
Per-Feature Accuracy of Liver Imaging Reporting and Data System Locoregional Treatment Response Algorithm: A Systematic Review and Meta-Analysis


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis and Statistical Analysis
3. Results
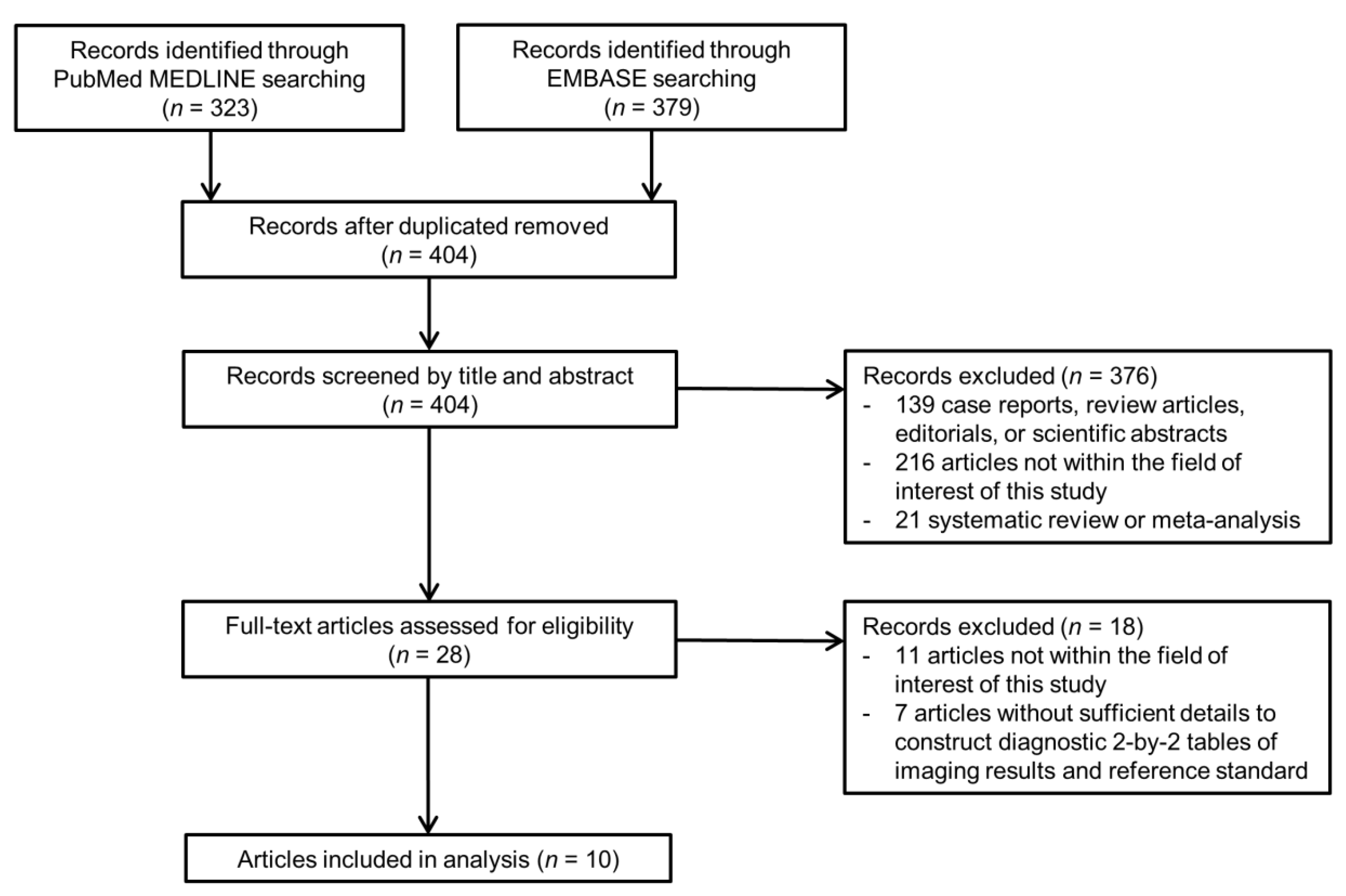
3.1. Literature Search
3.2. Study Characteristics
3.3. Quality of Included Studies
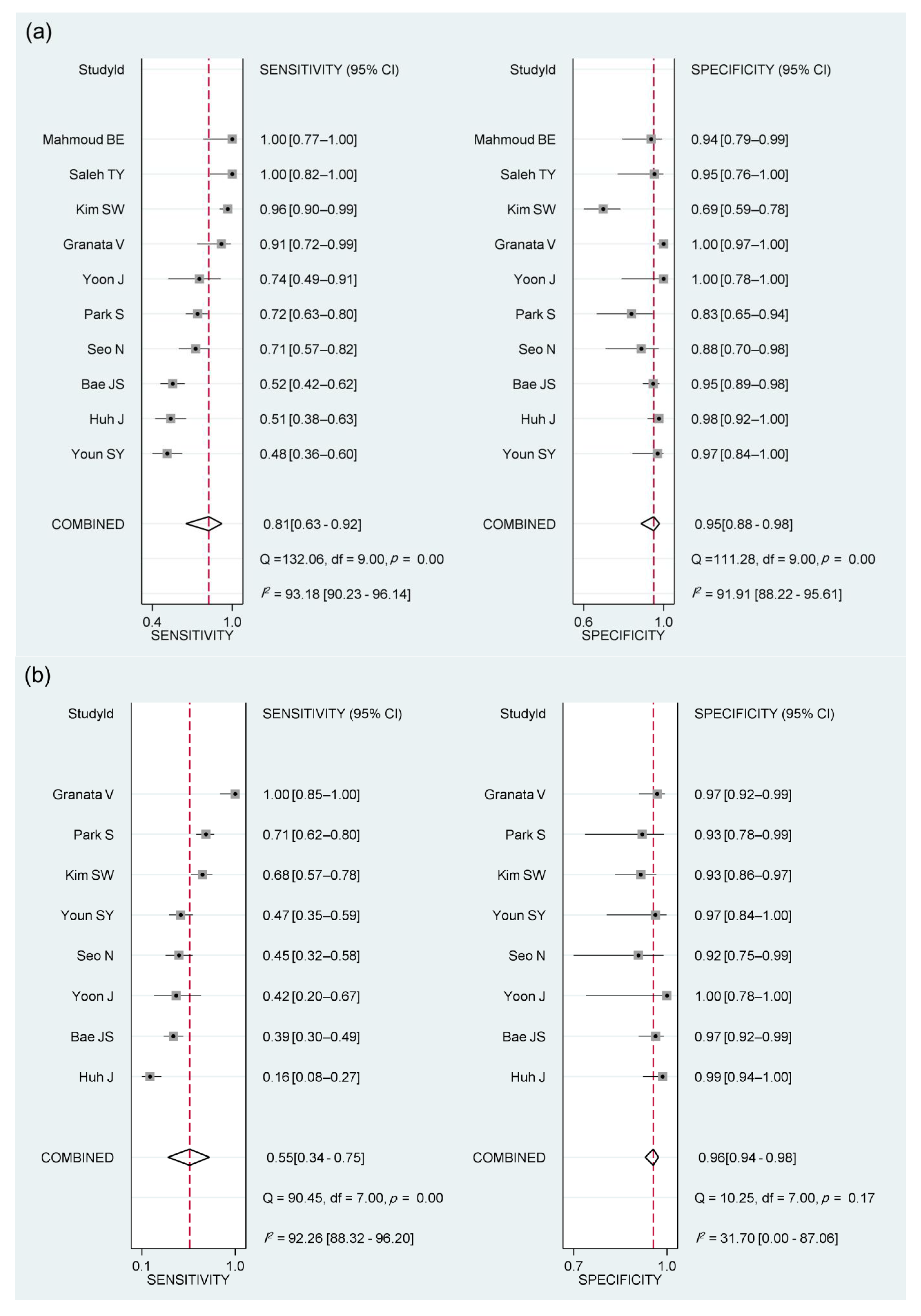
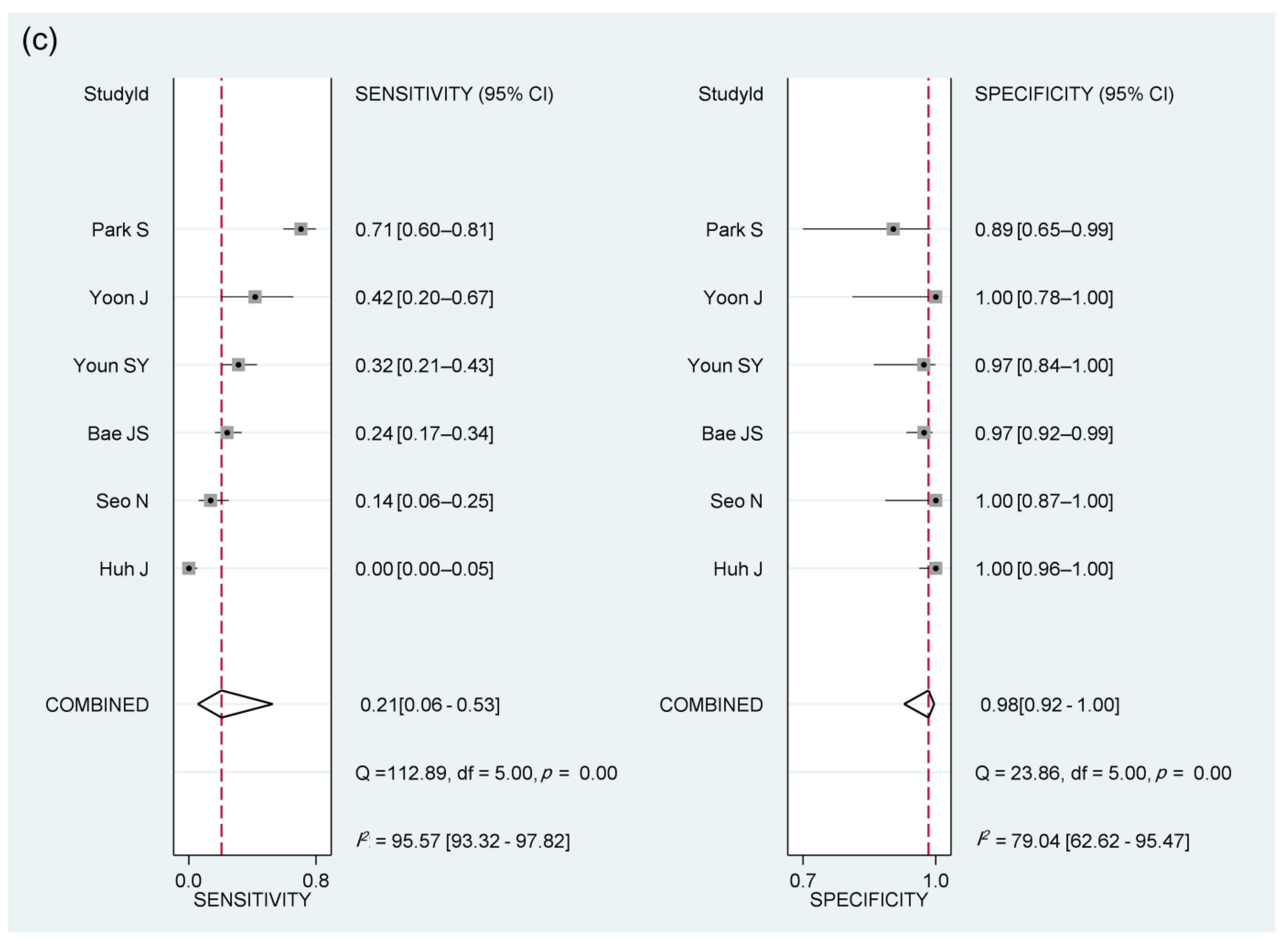
3.4. Diagnostic Performance of Imaging Features of the LR-TR Viable Category for Diagnosing Viable HCC
3.5. Subgroup Analyses According to Imaging Modality
3.6. Meta-Regression Analysis
3.7. Interobserver Agreement for Imaging Features of the LR-TR Viable Category
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bruix, J.; Sherman, M. Management of hepatocellular carcinoma: An update. Hepatology 2011, 53, 1020–1022. [Google Scholar] [CrossRef]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2017, 67, 358–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cescon, M.; Cucchetti, A.; Ravaioli, M.; Pinna, A.D. Hepatocellular carcinoma locoregional therapies for patients in the waiting list. Impact on transplantability and recurrence rate. J. Hepatol. 2013, 58, 609–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- Ho, M.-H.; Yu, C.-Y.; Chung, K.-P.; Chen, T.-W.; Chu, H.-C.; Lin, C.-K.; Hsieh, C.-B. Locoregional Therapy-Induced Tumor Necrosis as a Predictor of Recurrence after Liver Transplant in Patients with Hepatocellular Carcinoma. Ann. Surg. Oncol. 2011, 18, 3632–3639. [Google Scholar] [CrossRef] [PubMed]
- Allard, M.A.; Sebagh, M.; Ruiz, A.; Guettier, C.; Paule, B.; Vibert, E.; Cunha, A.S.; Cherqui, D.; Samuel, D.; Bismuth, H.; et al. Does pathological response after transarterial chemoembolization for hepatocellular carcinoma in cirrhotic patients with cirrhosis predict outcome after liver resection or transplantation? J. Hepatol. 2015, 63, 83–92. [Google Scholar] [CrossRef]
- American College of Radiology. Liver Imaging Reporting and Data System (LI-RADS). Available online: https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/LI-RADS/CT-MRI-LI-RADS-v2017 (accessed on 25 May 2021).
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) Assessment for Hepatocellular Carcinoma. Semin. Liver Dis. 2010, 30, 052–060. [Google Scholar] [CrossRef] [Green Version]
- Bruix, J.; Sherman, M.; Llovet, J.M.; Beaugrand, M.; Lencioni, R.; Burroughs, A.K.; Christensen, E.; Pagliaro, L.; Colombo, M.; Rodés, J. Clinical Management of Hepatocellular Carcinoma. Conclusions of the Barcelona-2000 EASL Conference. J. Hepatol. 2001, 35, 421–430. [Google Scholar] [CrossRef]
- Youn, S.Y.; Kim, D.H.; Choi, S.H.; Kim, B.; Choi, J.-I.; Shin, Y.R.; Oh, S.N.; Rha, S.E. Diagnostic performance of Liver Imaging Reporting and Data System treatment response algorithm: A systematic review and meta-analysis. Eur. Radiol. 2021, 31, 4785–4793. [Google Scholar] [CrossRef]
- Kim, S.W.; Joo, I.; Kim, H.-C.; Ahn, S.J.; Kang, H.-J.; Jeon, S.K.; Lee, J.M. LI-RADS treatment response categorization on gadoxetic acid-enhanced MRI: Diagnostic performance compared to mRECIST and added value of ancillary features. Eur. Radiol. 2020, 30, 2861–2870. [Google Scholar] [CrossRef] [PubMed]
- Bae, J.S.; Lee, J.M.; Yoon, J.H.; Kang, H.-J.; Jeon, S.K.; Joo, I.; Lee, K.B.; Kim, H. Evaluation of LI-RADS Version 2018 Treatment Response Algorithm for Hepatocellular Carcinoma in Liver Transplant Candidates: Intraindividual Comparison between CT and Hepatobiliary Agent–enhanced MRI. Radiology 2021, 299, 336–345. [Google Scholar] [CrossRef] [PubMed]
- Huh, J.; Kim, B.; Lee, J.H.; Won, J.H.; Kim, J.; Kwon, Y.; Kim, J.K. Added Value of CT Arterial Subtraction Images in Liver Imaging Reporting and Data System Treatment Response Categorization for Transcatheter Arterial Chemoembolization-Treated Hepatocellular Carcinoma. Investig. Radiol. 2020, 56, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Youn, S.Y.; Kim, D.H.; Choi, J.-I.; Choi, M.H.; Kim, B.; Shin, Y.R.; Oh, S.N.; Rha, S.E. Usefulness of Arterial Subtraction in Applying Liver Imaging Reporting and Data System (LI-RADS) Treatment Response Algorithm to Gadoxetic Acid-Enhanced MRI. Korean J. Radiol. 2021, 22, 1289–1299. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.; Reitsma, J.B.; Leeflang, M.; Sterne, J.; Bossuyt, P.M. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Devillé, W.L.; Buntinx, F.; Bouter, L.M.; Montori, V.M.; De Vet, H.C.W.; Windt, D.A.W.M.V.D.; Bezemer, P.D. Conducting systematic reviews of diagnostic studies: Didactic guidelines. BMC Med. Res. Methodol. 2002, 2, 9. [Google Scholar] [CrossRef] [Green Version]
- Shropshire, E.L.; Chaudhry, M.; Miller, C.M.; Allen, B.C.; Bozdogan, E.; Cardona, D.M.; King, L.Y.; Janas, G.L.; Do, R.K.; Kim, C.Y.; et al. LI-RADS Treatment Response Algorithm: Performance and Diagnostic Accuracy. Radiology 2019, 292, 226–234. [Google Scholar] [CrossRef]
- Chaudhry, M.; McGinty, K.A.; Mervak, B.; Lerebours, R.; Li, C.; Shropshire, E.; Ronald, J.; Commander, L.; Hertel, J.; Luo, S.; et al. The LI-RADS Version 2018 MRI Treatment Response Algorithm: Evaluation of Ablated Hepatocellular Carcinoma. Radiology 2020, 294, 320–326. [Google Scholar] [CrossRef]
- Cools, K.S.; Moon, A.M.; Burke, L.M.B.; McGinty, K.A.; Strassle, P.D.; Gerber, D.A. Validation of the Liver Imaging Reporting and Data System Treatment Response Criteria After Thermal Ablation for Hepatocellular Carcinoma. Liver Transplant. 2020, 26, 203–214. [Google Scholar] [CrossRef]
- Saleh, T.Y.; Bahig, S.; Shebrya, N.; Ahmed, A.Y. Value of dynamic and DWI MRI in evaluation of HCC viability after TACE via LI-RADS v2018 diagnostic algorithm. Egypt. J. Radiol. Nucl. Med. 2019, 50, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Seo, N.; Kim, M.S.; Park, M.-S.; Choi, J.-Y.; Do, R.K.G.; Han, K.; Kim, M.-J. Evaluation of treatment response in hepatocellular carcinoma in the explanted liver with Liver Imaging Reporting and Data System version 2017. Eur. Radiol. 2020, 30, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Joo, I.; Lee, D.H.; Bae, J.S.; Yoo, J.; Kim, S.W.; Lee, J.M. Diagnostic Performance of LI-RADS Treatment Response Algorithm for Hepatocellular Carcinoma: Adding Ancillary Features to MRI Compared with Enhancement Patterns at CT and MRI. Radiology 2020, 296, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Granata, V.; Grassi, R.; Fusco, R.; Setola, S.; Belli, A.; Piccirillo, M.; Pradella, S.; Giordano, M.; Cappabianca, S.; Brunese, L.; et al. Abbreviated MRI Protocol for the Assessment of Ablated Area in HCC Patients. Int. J. Environ. Res. Public Health 2021, 18, 3598. [Google Scholar] [CrossRef]
- Yoon, J.; Lee, S.; Shin, J.; Kim, S.-S.; Kim, G.M.; Won, J.Y. LI-RADS Version 2018 Treatment Response Algorithm: Diagnostic Performance after Transarterial Radioembolization for Hepatocellular Carcinoma. Korean J. Radiol. 2021, 22, 1279–1288. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, B.E.; Gadalla, A.A.E.H.; Elkholy, S.F. The role of dynamic and diffusion MR imaging in therapeutic response assessment after microwave ablation of hepatocellular carcinoma using LI-RADS v2018 treatment response algorithm. Egypt. J. Radiol. Nucl. Med. 2021, 52, 1–10. [Google Scholar] [CrossRef]
- Centonze, L.; Di Sandro, S.; Lauterio, A.; De Carlis, R.; Frassoni, S.; Rampoldi, A.; Tuscano, B.; Bagnardi, V.; Vanzulli, A.; De Carlis, L. Surgical Resection vs. Percutaneous Ablation for Single Hepatocellular Carcinoma: Exploring the Impact of Li-RADS Classification on Oncological Outcomes. Cancers 2021, 13, 1671. [Google Scholar] [CrossRef]
- Burgio, M.D.; Sartoris, R.; Libotean, C.; Zappa, M.; Sibert, A.; Vilgrain, V.; Ronot, M. Lipiodol retention pattern after TACE for HCC is a predictor for local progression in lesions with complete response. Cancer Imaging 2019, 19, 75–79. [Google Scholar] [CrossRef]
- De Baere, T.; Arai, Y.; Lencioni, R.; Geschwind, J.H.; Rilling, W.S.; Salem, R.; Matsui, O.; Soulen, M.C. Treatment of Liver Tumors with Lipiodol TACE: Technical Recommendations from Experts Opinion. Cardiovasc. Interv. Radiol. 2015, 39, 334–343. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.H.; Choi, S.H.; Byun, J.H.; Kang, J.H.; Lim, Y.-S.; Lee, S.J.; Kim, S.Y.; Won, H.J.; Shin, Y.M.; Kim, P.-N. Arterial subtraction images of gadoxetate-enhanced MRI improve diagnosis of early-stage hepatocellular carcinoma. J. Hepatol. 2019, 71, 534–542. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Choi, S.H.; Kim, S.Y.; Kim, M.-J.; Lee, S.S.; Byun, J.H. Gadoxetic Acid–enhanced MRI of Hepatocellular Carcinoma: Value of Washout in Transitional and Hepatobiliary Phases. Radiology 2019, 291, 651–657. [Google Scholar] [CrossRef]
- Tacconelli, E. Systematic reviews: CRD′s guidance for undertaking reviews in health care. Lancet Infect. Dis. 2010, 10, 226. [Google Scholar] [CrossRef]
- Motosugi, U.; Bannas, P.; Bookwalter, C.A.; Sano, K.; Reeder, S.B. An Investigation of Transient Severe Motion Related to Gadoxetic Acid–enhanced MR Imaging. Radiology 2016, 279, 93–102. [Google Scholar] [CrossRef] [Green Version]
- Tirkes, T.; Mehta, P.; Aisen, A.M.; Lall, C.; Akisik, F. Comparison of Dynamic Phase Enhancement of Hepatocellular Carcinoma Using Gadoxetate Disodium vs Gadobenate Dimeglumine. J. Comput. Assist. Tomogr. 2015, 39, 479–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bankier, A.A.; Levine, D.; Halpern, E.F.; Kressel, H.Y. Consensus interpretation in imaging research: Is there a better way? Radiology 2010, 257, 14–17. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Publication Year) | Study Design | Number of Patients | Patient Age, Years * | Dominant Etiology of Liver Disease | No. of Treated Observations | Type of Locoregional Treatment | Imaging Modality | MRI Magnet | MRI Contrast Agent | Image Analysis | No. of Reviewers (Years of Experience) | Reference Standards for Viable HCC |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Saleh TY (2019) [21] | Prospective | 30 | 62.6 (49–72), mean (range) | Chronic viral hepatitis | 41 | TACE (100%) | MRI | 3.0-T | ECA | NA | NA | CCRS † |
| Kim SW (2020) [11] | Retrospective | 183 | 59.9 ± 10.8 | Hepatitis B | 183 | TACE (72.1%), RFA (23.0%), or DEB-TACE | MRI | 1.5- or 3.0-T | HBA | Multiple reviewers with consensus | 2 (5, 7 years) | Pathology or CCRS † |
| Seo N (2020) [22] | Retrospective | 114 | 54.0 ± 6.9 | Hepatitis B | 206 | TACE (78.6%), RFA (16.5%), or DEB-TACE | CT (n = 113) or MRI (n = 53) | 1.5- or 3.0-T | HBA or ECA | Multiple independent reviewers | 2 (16, 17 years) | Pathology (explant) |
| Park S (2020) [23] | Retrospective | 138 | 58 ± 9 | Hepatitis B | 138 | TACE (66.7%), RFA or PEIT (13.0%) | CT (n = 138) and MRI (n = 138) | 1.5- or 3.0-T | HBA | Multiple reviewers with consensus | 2 (5, 7 years) | Pathology (explant or resection) |
| Bae JS (2021) [12] | Retrospective | 165 | 62 ± 9 | Hepatitis B | 237 | TACE (67.5%), RFA (22.0%), or PEIT (4.6%) | CT (n = 165) and MRI (n = 165) | 1.5- or 3.0-T | HBA | Multiple independent reviewers | 3 (7, 9, 14 years) | Pathology (explant) |
| Granata V (2021) [24] | Retrospective | 64 | 74 (62–83), median (range) | Hepatitis B | 136 | RFA (72.1%) or MWA (27.9%) | MRI | 1.5-T | ECA | Multiple reviewers with consensus | 3 (NA) | CCRS † |
| Huh J (2021) [13] | Retrospective | 115 | 65.5 ± 10.4 | Hepatitis B | 151 | TACE (100%) | CT | NA | NA | Multiple independent reviewers | 2 (>7 years) | Pathology or CCRS † |
| Mahmoud BE (2021) [26] | Retrospective | 45 | 58.6 (45–74), mean (range) | NA | 51 | MWA (100%) | MRI | 1.5-T | ECA | Multiple reviewers with consensus | 3 (9, 11, 12 years) | CCRS † |
| Yoon J (2021) [25] | Retrospective | 27 | 55.9 ± 9.1 | Hepatitis B | 34 | TARE (100%) | CT (n = 10) or MRI (n = 17) | 3.0-T | HBA or ECA | Multiple reviewers with consensus | 3 (2, 5, 9 years) | Pathology (explant or resection) |
| Youn SY (2021) [14] | Retrospective | 90 | 57 (38–84), mean (range) | Hepatitis B | 105 | TACE (57.0%), RFA (23.8%), or DEB-TACE | MRI | 1.5- or 3.0-T | HBA | Multiple reviewers with consensus | 2 (6, 9 years) | Pathology (explant or resection) |
| Imaging Feature | No. of Studies | No. of Observations | Summary Estimates | p for Publication Bias | ||||
|---|---|---|---|---|---|---|---|---|
| Sensitivity (95% CI) | I2 | Specificity (95% CI) | I2 | DOR (95% CI) | ||||
| Overall | ||||||||
| NMLIT with APHE | 10 | 1153 | 81% (63–92) | 93% | 95% (88–98) | 92% | 81 (25–261) | 0.15 |
| NMLIT with washout appearance | 8 | 1068 | 55% (34–75) | 92% | 96% (94–98) | 32% | 32 (13–82) | 0.54 |
| NMLIT with enhancement similar to pretreatment | 6 | 709 | 21% (6–53) | 96% | 98% (92–100) | 79% | 14 (5–39) | 0.44 |
| MRI | ||||||||
| NMLIT with APHE | 8 | 968 | 87% (67–96) | 96% | 93% (84–97) | 93% | 97 (23–408) | 0.16 |
| NMLIT with washout appearance | 6 | 883 | 66% (41–84) | 91% | 95% (93–97) | 25% | 39 (12–123) | 0.51 |
| NMLIT with enhancement similar to pretreatment | 4 | 485 | 32% (16–54) | 92% | 96% (89–99) | 59% | 12 (5–28) | 0.49 |
| CT | ||||||||
| NMLIT with APHE | 4 | 729 | 50% (36–64) | 91% | 95% (89–98) | 80% | 19 (11–35) | 0.93 |
| NMLIT with washout appearance | 4 | 729 | 35% (17–59) | 96% | 97% (93–99) | 54% | 19 (9–41) | 0.29 |
| NMLIT with enhancement similar to pretreatment | 4 | 689 | 15% (1–68) | 97% | 99% (87–100) | 85% | 12 (3–41) | 0.98 |
| Imaging Feature | Covariates | Sensitivity (95% CI) | Specificity (95% CI) | p |
|---|---|---|---|---|
| NMLIT with APHE | Reference standard for viable HCC | 0.02 | ||
| Pathology only | 63% (43, 84) | 94% (87, 100) | ||
| CCRS only or both | 91% (82, 100) | 95% (90, 100) | ||
| MRI contrast agent | 0.03 | |||
| Hepatobiliary agent | 73% (50, 97) | 89% (81, 97) | ||
| Extracellular agent or both | 90% (78, 100) | 97% (95, 100) | ||
| Type of LRT | 0.72 | |||
| Transcatheter therapy (>70%) * | 85% (68, 100) | 93% (85, 100) | ||
| Others † | 77% (54, 99) | 96% (92, 100) | ||
| Image analysis | 0.23 | |||
| Multiple independent reviewers | 62% (38, 85) | 96% (91, 100) | ||
| Multiple reviewers with consensus | 85% (73, 98) | 94% (86, 100) | ||
| Percentage of viable HCC | 0.23 | |||
| ≥50% | 67% (39, 94) | 94% (85, 100) | ||
| <50% | 88% (76, 100) | 95% (90, 100) | ||
| NMLIT with washout appearance | Reference standard for viable HCC | 0.71 | ||
| Pathology only | 49% (23, 76) | 96% (93, 99) | ||
| CCRS only or both | 66% (32, 99) | 96% (94, 99) | ||
| MRI contrast agent | 0.59 | |||
| Hepatobiliary agent | 57% (33, 81) | 95% (93, 98) | ||
| Extracellular agent or both | 68% (39, 97) | 97% (94, 100) | ||
| Type of LRT | 0.23 | |||
| Transcatheter therapy (>70%) * | 41% (15, 67) | 96% (93, 98) | ||
| Others † | 68% (43, 92) | 97% (95, 99) | ||
| Image analysis | 0.03 | |||
| Multiple independent reviewers | 34% (16, 53) | 97% (95, 99) | ||
| Multiple reviewers with consensus | 73% (56, 91) | 95% (92, 98) | ||
| Percentage of viable HCC | 0.75 | |||
| ≥50% | 52% (21, 82) | 95% (91, 99) | ||
| <50% | 59% (28, 90) | 97% (95, 98) | ||
| NMLIT with enhancement similar to pretreatment | MRI contrast agent | 0.20 | ||
| Hepatobiliary agent | 42% (19, 65) | 95% (90, 100) | ||
| Extracellular agent or both | 24% (1, 47) | 100 (100, 100) | ||
| Type of LRT | 0.08 | |||
| Transcatheter therapy (>70%) * | 9% (0, 24) | 100% (100, 100) | ||
| Others † | 42% (4, 79) | 95% (89, 100) | ||
| Image analysis | 0.24 | |||
| Multiple independent reviewers | 13% (0, 28) | 98% (96, 100) | ||
| Multiple reviewers with consensus | 52% (8, 95) | 94% (86, 100) | ||
| Percentage of viable HCC | 0.20 | |||
| ≥50% | 37% (8, 67) | 97% (93, 100) | ||
| <50% | 6% (0, 18) | 98% (96, 100) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huh, Y.J.; Kim, D.H.; Kim, B.; Choi, J.-I.; Rha, S.E. Per-Feature Accuracy of Liver Imaging Reporting and Data System Locoregional Treatment Response Algorithm: A Systematic Review and Meta-Analysis. Cancers 2021, 13, 4432. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13174432
Huh YJ, Kim DH, Kim B, Choi J-I, Rha SE. Per-Feature Accuracy of Liver Imaging Reporting and Data System Locoregional Treatment Response Algorithm: A Systematic Review and Meta-Analysis. Cancers. 2021; 13(17):4432. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13174432
Chicago/Turabian StyleHuh, Yeon Jong, Dong Hwan Kim, Bohyun Kim, Joon-Il Choi, and Sung Eun Rha. 2021. "Per-Feature Accuracy of Liver Imaging Reporting and Data System Locoregional Treatment Response Algorithm: A Systematic Review and Meta-Analysis" Cancers 13, no. 17: 4432. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13174432