
Is Laterality Prognostic in Resected KRAS-Mutated Colorectal Liver Metastases? A Systematic Review and Meta-Analysis

 , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Objective
2.2. Data Sources and Search Strategies
2.3. Inclusion Criteria
2.4. Data Extraction
2.5. Statistical Analysis
2.5.1. Sensitivity Analysis
2.5.2. Bias Assessment
2.5.3. Publication Bias
2.6. Statistical Packages
3. Results
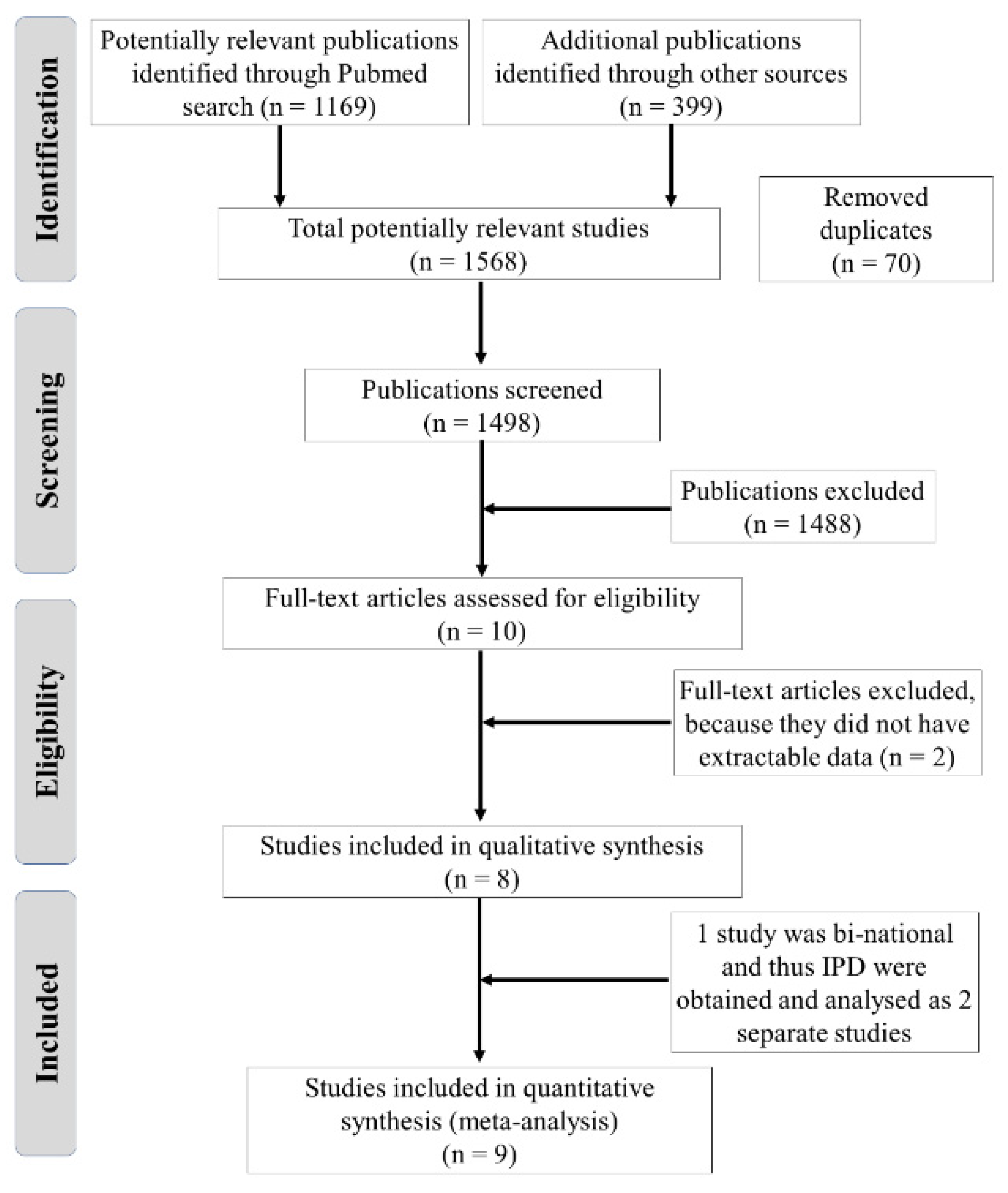
3.1. Study Selection
3.2. Study Characteristics
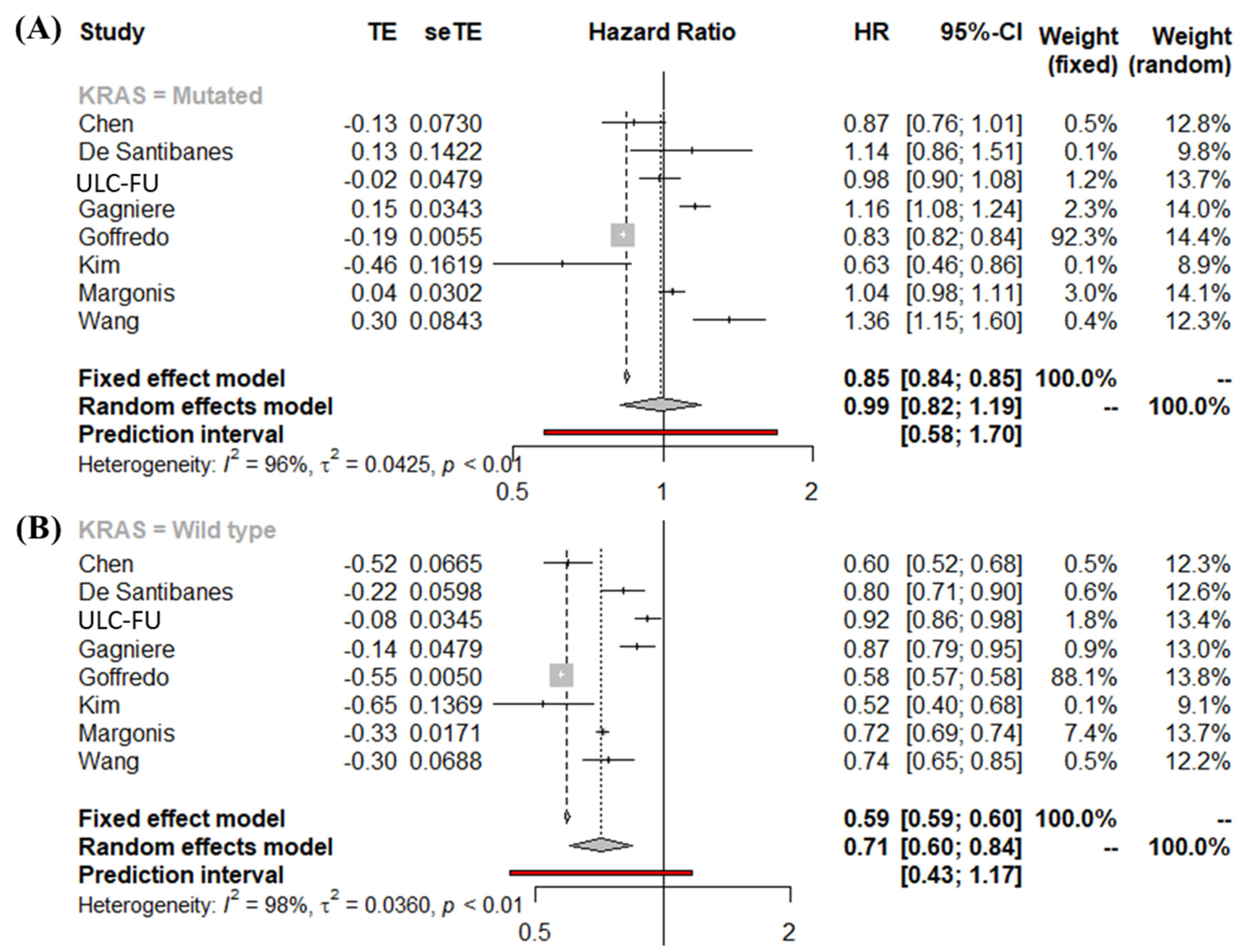
3.3. Meta-Analysis of Overall Survival Stratified by KRAS Mutational Status Using the First Definition of PTL
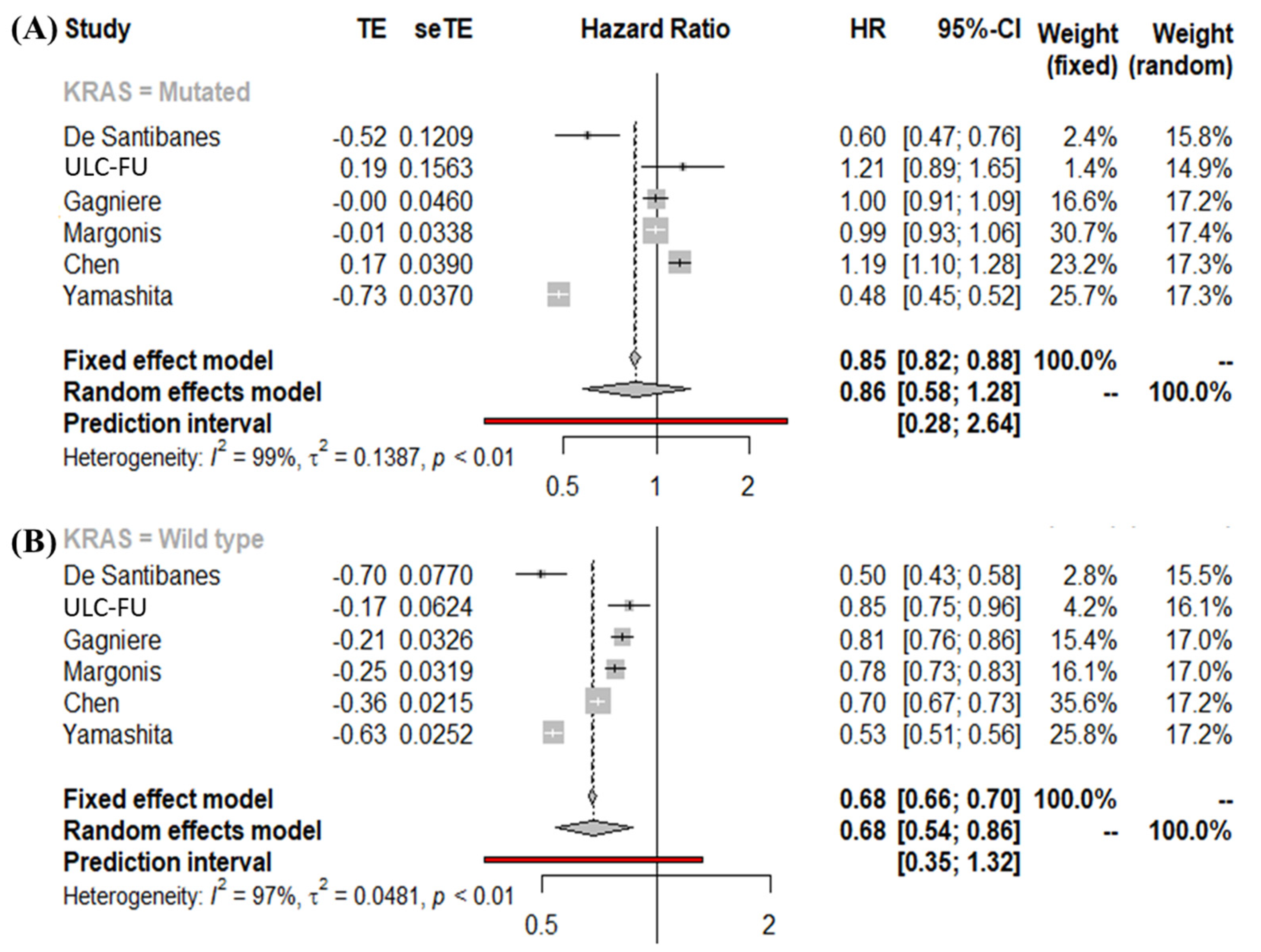
3.4. Meta-Analysis of Overall Survival Stratified by KRAS Mutational Status Using the Second Definition of PTL
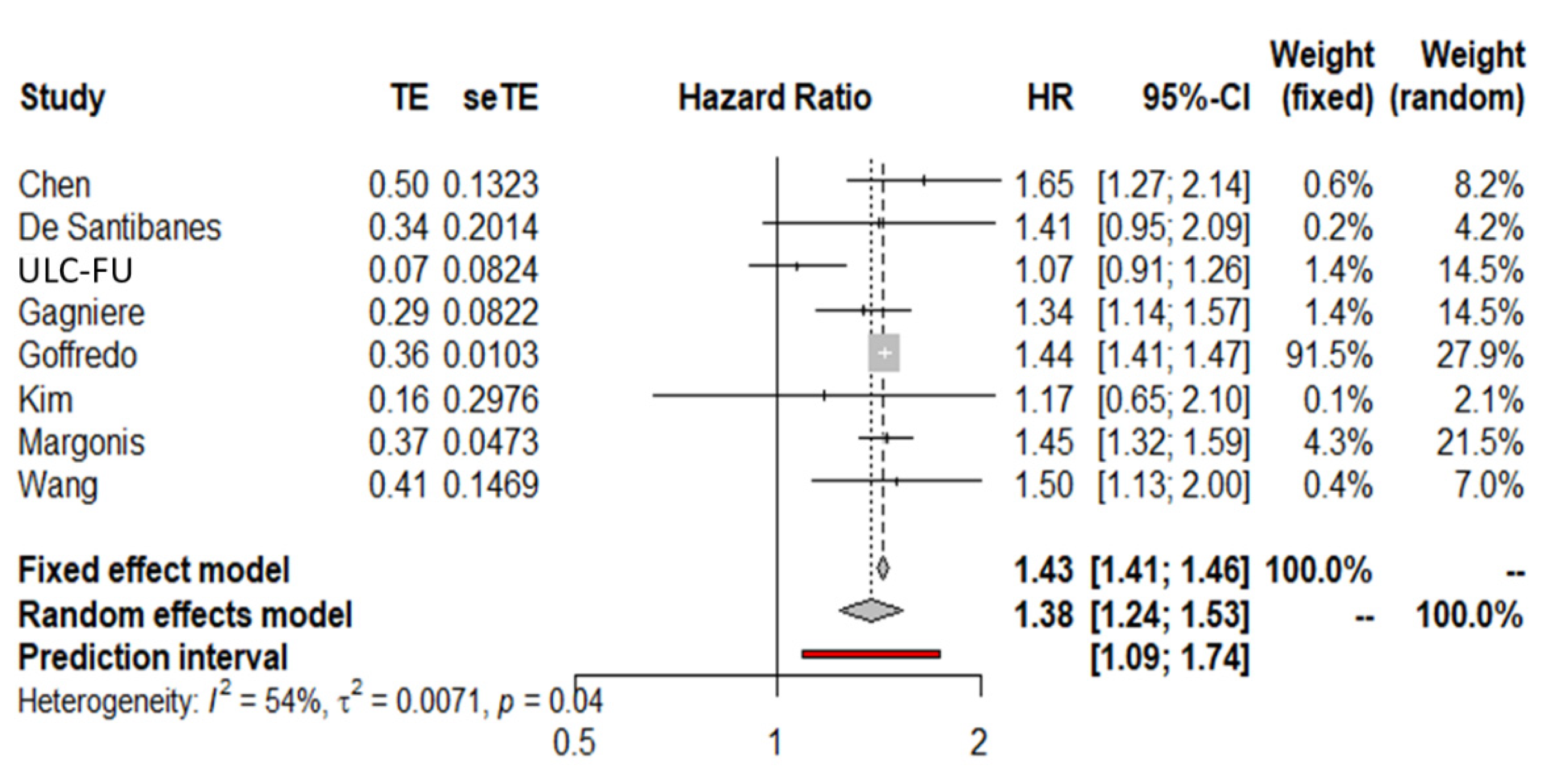
3.5. Meta-Analysis of Overall Survival Interaction Terms (MA-IT) Using the First Definition of PTL
3.6. Meta-Analysis of Overall Survival Interaction Terms (MA-IT) Using the Second Definition of PTL
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Loree, J.; Pereira, A.; Lam, M.; Willauer, A.; Raghav, K.; Dasari, A.; Morris, V.K.; Advani, S.M.; Menter, D.G.; Eng, C.; et al. Classifying Colorectal Cancer by Tumor Location Rather than Sidedness Highlights a Continuum in Mutation Profiles and Consensus Molecular Subtypes. Clin. Cancer Res. 2018, 24, 1062–1072. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnold, D.; Lueza, B.; Douillard, J.-Y.; Peeters, M.; Lenz, H.-J.; Venook, A.; Heinemann, V.; Van Cutsem, E.; Pignon, J.-P.; Tabernero, J.; et al. Prognostic and predictive value of primary tumour side in patients with RAS wild-type metastatic colorectal cancer treated with chemotherapy and EGFR directed antibodies in six randomized trials. Ann. Oncol. 2017, 28, 1713–1729. [Google Scholar] [CrossRef] [PubMed]
- Cremolini, C.; Antoniotti, C.; Lonardi, S.; Bergamo, F.; Cortesi, E.; Tomasello, G.; Moretto, R.; Ronzoni, M.; Racca, P.; Loupakis, F.; et al. Primary tumor sidedness and benefit from FOLFOXIRI plus bevacizumab as initial therapy for metastatic colorectal cancer. Retrospective analysis of the TRIBE trial by GONO. Ann. Oncol. 2018, 29, 1528–1534. [Google Scholar] [CrossRef]
- Sasaki, K.; Andreatos, N.; Margonis, G.A.; He, J.; Weiss, M.; Johnston, F.; Wolfgang, C.; Antoniou, E.; Pikoulis, E.; Pawlik, T.M. The prognostic implications of primary colorectal tumor location on recurrence and overall survival in patients undergoing resection for colorectal liver metastasis. J. Surg. Oncol. 2016, 114, 803–809. [Google Scholar] [CrossRef] [PubMed]
- Creasy, J.M.; Sadot, E.; Koerkamp, B.G.; Chou, J.F.; Gonen, M.; Kemeny, N.E.; Saltz, L.B.; Balachandran, V.P.; Kingham, T.P.; DeMatteo, R.P.; et al. The Impact of Primary Tumor Location on Long-Term Survival in Patients Undergoing Hepatic Resection for Metastatic Colon Cancer. Ann. Surg. Oncol. 2017, 25, 431–438. [Google Scholar] [CrossRef]
- Scherman, P.; Syk, I.; Holmberg, E.; Naredi, P.; Rizell, M. Influence of primary tumour and patient factors on survival in patients undergoing curative resection and treatment for liver metastases from colorectal cancer. BJS Open 2020, 4, 118–132. [Google Scholar] [CrossRef] [Green Version]
- Wang, K.; Xu, D.; Yan, X.-L.; Poston, G.; Xing, B.-C. The impact of primary tumour location in patients undergoing hepatic resection for colorectal liver metastasis. Eur. J. Surg. Oncol. (EJSO) 2018, 44, 771–777. [Google Scholar] [CrossRef]
- Wang, X.-Y.; Zhang, R.; Wang, Z.; Geng, Y.; Lin, J.; Ma, K.; Zuo, J.-L.; Lu, L.; Zhang, J.-B.; Zhu, W.-W.; et al. Meta-analysis of the association between primary tumour location and prognosis after surgical resection of colorectal liver metastases. Br. J. Surg. 2019, 106, 1747–1760. [Google Scholar] [CrossRef]
- Margonis, G.A.; Amini, N.; Buettner, S.; Kim, Y.; Wang, J.; Andreatos, N.; Wagner, D.; Sasaki, K.; Beer, A.; Kamphues, C.; et al. The Prognostic Impact of Primary Tumor Site Differs According to the KRAS Mutational Status: A Study By the International Genetic Consortium for Colorectal Liver Metastasis. Ann. Surg. 2021, 273, 1165–1172. [Google Scholar] [CrossRef]
- Yamashita, S.; Brudvik, K.W.; Kopetz, S.; Maru, D.; Clarke, C.N.; Passot, G.; Conrad, C.; Chun, Y.S.; Aloia, T.A.; Vauthey, J.-N. Embryonic Origin of Primary Colon Cancer Predicts Pathologic Response and Survival in Patients Undergoing Resection for Colon Cancer Liver Metastases. Ann. Surg. 2018, 267, 514–520. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Guyot, P.; Ades, A.E.; Ouwens, M.J.N.M.; Welton, N.J. Enhanced secondary analysis of survival data: Reconstructing the data from published Kaplan-Meier survival curves. BMC Med. Res. Methodol. 2012, 12, 9. [Google Scholar] [CrossRef] [Green Version]
- Seide, S.E.; Röver, C.; Friede, T. Likelihood-based random-effects meta-analysis with few studies: Empirical and simulation studies. BMC Med. Res. Methodol. 2019, 19, 16. [Google Scholar] [CrossRef] [PubMed]
- IntHout, J.; Ioannidis, J.P.; Borm, G.F. The Hartung-Knapp-Sidik-Jonkman method for random effects meta-analysis is straightforward and considerably outperforms the standard DerSimonian-Laird method. BMC Med. Res. Methodol. 2014, 14, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IntHout, J.; Ioannidis, J.P.; Rovers, M.M.; Goeman, J.J. Plea for routinely presenting prediction intervals in meta-analysis. BMJ Open 2016, 6, e010247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Sutton, A.J.; Ioannidis, J.P.A.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 343, d4002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goffredo, P.; Utria, A.F.; Beck, A.C.; Chun, Y.S.; Howe, J.; Weigel, R.J.; Vauthey, J.-N.; Hassan, I. The Prognostic Impact of KRAS Mutation in Patients Having Curative Resection of Synchronous Colorectal Liver Metastases. J. Gastrointest. Surg. 2018, 23, 1957–1963. [Google Scholar] [CrossRef]
- Gagnière, J.; Dupré, A.; Gholami, S.S.; Pezet, D.; Boerner, T.; Gönen, M.; Kingham, T.P.; Allen, P.J.; Balachandran, V.P.; De Matteo, R.P.; et al. Is Hepatectomy Justified for BRAF Mutant Colorectal Liver Metastases? A Multi-institutional Analysis of 1497 Patients. Ann. Surg. 2020, 271, 147–154. [Google Scholar] [CrossRef]
- Kim, H.S.; Lee, J.M.; Kim, H.S.; Yang, S.Y.; Han, Y.D.; Cho, M.S.; Hur, H.; Min, B.S.; Lee, K.Y.; Kim, N.K. Prognosis of Synchronous Colorectal Liver Metastases After Simultaneous Curative-Intent Surgery According to Primary Tumor Location and KRAS Mutational Status. Ann. Surg. Oncol. 2020, 27, 5150–5158. [Google Scholar] [CrossRef]
- Chen, T.-H.; Chen, W.-S.; Jiang, J.-K.; Yang, S.-H.; Wang, H.-S.; Chang, S.-C.; Lan, Y.-T.; Lin, C.-C.; Lin, H.-H.; Huang, S.-C.; et al. Effect of Primary Tumor Location on Postmetastasectomy Survival in Patients with Colorectal Cancer Liver Metastasis. J. Gastrointest. Surg. 2021, 25, 650–661. [Google Scholar] [CrossRef]
- O’Connor, J.M.; Sanchez Loria, F.; Ardiles, V.; Grondona, J.; Sanchez, P.; Andriani, O.; Fauda, M.; Brancato, F.; Huertas, E.; Alvarez, F.; et al. Prognostic impact of K-RAS mutational status and primary tumor location in patients undergoing resection for colorectal cancer liver metastases: An update. Future Oncol. 2019, 15, 3149–3157. [Google Scholar] [CrossRef] [PubMed]
- Kamphues, C.; Kadowaki, S.; Amini, N.; Berg, I.V.D.; Wang, J.; Andreatos, N.; Sakamoto, Y.; Ogura, T.; Kakuta, M.; Pikouli, A.; et al. The interplay of KRAS mutational status with tumor laterality in non-metastatic colorectal cancer: An international, multi-institutional study in patients with known KRAS, BRAF, and MSI status. J. Surg. Oncol. 2021, 123, 1005–1014. [Google Scholar] [CrossRef] [PubMed]
- Brudvik, K.W.; Kopetz, S.; Li, L.; Conrad, C.; Aloia, T.A.; Vauthey, J. Meta-analysis of KRAS mutations and survival after resection of colorectal liver metastases. Br. J. Surg. 2015, 102, 1175–1183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, J.; Cohen, R.; Jin, Z.; Liu, H.; Pederson, L.; Adams, R.; Grothey, A.; Maughan, T.S.; Venook, A.; Van Cutsem, E.; et al. Prognostic and Predictive Impact of Primary Tumor Sidedness for Previously Untreated Advanced Colorectal Cancer. JNCI J. Natl. Cancer Inst. 2021, 113, 1705–1713. [Google Scholar] [CrossRef]
- Cavallaro, P.; Bordeianou, L.; Stafford, C.; Clark, J.; Berger, D.; Cusack, J.; Kunitake, H.; Francone, T.; Ricciardi, R. Impact of Single-organ Metastasis to the Liver or Lung and Genetic Mutation Status on Prognosis in Stage IV Colorectal Cancer. Clin. Color. Cancer 2019, 19, e8–e17. [Google Scholar] [CrossRef]
- Kawaguchi, Y.; Kopetz, S.; Newhook, T.E.; De Bellis, M.; Chun, Y.S.; Tzeng, C.-W.D.; Aloia, T.A.; Vauthey, J.-N. Mutation Status of RAS, TP53, and SMAD4 is Superior to Mutation Status of RAS Alone for Predicting Prognosis after Resection of Colorectal Liver Metastases. Clin. Cancer Res. 2019, 25, 5843–5851. [Google Scholar] [CrossRef]
- Datta, J.; Smith, J.J.; Chatila, W.K.; McAuliffe, J.C.; Kandoth, C.; Vakiani, E.; Frankel, T.L.; Ganesh, K.; Wasserman, I.; Lipsyc-Sharf, M.; et al. Coaltered Ras/B-raf and TP53 Is Associated with Extremes of Survivorship and Distinct Patterns of Metastasis in Patients with Metastatic Colorectal Cancer. Clin. Cancer Res. 2020, 26, 1077–1085. [Google Scholar] [CrossRef]
- Nordlinger, B.; Sorbye, H.; Glimelius, B.; Poston, G.J.; Schlag, P.M.; Rougier, P.; Bechstein, W.O.; Primrose, J.N.; Walpole, E.T.; Finch-Jones, M.; et al. Perioperative chemotherapy with FOLFOX4 and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC Intergroup trial 40983): A randomised controlled trial. Lancet 2008, 371, 1007–1016. [Google Scholar] [CrossRef] [Green Version]
- Santini, D.; Loupakis, F.; Vincenzi, B.; Floriani, I.; Stasi, I.; Canestrari, E.; Rulli, E.; Maltese, P.E.; Andreoni, F.; Masi, G.; et al. High Concordance of KRAS Status Between Primary Colorectal Tumors and Related Metastatic Sites: Implications for Clinical Practice. Oncologist 2008, 13, 1270–1275. [Google Scholar] [CrossRef]
- Margonis, G.A.; Andreatos, N.; Kreis, M.E.; D’Angelica, M. The Interplay of Primary Tumor Location and KRAS Mutation Status in Patients with Synchronous Colorectal Cancer Liver Metastases: Current Data and Unanswered Questions. Ann. Surg. Oncol. 2020, 27, 4864–4866. [Google Scholar] [CrossRef]
- Amram, M.; Dunn, J.; Zhuo, Y.D. Optimal Policy Trees. arXiv 2020, arXiv:2012.02279. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Characteristics | Yamashita et al. [10] | Wang et al. [7] | Goffredo et al. [18] | Gagniere et al. [19] | Margonis et al. [9] | Kim et al. [20] | Chen et al. [21] | De Santibanes et al. [22] | ULC—FU * |
|---|---|---|---|---|---|---|---|---|---|
| Publication year | 2018 | 2018 | 2018 | 2018 | 2019 | 2020 | 2020 | 2019 | 2018 |
| Country | USA | China | USA | USA | USA | South Korea | Taiwan | Argentina | France |
| Study type | Single | Single | Population | Multicenter | Multicenter | Single | Single | Population | Single |
| Retrospective Design | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Interval of data collection | Nov. 1990–Feb. 2015 | Jan. 2002–Dec. 2015 | Jan. 2010–Dec. 2015 | Jan. 2001–Dec. 2016 | Jan. 2000–Dec. 2016 | Jan. 2006–Dec. 2015 | NR | NR | Jan. 2001–Dec. 2016 |
| Total patients | 725 | 420 a | 2665 | 775 | 1137 b | 227 | 336 c | 595 d | 695 |
| Median FU (months) | 27 | 26 | NR | 53.1 | 26.13 | 43.4 | 39.5 | 16.73 | 46.13 |
| KRAS mutated † | 262 | 97 | 1116 | 299 | 297 | 78 | 124 | 147 | 304 |
| Right/Left | 92/170 | 29/68 | 651/465 | 112/187 | 124/173 | 21/57 | 41/83 | 31/116 | 180/124 |
| KRAS wild type | 463 | 233 | 1539 | 476 | 840 | 149 | 212 | 448 | 391 |
| Right/Left | 146/317 | 38/195 | 541/998 | 99/377 | 200/640 | 20/129 | 28/184 | 82/366 | 240/151 |
| Patient Characteristics | Yamashita et al. [10] | Wang et al. [7] | Goffredo et al. [18] | Gagniere et al. [19] | Margonis et al. [9] | Kim et al. [20] | Chen et al. [21] | O Connoret al. [22] | ULC—FU * |
|---|---|---|---|---|---|---|---|---|---|
| Age, median [interquartile range]/Age, mean ± SD | 58 (50–65) | NR | NR | NA | 61 (51–68) | NR | NR | 67 (59–75) | 59.6 (51.6–67.9) |
| Right | 56 (49–64) | 58.5 (49.7–65.0) | NR | NA | 63.8 (55.0–71.5) | 59.8 ± 12.2 | 63.9 (61.2–66.7) | 70 (63.5–77.5) | 59.3 (51.3–67.9) |
| Left | 58 (50–66) | 57.0 (49.7–64.0) | NR | NA | 59.1 (49.7–66.6) | 57.6 ± 10.3 | 61 (59–63) | 67 (58–74) | 60.3 (52.0–68.0) |
| Gender (females %) | 41.8% | 38.8% | 46.2% | NA | 36% | 34.4% | 35.2% | 41.4% | 42.9% |
| Right | 44.5% | 53% | NR | NA | 43.8% | 43.9% | 44% | 43.1% | 49% |
| Left | 40.4% | 35% | NR | NA | 33% | 32.3% | 33% | 43.2% | 35% |
| Presentation of liver metastasis (synchronous %) | 74.1% | 51.2% | 100% | 64.4% | 48.2% | 100% | 63.2% | 62.4% | 53.4% |
| Right | 76% | 52.9% | 100% | 63.9% | 46.4% | 100% | 64.1% | 63.2% | 55% |
| Left | 73.1% | 50.8% | 100% | 62.6% | 49% | 100% | 62.1% | 70.8% | 54.8% |
| Number of liver metastases Median [IQR] OR Multiple % | Reported but on different a | NR | NR | 2 (1–4) | 2 (1–3) | Reported but on different b | Reported but on different c | 3 (1–4) | 2 (1–3) |
| Right | 2 (1–3.5) | NR | 2 (1–3) | 2 (1–3) | NR | NR | 3 (1–4) | 2 (1–3) | |
| Left | 2 (1–4) | NR | 2 (1–4) | 2 (1–4) | NR | NR | 3 (1–4) | 2 (1–3) | |
| Concurrent extrahepatic disease | NR | 11.9% | NR | 8.7% | 10.8% | NR | 0% | 18.3% | 7.19 |
| Right | 12.7% | NR | 9.5% | 11.8% | NR | 0% | 18% | 5.7% | |
| Left | 11.6% | NR | 8.2% | 10.5% | NR | 0% | 21.1% | 8.2% | |
| R0 resections (n, %) | 92.8% | NR | 85.7% | 89.4% | 80.2% | 79.7% | 98.1% | 98.7% | 95.2% |
| Right | 91.6% | NR | NR | 89.6% | 79.8% | 85.4% | 97.3% | 98.9% | 95.3% |
| Left | 93.4% | NR | NR | 91.5% | 81.3% | 78.5% | 99.3% | 98.1% | 95.2% |
| Modern prehepatectomy chemotherapy | 99% | NR | NR | 65% | NR | 23% | 41% | 91.9% | |
| Right | 99% | NR | NR | NR | 59% | NR | 20% | 43.4% | 91.9% |
| Left | 100% | NR | NR | NR | 67.5% | NR | 24% | 40.2% | 91.6% |
| Biologic agents | 55% | NR | NR | NR | 30.7% | 42.3% | 10.2% | 32.6% | 29.3% |
| Right | 55% | NR | NR | NR | 28% | 31.7% | 8% | 35.4% | 24% |
| Left | 55% | NR | NR | NR | 31.7% | 44.6% | 13% | 32% | 37% |
| Major response to chemotherapy † | 68% | NR | NR | NR | NR | NR | NR | NR | NR |
| Right | 62% | NR | NR | NR | NR | NR | NR | NR | NR |
| Left | 71% | NR | NR | NR | NR | NR | NR | NR | NR |
| Adjuvant chemotherapy | 66.2% | 56.7% | 91% | 93.2% | 58.3% | 91.6% | 85% | 30.2% | 96.5% |
| Right | 65.9% | 45.3% | NR | 92.3% | 56.5% | 85.4% | 82.3% | 28.6% | 93.6% |
| Left | 66.3% | 59.6% | NR | 93.6% | 62.8% | 93% | 88.8% | 31% | 97.1% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belias, M.; Sasaki, K.; Wang, J.; Andreatos, N.; Kamphues, C.; Kyriakos, G.; Seeliger, H.; Beyer, K.; Kreis, M.E.; Margonis, G.A. Is Laterality Prognostic in Resected KRAS-Mutated Colorectal Liver Metastases? A Systematic Review and Meta-Analysis. Cancers 2022, 14, 799. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14030799
Belias M, Sasaki K, Wang J, Andreatos N, Kamphues C, Kyriakos G, Seeliger H, Beyer K, Kreis ME, Margonis GA. Is Laterality Prognostic in Resected KRAS-Mutated Colorectal Liver Metastases? A Systematic Review and Meta-Analysis. Cancers. 2022; 14(3):799. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14030799
Chicago/Turabian StyleBelias, Michail, Kazunari Sasaki, Jane Wang, Nikolaos Andreatos, Carsten Kamphues, Georgios Kyriakos, Hendrik Seeliger, Katharina Beyer, Martin E. Kreis, and Georgios Antonios Margonis. 2022. "Is Laterality Prognostic in Resected KRAS-Mutated Colorectal Liver Metastases? A Systematic Review and Meta-Analysis" Cancers 14, no. 3: 799. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14030799