
Somatostatin Receptors in Human Meningiomas—Clinicopathological Aspects

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Immunohistochemistry
2.3. Manual Scoring of Immunohistochemistry
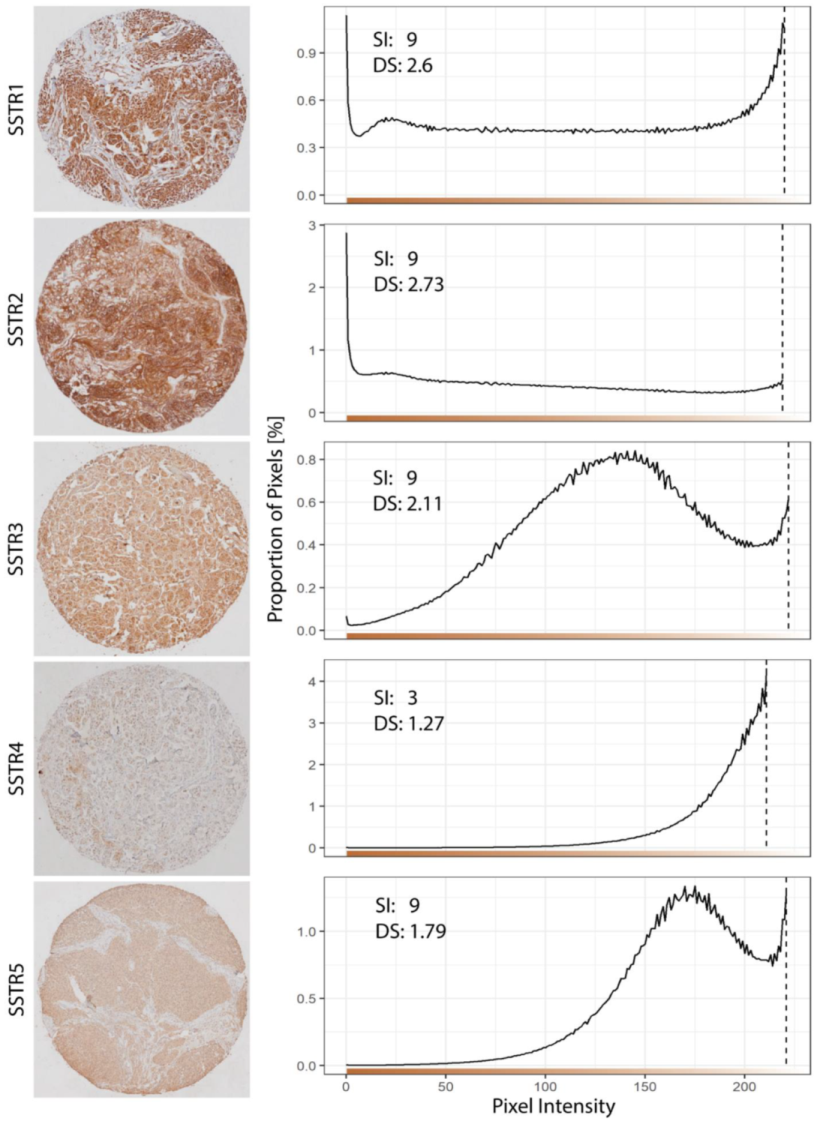
2.4. Image Acquisition and Digital Evaluation of SSTRs Expression
2.5. Statistical Analysis
3. Results
3.1. Patients
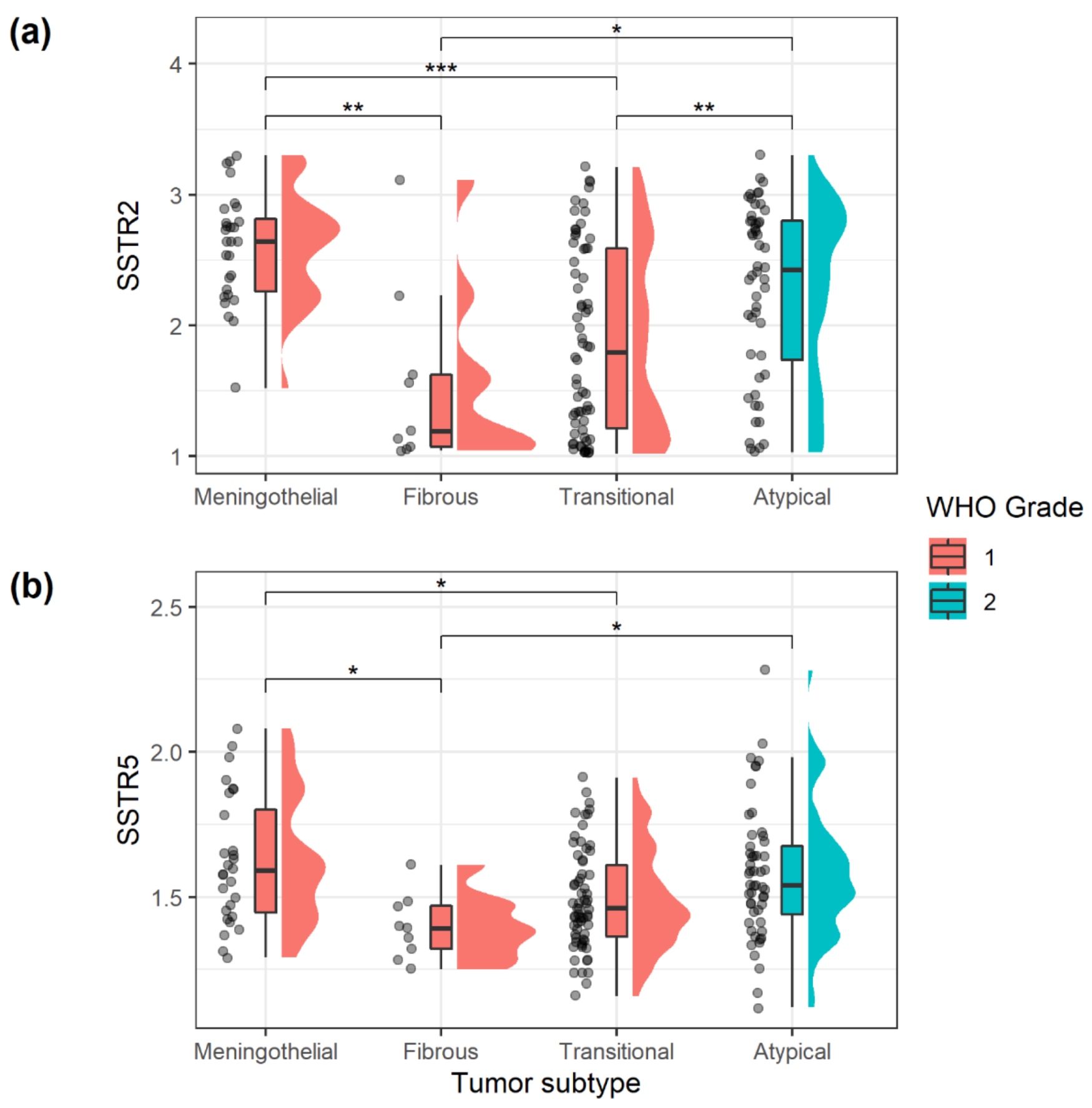
3.2. Immunohistochemical Expression of SSTRs in Meningiomas
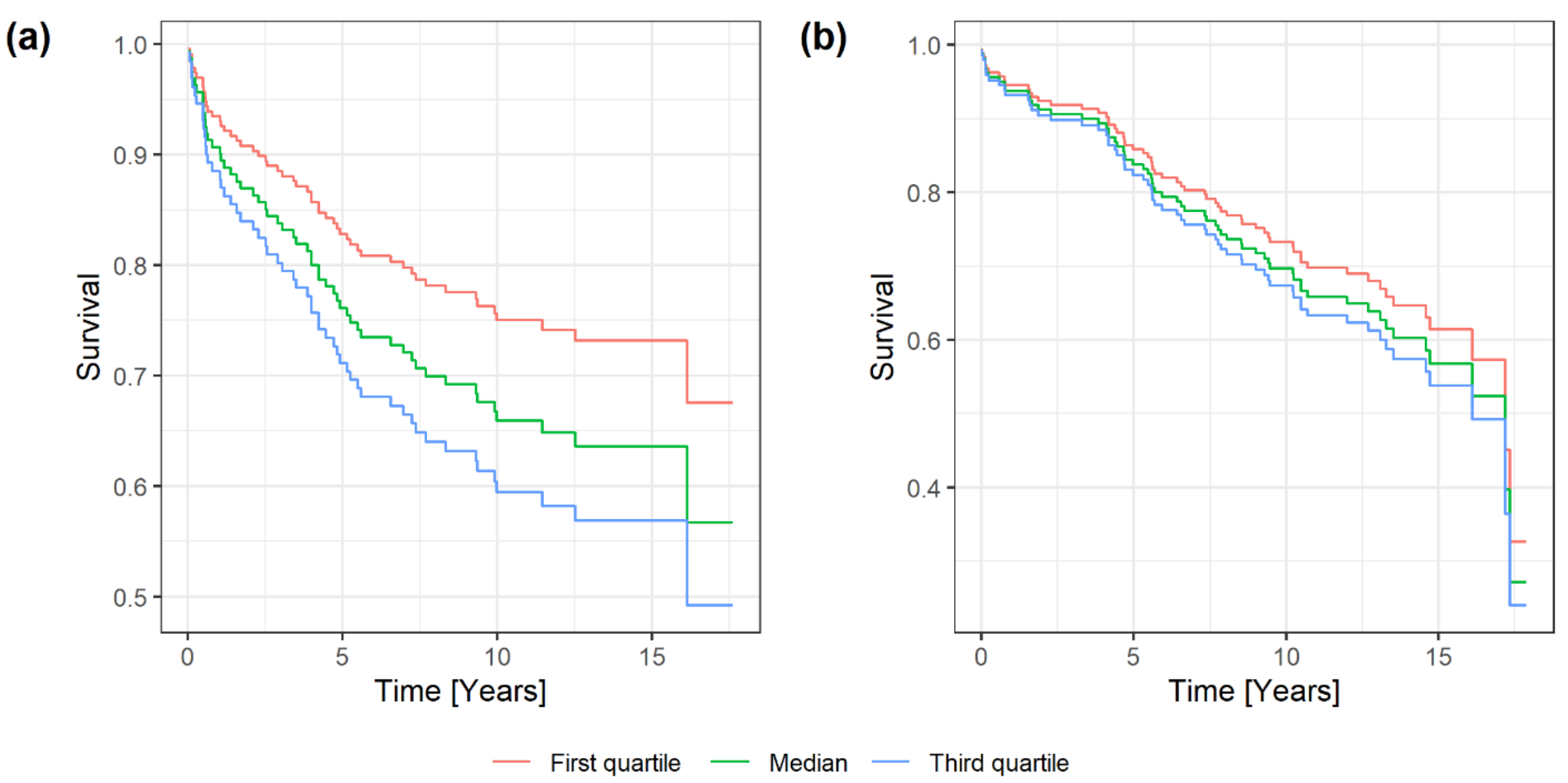
3.3. SSTRs and Prognosis in Meningiomas
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ostrom, Q.T.; Patil, N.; Cioffi, G.; Waite, K.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2013–2017. Neuro-Oncol. 2020, 22, iv1–iv96. [Google Scholar] [CrossRef] [PubMed]
- Harter, P.N.; Braun, Y.; Plate, K.H. Classification of Meningiomas-Advances and Controversies. Chin. Clin. Oncol. 2017, 6, S2. [Google Scholar] [CrossRef]
- Jääskeläinen, J. Seemingly Complete Removal of Histologically Benign Intracranial Meningioma: Late Recurrence Rate and Factors Predicting Recurrence in 657 Patients. A Multivariate Analysis. Surg. Neurol. 1986, 26, 461–469. [Google Scholar] [CrossRef]
- Zhao, L.; Zhao, W.; Hou, Y.; Wen, C.; Wang, J.; Wu, P.; Guo, Z. An Overview of Managements in Meningiomas. Front. Oncol. 2020, 10, 1523. [Google Scholar] [CrossRef]
- Brastianos, P.K.; Galanis, E.; Butowski, N.; Chan, J.W.; Dunn, I.F.; Goldbrunner, R.; Herold-Mende, C.; Ippen, F.M.; Mawrin, C.; McDermott, M.W.; et al. Advances in Multidisciplinary Therapy for Meningiomas. Neuro. Oncol. 2019, 21, i18–i31. [Google Scholar] [CrossRef] [Green Version]
- Lacy, J.; Saadati, H.; Yu, J.B. Complications of Brain Tumors and Their Treatment. Hematol. Oncol. Clin. N. Am. 2012, 26, 779–796. [Google Scholar] [CrossRef]
- Rogers, C.L.; Perry, A.; Pugh, S.; Vogelbaum, M.A.; Brachman, D.; McMillan, W.; Jenrette, J.; Barani, I.; Shrieve, D.; Sloan, A.; et al. Pathology Concordance Levels for Meningioma Classification and Grading in NRG Oncology RTOG Trial 0539. Neuro. Oncol. 2016, 18, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Reubi, J.C.; Kappeler, A.; Waser, B.; Laissue, J.; Hipkin, R.W.; Schonbrunn, A. Immunohistochemical Localization of Somatostatin Receptors Sst2A in Human Tumors. Am. J. Pathol. 1998, 153, 233–245. [Google Scholar] [CrossRef] [Green Version]
- Schulz, S.; Pauli, S.U.; Schulz, S.; Händel, M.; Dietzmann, K.; Firsching, R.; Höllt, V. Immunohistochemical Determination of Five Somatostatin Receptors in Meningioma Reveals Frequent Overexpression of Somatostatin Receptor Subtype Sst2A. Clin. Cancer Res. 2000, 6, 1865–1874. [Google Scholar]
- de Oliveira Silva, C.B.; Ongaratti, B.R.; Trott, G.; Haag, T.; Ferreira, N.P.; Leães, C.G.S.; Pereira-Lima, J.F.S.; da Costa Oliveira, M. Expression of Somatostatin Receptors (SSTR1-SSTR5) in Meningiomas and Its Clinicopathological Significance. Int. J. Clin. Exp. Pathol. 2015, 8, 13185–13192. [Google Scholar]
- Susini, C.; Buscail, L. Rationale for the Use of Somatostatin Analogs as Antitumor Agents. Ann. Oncol. 2006, 17, 1733–1742. [Google Scholar] [CrossRef]
- Barbieri, F.; Pattarozzi, A.; Gatti, M.; Porcile, C.; Bajetto, A.; Ferrari, A.; Culler, M.D.; Florio, T. Somatostatin Receptors 1, 2, and 5 Cooperate in the Somatostatin Inhibition of C6 Glioma Cell Proliferation in Vitro via a Phosphotyrosine Phosphatase-Eta-Dependent Inhibition of Extracellularly Regulated Kinase-1/2. Endocrinology 2008, 149, 4736–4746. [Google Scholar] [CrossRef] [Green Version]
- Theodoropoulou, M.; Stalla, G.K. Somatostatin Receptors: From Signaling to Clinical Practice. Front. Neuroendocrinol. 2013, 34, 228–252. [Google Scholar] [CrossRef]
- Graillon, T.; Romano, D.; Defilles, C.; Saveanu, A.; Mohamed, A.; Figarella-Branger, D.; Roche, P.-H.; Fuentes, S.; Chinot, O.; Dufour, H.; et al. Octreotide Therapy in Meningiomas: In Vitro Study, Clinical Correlation, and Literature Review. J. Neurosurg. 2017, 127, 660–669. [Google Scholar] [CrossRef]
- Hrachova, M.; Nguyen, E.N.T.; Fu, B.D.; Dandekar, M.J.; Kong, X.-T.; Cadena, G.; Hsu, F.P.K.; Billimek, J.; Taylor, T.H.; Bota, D.A. A Retrospective Interventional Cohort Study to Assess the Safety and Efficacy of Sandostatin LAR for Treatment of Recurrent and/or Refractory Meningiomas. Front. Neurol. 2020, 11, 373. [Google Scholar] [CrossRef]
- Mawrin, C.; Schulz, S.; Hellwig-Patyk, A.; Kirches, E.; Roessner, A.; Lendeckel, U.; Firsching, R.; Vorwerk, C.K.; Keilhoff, G.; Dietzmann, K.; et al. Expression and Function of Somatostatin Receptors in Peripheral Nerve Sheath Tumors. J. Neuropathol. Exp. Neurol. 2005, 64, 1080–1088. [Google Scholar] [CrossRef] [Green Version]
- Menke, J.R.; Raleigh, D.R.; Gown, A.M.; Thomas, S.; Perry, A.; Tihan, T. Somatostatin Receptor 2a Is a More Sensitive Diagnostic Marker of Meningioma than Epithelial Membrane Antigen. Acta Neuropathol. 2015, 130, 441–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arena, S.; Barbieri, F.; Thellung, S.; Pirani, P.; Corsaro, A.; Villa, V.; Dadati, P.; Dorcaratto, A.; Lapertosa, G.; Ravetti, J.-L.; et al. Expression of Somatostatin Receptor MRNA in Human Meningiomas and Their Implication in in Vitro Antiproliferative Activity. J. Neurooncol. 2004, 66, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Dutour, A.; Kumar, U.; Panetta, R.; Ouafik, L.; Fina, F.; Sasi, R.; Patel, Y.C. Expression of Somatostatin Receptor Subtypes in Human Brain Tumors. Int. J. Cancer 1998, 76, 620–627. [Google Scholar] [CrossRef]
- Durand, A.; Champier, J.; Jouvet, A.; Labrousse, F.; Honnorat, J.; Guyotat, J.; Fèvre-Montange, M. Expression of C-Myc, Neurofibromatosis Type 2, Somatostatin Receptor 2 and Erb-B2 in Human Meningiomas: Relation to Grades or Histotypes. Clin. Neuropathol. 2008, 27, 334–345. [Google Scholar] [CrossRef]
- Barresi, V.; Alafaci, C.; Salpietro, F.; Tuccari, G. Sstr2A Immunohistochemical Expression in Human Meningiomas: Is There a Correlation with the Histological Grade, Proliferation or Microvessel Density? Oncol. Rep. 2008, 20, 485–492. [Google Scholar] [CrossRef]
- Hamilton, P.W.; Bankhead, P.; Wang, Y.; Hutchinson, R.; Kieran, D.; McArt, D.G.; James, J.; Salto-Tellez, M. Digital Pathology and Image Analysis in Tissue Biomarker Research. Methods 2014, 70, 59–73. [Google Scholar] [CrossRef]
- Backer-Grøndahl, T.; Moen, B.H.; Sundstrøm, S.H.; Torp, S.H. Histopathology and Prognosis in Human Meningiomas. APMIS 2014, 122, 856–866. [Google Scholar] [CrossRef] [PubMed]
- Backer-Grøndahl, T.; Moen, B.H.; Torp, S.H. The Histopathological Spectrum of Human Meningiomas. Int. J. Clin. Exp. Pathol 2012, 5, 231–242. [Google Scholar]
- Arnli, M.B.; Winther, T.L.; Lydersen, S.; Torp, S.H. Prognostic Value of ErbB2/HER2 in Human Meningiomas. PLoS ONE 2018, 13, e0205846. [Google Scholar] [CrossRef] [PubMed]
- Perry, A.; Louis, D.N.; Budka, H.; von Deimling, A.; Sahm, F.; Rushing, E.J.; Mawrin, C.; Claus, E.B.; Loeffler, J.; Sadetzki, S. Meningiomas. In WHO Classification of Tumours of the Central Nervous System; IARC: Lyon, France, 2016; pp. 231–245. [Google Scholar]
- Torp, S.H.; Gulati, S.; Johannessen, E.; Dalen, A. Coexpression of C-ErbB 1-4 Receptor Proteins in Human Glioblastomas. An Immunohistochemical Study. J. Exp. Clin. Cancer Res. 2007, 26, 353–359. [Google Scholar]
- Varghese, F.; Bukhari, A.B.; Malhotra, R.; De, A. IHC Profiler: An Open Source Plugin for the Quantitative Evaluation and Automated Scoring of Immunohistochemistry Images of Human Tissue Samples. PLoS ONE 2014, 9, e96801. [Google Scholar] [CrossRef] [Green Version]
- Haub, P.; Meckel, T. A Model Based Survey of Colour Deconvolution in Diagnostic Brightfield Microscopy: Error Estimation and Spectral Consideration. Sci. Rep. 2015, 5, 12096. [Google Scholar] [CrossRef]
- Punt, C.J.A.; Buyse, M.; Köhne, C.-H.; Hohenberger, P.; Labianca, R.; Schmoll, H.J.; Påhlman, L.; Sobrero, A.; Douillard, J.-Y. Endpoints in Adjuvant Treatment Trials: A Systematic Review of the Literature in Colon Cancer and Proposed Definitions for Future Trials. JNCI: J. Natl. Cancer Inst. 2007, 99, 998–1003. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Yang, W.; Deng, J.; Zhang, J.; Ma, F.; Wang, J. Correlation between 99mTc-HYNIC-Octreotide SPECT/CT Somatostatin Receptor Scintigraphy and Pathological Grading of Meningioma. J. Neurooncol. 2013, 113, 519–526. [Google Scholar] [CrossRef]
- Boulagnon-Rombi, C.; Fleury, C.; Fichel, C.; Lefour, S.; Marchal Bressenot, A.; Gauchotte, G. Immunohistochemical Approach to the Differential Diagnosis of Meningiomas and Their Mimics. J. Neuropathol. Exp. Neurol 2017, 76, 289–298. [Google Scholar] [CrossRef]
- Morichetti, D.; Mazzucchelli, R.; Santinelli, A.; Stramazzotti, D.; Lopez-Beltran, A.; Scarpelli, M.; Bono, A.V.; Cheng, L.; Montironi, R. Immunohistochemical Expression and Localization of Somatostatin Receptor Subtypes in Prostate Cancer with Neuroendocrine Differentiation. Int. J. Immunopathol. Pharm. 2010, 23, 511–522. [Google Scholar] [CrossRef] [Green Version]
- Abdel-Rahman, O.; Lamarca, A.; Valle, J.W.; Hubner, R.A. Somatostatin Receptor Expression in Hepatocellular Carcinoma: Prognostic and Therapeutic Considerations. Endocr. Relat. Cancer 2014, 21, R485–R493. [Google Scholar] [CrossRef] [Green Version]
- Goldbrunner, R.; Minniti, G.; Preusser, M.; Jenkinson, M.D.; Sallabanda, K.; Houdart, E.; von Deimling, A.; Stavrinou, P.; Lefranc, F.; Lund-Johansen, M.; et al. EANO Guidelines for the Diagnosis and Treatment of Meningiomas. Lancet Oncol. 2016, 17, e383–e391. [Google Scholar] [CrossRef] [Green Version]
- Appay, R.; Tabouret, E.; Touat, M.; Carpentier, C.; Colin, C.; Ducray, F.; Idbaih, A.; Mokhtari, K.; Uro-Coste, E.; Dehais, C.; et al. Somatostatin Receptor 2A Protein Expression Characterizes Anaplastic Oligodendrogliomas with Favorable Outcome. Acta Neuropathol. Commun. 2018, 6, 89. [Google Scholar] [CrossRef]
- Raggi, C.C.; Maggi, M.; Renzi, D.; Calabrò, A.; Bagnoni, M.L.; Scaruffi, P.; Tonini, G.P.; Pazzagli, M.; De Bernardi, B.; Bernini, G.; et al. Quantitative Determination of Sst2 Gene Expression in Neuroblastoma Tumor Predicts Patient Outcome. J. Clin. Endocrinol. Metab. 2000, 85, 3866–3873. [Google Scholar] [CrossRef]
- Okuwaki, K.; Kida, M.; Mikami, T.; Yamauchi, H.; Imaizumi, H.; Miyazawa, S.; Iwai, T.; Takezawa, M.; Saegusa, M.; Watanabe, M.; et al. Clinicopathologic Characteristics of Pancreatic Neuroendocrine Tumors and Relation of Somatostatin Receptor Type 2A to Outcomes. Cancer 2013, 119, 4094–4102. [Google Scholar] [CrossRef]
- Song, K.B.; Kim, S.C.; Kim, J.H.; Seo, D.-W.; Hong, S.-M.; Park, K.-M.; Hwang, D.W.; Lee, J.H.; Lee, Y.-J. Prognostic Value of Somatostatin Receptor Subtypes in Pancreatic Neuroendocrine Tumors. Pancreas 2016, 45, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Sharma, K.; Patel, Y.C.; Srikant, C.B. Subtype-Selective Induction of Wild-Type P53 and Apoptosis, but Not Cell Cycle Arrest, by Human Somatostatin Receptor 3. Mol. Endocrinol. 1996, 10, 1688–1696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortolá Buigues, A.; Crespo Hernández, I.; Jorquera Moya, M.; Díaz Pérez, J.Á. Unresectable Recurrent Multiple Meningioma: A Case Report with Radiological Response to Somatostatin Analogues. Case Rep. Oncol. 2016, 9, 520–525. [Google Scholar] [CrossRef]
- García-Luna, P.P.; Relimpio, F.; Pumar, A.; Pereira, J.L.; Leal-Cerro, A.; Trujillo, F.; Cortés, A.; Astorga, R. Clinical Use of Octreotide in Unresectable Meningiomas. A Report of Three Cases. J. Neurosurg. Sci. 1993, 37, 237–241. [Google Scholar] [PubMed]
- Jaffrain-Rea, M.L.; Minniti, G.; Santoro, A.; Bastianello, S.; Tamburrano, G.; Gulino, A.; Cantore, G. Visual Improvement during Octreotide Therapy in a Case of Episellar Meningioma. Clin. Neurol. Neurosurg. 1998, 100, 40–43. [Google Scholar] [CrossRef]
- Rammo, R.; Rock, A.; Transou, A.; Raghunathan, A.; Rock, J. Anaplastic Meningioma: Octreotide Therapy for a Case of Recurrent and Progressive Intracranial Disease. J. Neurosurg. 2016, 124, 496–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schreglmann, S.R.; Jelčić, I.; Taegtmeyer, A.B.; Linnebank, M.; Weller, M. Multifocal CNS Demyelination after Octreotide Treatment for Metastatic Meningioma. Clin. Neurol. Neurosurg. 2013, 115, 817–819. [Google Scholar] [CrossRef] [Green Version]
- Norden, A.D. Phase II Study of Monthly Pasireotide LAR (SOM230C) for Recurrent or Progressive Meningioma. Neurology 2015, 84, 280–286. [Google Scholar] [CrossRef] [Green Version]
- Collamati, F.; Pepe, A.; Bellini, F.; Bocci, V.; Chiodi, G.; Cremonesi, M.; De Lucia, E.; Ferrari, M.E.; Frallicciardi, P.M.; Grana, C.M.; et al. Toward Radioguided Surgery with β- Decays: Uptake of a Somatostatin Analogue, DOTATOC, in Meningioma and High-Grade Glioma. J. Nucl. Med. 2015, 56, 3–8. [Google Scholar] [CrossRef] [Green Version]
- Rachinger, W.; Stoecklein, V.M.; Terpolilli, N.A.; Haug, A.R.; Ertl, L.; Pöschl, J.; Schüller, U.; Schichor, C.; Thon, N.; Tonn, J.-C. Increased 68Ga-DOTATATE Uptake in PET Imaging Discriminates Meningioma and Tumor-Free Tissue. J. Nucl. Med. 2015, 56, 347–353. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SSTR1 | Anti-SSTR1 (polyclonal IgG (rabbit), pH 6, 1:200 dilution, overnight incubation, somatostatin receptor 1, cat#HPA031506, Atlas Antibodies) |
| SSTR2 | Anti-Somatostatin Receptor 2 antibody (UMB1)—C-terminal (monoclonal (rabbit), pH 6, 1:100 dilution, overnight incubation, somatostatin receptor 2, cat#ab134152, Abcam) |
| SSTR3 | Somatostatin R3/SSTR3 Antibody (polyclonal (rabbit), pH6, 1:1000 dilution, overnight incubation, somatostatin receptor 3, cat#NB100-74538, Novus Biologicals) |
| SSTR4 | Anti-SSTR4 (polyclonal IgG (rabbit), pH 6, 1:25 dilution, overnight incubation, somatostatin receptor 4, cat#HPA064252, Atlas Antibodies) |
| SSTR5 | SSTR5: Anti-Somatostatin Receptor Type 5 Antibody (polyclonal (rabbit), pH 6, 1:100 dilution, overnight incubation, somatostatin receptor 5, cat#ab9287, Chemicon) |
| Patient Data | WHO Grade 1 | WHO Grade 2 | All Grades |
|---|---|---|---|
| Total number, n | 109 | 53 | 162 |
| Median age at operation (range), years | 58 (27–84) | 65 (25–86) | 60 (25–86) |
| Sex (female/male), n | 84/25 | 35/18 | 119/43 |
| WHO Performance Status (0–5), n | 15/73/20/1/0/0 | 5/39/7/1/1/0 | 20/112/27/2/1/0 |
| Simpson grade (I–V), n | 30/47/13/19/0 | 11/26/9/7/0 | 41/73/22/26/0 |
| Recurrence (yes/no), n | 23/86 | 18/35 | 41/121 |
| SSTR | Digital Scoring | Staining Index | ||
|---|---|---|---|---|
| Mean (SD) | Median (Min.–Max.) | Mean (SD) | Median (Min.–Max.) | |
| SSTR1 | 2.71 (0.43) | 2.72 (1.33–3.55) | 8.30 (1.41) | 9 (2–9) |
| SSTR2 | 2.13 (0.71) | 2.24 (1.02–3.30) | 7.91 (2.02) | 9 (2–9) |
| SSTR3 | 2.08 (0.23) | 2.09 (1.58–2.62) | 6.73 (1.83) | 6 (3–9) |
| SSTR4 | 1.17 (0.10) | 1.14 (1.04–1.65) | 1.35 (1.65) | 0 (0.00–6) |
| SSTR5 | 1.54 (0.21) | 1.51 (1.12–2.28) | 5.44 (1.81) | 6 (3–9) |
| Categorical Variables | n | SSTR1 | SSTR2 | SSTR3 | SSTR4 | SSTR5 | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mann–Whitney U | 161 | Median (Range) | p-Value | Median (Range) | p-Value | Median (Range) | p-Value | Median (Range) | p-Value | Median (Range) | p-Value |
| WHO Grade 1 | 109 | 2.70 (1.33–3.55) | 0.036 | 2.14 (1.02–3.30) | 0.009 | 2.05 (1.58–2.58) | 0.059 | 1.15 (1.04–1.65) | 0.166 | 1.48 (1.12–2.08) | 0.029 |
| WHO Grade 2 | 52 | 2.82 (2.05–3.55) | 2.52 (1.03–3.30) | 2.12 (1.62–2.62) | 1.12 (1.04–1.39) | 1.55 (1.17–2.28) | |||||
| Necrosis present | 37 | 2.76 (1.96–3.33) | 0.647 | 2.61 (1.03–3.11) | 0.010 | 2.12 (1.74–2.62) | 0.285 | 1.13 (1.04–1.42) | 0.368 | 1.54 (1.16–2.03) | 0.054 |
| Necrosis not seen | 124 | 2.71 (1.33–3.55) | 2.13 (1.02–3.30) | 2.07 (1.58–2.58) | 1.14 (1.04–1.65) | 1.48 (1.12–2.28) | |||||
| Hypercellularity | 42 | 2.68 (1.86–3.52) | 0.686 | 1.94 (1.02–3.30) | 0.208 | 2.10 (1.62–2.62) | 0.664 | 1.12 (1.04–1.26) | 0.016 | 1.50 (1.17–2.28) | 0.975 |
| Hypercellularity not seen | 119 | 2.72 (1.33–3.55) | 2.24 (1.03–3.30) | 2.08 (1.58–2.58) | 1.15 (1.04–1.65) | 1.51 (1.12–2.08) | |||||
| Sheeting present | 12 | 2.56 (2.22–3.37) | 0.181 | 2.40 (1.09–3.17) | 0.288 | 2.11 (1.77–2.42) | 0.748 | 1.11 (1.05–1.23) | 0.073 | 1.52 (1.25–1.95) | 0.857 |
| Sheeting not seen | 149 | 2.73 (1.33–3.55) | 2.19 (1.02–3.30) | 2.08 (1.58–2.62) | 1.15 (1.04–1.65) | 1.50 (1.12–2.28) | |||||
| Macronucleoli present | 11 | 2.83 (2.03–3.21) | 0.743 | 2.84 (1.06–3.10) | 0.019 | 2.11 (1.92–2.41) | 0.486 | 1.11 (1.06–1.29) | 0.418 | 1.61 (1.36–1.95) | 0.051 |
| Macronucleoli not seen | 150 | 2.71 (1.33–3.55) | 2.16 (1.02–3.30) | 2.08 (1.58–2.62) | 1.14 (1.04–1.65) | 1.50 (1.12–2.28) | |||||
| Small cells present | 15 | 2.87 (2.22–3.33) | 0.054 | 1.86 (1.04–3.13) | 0.803 | 2.10 (1.74–2.62) | 0.355 | 1.11 (1.04–1.24) | 0.181 | 1.50 (1.25–1.98) | 0.526 |
| Small cells not seen | 146 | 2.70 (1.33–3.55) | 2.24 (1.02–3.30) | 2.09 (1.58–2.58) | 1.14 (1.04–1.65) | 1.51 (1.12–2.28) | |||||
| Psammoma bodies present | 108 | 2.70 (1.58–3.42) | 0.075 | 2.13 (1.02–3.30) | 0.017 | 2.09 (1.61–2.62) | 0.757 | 1.13 (1.04–1.65) | 0.079 | 1.48 (1.12–2.03) | 0.114 |
| Psammoma bodies not seen | 53 | 2.80 (1.33–3.55) | 2.38 (1.03–3.30) | 2.09 (1.58–2.55) | 1.16 (1.04–1.52) | 1.54 (1.17–2.28) | |||||
| SSTR | Measure | TTR (n = 55) | OS (n = 63) |
|---|---|---|---|
| SSTR1 | HR (CI) (p-value) | 1.012 (0.535–1.915) (0.972) | 1.187 (0.640–2.203) (0.587) |
| SSTR2 | HR (CI) (p-value) | 1.548 (1.050–2.281) (0.027) | 1.194 (0.842–1.693) (0.319) |
| SSTR3 | HR (CI) (p-value) | 1.008 (0.305–3.335) (0.990) | 0.777 (0.257–2.345) (0.654) |
| SSTR4 | HR (CI) (p-value) | 1.761 (0.146–21.212) (0.656) | 2.289 (0.246–21.343) (0.467) |
| SSTR5 | HR (CI) (p-value) | 1.172 (0.335–4.103) (0.804) | 1.797 (0.574–5.628) (0.314) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tollefsen, S.E.; Jarmund, A.H.; Ytterhus, B.; Salvesen, Ø.; Mjønes, P.; Torp, S.H. Somatostatin Receptors in Human Meningiomas—Clinicopathological Aspects. Cancers 2021, 13, 5704. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13225704
Tollefsen SE, Jarmund AH, Ytterhus B, Salvesen Ø, Mjønes P, Torp SH. Somatostatin Receptors in Human Meningiomas—Clinicopathological Aspects. Cancers. 2021; 13(22):5704. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13225704
Chicago/Turabian StyleTollefsen, Sofie Eline, Anders H. Jarmund, Borgny Ytterhus, Øyvind Salvesen, Patricia Mjønes, and Sverre Helge Torp. 2021. "Somatostatin Receptors in Human Meningiomas—Clinicopathological Aspects" Cancers 13, no. 22: 5704. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13225704