
Faecal Diagnostic Biomarkers for Colorectal Cancer

 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results and Discussion
3.1. ELISA Calibration Curves for the Selected Biomarkers
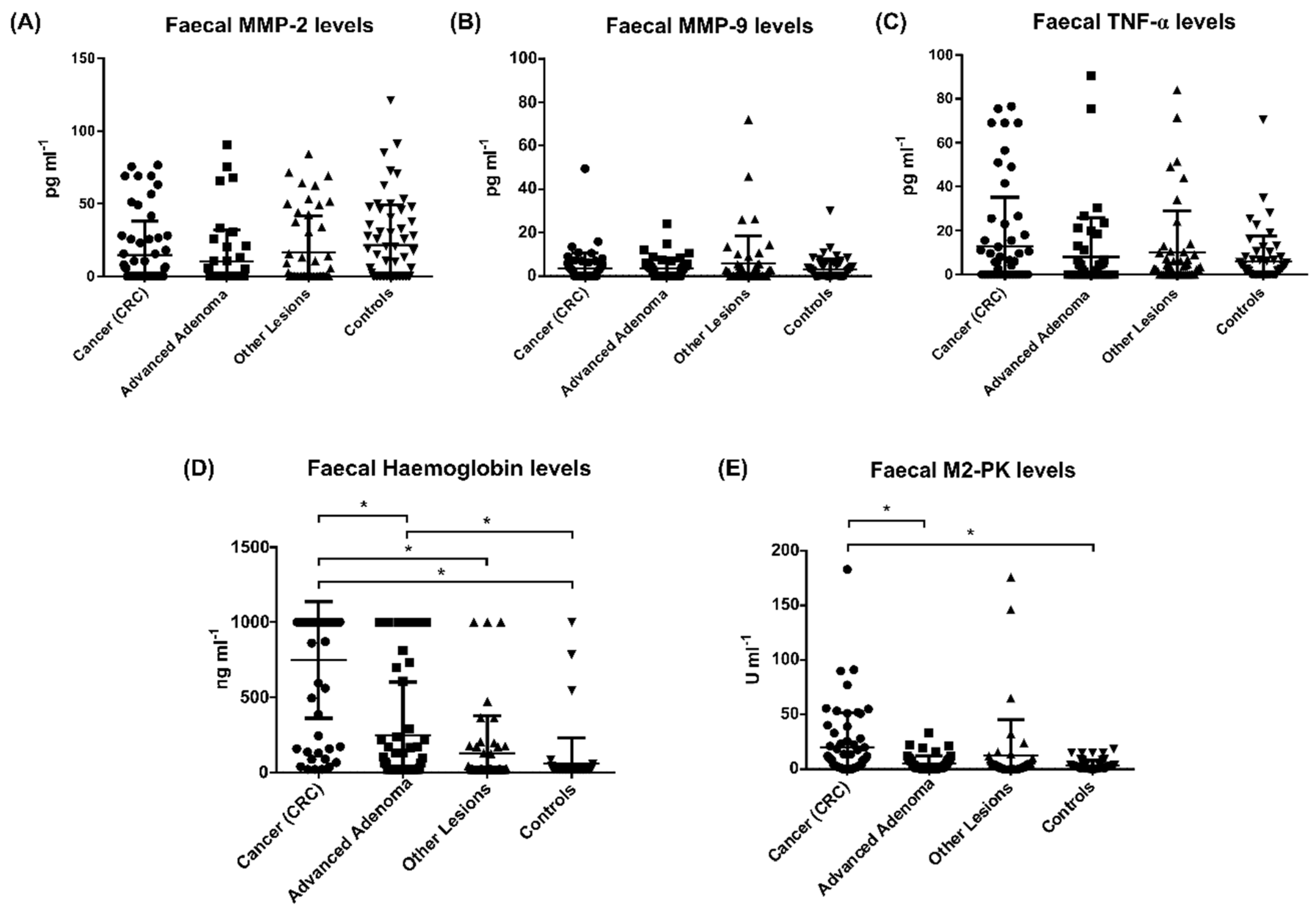
3.2. Stool Biomarker’s Levels between Groups
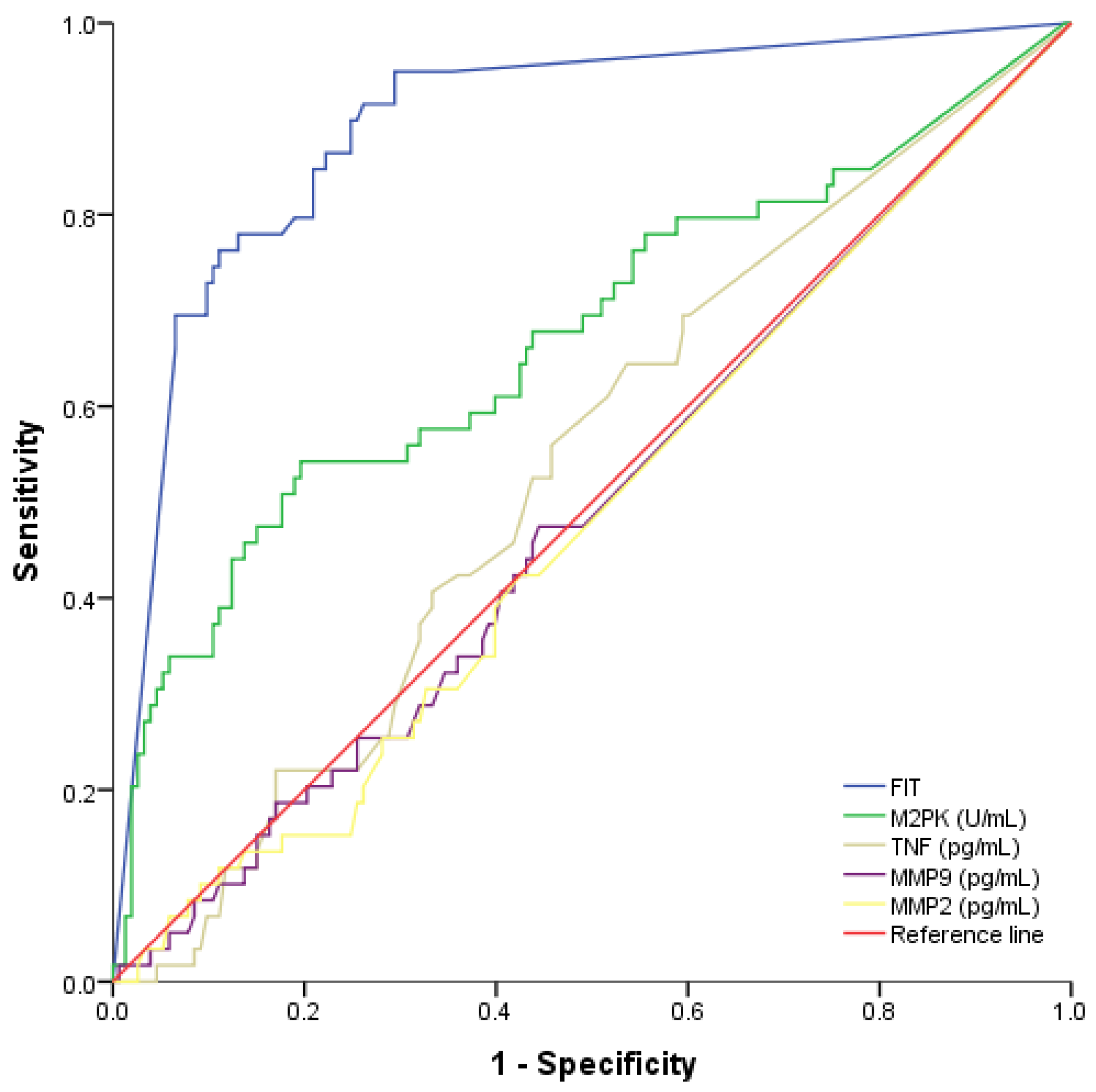
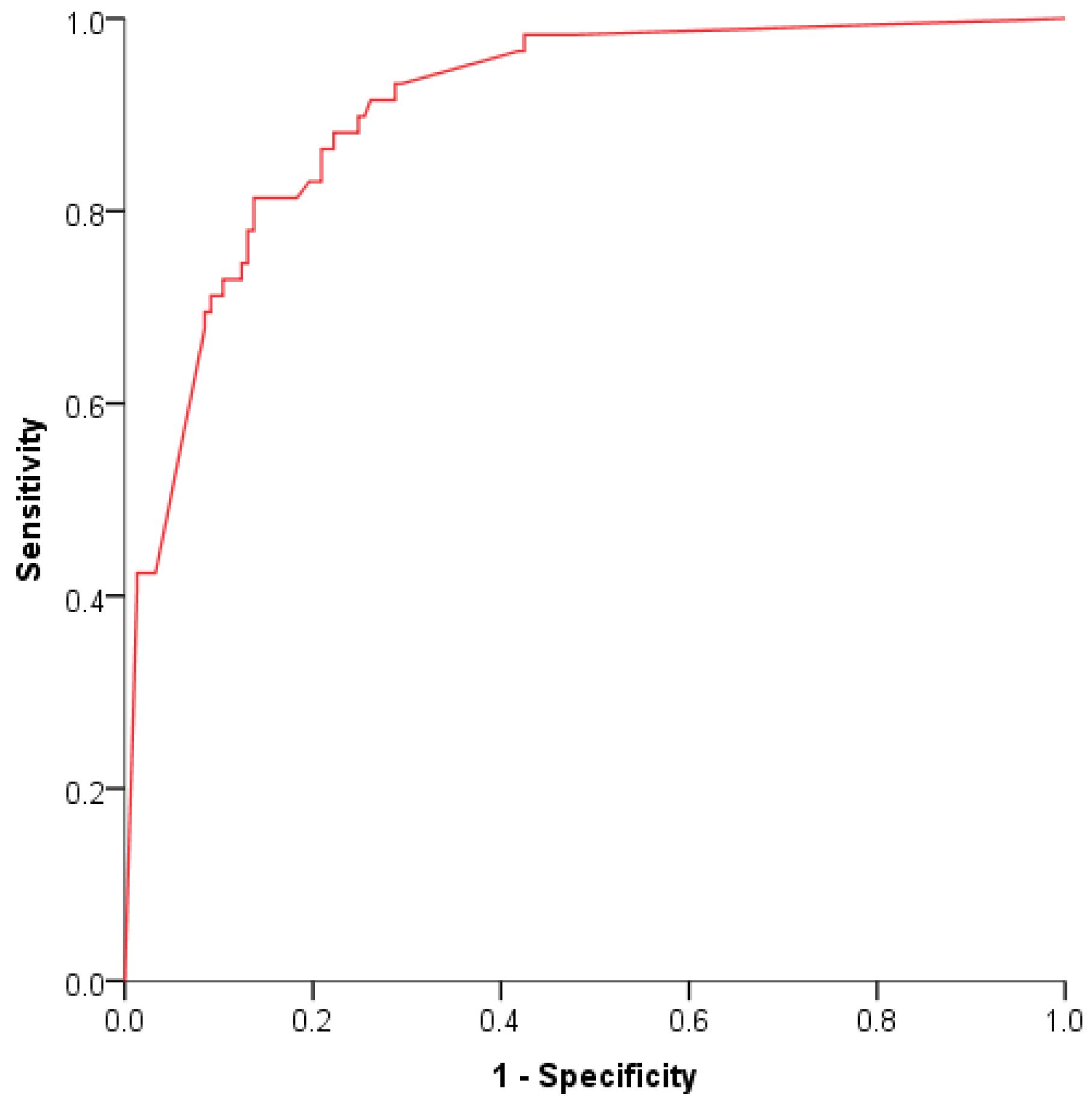
3.3. Determination of the Biomarkers Overall Performance for CRC Detection
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef]
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.; Piñeros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Douaiher, J.; Ravipati, A.; Grams, B.; Chowdhury, S.; Alatise, O.; Are, C. Colorectal cancer—Global burden, trends, and geographical variations. J. Surg. Oncol. 2017, 115, 619–630. [Google Scholar] [CrossRef]
- Loktionov, A. Biomarkers for detecting colorectal cancer non-invasively: DNA, RNA or proteins? World J. Gastrointest. Oncol. 2020, 12, 124–148. [Google Scholar] [CrossRef] [PubMed]
- Martins, B.A.A.; de Bulhões, G.F.; Cavalcanti, I.N.; Martins, M.M.; de Oliveira, P.G.; Martins, A.M.A. Biomarkers in Colorectal Cancer: The Role of Translational Proteomics Research. Front. Oncol. 2019, 9, 3389. [Google Scholar] [CrossRef]
- Zauber, A.G.; Winawer, S.J.; O’Brien, M.J.; Lansdorp-Vogelaar, I.; van Ballegooijen, M.D.; Hankey, B.F.; Weiji Shi, M.S.; Bond, J.H.; Schapiro, M.; Panish, J.F.; et al. Colonoscopy Polypectomy and Long-Term Prevention of Colorectal-Cancer Deaths. N. Engl. J. Med. 2012, 366, 687–696. [Google Scholar] [CrossRef]
- Rigi, F.; Jannatabad, A.; Izanloo, A.; Roshanravan, R.; Hashemian, H.R.; Kerachian, M.A. Expression of tumor pyruvate kinase M2 isoform in plasma and stool of patients with colorectal cancer or adenomatous polyps. BMC Gastroenterol. 2020, 20, 1–7. [Google Scholar] [CrossRef]
- Rutka, M.; Bor, R.; Balint, A.; Fábián, A.; Milassin, A.; Nagy, F.; Szepes, Z.; Szűcs, M.; Tiszlavicz, L.; Farkas, K.; et al. Diagnostic accuracy of five different fecal markers for the detection of precancerous and cancerous lesions of the colorectum. Mediat. Inflamm. 2016, 2016, 1–6. [Google Scholar] [CrossRef]
- Oh, H.-H.; Joo, Y.-E. Novel biomarkers for the diagnosis and prognosis of colorectal cancer. Intest. Res. 2020, 18, 168–183. [Google Scholar] [CrossRef]
- Kuipers, E.J.; Rösch, T.; Bretthauer, M. Colorectal cancer screening—Optimizing current strategies and new directions. Nat. Rev. Clin. Oncol. 2013, 10, 130–142. [Google Scholar] [CrossRef]
- Zou, H.; Harrington, J.J.; Klatt, K.K.; Ahlquist, D.A. A sensitive method to quantify human long DNA in stool: Relevance to colorectal cancer screening. Cancer Epidemiol. Biomark. Prev. 2006, 15, 1115–1119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilschut, J.; Habbema, J.D.F.; Van Leerdam, M.E.; Hol, L.; Lansdorp-Vogelaar, I.; Kuipers, E.J.; Van Ballegooijen, M. Fecal occult blood testing when colonoscopy capacity is limited. J. Natl. Cancer Inst. 2011, 103, 1741–1751. [Google Scholar] [CrossRef] [PubMed]
- Caviglia, G.P.; Cabianca, L.; Fagoonee, S.; Gili, F.M. Colorectal cancer detection in an asymptomatic population: Fecal immunochemical test for hemoglobin vs. Fecal M2-type pyruvate kinase. Biochem. Med. 2016, 26, 114–120. [Google Scholar] [CrossRef]
- de Wit, M.; Fijneman, R.J.; Verheul, H.M.; Meijer, G.A.; Jimenez, C.R. Proteomics in colorectal cancer translational research: Biomarker discovery for clinical applications. Clin. Biochem. 2013, 46, 466–479. [Google Scholar] [CrossRef]
- Coghlin, C.; Murray, G.I. Biomarkers of colorectal cancer: Recent advances and future challenges. Proteom. Clin. Appl. 2015, 9, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, A.J.; Colburn, W.A.; DeGruttola, V.G.; DeMets, D.L.; Downing, G.J.; Hoth, D.F.; Zeger, S.L. Biomarkers and surrogate endpoints: Preferred definitions and conceptual framework. Clin. Pharmacol. Ther. 2001, 69, 89–95. [Google Scholar] [CrossRef]
- Nikolouzakis, T.K.; Vassilopoulou, L.; Fragkiadaki, P.; Sapsakos, T.M.; Papadakis, G.Z.; Spandidos, D.; Tsatsakis, A.; Tsiaoussis, J. Improving diagnosis, prognosis and prediction by using biomarkers in CRC patients (Review). Oncol. Rep. 2018, 39, 2455–2472. [Google Scholar] [CrossRef] [Green Version]
- Al-Sindi, K.; Bukhari, M.; Al-Hamar, M. Role of a noninvasive stool-based molecular test in screening and early detection of colorectal cancers. Acta Med. Int. 2019, 6, 82. [Google Scholar] [CrossRef]
- Uppara, M.; Adaba, F.; Askari, A.; Clark, S.; Hanna, G.; Athanasiou, T.; Faiz, O. A systematic review and meta-analysis of the diagnostic accuracy of pyruvate kinase M2 isoenzymatic assay in diagnosing colorectal cancer. World J. Surg. Oncol. 2015, 13, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Mazurek, S. Pyruvate kinase type M2: A key regulator of the metabolic budget system in tumor cells. Int. J. Biochem. Cell Biol. 2011, 43, 969–980. [Google Scholar] [CrossRef]
- Huang, H. Matrix metalloproteinase-9 (MMP-9) as a cancer biomarker and MMP-9 biosensors: Recent advances. Sensors 2018, 18, 3249. [Google Scholar] [CrossRef] [Green Version]
- Said, A.H.; Raufman, J.P.; Xie, G. The role of matrix metalloproteinases in colorectal cancer. Cancers 2014, 6, 366–375. [Google Scholar] [CrossRef]
- Annahazi, A.; Ábrahám, S.; Farkas, K.; Rosztóczy, A.; Inczefi, O.; Földesi, I.; Szűcs, M.; Rutka, M.; Théodorou, V.; Eutamene, H.; et al. A pilot study on faecal MMP-9: A new noninvasive diagnostic marker of colorectal cancer. Br. J. Cancer 2016, 114, 787–792. [Google Scholar] [CrossRef] [Green Version]
- Mei, Z.; Liu, Y.; Liu, C.; Cui, A.; Liang, Z.; Wang, G.; Peng, H.; Cui, L.; Li, C. Tumour-infiltrating inflammation and prognosis in colorectal cancer: Systematic review and meta-analysis. Br. J. Cancer 2014, 110, 1595–1605. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Ye, Y.; Zhang, H.; Szmitkowski, M.; Mäkinen, M.; Li, P.; Xia, D.; Yang, J.; Wu, Y.; Wu, H. Diagnostic and prognostic value of serum interleukin-6 in colorectal cancer. Medicine 2016, 95, 1–10. [Google Scholar] [CrossRef]
- Stanilov, N.; Miteva, L.; Dobreva, Z.; Stanilova, S. Colorectal cancer severity and survival in correlation with tumour necrosis factor-alpha. Biotechnol. Biotechnol. Equip. 2014, 28, 911–917. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.; Zucknick, M.; London, R.; Kacevska, M.; Liddle, C.; Clarke, S.J. Systemic inflammatory response predicts prognosis in patients with advanced-stage colorectal cancer. Clin. Color. Cancer 2008, 7, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Olsen, J.; Kirkeby, L.T.; Olsen, J.; Eiholm, S.; Jess, P.; Gögenur, I.; Troelsen, J.T. High interleukin-6 mRNA expression is a predictor of relapse in colon cancer. Anticancer Res. 2015, 35, 2235–2240. [Google Scholar]
- Schultheiss, O.C.; Stanton, S.J. Assessment of Salivary Hormones. In Methods in Social Neuroscience; Harmon-Jones, E., Beer, J.S., Eds.; Guilford Press: New York, NY, USA, 2009; pp. 17–44. [Google Scholar]
- Baker, E.A.; Leaper, D.J. Measuring gelatinase activity in colorectal cancer. Eur. J. Surg. Oncol. 2002, 28, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.C.; Menges, M.; Orzechowski, H.-D.; Orendain, N.; Pistorius, G.; Feifel, G.; Zeitz, M.; Stallmach, A. Increased matrix metalloproteinase 2 concentration and transcript expression in advanced colorectal carcinomas. Int. J. Color. Dis. 2001, 16, 133–140. [Google Scholar] [CrossRef]
- Liabakk, N.B.; Talbot, I.; A Smith, R.; Wilkinson, K.; Balkwill, F. Matrix metalloprotease 2 (MMP-2) and matrix metalloprotease 9 (MMP-9) type IV collagenases in colorectal cancer. Cancer Res. 1996, 56, 190–196. [Google Scholar]
- Araújo, R.F.; Lira, G.; Vilaça, J.; Guedes, H.; Leitão, M.; Lucena, H.; Ramos, C. Prognostic and diagnostic implications of MMP-2, MMP-9, and VEGF-α expressions in colorectal cancer. Pathol. Res. Pr. 2015, 211, 71–77. [Google Scholar] [CrossRef]
- Yang, B.; Tang, F.; Zhang, B.; Zhao, Y.; Feng, J.; Rao, Z. Matrix metalloproteinase-9 overexpression is closely related to poor prognosis in patients with colon cancer. World J. Surg. Oncol. 2014, 12, 12–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dragutinović, V.V.; Radonjic, N.; Petronijević, N.D.; Tatić, S.B.; Dimitrijević, I.B.; Radovanović, N.S.; Krivokapić, Z.V. Matrix metalloproteinase-2 (MMP-2) and -9 (MMP-9) in preoperative serum as independent prognostic markers in patients with colorectal cancer. Mol. Cell. Biochem. 2011, 355, 173–178. [Google Scholar] [CrossRef]
- Sithambaram, S.; Hilmi, I.; Goh, K.L. The diagnostic accuracy of the M2 pyruvate kinase Quick stool test-A rapid office based assay test for the detection of colorectal cancer. PLoS ONE 2015, 10, 1371. [Google Scholar] [CrossRef] [PubMed]
- Koss, K.; Maxton, D.; Jankowski, J.A.Z. Faecal dimeric M2 pyruvate kinase in colorectal cancer and polyps correlates with tumour staging and surgical intervention. Color Dis. 2008, 10, 244–248. [Google Scholar] [CrossRef] [PubMed]
- Gies, A.; Bhardwaj, M.; Stock, C.; Schrotz-King, P.; Brenner, H. Quantitative fecal immunochemical tests for colorectal cancer screening. Int. J. Cancer 2018, 143, 234–244. [Google Scholar] [CrossRef] [Green Version]
- Fraser, C.G.; Allison, J.E.; Halloran, S.P.; Young, G.P. A proposal to standardize reporting units for fecal immunochemical tests for hemoglobin. J. Natl. Cancer Inst. 2012, 104, 810–814. [Google Scholar] [CrossRef] [Green Version]
- Habibzadeh, F.; Habibzadeh, P.; Yadollahie, M. On determining the most appropriate test cut-off value: The case of tests with continuous results. Biochem. Med. 2016, 26, 297–307. [Google Scholar] [CrossRef]
- Youden, W. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Parikh, C.R.; Thiessen-Philbrook, H. Key concepts and limitations of statistical methods for evaluating biomarkers of kidney disease. J. Am. Soc. Nephrol. 2014, 25, 1621–1629. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, T.; Fang, Y.; Rong, A.; Wang, J. Flexible combination of multiple diagnostic biomarkers to improve diagnostic accuracy Data analysis, statistics and modelling. BMC Med. Res. Methodol. 2015, 15, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leen, R.; Seng-Lee, C.; Holleran, G.; O’Morain, C.; McNamara, D. Comparison of faecal M2-PK and FIT in a population-based bowel cancer screening cohort. Eur. J. Gastroenterol. Hepatol. 2014, 26, 514–518. [Google Scholar] [CrossRef] [PubMed]
- Cubiella, J.; Salve, M.; Díaz-Ondina, M.; Vega, P.; Alves, M.T.; Iglesias, F.; Sánchez, E.; Macía, P.; Blanco, I.; Bujanda, L.; et al. Diagnostic accuracy of the faecal immunochemical test for colorectal cancer in symptomatic patients: Comparison with NICE and SIGN referral criteria. Color. Dis. 2014, 16, O273–O282. [Google Scholar] [CrossRef]
- Niedermaier, T.; Balavarca, Y.; Brenner, H. Stage-Specific Sensitivity of Fecal Immunochemical Tests for Detecting Colorectal Cancer: Systematic Review and Meta-Analysis. Am. J. Gastroenterol. 2020, 115, 56. [Google Scholar] [CrossRef] [Green Version]
- Pin-Vieito, N.; Tejido-Sandoval, C.; de Vicente-Bielza, N.; Sánchez-Gómez, C.; Cubiella, J. Faecal immunochemical tests safely enhance rational use of resources during the assessment of suspected symptomatic colorectal cancer in primary care: Systematic review and meta-analysis. Gut 2021, 0, 1–11. [Google Scholar]
- Lin, J.S.; Piper, M.A.; Perdue, L.A.; Rutter, C.M.; Webber, E.M.; O’Connor, E.; Smith, N.; Whitlock, E.P. Screening for Colorectal Cancer: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2016, 315, 2576–2594. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Group Description | Cancer (CRC) | Advanced Adenoma | Other Lesions | Controls | |
|---|---|---|---|---|---|
| Patient Number | 60 | 47 | 49 | 60 | |
| Mean Age, Range (years) | 69, (40–88) | 71, (47–86) | 65, (17–86) | 64, (37–87) | |
| Gender, n (%) | Female | 23 (38%) | 18 (38%) | 20 (41%) | 38 (63%) |
| Male | 37 (62%) | 29 (62%) | 29 (59%) | 22 (37%) | |
| Groups | Hb (ng/mL) | M2-PK (U/mL) | TNF (pg/mL) | MMP-9 (pg/mL) | MMP-2 (pg/mL) | |
|---|---|---|---|---|---|---|
| CRC | Number | 60.00 | 60.00 | 60.00 | 60.00 | 60.00 |
| Mean | 748.56 | 20.21 | 4.42 | 3.44 | 14.63 | |
| Median | 1000.00 | 8.66 | 3.78 | 0.00 | 0.00 | |
| SD | 388.86 | 31.25 | 4.53 | 7.11 | 23.36 | |
| Advanced Adenoma | Number | 47.00 | 47.00 | 47.00 | 47.00 | 47.00 |
| Mean | 247.72 | 5.14 | 5.31 | 3.34 | 10.19 | |
| Median | 58.50 | 1.46 | 1.86 | 0.33 | 0.00 | |
| SD | 353.99 | 7.26 | 7.57 | 4.85 | 21.82 | |
| Other lesions | Number | 49.00 | 49.00 | 49.00 | 49.00 | 49.00 |
| Mean | 127.67 | 12.42 | 4.24 | 5.66 | 16.59 | |
| Median | 19.00 | 2.86 | 3.40 | 0.00 | 0.00 | |
| SD | 247.563 | 33.20 | 4.89 | 12.89 | 24.95 | |
| Controls | Number | 60.00 | 60.00 | 60.00 | 60.00 | 60.00 |
| Mean | 59.35 | 3.56 | 4.93 | 3.40 | 21.58 | |
| Median | 19.00 | 1.68 | 2.63 | 1.00 | 10.25 | |
| SD | 171.44 | 4.44 | 7.66 | 4.81 | 27.64 | |
| Total | Number | 214.00 | 214.00 | 216.00 | 216.00 | 216.00 |
| Mean | 305.50 | 10.56 | 4.71 | 3.83 | 16.04 | |
| Median | 23.50 | 2.78 | 2.63 | 0.00 | 0.00 | |
| SD | 411.14 | 24.03 | 6.29 | 7.96 | 24.84 | |
| Biomarkers Parameters | Sensitivity (%) | Specificity (%) | LR *+ | LR− | Odds Ratio |
|---|---|---|---|---|---|
| Hb ≥ 10 µg/g | 91.5 (80.6–96.8) | 72.3 (64.4–79.0) | 3.3 (2.5–4.3) | 0.1 (0.05–0.3) | 28.1 (10.5–75.0) |
| M2-PK ≥ 8 U/mL | 55.0 (41.7–67.7) | 72.4 (65.8–78.2) | 2.6 (1.8–3.9) | 0.6 (0.4–0.8) | 4.7 (5.4–8.8) |
| Hb ≥ 10 µg/g and M2-PK ≥ 8 U/mL | 49.1 (36.0–62.4) | 93.5 (88.0–96.6) | 7.5 (3.9–14.4) | 0.5 (0.4–0.7) | 13.8 (6.1–31.4) |
| Hb ≥ 10 µg/g or M2-PK ≥ 8 U/mL | 96.6 (87.2–99.4) | 58.2 (49.9–66.0) | 2.3 (1.9–2.8) | 0.06 (0.01–0.2) | 39.6 (9.3–168.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cruz, A.; Carvalho, C.M.; Cunha, A.; Crespo, A.; Iglesias, Á.; García-Nimo, L.; Freitas, P.P.; Cubiella, J. Faecal Diagnostic Biomarkers for Colorectal Cancer. Cancers 2021, 13, 5568. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13215568
Cruz A, Carvalho CM, Cunha A, Crespo A, Iglesias Á, García-Nimo L, Freitas PP, Cubiella J. Faecal Diagnostic Biomarkers for Colorectal Cancer. Cancers. 2021; 13(21):5568. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13215568
Chicago/Turabian StyleCruz, Andrea, Carla M. Carvalho, Alexandra Cunha, Anais Crespo, Águeda Iglesias, Laura García-Nimo, Paulo P. Freitas, and Joaquín Cubiella. 2021. "Faecal Diagnostic Biomarkers for Colorectal Cancer" Cancers 13, no. 21: 5568. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13215568