
High Tumor Burden Predicts Poor Response to Enzalutamide in Metastatic Castration-Resistant Prostate Cancer Patients


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
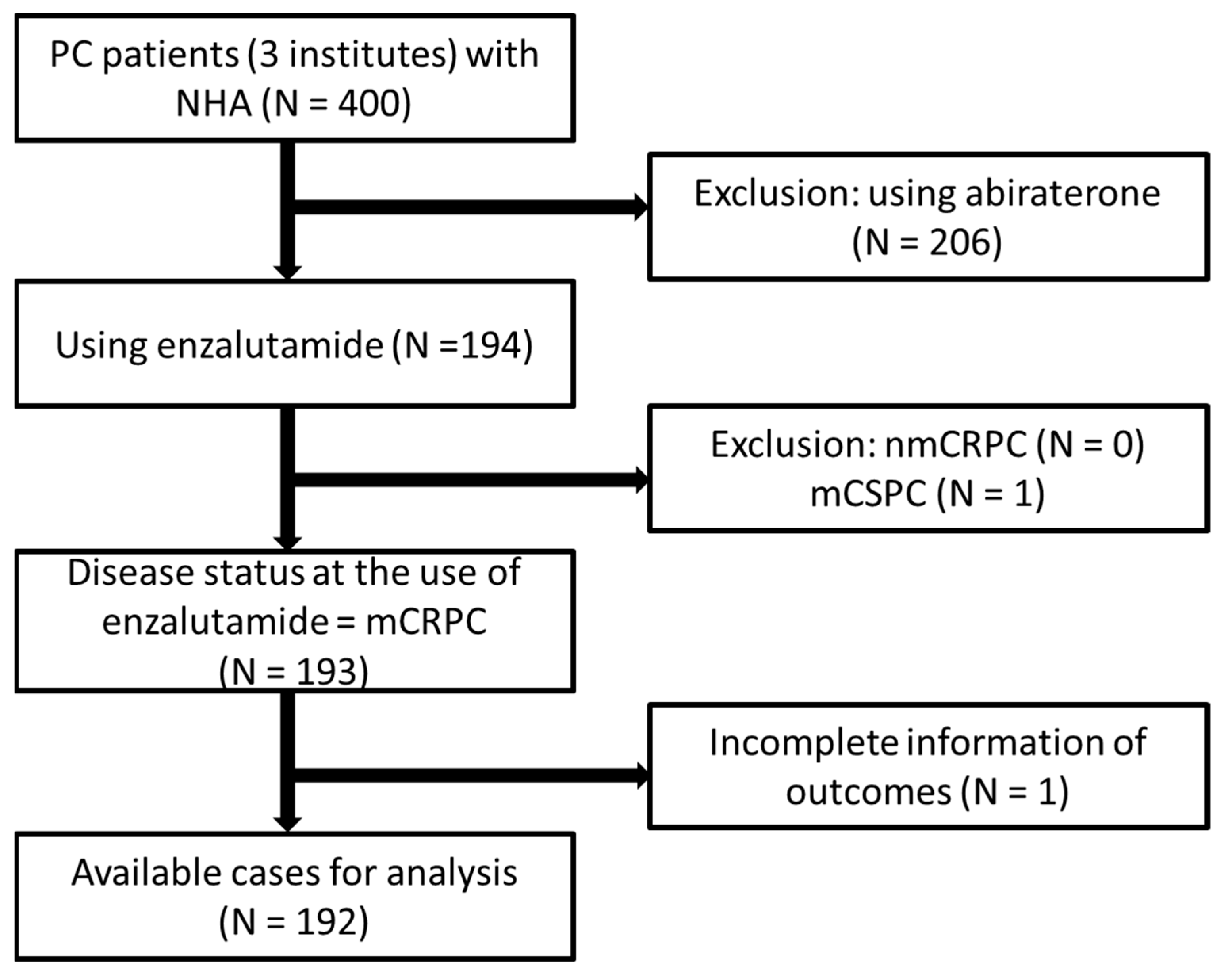
2.1. Patient Population and Selection Criteria
2.2. Definition of Tumor Burden
2.3. Clinical Information Collection and Outcome Measurement
2.4. Statistical Analysis
3. Results
3.1. Patient Demographics
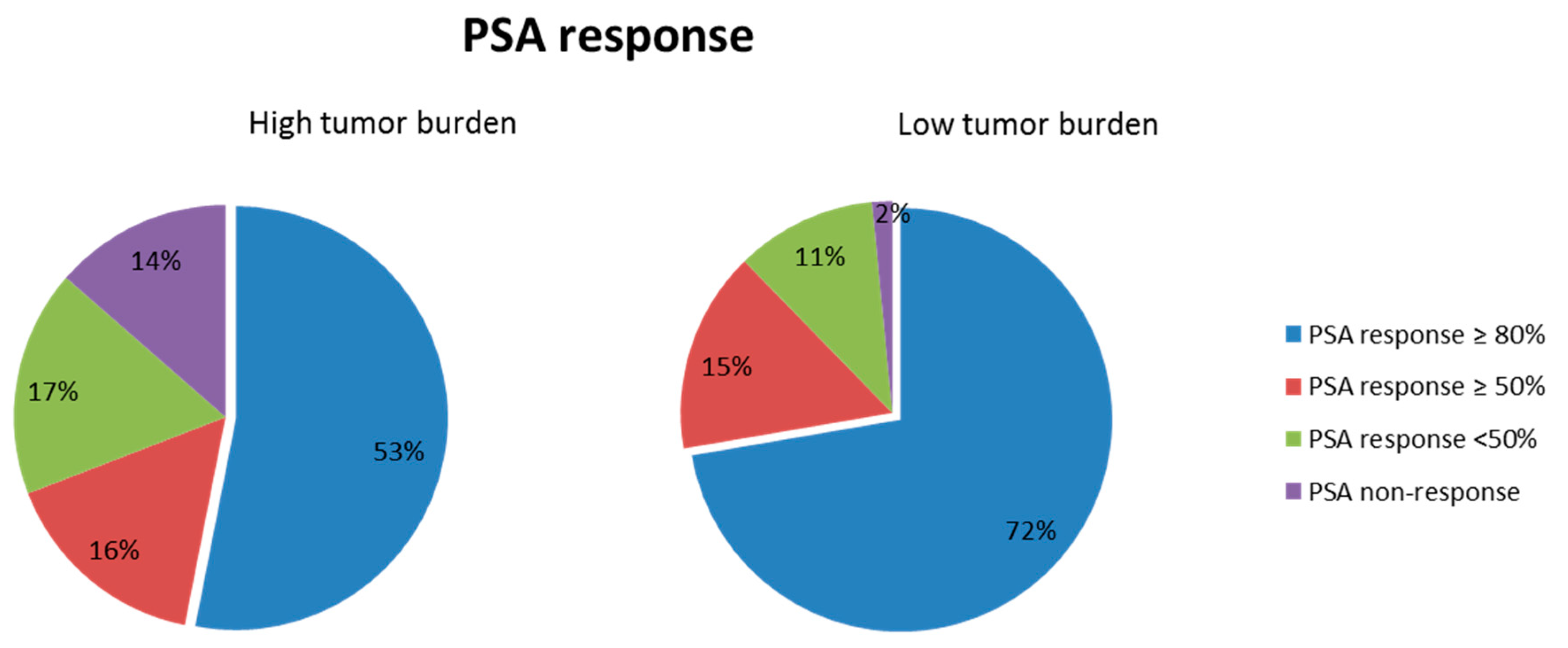
3.2. PSA Response
3.3. Radiological Response
3.4. Progression-Free Survival Duration
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chung, B.H.; Horie, S.; Chiong, E. The incidence, mortality, and risk factors of prostate cancer in Asian men. Prostate Int. 2019, 7, 1–8. [Google Scholar] [CrossRef]
- Taiwan Health and Welfare Report 2019. Available online: http://www.cdway.com.tw/gov/mhw2/book108/book01e/index.html (accessed on 15 December 2020).
- Cheng, Y.-T.; Hong, J.-H.; Lu, Y.-C.; Pu, Y.-S.; Huang, C.-Y.; Huang, K.-H.; Liu, S.P.; Chen, C.-H. Impact of high-volume disease in Asian population with newly diagnosed metastatic prostate cancer. Urol. Sci. 2018, 29, 136. [Google Scholar] [CrossRef]
- Chen, C.-H.; Tzai, T.-S.; Huang, S.-P.; Wu, H.-C.; Tai, H.-C.; Chang, Y.-H.; Pu, Y.-S. Clinical outcome of Taiwanese men with metastatic prostate cancer compared with other ethnic groups. Urology 2008, 72, 1287–1292. [Google Scholar] [CrossRef]
- Sweeney, C.J.; Chen, Y.-H.; Carducci, M.; Liu, G.; Jarrard, D.F.; Eisenberger, M.; Wong, Y.-N.; Hahn, N.; Kohli, M.; Cooney, M.M. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer. N. Engl. J. Med. 2015, 373, 737–746. [Google Scholar] [CrossRef] [PubMed]
- Kyriakopoulos, C.E.; Chen, Y.-H.; Carducci, M.A.; Liu, G.; Jarrard, D.F.; Hahn, N.M.; Shevrin, D.H.; Dreicer, R.; Hussain, M.; Eisenberger, M. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer: Long-term survival analysis of the randomized phase III E3805 CHAARTED trial. J. Clin. Oncol. 2018, 36, 1080. [Google Scholar] [CrossRef] [Green Version]
- James, N.D.; Sydes, M.R.; Clarke, N.W.; Mason, M.D.; Dearnaley, D.P.; Spears, M.R.; Ritchie, A.W.; Parker, C.C.; Russell, J.M.; Attard, G. Addition of docetaxel, zoledronic acid, or both to first-line long-term hormone therapy in prostate cancer (STAMPEDE): Survival results from an adaptive, multiarm, multistage, platform randomised controlled trial. Lancet 2016, 387, 1163–1177. [Google Scholar] [CrossRef] [Green Version]
- Fizazi, K.; Tran, N.; Fein, L.; Matsubara, N.; Rodriguez-Antolin, A.; Alekseev, B.Y.; Özgüroğlu, M.; Ye, D.; Feyerabend, S.; Protheroe, A. Abiraterone acetate plus prednisone in patients with newly diagnosed high-risk metastatic castration-sensitive prostate cancer (LATITUDE): Final overall survival analysis of a randomised, double-blind, phase 3 trial. Lancet Oncol. 2019, 20, 686–700. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. Prostate Cancer (Version 2.2021). Available online: https://www.nccn.org/professionals/physician_gls/default.aspx-prostate (accessed on 15 April 2021).
- Beer, T.M.; Armstrong, A.J.; Rathkopf, D.E.; Loriot, Y.; Sternberg, C.N.; Higano, C.S.; Iversen, P.; Bhattacharya, S.; Carles, J.; Chowdhury, S. Enzalutamide in metastatic prostate cancer before chemotherapy. N. Engl. J. Med. 2014, 371, 424–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scher, H.I.; Fizazi, K.; Saad, F.; Taplin, M.-E.; Sternberg, C.N.; Miller, K.; de Wit, R.; Mulders, P.; Chi, K.N.; Shore, N.D. Increased survival with enzalutamide in prostate cancer after chemotherapy. N. Engl. J. Med. 2012, 367, 1187–1197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eisenberger, M.A.; Blumenstein, B.A.; Crawford, E.D.; Miller, G.; McLeod, D.G.; Loehrer, P.J.; Wilding, G.; Sears, K.; Culkin, D.J.; Thompson, I.M., Jr. Bilateral orchiectomy with or without flutamide for metastatic prostate cancer. N. Engl. J. Med. 1998, 339, 1036–1042. [Google Scholar] [CrossRef] [Green Version]
- Hussain, M.; Goldman, B.; Tangen, C.; Higano, C.S.; Petrylak, D.P.; Wilding, G.; Akdas, A.M.; Small, E.J.; Donnelly, B.J.; Sundram, S.K. Prostate-specific antigen progression predicts overall survival in patients with metastatic prostate cancer: Data from Southwest Oncology Group Trials 9346 (Intergroup Study 0162) and 9916. J. Clin. Oncol. 2009, 27, 2450. [Google Scholar] [CrossRef] [PubMed]
- Rigaud, J.; Tiguert, R.; Le Normand, L.; Karam, G.; Glemain, P.; Buzelin, J.-M.; Bouchot, O. Prognostic value of bone scan in patients with metastatic prostate cancer treated initially with androgen deprivation therapy. J. Urol. 2002, 168 Pt 1, 1423–1426. [Google Scholar] [CrossRef]
- Buelens, S.; Poelaert, F.; Dhondt, B.; Fonteyne, V.; De Visschere, P.; Ost, P.; Verbeke, S.; Villeirs, G.; De Man, K.; Rottey, S. Metastatic Burden in Newly Diagnosed Hormone-Naive Metastatic Prostate Cancer: Comparing dEfinitions of CHAARTED and LATITUDE Trial; Urologic Oncology: Seminars and Original Investigations; Elsevier: Amsterdam, The Netherlands, 2018; pp. 158.e13–158.e20. [Google Scholar]
- Alhanafy, A.M.; Zanaty, F.; Ibrahem, R.; Omar, S. Prognostic factors for hormone sensitive metastatic prostate cancer: Impact of disease volume. Asian Pac. J. Cancer Prev. APJCP 2018, 19, 1113. [Google Scholar] [PubMed]
- Xu, X.S.; Ryan, C.J.; Stuyckens, K.; Smith, M.R.; Saad, F.; Griffin, T.W.; Park, Y.C.; Margaret, K.Y.; Vermeulen, A.; Poggesi, I. Correlation between Prostate-Specific Antigen Kinetics and Overall Survival in Abiraterone Acetate–Treated Castration-Resistant Prostate Cancer Patients. Clin. Cancer Res. 2015, 21, 3170–3177. [Google Scholar] [CrossRef] [Green Version]
- De Velasco, G.; Lora, D.; Lorente, D.; Choueiri, T.K.; Sweeney, C.; Castellano, D.E. Impact of statins on outcomes in patients (pts) with metastatic castration resistant prostate cancer (mCRPC): Post-hoc analysis of data from COU-AA-301 and COU-AA-302 trials. Am. Soc. Clin. Oncol. 2018, 36, 230–230. [Google Scholar] [CrossRef]
- Fuerea, A.; Baciarello, G.; Patrikidou, A.; Albigès, L.; Massard, C.; Di Palma, M.; Escudier, B.; Fizazi, K.; Loriot, Y. Early PSA response is an independent prognostic factor in patients with metastatic castration-resistant prostate cancer treated with next-generation androgen pathway inhibitors. Eur. J. Cancer 2016, 61, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, A.J.; Szmulewitz, R.Z.; Petrylak, D.P.; Holzbeierlein, J.; Villers, A.; Azad, A.; Alcaraz, A.; Alekseev, B.; Iguchi, T.; Shore, N.D. ARCHES: A randomized, phase III study of androgen deprivation therapy with enzalutamide or placebo in men with metastatic hormone-sensitive prostate cancer. J. Clin. Oncol. 2019, 37, 2974–2986. [Google Scholar] [CrossRef] [PubMed]
- Davis, I.D.; Martin, A.J.; Stockler, M.R.; Begbie, S.; Chi, K.N.; Chowdhury, S.; Coskinas, X.; Frydenberg, M.; Hague, W.E.; Horvath, L.G. Enzalutamide with standard first-line therapy in metastatic prostate cancer. N. Engl. J. Med. 2019, 381, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.-S.; Theeuwes, A.; Kwon, D.D.; Choi, Y.D.; Chung, B.H.; Lee, H.M.; Lee, K.H.; Lee, S.E. The PREVAIL trial of enzalutamide in men with chemotherapy-naïve, metastatic castration-resistant prostate cancer: Post hoc analysis of Korean patients. Investig. Clin. Urol. 2016, 57, 174–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, C.S.; Choi, Y.D.; Lee, S.E.; Lee, H.M.; Ueda, T.; Yonese, J.; Fukagai, T.; Chiong, E.; Lau, W.; Abhyankar, S. Post hoc analyses of East Asian patients from the randomized placebo-controlled PREVAIL trial of enzalutamide in patients with chemotherapy-naïve, metastatic castration-resistant prostate cancer. Medicine 2017, 96, e7223. [Google Scholar] [CrossRef]
- Kimura, G.; Yonese, J.; Fukagai, T.; Kamba, T.; Nishimura, K.; Nozawa, M.; Mansbach, H.; Theeuwes, A.; Beer, T.M.; Tombal, B. Enzalutamide in Japanese patients with chemotherapy-naïve, metastatic castration-resistant prostate cancer: A post-hoc analysis of the placebo-controlled PREVAIL trial. Int. J. Urol. 2016, 23, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Evans, C.P.; Higano, C.S.; Keane, T.; Andriole, G.; Saad, F.; Iversen, P.; Miller, K.; Kim, C.-S.; Kimura, G.; Armstrong, A.J. The PREVAIL study: Primary outcomes by site and extent of baseline disease for enzalutamide-treated men with chemotherapy-naive metastatic castration-resistant prostate cancer. Eur. Urol. 2016, 70, 675–683. [Google Scholar] [CrossRef] [PubMed]
- Chi, K.; Hotte, S.; Joshua, A.; North, S.; Wyatt, A.; Collins, L.; Saad, F. Treatment of mCRPC in the AR-axis-targeted therapy-resistant state. Ann. Oncol. 2015, 26, 2044–2056. [Google Scholar] [CrossRef] [Green Version]
- Saad, F.; de Bono, J.; Shore, N.; Fizazi, K.; Loriot, Y.; Hirmand, M.; Franks, B.; Haas, G.P.; Scher, H.I. Efficacy outcomes by baseline prostate-specific antigen quartile in the AFFIRM trial. Eur. Urol. 2015, 67, 223–230. [Google Scholar] [CrossRef]
- Poon, D.M.; Wong, K.C.; Chan, T.; Law, K.; Chan, K.; Lee, E.K.; Lee, C.; Chan, M.; Hong Kong Society of Uro-Oncology (HKSUO). Survival outcomes, prostate-specific antigen response, and tolerance in first and later lines of enzalutamide treatment for metastatic castration-resistant prostate cancer: A real-world experience in Hong Kong. Clin. Genitourin. Cancer 2018, 16, 402–412.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mori, K.; Kimura, T.; Onuma, H.; Kimura, S.; Yamamoto, T.; Sasaki, H.; Miki, J.; Miki, K.; Egawa, S. Lactate dehydrogenase predicts combined progression-free survival after sequential therapy with abiraterone and enzalutamide for patients with castration-resistant prostate cancer. Prostate 2017, 77, 1144–1150. [Google Scholar] [CrossRef] [PubMed]
- Chi, K.N.; Kheoh, T.; Ryan, C.J.; Molina, A.; Bellmunt, J.; Vogelzang, N.J.; Rathkopf, D.E.; Fizazi, K.; Kantoff, P.W.; Li, J. A prognostic index model for predicting overall survival in patients with metastatic castration-resistant prostate cancer treated with abiraterone acetate after docetaxel. Ann. Oncol. 2016, 27, 454–460. [Google Scholar] [CrossRef]
- Templeton, A.J.; Pezaro, C.; Omlin, A.; McNamara, M.G.; Leibowitz-Amit, R.; Vera-Badillo, F.E.; Attard, G.; De Bono, J.S.; Tannock, I.F.; Amir, E. Simple prognostic score for metastatic castration-resistant prostate cancer with incorporation of neutrophil-to-lymphocyte ratio. Cancer 2014, 120, 3346–3352. [Google Scholar] [CrossRef]
- Linder, S.; van der Poel, H.G.; Bergman, A.M.; Zwart, W.; Prekovic, S. Enzalutamide therapy for advanced prostate cancer: Efficacy, resistance and beyond. Endocr. Relat. Cancer 2019, 26, R31–R52. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups * | All Patients | Low Tumor Burden | High Tumor Burden | p-Value | ||
|---|---|---|---|---|---|---|
| Patient number (n) | 192 | 88 | 45.8% | 104 | 54.2% | |
| Median age (range, years) | 72 (46–94) | 74 (51–94) | 71 (46–90) | 0.065 | ||
| Median mPC to mCRPC (range, months) | 14 (0–148.9) | 13.3 (0–148.9) | 14.3 (0–125.9) | 0.955 | ||
| Median mCRPC to enzalutamide (range, months) | 4 (0–106.2) | 4 (0–72.1) | 3.9 (0–106.2) | 0.848 | ||
| Median PSA at diagnosis | 117.3 (3.2–16,410.5) | 63.4 (3.3–9424.7) | 256.6 (3.2–16,410) | <0.001 | ||
| ECOG | 0.278 | |||||
| 0 | 105 | 53 | 60.2% | 52 | 50.0% | |
| 1 | 67 | 29 | 33.0% | 38 | 36.5% | |
| 2 and 3 | 20 | 6 | 6.8% | 14 | 13.5% | |
| Gleason sum | 0.724 | |||||
| ≤6 | 10 | 5 | 5.7% | 5 | 4.8% | |
| 3 + 4 | 12 | 4 | 4.5% | 8 | 7.7% | |
| 4 + 3 | 29 | 15 | 17.0% | 14 | 13.5% | |
| 8~10 | 128 | 57 | 64.8% | 71 | 68.3% | |
| Missing | 13 | 7 | 8.0% | 6 | 5.8% | |
| Abnormal PSA only | 0.368 | |||||
| Yes | 71 | 36 | 40.9% | 35 | 33.7% | |
| No | 121 | 52 | 59.1% | 69 | 66.3% | |
| Abnormal PSA and DRE | 0.171 | |||||
| Yes | 54 | 29 | 33.0% | 25 | 24.0% | |
| No | 138 | 59 | 67.0% | 79 | 76.0% | |
| LUTS | 0.664 | |||||
| Yes | 90 | 43 | 48.9% | 47 | 45.2% | |
| No | 102 | 45 | 51.1% | 57 | 54.8% | |
| Hematuria | 0.473 | |||||
| Yes | 8 | 5 | 5.7% | 3 | 2.9% | |
| No | 184 | 83 | 94.3% | 101 | 54.9% | |
| Bone pain | 0.007 | |||||
| Yes | 28 | 6 | 6.8% | 22 | 21.2% | |
| No | 164 | 82 | 93.2% | 82 | 78.9% | |
| Other metastasis-related symptoms | 0.064 | |||||
| Yes | 5 | 0 | 0.0% | 5 | 4.8% | |
| No | 187 | 88 | 100% | 99 | 95.2% | |
| Skeletal-related events | 0.03 | |||||
| Yes | 25 | 6 | 6.8% | 19 | 18.3% | |
| No | 167 | 82 | 93.2% | 85 | 81.7% | |
| Prior chemotherapy | 0.005 | |||||
| Yes | 62 | 19 | 21.6% | 43 | 41.4% | |
| No | 130 | 69 | 78.4% | 61 | 58.7% | |
| PSA response | 0.026 | |||||
| >80% | 90 | 47 | 53.4% | 43 | 41.3% | |
| <80% | 56 | 18 | 20.5% | 38 | 36.5% | |
| NA or missing | 46 | 23 | 26.1% | 23 | 22.1% | |
| Radiological response | 0.017 | |||||
| CR, PR and SD | 109 | 52 | 59.1% | 57 | 54.8% | |
| PD | 22 | 4 | 4.5% | 18 | 17.3% | |
| NA or missing | 61 | 32 | 36.4% | 29 | 27.9% |
| Variables | Case Number | Events | Univariable | Multivariable * | ||||
|---|---|---|---|---|---|---|---|---|
| OR | Range | p Value | OR | Range | p Value | |||
| Age | 146 | 90 | 1.02 | 0.99–1.06 | 0.232 | — | — | — |
| Time from mPC to mCRPC (months) | 141 (5 missing) | 87 | 1.01 | 0.99–1.03 | 0.277 | — | — | — |
| Time from mCRPC to enzalutamide (range, months) | 141 (5 missing) | 87 | 1.01 | 0.98–1.03 | 0.648 | — | — | — |
| PSA before enzalutamide (ng/mL) | ||||||||
| <10 | 54 | 35 | 1 | — | — | — | — | — |
| 10~<50 | 54 | 31 | 0.73 | 0.34–1.59 | 0.43 | — | — | — |
| ≥50 | 38 | 24 | 0.93 | 0.39–2.21 | 0.87 | — | — | — |
| Gleason sum | ||||||||
| ≤7 | 35 | 24 | 1 | — | — | — | — | — |
| 8~10 | 100 | 60 | 0.69 | 0.30–1.56 | 0.369 | — | — | — |
| Missing | 11 | 6 | 0.55 | 0.14–2.2 | 0.397 | — | — | — |
| ECOG | ||||||||
| 0 | 75 | 46 | 1 | — | — | — | — | — |
| 1 | 54 | 32 | 0.92 | 0.45–1.87 | 0.812 | — | — | — |
| 2 and 3 | 17 | 12 | 1.51 | 0.48–4.74 | 0.477 | — | — | — |
| Initial presentation | ||||||||
| Abnormal PSA only | ||||||||
| No | 97 | 59 | 1 | — | — | — | — | — |
| Yes | 49 | 31 | 1.11 | 0.55–2.26 | 0.775 | — | — | — |
| Abnormal PSA and DRE | ||||||||
| No | 104 | 58 | 1 | — | — | — | — | — |
| Yes | 42 | 32 | 2.48 | 1.11–5.58 | 0.028 | — | — | — |
| LUTS | ||||||||
| No | 78 | 46 | 1 | — | — | — | — | — |
| Yes | 68 | 44 | 1.28 | 0.65–2.5 | 0.478 | — | — | — |
| Hematuria | ||||||||
| No | 143 | 89 | 1 | — | — | — | — | — |
| Yes | 3 | 1 | 0.30 | 0.03–3.43 | 0.335 | — | — | — |
| Bone pain | ||||||||
| No | 125 | 77 | 1 | — | — | — | — | — |
| Yes | 21 | 13 | 1.01 | 0.39–2.62 | 0.979 | — | — | — |
| Other metastasis-related symptoms | ||||||||
| No | 142 | 87 | 1 | — | — | — | — | — |
| Yes | 4 | 3 | 1.90 | 0.19–18.7 | 0.584 | — | — | — |
| Comorbidities | ||||||||
| Hypertension | ||||||||
| No | 57 | 29 | 1 | — | — | 1 | — | — |
| Yes | 89 | 61 | 2.10 | 1.06–4.18 | 0.033 | 3.00 | 1.31–6.84 | 0.009 |
| Diabetes mellitus | ||||||||
| No | 111 | 66 | 1 | — | — | — | — | — |
| Yes | 35 | 24 | 1.49 | 0.66–3.34 | 0.335 | — | — | — |
| Heart disease | ||||||||
| No | 112 | 68 | 1 | — | — | — | — | — |
| Yes | 34 | 22 | 1.19 | 0.53–2.64 | 0.675 | — | — | — |
| Liver disease | ||||||||
| No | 131 | 84 | 1 | — | — | 1 | — | — |
| Yes | 15 | 6 | 0.37 | 0.13–1.11 | 0.077 | 0.44 | 0.12–1.63 | 0.217 |
| Renal disease | ||||||||
| No | 128 | 78 | 1 | — | — | — | — | — |
| Yes | 18 | 12 | 1.28 | 0.45–3.64 | 0.64 | — | — | — |
| Symptomatic BPE | ||||||||
| No | 92 | 52 | 1 | — | — | 1 | — | — |
| Yes | 54 | 38 | 1.83 | 0.89–3.73 | 0.099 | 1.52 | 0.65–3.54 | 0.332 |
| Tumor-associated status before enzalutamide | ||||||||
| Tumor burden | ||||||||
| Low | 65 | 47 | 1 | — | — | 1 | — | — |
| High | 81 | 43 | 0.43 | 0.22–0.87 | 0.019 | 0.44 | 0.19–1.0 | 0.05 |
| Prior chemotherapy history | ||||||||
| No | 101 | 67 | 1 | — | — | 1 | — | — |
| Yes | 45 | 23 | 0.53 | 0.26–1.09 | 0.082 | 0.51 | 0.19–1.35 | 0.174 |
| Bone pain | ||||||||
| No | 120 | 72 | 1 | — | — | — | — | — |
| Yes | 26 | 18 | 1.50 | 0.60–3.72 | 0.382 | — | — | — |
| Skeletal-related events | ||||||||
| No | 130 | 80 | 1 | — | — | — | — | — |
| Yes | 16 | 10 | 1.04 | 0.36–3.04 | 0.941 | — | — | — |
| Laboratory data before enzalutamide | ||||||||
| Hemoglobulin (g/dL) | ||||||||
| <12 | 52 | 27 | 1 | — | — | — | — | — |
| ≥12 | 50 | 35 | 2.16 | 0.96–4.87 | 0.063 | 2.70 | 1.07–6.8 | 0.035 |
| Missing | 44 | 28 | 1.62 | 0.71–3.68 | 0.249 | 1.89 | 0.59–6.03 | 0.283 |
| Platelet count (k/μL) | ||||||||
| <200 | 55 | 39 | 1 | — | — | 1 | — | — |
| ≥200 | 73 | 41 | 0.53 | 0.25–1.11 | 0.09 | 0.48 | 0.2–1.12 | 0.088 |
| Missing | 18 | 10 | 0.51 | 0.17–1.54 | 0.233 | 0.59 | 0.14–2.56 | 0.482 |
| LDH (IU/L) | ||||||||
| <200 | 18 | 15 | 1 | — | — | 1 | — | — |
| ≥200 | 18 | 9 | 0.20 | 0.04–0.94 | 0.041 | 0.19 | 0.34–1.04 | 0.055 |
| Missing | 110 | 66 | 0.30 | 0.08–1.1 | 0.069 | 0.16 | 0.04–0.69 | 0.014 |
| Variables | Case Number | Events | Univariable | Multivariable * | ||||
|---|---|---|---|---|---|---|---|---|
| OR | Range | p-Value | OR | Range | p-Value | |||
| Age | 131 | 109 | 1.01 | 0.96–1.07 | 0.653 | — | — | — |
| time from mPC to mCRPC (months) | 128 (3 missing) | 108 | 1.00 | 0.98–1.03 | 0.912 | — | — | — |
| Time from mCRPC to enzalutamide (range, months) | 127 (4 missing) | 107 | 0.98 | 0.95–1.01 | 0.206 | — | — | — |
| PSA before enzalutamide (ng/mL) | ||||||||
| <10 | 48 | 39 | 1 | — | — | — | — | — |
| 10~<50 | 51 | 44 | 1.45 | 0.49–4.26 | 0.499 | — | — | — |
| ≥50 | 32 | 26 | 1.00 | 0.32–3.15 | 1 | — | — | — |
| Gleason sum | ||||||||
| ≤7 | 27 | 21 | 1 | — | — | — | — | — |
| 8~10 | 99 | 83 | 1.48 | 0.52–4.25 | 0.464 | — | — | — |
| Missing | 5 | 5 | Drop due to perfect prediction | — | — | — | ||
| ECOG | ||||||||
| 0 | 72 | 61 | 1 | — | — | — | — | — |
| 1 | 46 | 38 | 0.86 | 0.32–2.32 | 0.761 | — | — | — |
| 2 and 3 | 13 | 10 | 0.60 | 0.14–2.54 | 0.489 | — | — | — |
| Initial presentation | ||||||||
| Abnormal PSA only | ||||||||
| No | 87 | 74 | 1 | — | — | — | — | — |
| Yes | 44 | 35 | 0.68 | 0.27–1.75 | 0.427 | — | — | — |
| Abnormal PSA and DRE | ||||||||
| No | 91 | 74 | 1 | — | — | — | — | — |
| Yes | 40 | 35 | 1.51 | 0.51–4.46 | 0.453 | — | — | — |
| LUTS | ||||||||
| No | 77 | 63 | 1 | — | — | — | — | — |
| Yes | 54 | 46 | 1.28 | 0.5–3.3 | 0.612 | — | — | — |
| Hematuria | ||||||||
| No | 128 | 108 | 1 | — | — | 1 | — | — |
| Yes | 3 | 1 | 0.09 | 0.01–1.07 | 0.057 | 0.21 | 0.01–4.43 | 0.319 |
| Bone pain | ||||||||
| No | 113 | 94 | 1 | — | — | — | — | — |
| Yes | 18 | 15 | 1.01 | 0.26–3.84 | 0.988 | — | — | — |
| Other metastasis-related symptoms | ||||||||
| No | 128 | 107 | 1 | — | — | — | — | — |
| Yes | 3 | 2 | 0.39 | 0.34–4.53 | 0.454 | — | — | — |
| Comorbidities | ||||||||
| Hypertension | ||||||||
| No | 50 | 39 | 1 | — | — | — | — | — |
| Yes | 81 | 70 | 1.79 | 0.71–4.52 | 0.214 | — | — | — |
| Diabetes mellitus | ||||||||
| No | 99 | 84 | 1 | — | — | — | — | — |
| Yes | 32 | 25 | 0.64 | 0.23–1.74 | 0.379 | — | — | — |
| Heart disease | ||||||||
| No | 102 | 85 | 1 | — | — | — | — | — |
| Yes | 29 | 24 | 0.96 | 0.32–2.87 | 0.942 | — | — | — |
| Liver disease | ||||||||
| No | 116 | 96 | 1 | — | — | — | — | — |
| Yes | 15 | 13 | 1.35 | 0.28–6.48 | 0.704 | — | — | — |
| Renal disease | ||||||||
| No | 115 | 95 | 1 | — | — | — | — | — |
| Yes | 16 | 14 | 1.47 | 0.31–7.0 | 0.626 | — | — | — |
| Symptomatic BPE | ||||||||
| No | 79 | 67 | 1 | — | — | — | — | — |
| Yes | 52 | 42 | 0.75 | 0.3–1.89 | 0.546 | — | — | — |
| Tumor-associated status before enzalutamide | ||||||||
| Tumor burden | ||||||||
| Low | 50 | 66 | 1 | — | — | 1 | — | — |
| High | 81 | 43 | 0.24 | 0.07–0.77 | 0.016 | 0.21 | 0.06–0.77 | 0.018 |
| Prior chemotherapy history | ||||||||
| No | 86 | 75 | 1 | — | — | 1 | — | — |
| Yes | 45 | 34 | 0.45 | 0.18–1.15 | 0.095 | 0.60 | 0.18–2.00 | 0.407 |
| Bone pain | ||||||||
| No | 109 | 90 | 1 | — | — | — | — | — |
| Yes | 22 | 19 | 1.34 | 0.36–4.98 | 0.665 | — | — | — |
| Skeletal-related events | ||||||||
| No | 113 | 95 | 1 | — | — | — | — | — |
| Yes | 18 | 14 | 0.66 | 0.2–2.25 | 0.509 | — | — | — |
| Laboratory data before enzalutamide | ||||||||
| Hemoglobulin (g/dL) | ||||||||
| <12 | 44 | 34 | 1 | — | — | 1 | — | — |
| ≥12 | 47 | 43 | 3.16 | 0.91–10.7 | 0.07 | 4.14 | 1.04–16.4 | 0.043 |
| Missing | 40 | 32 | 1.18 | 0.41–33.5 | 0.761 | 0.56 | 0.13–2.52 | 0.454 |
| Segment WBC (%) | ||||||||
| <60 | 32 | 26 | 1 | — | — | 1 | — | — |
| ≥60 | 41 | 29 | 0.56 | 0.18–1.7 | 0.304 | 0.80 | 0.10–6.24 | 0.828 |
| Missing | 58 | 54 | 3.12 | 0.81–12.0 | 0.099 | 4.24 | 0.33–54.2 | 0.266 |
| Lymphocyte (%) | ||||||||
| <30 | 51 | 39 | 1 | — | — | 1 | — | — |
| ≥30 | 43 | 35 | 1.35 | 0.49–3.68 | 0.562 | 2.07 | 0.27–15.7 | 0.480 |
| Missing | 37 | 35 | 5.38 | 1.13–25.8 | 0.035 | 2.34 | 0.24–23.4 | 0.469 |
| Variables | Case Number | Failure Events | Univariable | Multivariable | ||||
|---|---|---|---|---|---|---|---|---|
| HR | Range | p-Value | HR | Range | p-Value | |||
| Age | 192 | 89 | 1.00 | 0.98–1.02 | 0.926 | — | — | — |
| time from mPC to mCRPC (months) | 181 (11 missing) | 87 | 0.98 | 0.97–1.00 | 0.010 | 0.99 | 0.97–1.00 | 0.058 |
| Time from mCRPC to enzalutamide (range, months) | 179 (13 missing) | 86 | 1.00 | 0.98–1.01 | 0.676 | — | — | — |
| PSA before enzalutamide (ng/mL) | ||||||||
| <10 | 79 | 25 | 1 | — | — | 1 | — | — |
| 10~<50 | 64 | 35 | 1.99 | 1.19–3.32 | 0.009 | 1.84 | 0.99–3.40 | 0.052 |
| ≥50 | 49 | 29 | 3.22 | 1.87–5.55 | <0.001 | 2.43 | 1.26–4.67 | 0.008 |
| Gleason sum | ||||||||
| ≤7 | 51 | 18 | 1 | — | — | 1 | — | — |
| 8~10 | 128 | 66 | 1.60 | 0.95–2.70 | 0.076 | 1.06 | 0.59–1.89 | 0.857 |
| Missing | 13 | 5 | 12.6 | 0.47–3.40 | 0.645 | 0.93 | 0.31–2.77 | 0.898 |
| ECOG | ||||||||
| 0 | 105 | 41 | 1 | — | — | 1 | — | — |
| 1 | 67 | 38 | 2.05 | 1.32–3.20 | 0.001 | 1.05 | 0.59–1.89 | 0.858 |
| 2, 3 | 20 | 10 | 2.35 | 1.17–4.73 | 0.017 | 1.59 | 0.68–3.77 | 0.287 |
| Initial presentation | ||||||||
| Abnormal PSA only | ||||||||
| No | 121 | 63 | 1 | — | — | — | — | — |
| Yes | 71 | 26 | 0.80 | 0.51–1.27 | 0.351 | — | — | — |
| Abnormal PSA and DRE | ||||||||
| No | 138 | 63 | 1 | — | — | — | — | — |
| Yes | 54 | 26 | 0.84 | 0.53–1.34 | 0.466 | — | — | — |
| LUTS | ||||||||
| No | 102 | 47 | 1 | — | — | — | — | — |
| Yes | 90 | 42 | 1.03 | 0.68–1.57 | 0.872 | — | — | — |
| Hematuria | ||||||||
| No | 184 | 86 | 1 | — | — | — | — | — |
| Yes | 8 | 3 | 1.88 | 0.59–6.01 | 0.288 | — | — | — |
| Bone pain | ||||||||
| No | 164 | 79 | 1 | — | — | — | — | — |
| Yes | 28 | 10 | 0.79 | 0.41–1.52 | 0.474 | — | — | — |
| Other metastasis-related symptoms | ||||||||
| No | 187 | 86 | 1 | — | — | — | — | — |
| Yes | 5 | 3 | 1.33 | 0.42–4.22 | 0.624 | — | — | — |
| Comorbidities | ||||||||
| Hypertension | ||||||||
| No | 72 | 38 | 1 | — | — | — | — | — |
| Yes | 120 | 51 | 0.72 | 0.47–1.1 | 0.129 | — | — | — |
| Diabetes mellitus | ||||||||
| No | 146 | 67 | 1 | — | — | — | — | — |
| Yes | 46 | 22 | 1.13 | 0.7–1.83 | 0.614 | — | — | — |
| Heart disease | ||||||||
| No | 143 | 67 | 1 | — | — | — | — | — |
| Yes | 49 | 22 | 1.06 | 0.65–1.72 | 0.819 | — | — | — |
| Liver disease | ||||||||
| No | 170 | 79 | 1 | — | — | — | — | — |
| Yes | 22 | 10 | 1.16 | 00.6–2.24 | 0.657 | — | — | — |
| Renal disease | ||||||||
| No | 171 | 77 | 1 | — | — | — | — | — |
| Yes | 21 | 12 | 1.17 | 0.63–2.14 | 0.622 | — | — | — |
| Symptomatic BPE | ||||||||
| No | 116 | 57 | 1 | — | — | — | — | — |
| Yes | 76 | 32 | 0.81 | 0.53–1.25 | 0.339 | — | — | — |
| Tumor-associated status before enzalutatmide | ||||||||
| Tumor burden | ||||||||
| Low | 88 | 32 | 1 | — | — | 1 | — | — |
| High | 104 | 57 | 1.91 | 1.24–3.0 | 0.003 | 1.40 | 0.82–2.38 | 0.221 |
| Prior chemotherapy history | ||||||||
| No | 130 | 50 | 1 | — | — | 1 | — | — |
| Yes | 62 | 39 | 2.42 | 1.59–3.7 | <0.001 | 2.23 | 1.13–4.40 | 0.021 |
| Bone pain | ||||||||
| No | 160 | 71 | 1 | — | — | — | — | — |
| Yes | 32 | 18 | 1.41 | 0.84–2.38 | 0.190 | — | — | — |
| Skeletal-related events | ||||||||
| No | 167 | 75 | 1 | — | — | — | — | — |
| Yes | 25 | 14 | 2.01 | 1.13–3.57 | 0.017 | 1.29 | 0.64–2.59 | 0.484 |
| Laboratory data before enzalutamide | ||||||||
| Hemoglobulin (g/dL) | ||||||||
| <12 | 63 | 34 | 1 | — | — | 1 | — | — |
| ≥12 | 69 | 30 | 0.54 | 0.33–0.88 | 0.014 | 0.61 | 0.32–1.14 | 0.123 |
| Missing | 60 | 25 | 0.56 | 0.34–0.95 | 0.030 | 0.67 | 0.31–1.47 | 0.316 |
| Segment WBC (%) | ||||||||
| <60 | 52 | 20 | 1 | — | — | 1 | — | — |
| ≥60 | 55 | 35 | 1.86 | 1.07–3.22 | 0.027 | 2.18 | 1.16–4.08 | 0.033 |
| Missing | 85 | 34 | 1.22 | 0.7–2.12 | 0.489 | 1.30 | 0.61–2.74 | 0.594 |
| Platelet count (k/μL) | ||||||||
| <200 | 70 | 25 | 1 | — | — | 1 | — | — |
| ≥200 | 100 | 52 | 1.65 | 1.02–2.66 | 0.040 | 1.15 | 0.66–1.99 | 0.628 |
| Missing | 22 | 12 | 1.47 | 0.74–2.94 | 0.269 | 1.88 | 0.64–5.56 | 0.253 |
| Alanine aminotransferase (U/L) | ||||||||
| <16 | 79 | 46 | 1 | — | — | 1 | — | — |
| ≥16 | 88 | 33 | 0.56 | 0.36–0.88 | 0.011 | 0.53 | 0.31–0.92 | 0.023 |
| Missing | 25 | 10 | 0.57 | 0.29–1.13 | 0.109 | 0.56 | 0.24–1.29 | 0.172 |
| Alkaline phosphatase (U/L) | ||||||||
| <100 | 47 | 22 | 1 | — | — | 1 | — | — |
| ≥100 | 19 | 13 | 2.60 | 1.3–5.2 | 0.007 | 2.18 | 1.00–4.77 | 0.051 |
| Missing | 126 | 54 | 1.00 | 0.61–1.64 | 0.999 | 1.51 | 0.77–2.97 | 0.234 |
| LDH (IU/L) | ||||||||
| <200 | 21 | 8 | 1 | — | — | 1 | — | — |
| ≥200 | 20 | 17 | 4.38 | 1.89–10.17 | 0.001 | 7.46 | 2.68–20.8 | <0.001 |
| Missing | 151 | 64 | 1.37 | 0.66–2.87 | 0.398 | 1.81 | 0.76–4.31 | 0.180 |
| Calcium (mmol/L) | ||||||||
| <2.3 | 39 | 23 | 1 | — | — | 1 | — | — |
| ≥2.3 | 56 | 24 | 0.50 | 0.28–0.89 | 0.018 | 0.58 | 0.27–1.24 | 0.162 |
| Missing | 97 | 42 | 0.58 | 0.35–0.97 | 0.037 | 1.05 | 0.50–2.21 | 0.900 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsieh, Y.-T.; Chiang, B.-J.; Wu, C.-C.; Liao, C.-H.; Lin, C.-D.; Chen, C.-H. High Tumor Burden Predicts Poor Response to Enzalutamide in Metastatic Castration-Resistant Prostate Cancer Patients. Cancers 2021, 13, 3966. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13163966
Hsieh Y-T, Chiang B-J, Wu C-C, Liao C-H, Lin C-D, Chen C-H. High Tumor Burden Predicts Poor Response to Enzalutamide in Metastatic Castration-Resistant Prostate Cancer Patients. Cancers. 2021; 13(16):3966. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13163966
Chicago/Turabian StyleHsieh, Yu-Ting, Bing-Juin Chiang, Chia-Chang Wu, Chun-Hou Liao, Chia-Da Lin, and Chung-Hsin Chen. 2021. "High Tumor Burden Predicts Poor Response to Enzalutamide in Metastatic Castration-Resistant Prostate Cancer Patients" Cancers 13, no. 16: 3966. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13163966