 2 | 2 | 2 | 2 | 0 | 0 | 0 | X | X | X | X | 10/16 |
| (Rudin et al., 2019) [49] | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 0 | 2 | 0 | 2 | 2 | 18/24 |
| (van den Bos et al., 2019) [50] | 2 | 2 | 2 | 2 | 2 | 1 | 0 | 0 | X | X | X | X | 11/16 |
| (Falco et al., 2017) [51] | 2 | 2 | 2 | 2 | 1 | 0 | 0 | 0 | X | X | X | X | 9/16 |
| (Lang et al., 2017) [52] | 2 | 2 | 2 | 2 | 2 | 0 | 0 | 0 | X | X | X | X | 10/16 |
| (Serra et al., 2020) [53] | 1 | 2 | 2 | 2 | 2 | 2 | 0 | 0 | 2 | 2 | 2 | 2 | 19/24 |
| (Lerchenberger et al., 2019) [54] | 2 | 2 | 2 | 1 | 1 | 0 | 0 | 0 | X | X | X | X | 8/16 |
| (De Leeuw et al., 2016) [55] | 2 | 2 | 2 | 2 | 0 | 0 | 0 | 0 | X | X | X | X | 8/16 |
| (Llorente et al., 2020) [56] | 2 | 2 | 2 | 2 | 0 | 2 | 0 | 0 | X | X | X | X | 10/16 |
| (S. W. Kim et al., 2016) [42] | 2 | 2 | 2 | 2 | 1 | 0 | 2 | 0 | X | X | X | X | 11/16 |
| (S. W. Kim et al., 2018) [57] | 2 | 2 | 2 | 2 | 1 | 0 | 2 | 0 | X | X | X | X | 11/16 |
| (R. Ladurner et al., 2018) [58] | 2 | 2 | 2 | 2 | 1 | 0 | 0 | 0 | X | X | X | X | 9/16 |
| (Roland Ladurner et al., 2019) [54] | 2 | 2 | 2 | 2 | 1 | 0 | 0 | 0 | X | X | X | X | 9/16 |
| (Vidal Fortuny et al., 2016) [60] | 2 | 2 | 2 | 2 | 2 | 0 | 0 | 0 | X | X | X | X | 10/16 |
| (Vidal Fortuny et al., 2018) [61] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 22/24 |
| (Dip et al., 2019) [62] | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 0 | 2 | 2 | 2 | 2 | 22/24 |
| (Zaidi et al., 2016) [63] | 2 | 2 | 2 | 2 | 1 | 0 | 2 | 0 | X | X | X | X | 11/16 |
| (Y. S. Kim et al., 2020) [64] | 2 | 2 | 1 | 2 | 1 | 2 | 0 | 0 | 2 | 1 | 2 | 2 | 17/24 |
| (Jin & Cui, 2020) [65] | 2 | 2 | 2 | 2 | 1 | 2 | 0 | 0 | 2 | 2 | 2 | 2 | 19/24 |
| (D. H. Kim et al., 2021) [66] | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 0 | 2 | 1 | 2 | 2 | 19/24 |
| Study | Autofluorescence or Exogenous Dye | Type of Exogenous Dye | Dose | Timing of Administration | Fluorescence System |
|---|---|---|---|---|---|
| (De Leeuw et al., 2016) [55] | AF | NA | NA | NA | Fluobeam 800 clinical system (Fluoptics, Grenoble, France) |
| (Serra et al., 2020) [53] | AF | NA | NA | NA | Custom NIRAF device (Thorlabs GmbH, Dachau, Deutschland and CCD Sony ICX254AL image detector) |
| (McWade et al., 2019) [43] | AF | NA | NA | NA | Overlay tissue imaging system (OTIS) |
| (Benmiloud et al., 2020) [45] | AF | NA | NA | NA | Fluobeam 800 system (Fluoptics) |
| (Kose et al., 2020) [46] | AF | NA | NA | NA | Fluobeam device (Fluoptics) |
| (S. W. Kim et al., 2016) [42] | AF | NA | NA | NA | Digital camera, NIR light-emitting diode (LED), and IR illuminating lights |
| (S. W. Kim et al., 2018) [57] | AF | NA | NA | NA | M780L3-C1, Thorlabs, Newton, NJ, USA and INFRALUX-300, Daekyung Electro Medical Co., Republic of Korea |
| (R. Ladurner et al., 2018) [58] | AF | NA | NA | NA | NIR/ICG endoscopic system (Karl Storz, Tuttlingen, Germany). |
| (Y. S. Kim et al., 2020) [64] | AF | NA | NA | NA | Fluobeam; Fluoptics, Grenoble, France |
| (D. H. Kim et al., 2021) [66] | AF | NA | NA | NA | Modified DSLR camera and LED (M780L3-C1, Thorlabs, New Jersey, USA) light source |
| (Dip et al., 2019) [62] | White light alone vs. AF + white light | NA | NA | NA | Fluobeam 800 system (Fluoptics) |
| (Lerchenberger et al., 2019) [54] | AF vs. exogenous | ICG | 5 mg | After lateral mobilization of the thyroid and exposure of the RLN | NIR/ICG endoscopic system (Karl Storz, Tuttlingen, Germany). |
| (Roland Ladurner et al., 2019) [59] | AF and exogenous | ICG-Pulsion | 5 mg | After lateral mobilization of the thyroid gland | Storz laparoscopic NIR/ICG imaging system |
| (Falco et al., 2017) [51] | Exogenous | ICG | 0.5 mL | After exposure of the thyroid gland | NIRL (near infrared light) using a laser system |
| (Lang et al., 2017) [52] | Exogenous | ICG | 2.5 mg | After resection of the thyroid gland | SPY fluorescent imaging system (Novadaq Technologies, Inc., Mississauga, ON, Canada) |
| (Jin et al., 2018) [44] | Exogenous | ICG | 5 mg | After adequate exposure of each central neck compartment | Intraoperative navigation system (Digi-MIH-001-I, Digital Precision Medicine Technology Co., Ltd., Beijing, China); fluorescence imaging system |
| (Llorente et al., 2020) [56] | Exogenous | ICG | Not stated | After thyroid resection | Not specified |
| (Enny et al., 2020) [47] | Exogenous | Fluorescein dye | 500 mg | After thyroid gland resection | LED blue light |
| (Razavi et al., 2019) [48] | Exogenous | ICG | 5 mg | At the end of surgery | Not specified |
| (Rudin et al., 2019) [49] | Exogenous | ICG | 6 mL (3 per side) | At the end of surgery | Laparoscopic PINPOINT camera (NOVADAQ, ON, Canada) |
| (van den Bos et al., 2019) [50] | Exogenous | ICG | 7.5 mg twice, i.e., 15 mg | Before and after resection of the thyroid gland | Laparoscopic fluorescence imaging system (Karl Storz GmbH & Co., Tuttlingen, Germany) |
| (Vidal Fortuny et al., 2016) [60] | Exogenous | ICG | 3 to 5 mL doses (75–150 mg) up to 5 mg/kg/day | After excision of the thyroid gland | Laparoscopic PINPOINT® camera (Novadaq, ON, Canada) |
| (Vidal Fortuny et al., 2018) [61] | Exogenous | ICG | 2.5 mg doses up to 5 mg/kg/day | After excision of the thyroid gland | NIR camera (Pinpoint®; Novadaq, Toronto, ON, Canada |
| (Zaidi et al., 2016) [63] | Exogenous | ICG | 5 mg | Before and after thyroid resection | Pinpoint video-assisted NIR system (Novadaq, Inc., Toronto, ON, Canada) |
| (Jin & Cui, 2020) [65] | Exogenous | ICG | 5 mg/kg | After resection of thyroid lobes | Digi-MIH-I-001, Digital Precision Medicine Technology Co., Ltd, Beijing, China |
| Study | PG Visualization and Preservation | Postoperative Serum PTH | Postoperative Serum Calcium |
|---|---|---|---|
| (Jin et al., 2018) [44] | Among 104 PGs, 86 were identified. | In the 22 patients with at least one PG with an ICG score of 2, postoperative PTH levels were normal. In four patients, ICG did not demonstrate a well-vascularized PG. Two of these patients developed transient hypoparathyroidism. | None of the patients developed hypocalcemia at the time of measurement. |
| (Benmiloud et al., 2020) [45] | The rate of patients with four identified PGs was higher in the NIRAF group (47.1% (95% CI, 38.5–56.4%)) than in the standard-care group (19.2% (95% CI, 12.1–26.2%); p < 0.001) | The PTH concentration at POD 1 was not significantly lower in the standard-care group (median (IQR), 28.6 (12.0–46.5) pg/mL) than in the NIRAF group (median (IQR), 33.2 (21.9–48.1) pg/mL). | The postoperative hypocalcemia rate was significantly lower in the NIRAF group (9.1% (95% CI, 4.0–14.2%)) than in the standard-care group (21.7% (95% CI, 14.3–29.0%); p = 0.007). |
| (Kose et al., 2020) [46] | For patients that underwent thyroidectomy, AF was demonstrated in 496 (98.6%) of the PGs; 33% had been first identified with NIRAF prior to visual recognition by the surgeon. In 5%, NIFI helped identify incidentally resected PGs. | Not measured | Not measured |
| (Enny et al., 2020) [47] | Two PGs in 30 (44.4%) patients, 0 PGs in 6 (6.9%) patients, and 4 PGs in 7 (9.7%) patients were visualized with fluorescein dye. With naked eye evaluation, 0 PGs in 1 patient, 2 PGs in 29 (41.7%) patients, and 4 PGs in 11 (15.3%) patients were visualized. | Not measured | Clinical hypocalcemia was observed in all patients in whom no PGs were visualized with fluorescein dye, whereas none of the patients in whom three or four PGs were visualized developed hypocalcemia. Among patients in whom three or four PGs were observed by the naked eye, 7 (28%) and 3 (23.7%) patients developed clinical hypocalcemia, respectively. |
| (Razavi et al., 2019) [48] | Not specified | Mean postoperative PTH decreased by 23.48 pg/mL for conventional care and 29.24 pg/mL for ICG. | Symptomatic hypocalcemia was observed in 3.90% of those who underwent conventional treatment and 7.90% of those in the ICG group. |
| (McWade et al., 2019) [43] | In total, 67 (97%) of exposed tissues of interest were correctly visualized as PGs. | Not measured | Not measured |
| (Rudin et al., 2019) [49] | Identification and autotransplantation were more common in the ICGA group at 36%, compared with 12% in the control group (p = 0.0001). | At POD 1, PTH was found to be low in 36% of controls and 37% of ICGA patients. An undetectable PTH level was present in 14% of control patients and 15% of ICGA patients. One patient in each group had permanent hypoparathyroidism. | Not measured |
| (van den Bos et al., 2019) [50] | In total, 41 PGs were visualized with white light in 25 patients, whereas 31 PGs were identified in 23 patients by NIRAF imaging. | Not measured | Three patients had transient hypocalcemia that resolved after 2 weeks. |
| (Falco et al., 2017) [51] | The mean number of identified PGs was 2.5 (±0.8) and 3.7 (±0.7) with WL (white light) and NIRAF respectively. In 86.5% (n = 64) of patients, four PGs were identified with NIFI, whereas four PGs were visualized with WL in only 12.2% (n = 9) of patients. | Not measured | Not stated |
| (Lang et al., 2017) [52] | A total of 340 PGs were identified, and 324 (95.3%) PGs were later confirmed to be PGs on histology. | Not measured | Nine (12.9%) patients developed transient hypocalcemia, while no patients had permanent hypocalcemia. There was a significant relationship between intensity of fluorescence image and the development of hypocalcemia. No patients with a greatest fluorescent light intensity developed postoperative hypocalcemia |
| (Serra et al., 2020) [53] | The mean number of PGs identified per patient was 3.47 in the study group and 2.33 in the control group (p < 0.0001). | Determinations of PTH 24 h after surgery showed a statistically significant difference favoring the study group. | In the study group, 24.4% presented 24-h postoperative hypocalcemia vs. 30% of the control group. At 6 months postoperation, three patients in the control group had permanent hypocalcemia, compared with no patients in the study group. |
| (Lerchenberger et al., 2019) [54] | A total of 64 (82%) PGs were visualized with AF; AF could not indicate whether the blood supply was still viable. On ICG administration, 63 PGs (81%) showed persistent fluorescence after a decrease in thyroid fluorescence. | Not measured | Only two patients developed transient hypocalcemia. No patients had permanent hypocalcemia |
| (De Leeuw et al., 2016) [55] | In total, 80 PGs were identified using the NIR system, and 81 glands were confirmed on frozen section to be PGs. | Not measured | Not measured |
| (Llorente et al., 2020) [56] | Not specified | Not measured | Eleven (22%) patients developed postoperative hypocalcemia. ICGA would allow immediate decision-making without the need to wait for intraoperative PTH measurements. |
| (S. W. Kim et al., 2016) [42] | All PGs were visualized. | No patient had postoperative hypoparathyroidism. | Not measured |
| (S. W. Kim et al., 2018) [57] | All but one PG were identified in vivo and preserved. The excised PG was autotransplanted | Not measured | Only one patient had transient hypocalcemia. |
| (R. Ladurner et al., 2018) [58] | Of the 41 PGs examined, 37 were identified by AF. AF assisted the preservation and autotransplantation of PGs in two patients | Not measured | Not measured |
| (Roland Ladurner et al., 2019) [59] | In total, 179 PGs (87.3%) displayed NIRAF showing a typical bluish violet color. | Not measured | Not measured |
| (Vidal Fortuny et al., 2016) [60] | Of the 36 patients who underwent ICGA, 30 had an ICG score of 2 for at least one PG. Autotransplantation was performed for those with poor ICG scores. | In the 30 patients with at least one PG with an ICG score of 2, postoperative PTH levels were in the normal range. | The postoperative adjusted calcium levels were within the normal range in 29 (80.6%) patients. |
| (Vidal Fortuny et al., 2018) [61] | In 146 patients, at least one preserved PG had an ICG score of 2. | Hypoparathyroidism was not observed in either group. | Hypocalcemia was not observed in either group. |
| (Dip et al., 2019) [62] | With NIRI, an average of 2.6 (0.85) PGs were detected prior to dissection. In four patients, PGs were transplanted after identification with NIRI. | Not measured | Significantly higher mean serum calcium levels were observed in the study group, with 8.2% having serum calcium <8 mg/dL compared with 16.5% in the control group. However, 1.2% in both groups required long-term calcium replacement, which was resolved by 6 months. |
| (Zaidi et al., 2016) [63] | A total of 71 (84%) PGs were identified on fluorescence. | The mean POD-1 PTH level of patients with at least two glands exhibiting <30% fluorescence at completion of thyroidectomy was 9 pg/dL, whereas those with fewer than two glands demonstrating <30% fluorescence had a POD-1 PTH of 19.5 pg/dL (p = 0.05). | Postoperatively, three patients (11%) had a serum calcium value <8 mg/dL, and one patient was symptomatic. |
| (Y. S. Kim et al., 2020) [64] | The mean number of PGs identified intraoperatively was similar between the two groups. The rate of incidental parathyroidectomy reported by pathology was higher in the conventional group (14%) than in the NIFI group (6%) (p = 0.039). | The POD-1 value was 23.9 pg/mL (17.6) in the NIRI group and 23.0 pg/mL (22.4) in the control group. The POD-14 level was 38.9 pg/mL (35.5) in the NIRI group and 35.8 pg/mL (26.1) in the control group. | At POD 1, the NIFI group had a level of 9.0 mg/dL (0.6) compared with 8.8 mg/dL (0.6) for the control group (p = 0.004). At POD 14, the NIFI group had a value of 8.8 mg/dL (0.6), compared with 8.6 mg/dL (0.6) for the control group (p = 0.008). All 5 patients with postoperative hypocalcemia in the NIFI group recovered within 2 weeks, while 1 of 14 patients with postoperative hypocalcemia in the conventional group had persistent hypocalcemia beyond 6 months. |
| Jin & Cui, 2020) [65] | In total, 186 PGs were visualized in 56 patients. | No patient in either group developed hypoparathyroidism. | No patient in either group developed hypocalcemia. |
| (D. H. Kim et al., 2021) [66] | PGs were found in 244 cases (93.5%) in the NIRAF group and in 260 cases (92.5%) in the control group. The mean count of identified PGs was 3.91 ± 0.36 in the NIRAF group vs. 3.90 ± 0.39 in the control group (p = 0.351). | The incidence of transient postoperative hypoparathyroidism was significantly lower in the NIRAF group than in the control group during hospitalization (33.7% vs. 46.6%; p = 0.002) and at 1 month (8.8% vs. 18.9%; p = 0.001) | The incidence of hypocalcemia during hospitalization was 6.5% in the NIRAF group and 10.0% in the control group. There was no significant difference in the rate of hypocalcemia between the two groups for any follow-up period. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Demarchi, M.S.; Seeliger, B.; Lifante, J.-C.; Alesina, P.F.; Triponez, F. Fluorescence Image-Guided Surgery for Thyroid Cancer: Utility for Preventing Hypoparathyroidism. Cancers 2021, 13, 3792. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13153792
Demarchi MS, Seeliger B, Lifante J-C, Alesina PF, Triponez F. Fluorescence Image-Guided Surgery for Thyroid Cancer: Utility for Preventing Hypoparathyroidism. Cancers. 2021; 13(15):3792. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13153792
Chicago/Turabian StyleDemarchi, Marco Stefano, Barbara Seeliger, Jean-Christophe Lifante, Pier Francesco Alesina, and Frédéric Triponez. 2021. "Fluorescence Image-Guided Surgery for Thyroid Cancer: Utility for Preventing Hypoparathyroidism" Cancers 13, no. 15: 3792. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13153792