
The Role of Conventionally Fractionated Radiotherapy and Stereotactic Radiotherapy in the Treatment of Carcinoid Tumors and Large-Cell Neuroendocrine Cancer of the Lung

 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. NET Classification and Characteristics
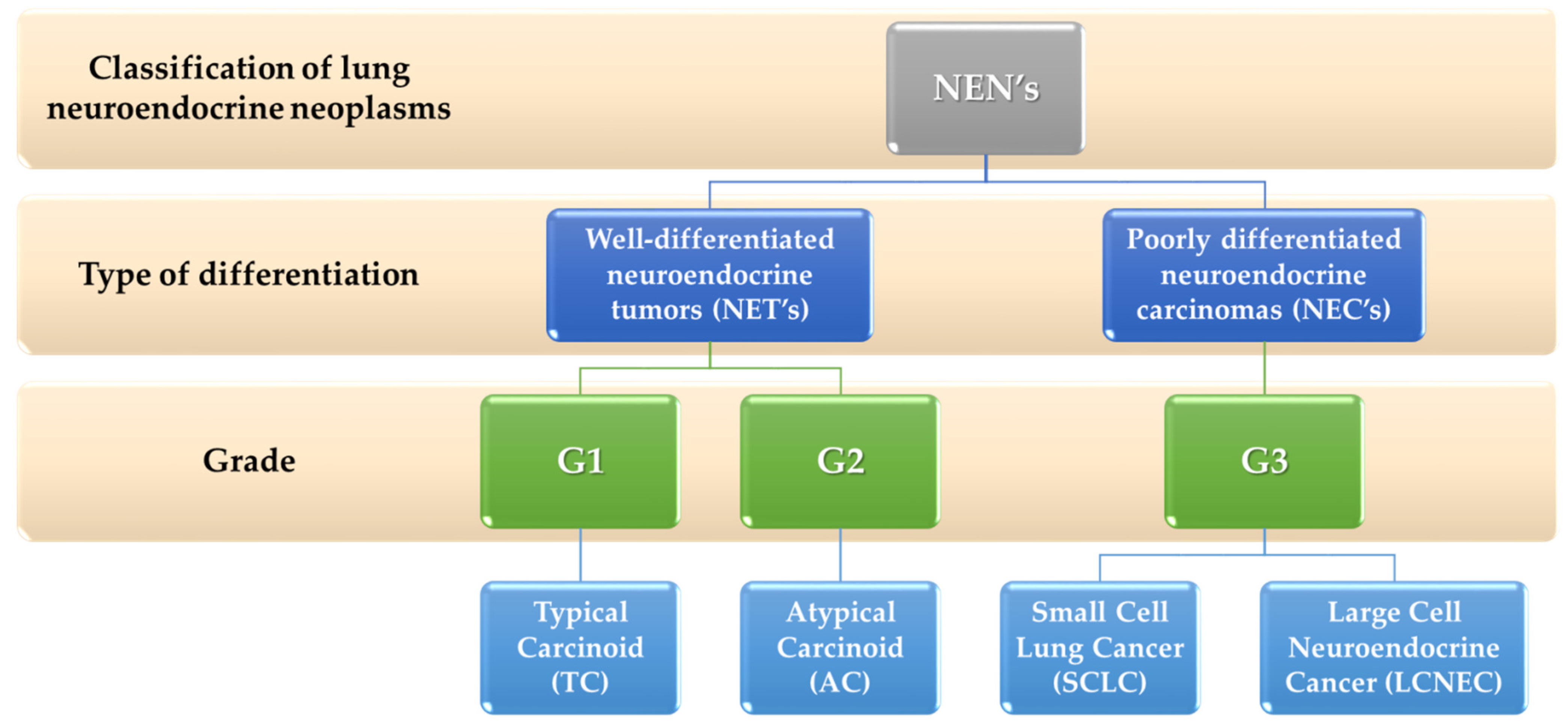
- G1 neoplasms are well-differentiated, low-grade.
- G2 neoplasms are well-differentiated and have an intermediate degree of malignancy.
- G3 are maldifferentiated, high-grade neoplasms.
3. Classification and Characteristics of Lung Neuroendocrine Neoplasms
4. The Role of Radiotherapy in the Treatment of TC and AT Carcinoids
- Radical—the highest effective doses of ionizing radiation are used to destroy tumor cells as much as possible [55].
- Palliative—radiation doses are used in order to effectively relieve symptoms, such as cancer pain, during or after anticancer treatment. It is usually given on an outpatient basis in a clinic or hospital during usually one or 5–10 fractions. Patients treated with this method do not pose a threat to other people because they do not emit radiation [56,57].
4.1. Conventional Radical and Palliative Radiotherapy and Radiochemotherapy
4.2. The Abscopal Effect in the Treatment of Carcinoids
4.3. Stereotactic Fractionated Radiation Therapy
5. The Role of Radiotherapy in the Treatment of LCNEC
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rindi, G.; Klimstra, D.S.; Abedi-Ardekani, B.; Asa, S.L.; Bosman, F.T.; Brambilla, E.; Busam, K.J.; De Krijger, R.R.; Dietel, M.; El-Naggar, A.K.; et al. A common classification framework for neuroendocrine neoplasms: An International Agency for Research on Cancer (IARC) and World Health Organization (WHO) expert consensus proposal. Mod. Pathol. 2018, 31, 1770–1786. [Google Scholar] [CrossRef]
- Klimstra, D.S.; Modlin, I.R.; Adsay, N.V.; Chetty, R.; Deshpande, V.; Gönen, M.; Jensen, R.T.; Kidd, M.; Kulke, M.H.; Lloyd, R.V.; et al. Pathology Reporting of Neuroendocrine Tumors: Application of the Delphic Consensus Process to the Development of a Minimum Pathology Data Set. Am. J. Surg. Pathol. 2010, 34, 300–313. [Google Scholar] [CrossRef] [PubMed]
- Klöppel, G. Neuroendocrine Neoplasms: Dichotomy, Origin and Classifications. Visc. Med. 2017, 33, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Inzani, F.; Petrone, G.; Fadda, G.; Rindi, G. Cyto-histology in NET: What is necessary today and what is the future? Rev. Endocr. Metab. Disord. 2017, 18, 381–391. [Google Scholar] [CrossRef] [PubMed]
- Ramage, J.; De Herder, W.; Fave, G.D.; Ferolla, P.; Ferone, D.; Ito, T.; Ruszniewski, P.; Sundin, A.; Weber, W.; Zheng-Pei, Z.; et al. ENETS Consensus Guidelines Update for Colorectal Neuroendocrine Neoplasms. Neuroendocrinology 2016, 103, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Kos-Kudła, B.; Blicharz-Dorniak, J.; Strzelczyk, J.; Bałdys-Waligórska, A.; Bednarczuk, T.; Bolanowski, M.; Boratyn-Nowicka, A.; Borowska, M.; Cichocki, A.; Ćwikła, J.B.; et al. Diagnostic and Therapeutic Guidelines for Gastro-Entero-Pancreatic Neuroendocrine Neoplasms (Recommended by the Polish Network of Neuroendocrine Tumours). Endokrynol. Pol. 2017, 68, 79–110. [Google Scholar] [CrossRef]
- Oberg, K.; Jelic, S. Neuroendocrine gastroenteropancreatic tumors: ESMO Clinical Recommendation for diagnosis, treatment and follow-up. Ann. Oncol. 2009, 20, iv150–iv153. [Google Scholar] [CrossRef]
- National Institutes of Health (NIH). Surveillance, Epidemiology, and End Results Program. Available online: https://seer.cancer.gov/index.html (accessed on 27 October 2020).
- Chauhan, A.; Yu, Q.; Ray, N.; Farooqui, Z.; Huang, B.; Durbin, E.B.; Tucker, T.; Evers, M.; Arnold, S.; Anthony, L.B. Global burden of neuroendocrine tumors and changing incidence in Kentucky. Oncotarget 2018, 9, 19245–19254. [Google Scholar] [CrossRef] [Green Version]
- Riihimäki, M.; Hemminki, A.; Sundquist, K.; Sundquist, J.; Hemminki, K. The epidemiology of metastases in neuroendocrine tumors. Int. J. Cancer 2016, 139, 2679–2686. [Google Scholar] [CrossRef]
- O’Connor, J.M.; Marmissolle, F.; Bestani, C.; Pesce, V.; Belli, S.; Dominichini, E.; Mendez, G.; Price, P.; Giacomi, N.; Pairola, A.; et al. Observational study of patients with gastroenteropancreatic and bronchial neuroendocrine tumors in Argentina: Results from the large database of a multidisciplinary group clinical multicenter study. Mol. Clin. Oncol. 2014, 2, 673–684. [Google Scholar] [CrossRef]
- Lombard-Bohas, C.; Mitry, E.; O’Toole, D.; Louvet, C.; Pillon, D.; Cadiot, G.; Borson-Chazot, F.; Aparicio, T.; Ducreux, M.; LeComte, T.; et al. Thirteen-Month Registration of Patients with Gastroenteropancreatic Endocrine Tumours in France. Neuroendocrinology 2009, 89, 217–222. [Google Scholar] [CrossRef]
- Sandvik, O.M.; Søreide, K.; Gudlaugsson, E.; Kvaløy, J.T.; A Søreide, J. Epidemiology and classification of gastroenteropancreatic neuroendocrine neoplasms using current coding criteria. Br. J. Surg. 2016, 103, 226–232. [Google Scholar] [CrossRef] [Green Version]
- Hallet, J.; Law, C.H.L.; Cukier, M.; Saskin, R.; Liu, N.; Singh, S. Exploring the rising incidence of neuroendocrine tumors: A population-based analysis of epidemiology, metastatic presentation, and outcomes. Cancer 2015, 121, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Giandomenico, V.; Modlin, I.M.; Pontén, F.; Nilsson, M.; Landegren, U.; Bergqvist, J.; Khan, M.S.; Millar, R.P.; Långström, B.; Borlak, J.; et al. Improving the Diagnosis and Management of Neuroendocrine Tumors: Utilizing New Advances in Biomarker and Molecular Imaging Science. Neuroendocrinology 2013, 98, 16–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berner, A.M.; Pipinikas, C.; Ryan, A.; Dibra, H.; Moghul, I.; Webster, A.; Luong, T.V.; Thirlwell, C. Diagnostic Approaches to Neuroendocrine Neoplasms of Unknown Primary Site. Neuroendocrinology 2020, 110, 563–573. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Poon, R.; Wong, R.; Metser, U. 68Ga PET Imaging in Patients with Neuroendocrine Tumors: A Systematic Review and Meta-Analysis. Clin. Nucl. Med. 2018, 43, 802–810. [Google Scholar] [CrossRef] [PubMed]
- Hope, T.A.; Bergsland, E.K.; Bozkurt, M.F.; Graham, M.; Heaney, A.P.; Herrmann, K.; Howe, J.; Kulke, M.H.; Kunz, P.L.; Mailman, J.; et al. Appropriate Use Criteria for Somatostatin Receptor PET Imaging in Neuroendocrine Tumors. J. Nucl. Med. 2018, 59, 66–74. [Google Scholar] [CrossRef]
- Chan, J.A.; Kulke, M.H. Progress in the treatment of neuroendocrine tumors. Curr. Oncol. Rep. 2009, 11, 193–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrera-Martínez, A.D.; Hofland, J.; Hofland, L.J.; Brabander, T.; Eskens, F.A.L.M.; Moreno, M.A.G.; Luque, R.M.; Castaño, J.P.; De Herder, W.W.; Feelders, R.A. Targeted Systemic Treatment of Neuroendocrine Tumors: Current Options and Future Perspectives. Drugs 2019, 79, 21–42. [Google Scholar] [CrossRef] [Green Version]
- Clinical Practice Guidelines—Lung and Thymic Carcinoids—European Society for Medical Oncology. Available online: https://www.esmo.org/guidelines/endocrine-and-neuroendocrine-cancers/lung-and-thymic-carcinoids (accessed on 20 December 2021).
- Öberg, K. Management of functional neuroendocrine tumors of the pancreas. Gland. Surg. 2018, 7, 20–27. [Google Scholar] [CrossRef] [Green Version]
- Cloyd, J.M. Non-functional neuroendocrine tumors of the pancreas: Advances in diagnosis and management. World J. Gastroenterol. 2015, 21, 9512–9525. [Google Scholar] [CrossRef] [PubMed]
- Guidelines Detail. Available online: https://www.nccn.org/guidelines/guidelines-detail (accessed on 27 October 2021).
- Klöppel, G.; Couvelard, A.; Hruban, R.H.; Klimstra, D.S.; Komminoth, P.; Osamura, R.Y.; Perren, A.; Rindi, G. WHO Classification of Tumours of the Endocrine Organs; WHO/IARC Classification of Tumours; IARC Press: Lyon, France, 2017; Volume 10, pp. 210–239. ISBN 978-92-832-4493-6. [Google Scholar]
- Philips, P.; Kooby, D.A.; Maithel, S.; Merchant, N.B.; Weber, S.M.; Winslow, E.R.; Ahmad, S.; Kim, H.J.; Scoggins, C.R.; McMasters, K.M.; et al. Grading Using Ki-67 Index and Mitotic Rate Increases the Prognostic Accuracy of Pancreatic Neuroendocrine Tumors. Pancreas 2018, 47, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Tracht, J.; Zhang, K.; Peker, D. Grading and Prognostication of Neuroendocrine Tumors of the Pancreas: A Comparison Study of Ki67 and PHH3. J. Histochem. Cytochem. 2017, 65, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Nadler, A.; Cukier, M.; Rowsell, C.; Kamali, S.; Feinberg, Y.; Singh, S.; Law, C.H.L. Ki-67 is a reliable pathological grading marker for neuroendocrine tumors. Virchows Arch. 2013, 462, 501–505. [Google Scholar] [CrossRef] [PubMed]
- Hofman, M.; Hicks, R.J. Changing paradigms with molecular imaging of neuroendocrine tumors. Discov. Med. 2012, 14, 71–81. [Google Scholar]
- Pancreatic Neuroendocrine Tumors: State-of-the-Art Diagnosis and Management. Available online: https://www.cancernetwork.com/view/pancreatic-neuroendocrine-tumors-state-art-diagnosis-and-management (accessed on 27 October 2021).
- Sorbye, H.; Welin, S.; Langer, S.W.; Vestermark, L.W.; Holt, N.; Osterlund, P.; Dueland, S.; Hofsli, E.; Guren, M.G.; Ohrling, K.; et al. Predictive and prognostic factors for treatment and survival in 305 patients with advanced gastrointestinal neuroendocrine carcinoma (WHO G3): The NORDIC NEC study. Ann. Oncol. 2013, 24, 152–160. [Google Scholar] [CrossRef]
- Scarpa, A.; Mantovani, W.; Capelli, P.; Beghelli, S.; Boninsegna, L.; Bettini, R.; Panzuto, F.; Pederzoli, P.; Fave, G.D.; Falconi, M. Pancreatic endocrine tumors: Improved TNM staging and histopathological grading permit a clinically efficient prognostic stratification of patients. Mod. Pathol. 2010, 23, 824–833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strosberg, J.R.; Weber, J.M.; Feldman, M.; Coppola, D.; Meredith, K.; Kvols, L.K. Prognostic Validity of the American Joint Committee on Cancer Staging Classification for Midgut Neuroendocrine Tumors. J. Clin. Oncol. 2013, 31, 420–425. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rindi, G.; Klöppel, G.; Alhman, H.; Caplin, M.; Couvelard, A.; de Herder, W.W.; Erikssson, B.; Falchetti, A.; Falconi, M.; Komminoth, P.; et al. TNM staging of foregut (neuro)endocrine tumors: A consensus proposal including a grading system. Virchows Arch. 2006, 449, 395–401. [Google Scholar] [CrossRef] [Green Version]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. (Eds.) AJCC Cancer Staging Manual, 8th ed.; Springer: Berlin/Heidelberg, Germany, 2017; ISBN 978-3-319-40617-6. [Google Scholar]
- Qian, Z.R.; Ter-Minassian, M.; Chan, J.A.; Imamura, Y.; Hooshmand, S.M.; Kuchiba, A.; Morikawa, T.; Brais, L.K.; Daskalova, A.; Heafield, R.; et al. Prognostic Significance of MTOR Pathway Component Expression in Neuroendocrine Tumors. J. Clin. Oncol. 2013, 31, 3418–3425. [Google Scholar] [CrossRef] [Green Version]
- Francis, J.M.; Kiezun, A.; Ramos, A.H.; Serra, S.; Pedamallu, C.S.; Qian, Z.R.; Banck, M.S.; Kanwar, R.; A Kulkarni, A.; Karpathakis, A.; et al. Somatic mutation of CDKN1B in small intestine neuroendocrine tumors. Nat. Genet. 2013, 45, 1483–1486. [Google Scholar] [CrossRef]
- Kim, H.S.; Lee, H.S.; Nam, K.H.; Choi, J.; Kim, W.H. P27 Loss Is Associated with Poor Prognosis in Gastroenteropancreatic Neuroendocrine Tumors. Cancer Res. Treat. 2014, 46, 383–392. [Google Scholar] [CrossRef]
- Herrera-Martínez, A.D.; Hofland, L.J.; Moreno, M.A.G.; Castaño, J.P.; De Herder, W.W.; A Feelders, R. Neuroendocrine neoplasms: Current and potential diagnostic, predictive and prognostic markers. Endocr.-Relat. Endocr.-Relat. Cancer 2019, 26, R157–R179. [Google Scholar] [CrossRef] [Green Version]
- Öberg, K. Molecular Genomic Blood Biomarkers for Neuroendocrine Tumors: The Long and Winding Road from Berzelius and Bence Jones to a Neuroendocrine Destination. Neuroendocrinology 2021, 111, 297–303. [Google Scholar] [CrossRef]
- Oberg, K.; Modlin, I.M.; De Herder, W.; Pavel, M.; Klimstra, D.; Frilling, A.; Metz, D.C.; Heaney, A.; Kwekkeboom, D.J.; Strosberg, J.R.; et al. Consensus on biomarkers for neuroendocrine tumour disease. Lancet Oncol. 2015, 16, e435–e446. [Google Scholar] [CrossRef] [Green Version]
- Metovic, J.; Barella, M.; Pelosi, G. Neuroendocrine neoplasms of the lung: A pathology update. MEMO Mag. Eur. Med. Oncol. 2021, 1–5. [Google Scholar] [CrossRef]
- World Health Organization. WHO Classification of Tumours of the Lung, Pleura, Thymus and Heart; Travis, W.D., Brambilla, E., Burke, A.P., Marx, A., Nicholson, A.G., Eds.; WHO: Geneva, Switzerland, 2015; ISBN 978-92-832-2436-5. [Google Scholar]
- Travis, W.D.; Brambilla, E.; Nicholson, A.G.; Yatabe, Y.; Austin, J.H.M.; Beasley, M.B.; Chirieac, L.R.; Dacic, S.; Duhig, E.; Flieder, D.B.; et al. The 2015 World Health Organization Classification of Lung Tumors: Impact of Genetic, Clinical and Radiologic Advances Since the 2004 Classification. J. Thorac. Oncol. 2015, 10, 1243–1260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuroendocrine Tumor of the Lung—Statistics. Available online: https://www.cancer.net/cancer-types/neuroendocrine-tumor-lung/statistics (accessed on 27 October 2021).
- Hemminki, K.; Li, X. Incidence trends and risk factors of carcinoid tumors. Cancer 2001, 92, 2204–2210. [Google Scholar] [CrossRef]
- Limaiem, F.; Tariq, M.A.; Wallen, J.M. Lung Carcinoid Tumors. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Gosain, R.; Mukherjee, S.; Yendamuri, S.S.; Iyer, R. Management of Typical and Atypical Pulmonary Carcinoids Based on Different Established Guidelines. Cancers 2018, 10, 510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clinical Lung Cancer Genome Project (CLCGP) and Network Genomic Medicine (NGM) A Genomics-Based Classification of Human Lung Tumors. Sci. Transl. Med. 2013, 5, 209ra153. [CrossRef] [Green Version]
- Oronsky, B.; Ma, P.C.; Morgensztern, D.; Carter, C.A. Nothing But NET: A Review of Neuroendocrine Tumors and Carcinomas. Neoplasia 2017, 19, 991–1002. [Google Scholar] [CrossRef]
- Pelosi, G.; Pattini, L.; Morana, G.; Fabbri, A.; Faccinetto, A.; Fazio, N.; Valeri, B.; Sonzogni, A. Grading lung neuroendocrine tumors: Controversies in search of a solution. Histol. Histopathol. 2017, 32, 223–241. [Google Scholar] [CrossRef]
- Neuroendocrine Tumor of the Lung—Risk Factors. Available online: https://www.cancer.net/cancer-types/neuroendocrine-tumor-lung/risk-factors (accessed on 27 October 2021).
- Neuroendocrine Tumor of the Lung—Symptoms and Signs. Available online: https://www.cancer.net/cancer-types/neuroendocrine-tumor-lung/symptoms-and-signs (accessed on 27 October 2021).
- Neuroendocrine Tumor of the Lung—Diagnosis. Available online: https://www.cancer.net/cancer-types/neuroendocrine-tumor-lung/diagnosis (accessed on 27 October 2021).
- NICE Guideline Updates Team. Radical Radiotherapy; National Institute for Health and Care Excellence: London, UK, 2019. [Google Scholar]
- D’Souza, N.; Holden, L.; Robson, S.; Mah, K.; Di Prospero, L.; Wong, C.S.; Chow, E.; Spayne, J. Modern palliative radiation treatment: Do complexity and workload contribute to medical errors? Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, e43–e48. [Google Scholar] [CrossRef]
- Tao, M.J.; Probyn, L.; Poon, M.; Kreder, H.; Wan, B.A.; Diaz, P.; Chow, E. Symptomatic Palliation with Radiotherapy in Ex-tensive Heterotopic Ossifications. Ann. Palliat. Med. 2018, 6, S260–S263. [Google Scholar] [CrossRef]
- Radiation Therapy|Radiation Treatment for Cancer. Available online: https://www.cancer.org/treatment/treatments-and-side-effects/treatment-types/radiation.html (accessed on 27 October 2021).
- Stein, J.J.; Ottoman, R.E.; Langdon, E.A.; Gore, W.A. Use of Megavoltage Therapy in Cancer: End-Results. Radiology 1962, 79, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Shrimali, R.K.; Nallathambi, C.; Saha, A.; Das, A.; Prasath, S.; Mahata, A.; Arun, B.; Mallick, I.; Achari, R.; Dabkara, D.; et al. Radical radiotherapy or chemoradiotherapy for inoperable, locally advanced, non-small cell lung cancer: Analysis of patient profile, treatment approaches, and outcomes for 213 patients at a tertiary cancer center. Indian J. Cancer 2018, 55, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Cattoni, M.; Vallières, E.; Brown, L.M.; Sarkeshik, A.A.; Margaritora, S.; Siciliani, A.; Filosso, P.L.; Guerrera, F.; Imperatori, A.; Rotolo, N.; et al. Improvement in TNM staging of pulmonary neuroendocrine tumors requires histology and regrouping of tumor size. J. Thorac. Cardiovasc. Surg. 2018, 155, 405–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cancer Staging System. Available online: http://www.facs.org/quality-programs/cancer/ajcc/cancer-staging (accessed on 27 October 2021).
- Wirth, L.J.; Carter, M.R.; Jänne, P.A.; Johnson, B.E. Outcome of patients with pulmonary carcinoid tumors receiving chemotherapy or chemoradiotherapy. Lung Cancer 2004, 44, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Chong, C.R.; Wirth, L.J.; Nishino, M.; Chen, A.B.; Sholl, L.M.; Kulke, M.H.; McNamee, C.J.; Jänne, P.A.; Johnson, B.E. Chemotherapy for locally advanced and metastatic pulmonary carcinoid tumors. Lung Cancer 2014, 86, 241–246. [Google Scholar] [CrossRef] [Green Version]
- Dasari, A.; Bergsland, E.K.; Benson, A.B.; Cai, B.; Huynh, L.; Totev, T.; Shea, J.; Duh, M.S.; Neary, M.P.; Dagohoy, C.G.; et al. Treatment Patterns and Clinical Outcomes in Advanced Lung Neuroendocrine Tumors in Real-World Settings: A Multicenter Retrospective Chart Review Study. Oncologist 2019, 24, 1066–1075. [Google Scholar] [CrossRef] [Green Version]
- Okoye, C.C.; Jablons, D.M.; Jahan, T.M.; Kukreja, J.; Cardozo, S.; Yom, S.S. Divergent Management Strategies for Typical Versus Atypical Carcinoid Tumors of the Thoracic Cavity. Am. J. Clin. Oncol. 2014, 37, 350–355. [Google Scholar] [CrossRef]
- Kaifi, J.T.; Kayser, G.; Ruf, J.; Passlick, B. The Diagnosis and Treatment of Bronchopulmonary Carcinoid. Dtsch. Aerzteblatt Online 2015, 112, 479–485. [Google Scholar] [CrossRef] [Green Version]
- Mackley, H.B.; Videtic, G.M.M. Primary carcinoid tumors of the lung: A role for radiotherapy. Oncology 2006, 20, 1537–1543, discussion 1544–1545,1549. [Google Scholar]
- Kareff, S.A.; Lischalk, J.W.; Krochmal, R.; Kim, C. Abscopal effect in pulmonary carcinoid tumor following ablative stereotactic body radiation therapy: A case report. J. Med. Case Rep. 2020, 14, 177. [Google Scholar] [CrossRef] [PubMed]
- Bilski, M.; Stefaniuk, P.; Jędrejek, M.; Cisek, P.; Bilska, M.; Cisek, I.; Grzybowska-Szatkowska, L. Abscopal Effect of Radiotherapy—The Pursuit of the Unknown. In Proceedings of the RAD 2018: Sixth Inter-National Conference on Radiation and Applications in Various Fields of Research, Ohrid, Macedonia, 18–22 June 2018; p. 324. Available online: https://Www.Rad-Conference.Org/Book_of_Abstracts-RAD_2018.Pdf (accessed on 19 December 2021).
- Yilmaz, M.T.; Elmali, A.; Yazici, G. Abscopal Effect, From Myth to Reality: From Radiation Oncologists’ Perspective. Cureus 2019, 11, e3860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dagoglu, N.; Karaman, S.; Caglar, H.B.; Oral, E.N. Abscopal Effect of Radiotherapy in the Immunotherapy Era: Systematic Review of Reported Cases. Cureus 2019, 11, e4103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sato, H.; Suzuki, Y.; Yoshimoto, Y.; Noda, S.-E.; Murata, K.; Takakusagi, Y.; Okazaki, A.; Sekihara, T.; Nakano, T. An abscopal effect in a case of concomitant treatment of locally and peritoneally recurrent gastric cancer using adoptive T-cell immunotherapy and radiotherapy. Clin. Case Rep. 2017, 5, 380–384. [Google Scholar] [CrossRef]
- Kingsley, D.P.E. An interesting case of possible abscopal effect in malignant melanoma. Br. J. Radiol. 1975, 48, 863–866. [Google Scholar] [CrossRef]
- Robins, H.I.; Buchon, J.A.; Varanasi, V.R.; Weinstein, A.B. The abscopal effect: Demonstration in lymphomatous involvement of kidneys. Med. Pediatr. Oncol. 1981, 9, 473–476. [Google Scholar] [CrossRef] [PubMed]
- Wersäll, P.J.; Blomgren, H.; Pisa, P.; Lax, I.; Kälkner, K.-M.; Svedman, C. Regression of non-irradiated metastases after extracranial stereotactic radiotherapy in metastatic renal cell carcinoma. Acta Oncol. 2006, 45, 493–497. [Google Scholar] [CrossRef] [PubMed]
- Cummings, A.L.; Kaprealian, T.B.; Sarantopoulos, G.P.; Mendenhall, M.A.; Goldman, J.W. An Abscopal Effect in a Case of Neuroendocrine Atypical Carcinoid Lung Cancer. Appl. Radiat. Oncol. 2017, 6, 38–39. [Google Scholar]
- Ball, D.; Mai, G.T.; Vinod, S.; Babington, S.; Ruben, J.; Kron, T.; Chesson, B.; Herschtal, A.; Vanevski, M.; Rezo, A.; et al. Stereotactic ablative radiotherapy versus standard radiotherapy in stage 1 non-small-cell lung cancer (TROG 09.02 CHISEL): A phase 3, open-label, randomised controlled trial. Lancet Oncol. 2019, 20, 494–503. [Google Scholar] [CrossRef]
- Figlia, V.; Mazzola, R.; Cuccia, F.; Alongi, F.; Mortellaro, G.; Cespuglio, D.; Cucchiara, T.; Iacoviello, G.; Valenti, V.; Molino, M.; et al. Hypo-fractionated stereotactic radiation therapy for lung malignancies by means of helical tomotherapy: Report of feasibility by a single-center experience. Radiol. Med. 2018, 123, 406–414. [Google Scholar] [CrossRef] [PubMed]
- Cuccia, F.; Mortellaro, G.; Mazzola, R.; Donofrio, A.; Valenti, V.; Tripoli, A.; Matranga, D.; Casto, A.L.; Failla, G.; Di Miceli, G.; et al. Prognostic value of two geriatric screening tools in a cohort of older patients with early stage Non-Small Cell Lung Cancer treated with hypofractionated stereotactic radiotherapy. J. Geriatr. Oncol. 2020, 11, 475–481. [Google Scholar] [CrossRef]
- Siva, S.; Correa, R.J.; Warner, A.; Staehler, M.; Ellis, R.J.; Ponsky, L.; Kaplan, I.D.; Mahadevan, A.; Chu, W.; Gandhidasan, S.; et al. Stereotactic Ablative Radiotherapy for ≥T1b Primary Renal Cell Carcinoma: A Report from the International Radiosurgery Oncology Consortium for Kidney (IROCK). Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, 941–949. [Google Scholar] [CrossRef] [PubMed]
- Grant, S.R.; Lei, X.; Hess, K.R.; Smith, G.L.; Matin, S.F.; Wood, C.G.; Nguyen, Q.; Frank, S.J.; Anscher, M.S.; Smith, B.D.; et al. Stereotactic Body Radiation Therapy for the Definitive Treatment of Early Stage Kidney Cancer: A Survival Comparison With Surgery, Tumor Ablation, and Observation. Adv. Radiat. Oncol. 2020, 5, 495–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siva, S.; Chesson, B.; Bressel, M.; Pryor, D.; Higgs, B.; Reynolds, H.M.; Hardcastle, N.; Montgomery, R.; Vanneste, B.; Khoo, V.; et al. TROG 15.03 phase II clinical trial of Focal Ablative STereotactic Radiosurgery for Cancers of the Kidney—FASTRACK II. BMC Cancer 2018, 18, 1030. [Google Scholar] [CrossRef] [Green Version]
- Colaco, R.J.; Decker, R.H. Stereotactic Radiotherapy in the Treatment of Primary Bronchial Carcinoid Tumor. Clin. Lung Cancer 2015, 16, e11–e14. [Google Scholar] [CrossRef]
- Singh, D.; Chen, Y.; Cummings, M.A.; Milano, M.T. Inoperable Pulmonary Carcinoid Tumors: Local Control Rates with Stereotactic Body Radiotherapy/Hypofractionated RT with Image-Guided Radiotherapy. Clin. Lung Cancer 2019, 20, e284–e290. [Google Scholar] [CrossRef] [PubMed]
- Wegner, R.E.; Abel, S.; Horne, Z.D.; Hasan, S.; Colonias, A.; Verma, V. Stereotactic body radiation therapy versus fractionated radiation therapy for early-stage bronchopulmonary carcinoid. Lung Cancer Manag. 2019, 8, LMT14. [Google Scholar] [CrossRef]
- Rieber, J.; Schmitt, J.; Warth, A.; Muley, T.; Kappes, J.; Eichhorn, F.; Hoffmann, H.; Heussel, C.P.; Welzel, T.; Debus, J.; et al. Outcome and prognostic factors of multimodal therapy for pulmonary large-cell neuroendocrine carcinomas. Eur. J. Med. Res. 2015, 20, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, Y.; Lei, C.; Zhang, X.; Cui, Y.; Che, K.; Shen, H. Double-edged role of radiotherapy in patients with pulmonary large-cell neuroendocrine carcinoma. J. Cancer 2019, 10, 6422–6430. [Google Scholar] [CrossRef]
- Prelaj, A.; Rebuzzi, S.E.; Del Bene, G.; Berrìos, J.R.G.; Emiliani, A.; De Filippis, L.; Prete, A.A.; Pecorari, S.; Manna, G.; Ferrara, C.; et al. Evaluation of the efficacy of cisplatin–etoposide and the role of thoracic radiotherapy and prophylactic cranial irradiation in LCNEC. ERJ Open Res. 2017, 3, 00128–02016. [Google Scholar] [CrossRef]
- Pavel, M.; O’Toole, D.; Costa, F.; Capdevila, J.; Gross, D.; Kianmanesh, R.; Krenning, E.; Knigge, U.; Salazar, R.; Pape, U.-F.; et al. ENETS Consensus Guidelines Update for the Management of Distant Metastatic Disease of Intestinal, Pancreatic, Bronchial Neuroendocrine Neoplasms (NEN) and NEN of Unknown Primary Site. Neuroendocrinology 2016, 103, 172–185. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | G1 | G2 | G3 |
|---|---|---|---|
| Grade | Low | medium | high |
| Differentiation | Well | well | poorly |
| Ki-67 index [%] | ≤2 | 3–20 | >20 |
| Mitotic index | <2/10 HPF | 2–20/10 HPF | >20/10 HPF |
| Angioinvasion | Never | delay | always |
| Metastasis | − | − | + |
| Muscularis propia invasion | − | ± | + |
| Prognosis | Slowly growing | Slowly growing | Agressive |
| Characteristic | TC | AC | SCLC | LCNEC |
|---|---|---|---|---|
| Grade | Low | Intermediate | High | High |
| Morphological diversity | Well differentiated | Well differentiated | Poorly differentiated | Poorly differentiated |
| Common localization in the lung | central | peripherial | peripherial | Hilar/peripherial |
| Number of mitosis/2 mm² | <2 | 2–10 | >10 | >10 |
| Presence of necrosis | Absence | Possible spot outbreaks | Very often on large fragments | Often on large fragments |
| Lymph node metastases at diagnosis | 10–15% | 50% | 60–80% | 60–80% |
| Distant metastases at diagnosis | 3–5% | 20–25% | 40% | 60–70% |
| Paraneoplastic syndrome | + | ++ | + | ++++ |
| Grade | T Describes the Original Tumor | N Describes Whether or Not the Cancer Has Reached nearby Lymph Nodes | M Describes Whether There Are Distant Metastases |
|---|---|---|---|
| Latent cancer | Tx | N0 | M0 |
| Grade 0 | Tis | N0 | M0 |
| Grade IA1 | T1mi, T1a | N0 | M0 |
| Grade IA2 | T1b | N0 | M0 |
| GradeIA3 | T1c | N0 | M0 |
| Grade IB | T2a | N0 | M0 |
| Grade IIA | T2b | N0 | M0 |
| Grade IIB | T1a, T1b, T1c T2a, T2b T3 | N1 N1 N0 | M0 M0 M0 |
| Grade IIIA | T1a, T1b, T1c T2a, T2b T3 T4 | N2 N2 N1 N0, N1 | M0 M0 M0 M0 |
| Grade IIIB | T1a, T1b, T1c T2a, T2b T3 T4 | N3 N3 N2 N2 | M0 M0 M0 M0 |
| Grade IIIC | T3 T4 | N3 N3 | M0 M0 |
| Grade IVA | Any T Any T | Any N Any N | M1a M1b |
| Grade IVB | Any T | Any N | M1c |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bilski, M.; Mertowska, P.; Mertowski, S.; Sawicki, M.; Hymos, A.; Niedźwiedzka-Rystwej, P.; Grywalska, E. The Role of Conventionally Fractionated Radiotherapy and Stereotactic Radiotherapy in the Treatment of Carcinoid Tumors and Large-Cell Neuroendocrine Cancer of the Lung. Cancers 2022, 14, 177. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14010177
Bilski M, Mertowska P, Mertowski S, Sawicki M, Hymos A, Niedźwiedzka-Rystwej P, Grywalska E. The Role of Conventionally Fractionated Radiotherapy and Stereotactic Radiotherapy in the Treatment of Carcinoid Tumors and Large-Cell Neuroendocrine Cancer of the Lung. Cancers. 2022; 14(1):177. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14010177
Chicago/Turabian StyleBilski, Mateusz, Paulina Mertowska, Sebastian Mertowski, Marcin Sawicki, Anna Hymos, Paulina Niedźwiedzka-Rystwej, and Ewelina Grywalska. 2022. "The Role of Conventionally Fractionated Radiotherapy and Stereotactic Radiotherapy in the Treatment of Carcinoid Tumors and Large-Cell Neuroendocrine Cancer of the Lung" Cancers 14, no. 1: 177. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14010177