
A Guide for Water Bolus Temperature Selection for Semi-Deep Head and Neck Hyperthermia Treatments Using the HYPERcollar3D Applicator

 , , , and
, , , and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
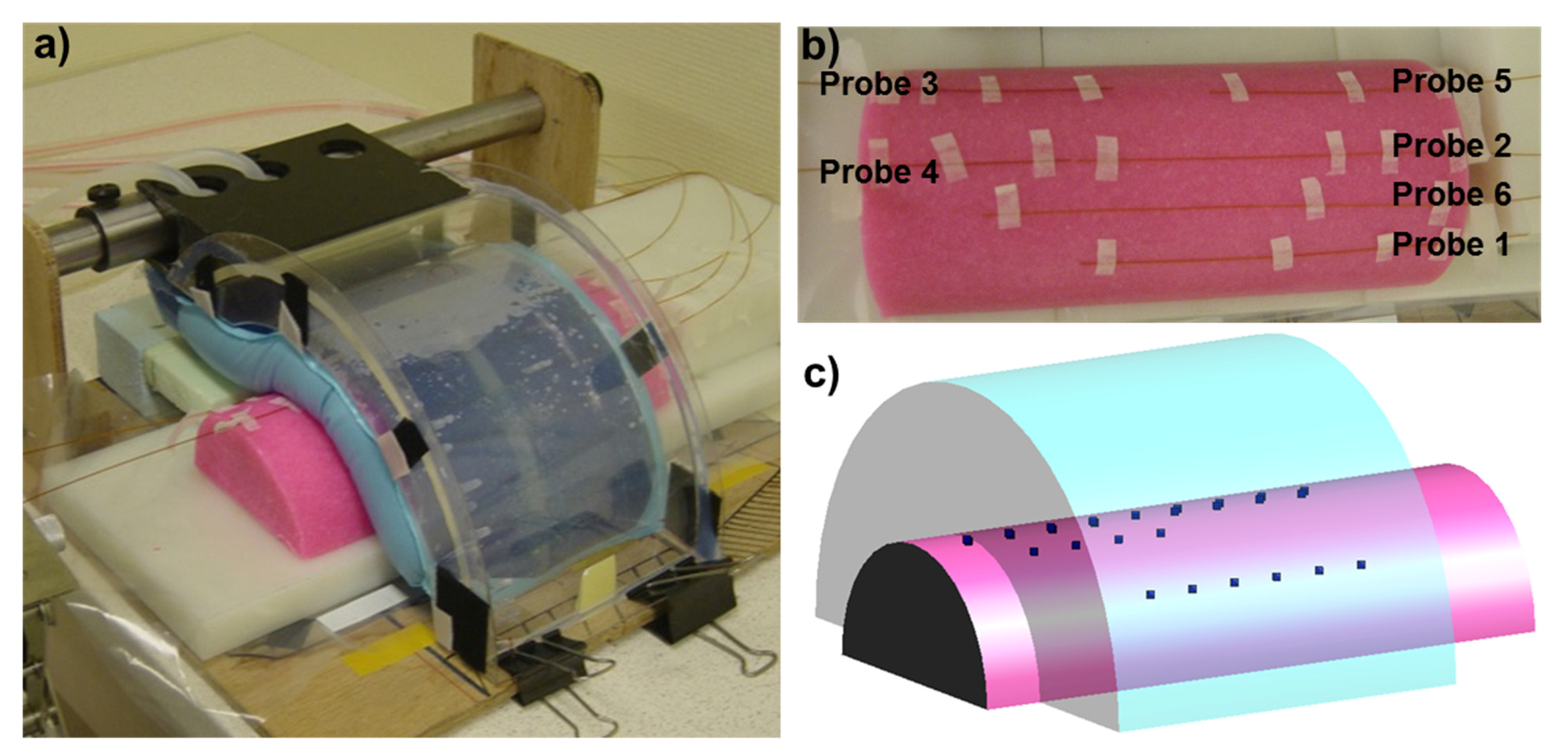
2.1. Water Bolus Experiment to Assess the Heat-Transfer Coefficient
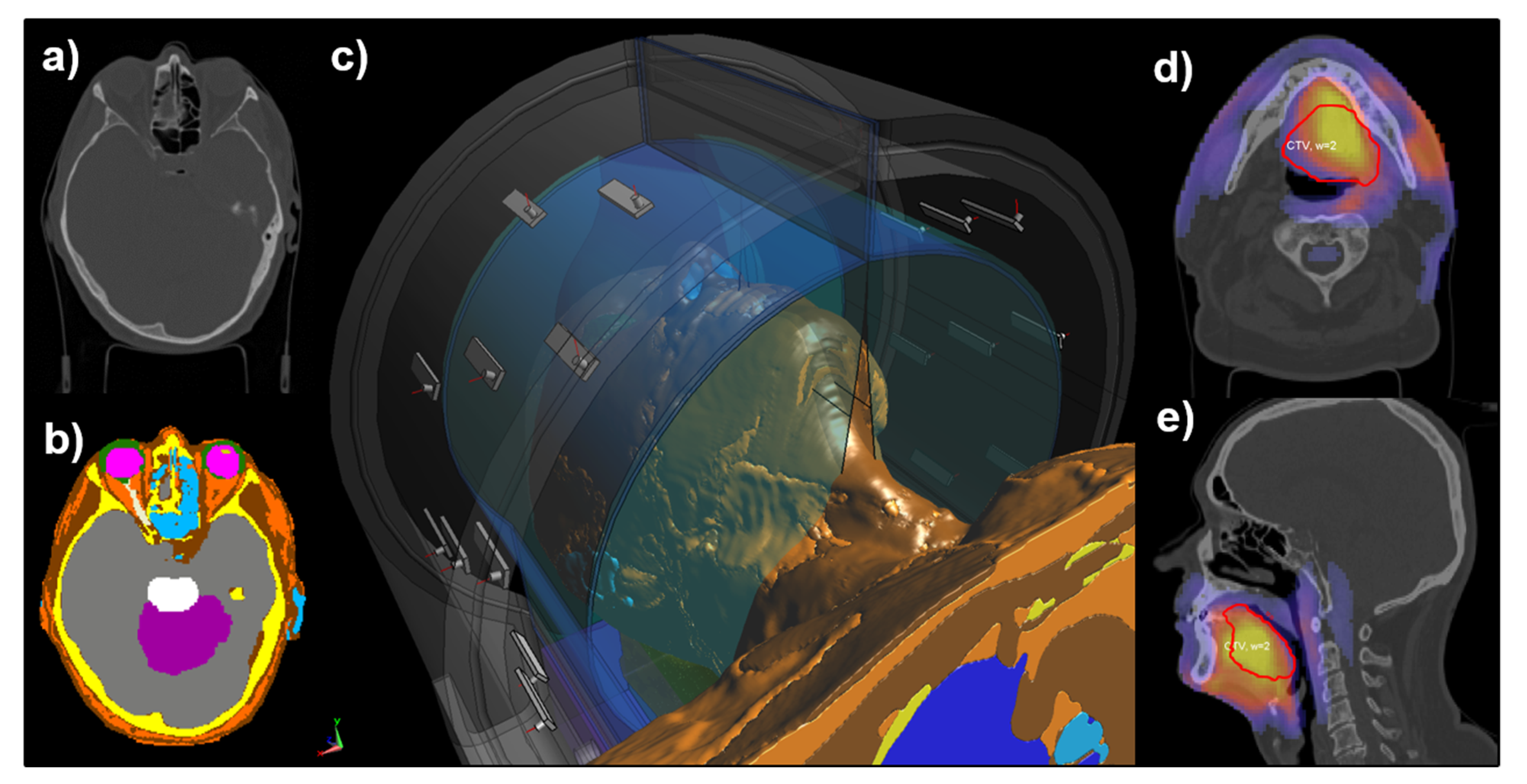
2.2. Hyperthermia Treatment Planning
2.3. Temperature Modeling
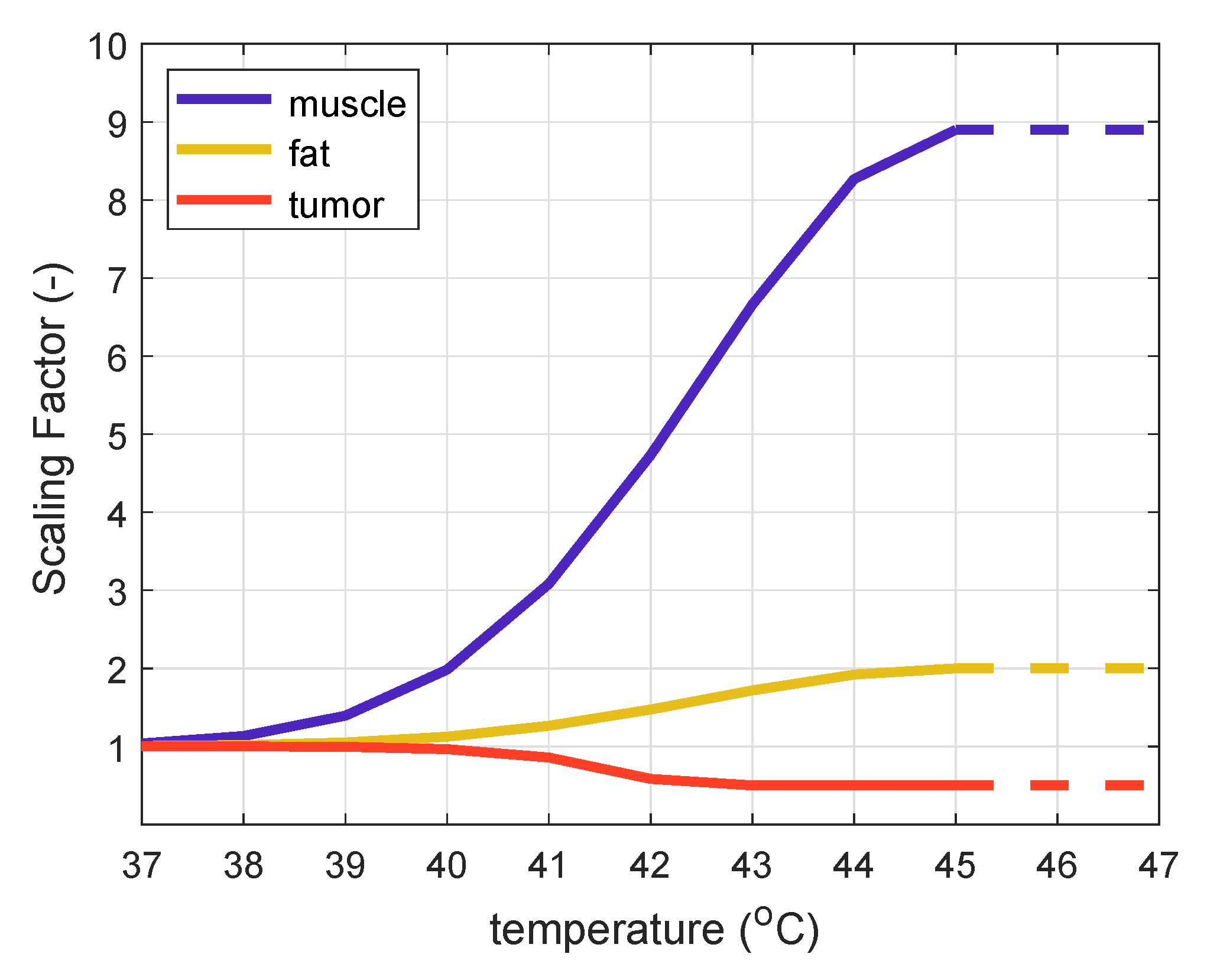
2.4. Thermal Tissue Property Models
2.5. Impact of Water Bolus on 3D Temperature Distribution
3. Results
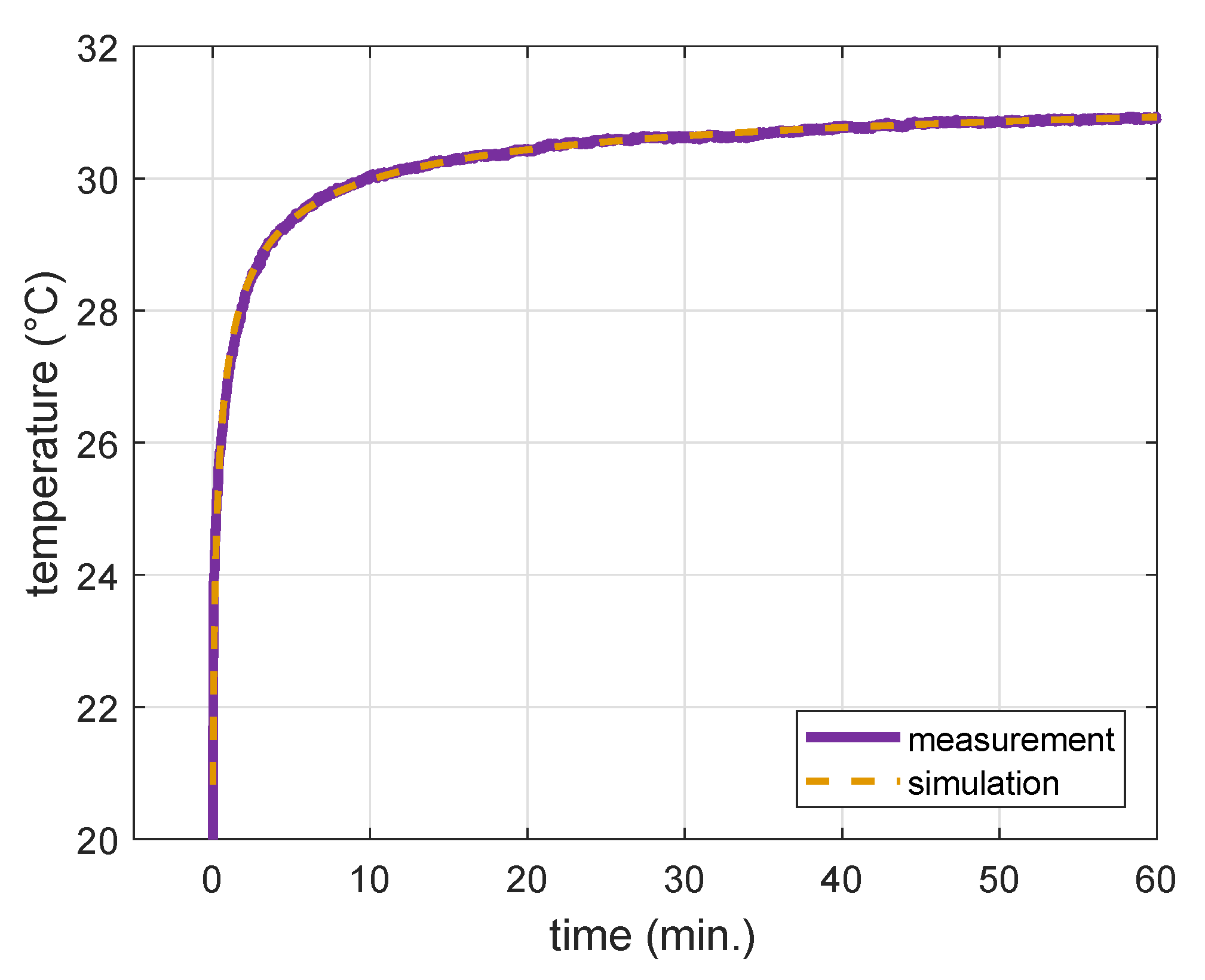
3.1. Water Bolus Convection Coefficient
3.2. Impact of Water Bolus on 3D Temperature Distribution
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rijnen, Z.; Togni, P.; Roskam, R.; van de Geer, S.G.; Goossens, R.H.M.; Paulides, M.M. Quality and comfort in head and neck hyperthermia: A redesign according to clinical experience and simulation studies. Int. J. Hyperth. 2015, 31, 823–830. [Google Scholar] [CrossRef] [Green Version]
- Verduijn, G.M.; de Wee, E.M.; Rijnen, Z.; Togni, P.; Hardillo, J.A.U.; Ten Hove, I.; Franckena, M.; Van Rhoon, G.C.; Paulides, M. Deep hyperthermia with the HYPERcollar system combined with irradiation for advanced head and neck carcinoma—A feasibility study. Int. J. Hyperth. 2018, 34, 994–1001. [Google Scholar] [CrossRef]
- Kroesen, M.; Mulder, H.T.; van Holthe, J.M.L.; Aangeenbrug, A.A.; Mens, J.W.M.; van Doorn, H.C.; Paulides, M.M.; Hoop, E.O.-D.; Vernhout, R.M.; Lutgens, L.C.; et al. Confirmation of thermal dose as a predictor of local control in cervical carcinoma patients treated with state-of-the-art radiation therapy and hyperthermia. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2019, 140, 150–158. [Google Scholar] [CrossRef]
- Togni, P.; Rijnen, Z.; Numan, W.C.M.; Verhaart, R.F.; Bakker, J.F.; van Rhoon, G.C.; Paulides, M. Electromagnetic redesign of the HYPERcollar applicator: Toward improved deep local head-and-neck hyperthermia. Phys. Med. Biol. 2013, 58, 5997–6009. [Google Scholar] [CrossRef]
- Drizdal, T.; Paulides, M.M.; van Holthe, N.; van Rhoon, G.C. Hyperthermia treatment planning guided applicator selection for sub-superficial head and neck tumors heating. Int. J. Hyperth. 2018, 34, 704–713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paulides, M.M.; Bakker, J.F.; Neufeld, E.; van der Zee, J.; Jansen, P.P.; Levendag, P.C.; van Rhoon, G.C. Winner of the “New Investigator Award” at the European Society of Hyperthermia Oncology Meeting 2007. The HYPERcollar: A novel applicator for hyperthermia in the head and neck. Int. J. Hyperth. 2007, 23, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Paulides, M.M.; Bakker, J.F.; Linthorst, M.; van der Zee, J.; Rijnen, Z.; Neufeld, E.; Pattynama, P.M.T.; Jansen, P.P.; Levendag, P.C.; van Rhoon, G.C. The clinical feasibility of deep hyperthermia treatment in the head and neck: New challenges for positioning and temperature measurement. Phys. Med. Biol. 2010, 55, 2465–2480. [Google Scholar] [CrossRef] [Green Version]
- Paulides, M.M.; Bakker, J.F.; Chavannes, N.; Rhoon, G.C.V. A patch antenna design for application in a phased-array head and neck hyperthermia applicator. IEEE Trans. Biomed. Eng. 2007, 54, 2057–2063. [Google Scholar] [CrossRef] [Green Version]
- der Gaag, M.L.V.; de Bruijne, M.; Samaras, T.; van der Zee, J.; van Rhoon, G.C. Development of a guideline for the water bolus temperature in superficial hyperthermia. Int. J. Hyperth. 2006, 22, 637–656. [Google Scholar] [CrossRef]
- Ito, K.; Furuya, K.; Okano, Y.; Hamada, L. Development and characteristics of a biological tissue-equivalent phantom for microwaves. Electron. Commun. Jpn. (Part I: Commun.) 2001, 84, 67–77. [Google Scholar] [CrossRef]
- Fortunati, V.; Verhaart, R.F.; Niessen, W.J.; Veenland, J.F.; Paulides, M.M.; van Walsum, T. Automatic tissue segmentation of head and neck MR images for hyperthermia treatment planning. Phys. Med. Biol. 2015, 60, 6547. [Google Scholar] [CrossRef] [PubMed]
- Rijnen, Z.; Bakker, J.F.; Canters, R.A.M.; Togni, P.; Verduijn, G.M.; Levendag, P.C.; Van Rhoon, G.C.; Paulides, M. Clinical integration of software tool VEDO for adaptive and quantitative application of phased array hyperthermia in the head and neck. Int. J. Hyperth. 2013, 29, 181–193. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, S.; Lau, R.W.; Gabriel, C. The dielectric properties of biological tissues: III. Parametric models for the dielectric spectrum of tissues. Phys. Med. Biol. 1996, 41, 2271–2293. [Google Scholar] [CrossRef] [Green Version]
- Hasgall, P.A.; Neufeld, E.; Gosselin, M.C.; Klingenbck, A.; Kuster, N.K. IT’IS Database for Thermal and Electromagnetic Parameters of Biological Tissues, Version 4.0; IT’IS: Zurich, Switzerland, 2018; Available online: www.itis.ethz.ch/database (accessed on 31 May 2018). [CrossRef]
- Verhaart, R.F.; Verduijn, G.M.; Fortunati, V.; Rijnen, Z.; van Walsum, T.; Veenland, J.F.; Paulides, M.M. Accurate 3D temperature dosimetry during hyperthermia therapy by combining invasive measurements and patient-specific simulations. Int. J. Hyperth. 2015, 31, 686–692. [Google Scholar] [CrossRef] [Green Version]
- Lang, J.; Erdmann, B.; Seebass, M. Impact of nonlinear heat transfer on temperature control in regional hyperthermia. IEEE Trans. Biomed. Eng. 1999, 46, 1129–1138. [Google Scholar] [CrossRef] [PubMed]
- Pennes, H.H. Analysis of tissue and arterial blood temperatures in the resting human forearm. Journal of Applied Physiology. J. Appl. Physiol. 1948, 1, 93–122. [Google Scholar] [CrossRef]
- Song, C.W.; Lokshina, A.; Rhee, J.G.; Patten, M.; Levitt, S.H. Implication of Blood Flow in Hyperthermic Treatment of Tumors. IEEE Trans. Biomed. Eng. 1984, BME-31, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Drizdal, T.; Togni, P.; Visek, L.; Vrba, J. Comparison of constant and temperature dependent blood perfusion in temperature prediction for superficial hyperthermia [Article]. Radioengineering 2010, 19, 281–289. [Google Scholar]
- Stauffer, P.R.; Maccarini, P.; Arunachalam, K.; Craciunescu, O.; Diederich, C.; Juang, T.; Rossetto, F.; Schlorff, J.; Milligan, A.; Hsu, J.; et al. Conformal microwave array (CMA) applicators for hyperthermia of diffuse chest wall recurrence. Int. J. Hyperth. 2010, 26, 686–698. [Google Scholar] [CrossRef] [Green Version]
- Birkelund, Y.; Jacobsen, S.; Arunachalam, K.; Maccarini, P.; Stauffer, P.R. Flow patterns and heat convection in a rectangular water bolus for use in superficial hyperthermia. Phys. Med. Biol. 2009, 54, 3937–3953. [Google Scholar] [CrossRef] [Green Version]
- Kok, H.P.; Gellermann, J.; van den Berg, C.A.T.; Stauffer, P.R.; Hand, J.W.; Crezee, J. Thermal modelling using discrete vasculature for thermal therapy: A review. Int. J. Hyperth. Off. J. Eur. Soc. Hyperthermic Oncol. N. Am. Hyperth. Group 2013, 29, 336–345. [Google Scholar] [CrossRef] [PubMed]
- Sumser, K.; Neufeld, E.; Verhaart, R.F.; Fortunati, V.; Verduijn, G.M.; Drizdal, T.; Van Walsum, T.; Veenland, J.F.; Paulides, M. Feasibility and relevance of discrete vasculature modeling in routine hyperthermia treatment planning. Int. J. Hyperth. 2019, 36, 801–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Tissue | ρ | σ | εr | k | c | ω | Q |
|---|---|---|---|---|---|---|---|
| (kg/m3) | (S/m) | (-) | (W/m·K) | (J/kg·K) | (ml/min·kg) | (W/kg) | |
| Air | 1.2 | 0 | 1 | - | - | - | - |
| Blood | 1050 | - | - | - | 3617 | - | - |
| Bone | 1908 | 0.09 | 13.1 | 0.32 | 1312 | 10 | 0.15 |
| Brainstem | 1046 | 1.05 | 55.1 | 0.51 | 3630 | 559 | 11.4 |
| Cartilage | 1099 | 0.6 | 45.1 | 0.49 | 3568 | 35 | 0.54 |
| Cerebellum | 1045 | 1.05 | 55.1 | 0.51 | 3653 | 763 | 15.5 |
| Cerebrum | 1045 | 0.75 | 56.8 | 0.55 | 3696 | 763 | 15.5 |
| Fat | 911 | 0.08 | 11.6 | 0.21/0.5 * | 2348 | 32.7/255 * | 0.51 |
| Lucite | 1180 | 0.003 | 2.6 | - | - | - | - |
| Lung | 394 | 0.38 | 23.6 | - | - | - | - |
| Muscle | 1090 | 0.8 | 56.7 | 0.49/0.4 * | 3421 | 39.1/442.8 * | 0.96 |
| Optical nerve | 1075 | 0.46 | 35 | 0.49 | 3613 | 160 | 2.5 |
| Sclera | 1032 | 1.01 | 57.4 | 0.58 | 4200 | 380 | 5.9 |
| Spinal cord | 1005 | 1.53 | 69 | 0.59 | 4047 | 160 | 2.5 |
| Tumor/GTV | 1050 | 0.89 | 59 | 0.51/1.5 * | 3950 | 72.3/848 * | 0 |
| Thyroid | 1050 | 0.89 | 61.3 | 0.52 | 3609 | 5624 | 87 |
| Vitreous humor | 1005 | 1.53 | 69 | 0.59 | 4047 | 0 | 0 |
| Water | 1000 | 0.04 | 78 | - | - | - | - |
| Patient | Age (Years) | Gender | CTV Location | CTV Median Depth (mm) | CTV Minimum Depth (mm) | CTV Maximum Depth (mm) | HT Treatments |
|---|---|---|---|---|---|---|---|
| 1 | 23 | M | nasopharynx | 52.5 | 36.5 | 70.8 | 6 |
| 2 | 65 | M | oropharynx | 38.1 | 19.5 | 58.1 | 3 |
| 3 | 75 | F | parotid gland | 8.9 | 0.3 | 29.1 | 4 |
| 4 | 69 | M | oropharynx | 20.5 | 3.6 | 38.8 | 3 |
| 5 | 45 | M | neck node metastasis | 15.2 | 0 | 54.6 | 5 |
| 6 | 68 | M | oropharynx | 43.0 | 11.7 | 78.5 | 3 |
| 7 | 65 | M | neck node metastasis | 14.7 | 0.9 | 34.4 | 5 |
| 8 | 55 | M | oropharynx | 39.9 | 22.5 | 60.0 | 3 |
| 9 | 68 | M | neck node metastasis | 10.7 | 2.1 | 30.6 | 4 |
| 10 | 69 | M | oropharynx | 9.6 | 0 | 29.2 | 3 |
| 11 | 67 | F | parotid gland | 22.3 | 4.8 | 45.9 | 6 |
| 12 | 60 | M | oropharynx | 21.9 | 7.8 | 46.0 | 5 |
| 13 | 56 | F | hypopharynx | 16.5 | 3.1 | 35.9 | 6 |
| 14 | 54 | F | larynx | 9.8 | 0 | 28.0 | 7 |
| 15 | 75 | M | oropharynx | 29.8 | 1.9 | 63.2 | 7 |
| 16 | 68 | M | oropharynx | 39.1 | 26.6 | 57.7 | 3 |
| 17 | 72 | F | oral cavity | 24.9 | 1.2 | 52.6 | 5 |
| 18 | 65 | M | larynx | 24.0 | 5.7 | 46.6 | 6 |
| 19 | 61 | M | oropharynx | 20.8 | 2.2 | 60.9 | 5 |
| 20 | 53 | F | sinus maxillaris | 52.1 | 27.9 | 71.6 | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drizdal, T.; van Rhoon, G.C.; Verhaart, R.F.; Fiser, O.; Paulides, M.M. A Guide for Water Bolus Temperature Selection for Semi-Deep Head and Neck Hyperthermia Treatments Using the HYPERcollar3D Applicator. Cancers 2021, 13, 6126. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13236126
Drizdal T, van Rhoon GC, Verhaart RF, Fiser O, Paulides MM. A Guide for Water Bolus Temperature Selection for Semi-Deep Head and Neck Hyperthermia Treatments Using the HYPERcollar3D Applicator. Cancers. 2021; 13(23):6126. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13236126
Chicago/Turabian StyleDrizdal, Tomas, Gerard C. van Rhoon, Rene F. Verhaart, Ondrej Fiser, and Margarethus M. Paulides. 2021. "A Guide for Water Bolus Temperature Selection for Semi-Deep Head and Neck Hyperthermia Treatments Using the HYPERcollar3D Applicator" Cancers 13, no. 23: 6126. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13236126