
Real-World Time on Treatment with First-Line Pembrolizumab Monotherapy for Advanced NSCLC with PD-L1 Expression ≥ 50%: 3-Year Follow-Up Data

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
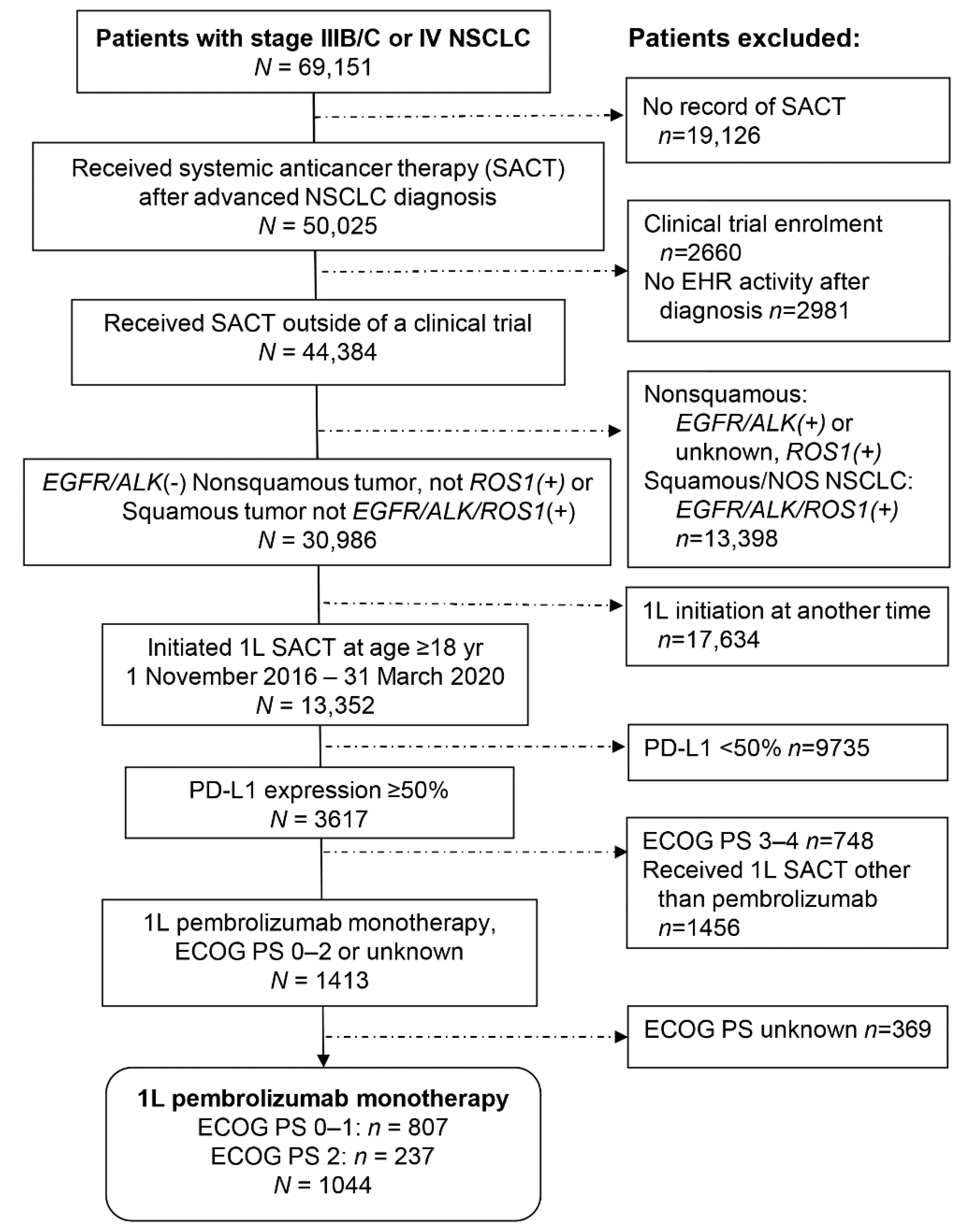
2.1. Patients and Data Source
2.2. Assessments and Statistical Analyses
3. Results
3.1. Patient Characteristics
3.2. First-Line Treatment with Pembrolizumab Monotherapy: Real-World Time on Treatment
3.3. Subanalysis of rwToT by KRAS Mutation Status for Nonsquamous NSCLC, PS 0–1
3.4. Sensitivity Analysis Including Only Patients with Stage-IV NSCLC at Diagnosis
3.5. Subsequent Systemic Anticancer Therapy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Cancer Institute: Surveillance, E. and End Results Program (SEER). Cancer Stat Facts: Lung and Bronchus Cancer. Available online: https://seer.cancer.gov/statfacts/html/lungb.html (accessed on 3 February 2022).
- Howlader, N.; Forjaz, G.; Mooradian, M.J.; Meza, R.; Kong, C.Y.; Cronin, K.A.; Mariotto, A.B.; Lowy, D.R.; Feuer, E.J. The effect of advances in lung-cancer treatment on population mortality. N. Engl. J. Med. 2020, 383, 640–649. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Grant, M.J.; Herbst, R.S.; Goldberg, S.B. Selecting the optimal immunotherapy regimen in driver-negative metastatic NSCLC. Nat. Rev. Clin. Oncol. 2021, 18, 625–644. [Google Scholar] [CrossRef] [PubMed]
- Steuer, C.E.; Ramalingam, S.S. Advances in immunotherapy and implications for current practice in non-small-cell lung cancer. JCO Oncol. Pract. 2021, 17, 662–668. [Google Scholar] [CrossRef] [PubMed]
- Calles, A.; Riess, J.W.; Brahmer, J.R. Checkpoint blockade in lung cancer with driver mutation: Choose the road wisely. Am. Soc. Clin. Oncol. Educ. Book 2020, 40, 372–384. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology: Non-Small Cell Lung Cancer, Version 1.2022—7 December 2021. Available online: https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdf (accessed on 3 February 2022).
- El Osta, B.; Behera, M.; Kim, S.; Berry, L.D.; Sica, G.; Pillai, R.N.; Owonikoko, T.K.; Kris, M.G.; Johnson, B.E.; Kwiatkowski, D.J.; et al. Characteristics and outcomes of patients with metastatic KRAS-mutant lung adenocarcinomas: The Lung Cancer Mutation Consortium experience. J. Thorac. Oncol. 2019, 14, 876–889. [Google Scholar] [CrossRef] [PubMed]
- Mazieres, J.; Drilon, A.; Lusque, A.; Mhanna, L.; Cortot, A.B.; Mezquita, L.; Thai, A.A.; Mascaux, C.; Couraud, S.; Veillon, R.; et al. Immune checkpoint inhibitors for patients with advanced lung cancer and oncogenic driver alterations: Results from the IMMUNOTARGET registry. Ann. Oncol. 2019, 30, 1321–1328. [Google Scholar] [CrossRef]
- Herbst, R.S.; Lopes, G.; Kowalski, D.M.; Kasahara, K.; Wu, Y.L.; De Castro, G.; Cho, B.C.; Turna, H.Z.; Cristescu, R.; Aurora-Garg, D.; et al. LBA4 Association of KRAS mutational status with response to pembrolizumab monotherapy given as first-line therapy for PD-L1-positive advanced non-squamous NSCLC in Keynote-042. Ann. Oncol. 2019, 30, xi63–xi64. [Google Scholar] [CrossRef]
- Noordhof, A.L.; Damhuis, R.A.M.; Hendriks, L.E.L.; de Langen, A.J.; Timens, W.; Venmans, B.J.W.; van Geffen, W.H. Prognostic impact of KRAS mutation status for patients with stage IV adenocarcinoma of the lung treated with first-line pembrolizumab monotherapy. Lung Cancer 2021, 155, 163–169. [Google Scholar] [CrossRef]
- Reck, M.; Rodriguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csoszi, T.; Fulop, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [Green Version]
- Reck, M.; Rodriguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csoszi, T.; Fulop, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Updated analysis of KEYNOTE-024: Pembrolizumab versus platinum-based chemotherapy for advanced non-small-cell lung cancer with PD-L1 tumor proportion score of 50% or greater. J. Clin. Oncol. 2019, 37, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Rodriguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csoszi, T.; Fulop, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Five-year outcomes with pembrolizumab versus chemotherapy for metastatic non-small-cell lung cancer with PD-L1 tumor proportion score ≥ 50%. J. Clin. Oncol. 2021, 39, 2339–2349. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.S.; Wong, J.L. Using oncology real-world evidence for quality improvement and discovery: The case for ASCO’s CancerLinQ. Future Oncol. 2018, 14, 5–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berger, M.L.; Curtis, M.D.; Smith, G.; Harnett, J.; Abernethy, A.P. Opportunities and challenges in leveraging electronic health record data in oncology. Future Oncol. 2016, 12, 1261–1274. [Google Scholar] [CrossRef] [PubMed]
- Friends of Cancer Research. Establishing a Framework to Evaluate Real-World Endpoints. Available online: https://www.focr.org/publications/establishing-framework-evaluate-real-world-endpoints (accessed on 3 February 2022).
- Blumenthal, G.M.; Gong, Y.; Kehl, K.; Mishra-Kalyani, P.; Goldberg, K.B.; Khozin, S.; Kluetz, P.G.; Oxnard, G.R.; Pazdur, R. Analysis of time-to-treatment discontinuation of targeted therapy, immunotherapy, and chemotherapy in clinical trials of patients with non-small-cell lung cancer. Ann. Oncol. 2019, 30, 830–838. [Google Scholar] [CrossRef]
- Stewart, M.; Norden, A.D.; Dreyer, N.; Henk, H.J.; Abernethy, A.P.; Chrischilles, E.; Kushi, L.; Mansfield, A.S.; Khozin, S.; Sharon, E.; et al. An exploratory analysis of real-world end points for assessing outcomes among immunotherapy-treated patients with advanced non-small-cell lung cancer. JCO Clin. Cancer Inform. 2019, 3, 1–15. [Google Scholar] [CrossRef]
- Khozin, S.; Miksad, R.A.; Adami, J.; Boyd, M.; Brown, N.R.; Gossai, A.; Kaganman, I.; Kuk, D.; Rockland, J.M.; Pazdur, R.; et al. Real-world progression, treatment, and survival outcomes during rapid adoption of immunotherapy for advanced non-small cell lung cancer. Cancer 2019, 125, 4019–4032. [Google Scholar] [CrossRef] [Green Version]
- Kehl, K.L.; Riely, G.J.; Lepisto, E.M.; Lavery, J.A.; Warner, J.L.; LeNoue-Newton, M.L.; Sweeney, S.M.; Rudolph, J.E.; Brown, S.; Yu, C.; et al. Correlation between surrogate end points and overall survival in a multi-institutional clinicogenomic cohort of patients with non-small cell lung or colorectal cancer. JAMA Netw. Open 2021, 4, e2117547. [Google Scholar] [CrossRef]
- Velcheti, V.; Chandwani, S.; Chen, X.; Pietanza, M.C.; Burke, T. First-line pembrolizumab monotherapy for metastatic PD-L1-positive NSCLC: Real-world analysis of time on treatment. Immunotherapy 2019, 11, 889–901. [Google Scholar] [CrossRef]
- Flatiron Health. Flatiron Health Database. Available online: https://flatiron.com/real-world-evidence/ (accessed on 3 February 2022).
- Abernethy, A.P.; Gippetti, J.; Parulkar, R.; Revol, C. Use of electronic health record data for quality reporting. J. Oncol. Pract. 2017, 13, 530–534. [Google Scholar] [CrossRef]
- Griffith, S.D.; Tucker, M.; Bowser, B.; Calkins, G.; Chang, C.J.; Guardino, E.; Khozin, S.; Kraut, J.; You, P.; Schrag, D.; et al. Generating real-world tumor burden endpoints from electronic health record data: Comparison of RECIST, radiology-anchored, and clinician-anchored approaches for abstracting real-world progression in non-small cell lung cancer. Adv. Ther. 2019, 36, 2122–2136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, N.F.; Perera, R.; Harper, S.; Rose, P.W. Adaptation and validation of the Charlson Index for Read/OXMIS coded databases. BMC Fam. Pract. 2010, 11, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velcheti, V.; Chandwani, S.; Chen, X.; Pietanza, M.C.; Piperdi, B.; Burke, T. Outcomes of first-line pembrolizumab monotherapy for PD-L1-positive (TPS ≥ 50%) metastatic NSCLC at US oncology practices. Immunotherapy 2019, 11, 1541–1554. [Google Scholar] [CrossRef]
- Pocock, S.J.; Clayton, T.C.; Altman, D.G. Survival plots of time-to-event outcomes in clinical trials: Good practice and pitfalls. Lancet 2002, 359, 1686–1689. [Google Scholar] [CrossRef]
- Latimer, N.R. Survival analysis for economic evaluations alongside clinical trials--extrapolation with patient-level data: Inconsistencies, limitations, and a practical guide. Med. Decis. Mak. 2013, 33, 743–754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mok, T.S.K.; Wu, Y.L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G., Jr.; Srimuninnimit, V.; Laktionov, K.K.; Bondarenko, I.; et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): A randomised, open-label, controlled, phase 3 trial. Lancet 2019, 393, 1819–1830. [Google Scholar] [CrossRef]
- Khozin, S.; Abernethy, A.P.; Nussbaum, N.C.; Zhi, J.; Curtis, M.D.; Tucker, M.; Lee, S.E.; Light, D.E.; Gossai, A.; Sorg, R.A.; et al. Characteristics of real-world metastatic non-small cell lung cancer patients treated with nivolumab and pembrolizumab during the year following approval. Oncologist 2018, 23, 328–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenei, K.; Meyers, D.E.; Prasad, V. The inclusion of women in global oncology drug trials over the past 20 years. JAMA Oncol. 2021, 7, 1569–1570. [Google Scholar] [CrossRef] [PubMed]
- Murthy, V.H.; Krumholz, H.M.; Gross, C.P. Participation in cancer clinical trials: Race-, sex-, and age-based disparities. JAMA 2004, 291, 2720–2726. [Google Scholar] [CrossRef]
- Stenehjem, D.; Lubinga, S.; Betts, K.A.; Tang, W.; Jenkins, M.; Yuan, Y.; Hartman, J.; Rao, S.; Lam, J.; Waterhouse, D. Treatment patterns in patients with metastatic non-small-cell lung cancer in the era of immunotherapy. Future Oncol. 2021, 17, 2940–2949. [Google Scholar] [CrossRef]
- Waterhouse, D.; Lam, J.; Betts, K.A.; Yin, L.; Gao, S.; Yuan, Y.; Hartman, J.; Rao, S.; Lubinga, S.; Stenehjem, D. Real-world outcomes of immunotherapy-based regimens in first-line advanced non-small cell lung cancer. Lung Cancer 2021, 156, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Herbst, R.S.; Giaccone, G.; de Marinis, F.; Reinmuth, N.; Vergnenegre, A.; Barrios, C.H.; Morise, M.; Felip, E.; Andric, Z.; Geater, S.; et al. Atezolizumab for first-line treatment of PD-L1-selected patients with NSCLC. N. Engl. J. Med. 2020, 383, 1328–1339. [Google Scholar] [CrossRef] [PubMed]
- Sezer, A.; Kilickap, S.; Gumus, M.; Bondarenko, I.; Ozguroglu, M.; Gogishvili, M.; Turk, H.M.; Cicin, I.; Bentsion, D.; Gladkov, O.; et al. Cemiplimab monotherapy for first-line treatment of advanced non-small-cell lung cancer with PD-L1 of at least 50%: A multicentre, open-label, global, phase 3, randomised, controlled trial. Lancet. 2021, 397, 592–604. [Google Scholar] [CrossRef]
- Skoulidis, F.; Goldberg, M.E.; Greenawalt, D.M.; Hellmann, M.D.; Awad, M.M.; Gainor, J.F.; Schrock, A.B.; Hartmaier, R.J.; Trabucco, S.E.; Gay, L.; et al. STK11/LKB1 Mutations and PD-1 inhibitor resistance in KRAS-mutant lung adenocarcinoma. Cancer Discov. 2018, 8, 822–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arbour, K.C.; Rizvi, H.; Plodkowski, A.J.; Hellmann, M.D.; Knezevic, A.; Heller, G.; Yu, H.A.; Ladanyi, M.; Kris, M.G.; Arcila, M.E.; et al. Treatment outcomes and clinical characteristics of patients with KRAS-G12C-mutant non-small cell lung cancer. Clin. Cancer Res. 2021, 27, 2209–2215. [Google Scholar] [CrossRef] [PubMed]
- Sun, L.; Davis, C.W.; Hwang, W.T.; Jeffries, S.; Sulyok, L.F.; Marmarelis, M.E.; Singh, A.P.; Berman, A.T.; Feigenberg, S.J.; Levin, W.; et al. Outcomes in patients with non-small-cell lung cancer with brain metastases treated with pembrolizumab-based therapy. Clin. Lung Cancer 2021, 22, 58–66.e53. [Google Scholar] [CrossRef] [PubMed]
- Di Federico, A.; De Giglio, A.; Parisi, C.; Gelsomino, F. STK11/LKB1 and KEAP1 mutations in non-small cell lung cancer: Prognostic rather than predictive? Eur. J. Cancer 2021, 157, 108–113. [Google Scholar] [CrossRef]
- Gkountakos, A.; Sartori, G.; Falcone, I.; Piro, G.; Ciuffreda, L.; Carbone, C.; Tortora, G.; Scarpa, A.; Bria, E.; Milella, M.; et al. PTEN in lung cancer: Dealing with the problem, building on new knowledge and turning the game around. Cancers 2019, 11, 1141. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | ECOG PS 0–1 N = 807 | ECOG PS 2 N = 237 |
|---|---|---|
| Men | 410 (50.8) | 118 (49.8) |
| Age, median (range), years | 72 (38–84) | 75 (48–84) |
| <75 years | 484 (60.0) | 116 (48.9) |
| ≥75 years | 323 (40.0) | 121 (51.1) |
| Race data available, N | 724 | 209 |
| White 1 | 566 (78.2) | 159 (76.1) |
| Black 1 | 68 (9.4) | 23 (11.0) |
| Asian 1 | 20 (2.8) | 1 (0.5) |
| Other race 1 | 70 (9.7) | 26 (12.4) |
| Current/former smoker | 747 (92.6) | 226 (95.4) |
| No smoking history | 60 (7.4) | 11 (4.6) |
| Charlson comorbidity index score, mean (SD) | 4.9 (3.1) | 5.4 (3.1) |
| Median (range) | 3 (0–14) | 4 (2–12) |
| NSCLC histology | ||
| Nonsquamous | 544 (67.4) | 170 (71.7) |
| Squamous | 220 (27.3) | 57 (24.1) |
| NSCLC histology NOS | 43 (5.3) | 10 (4.2) |
| NSCLC first diagnosed at stage IV | 566 (70.1) | 178 (75.1) |
| KRAS mutation status (nonsquamous only), N | 544 | 170 |
| Positive 2 | 164 (30.1) | 49 (28.8) |
| Wild-type | 166 (30.5) | 48 (28.2) |
| Indeterminate, unknown, pending, untested | 214 (39.3) | 73 (42.9) |
| Record of brain metastases 3 | 81 (10.0) | 27 (11.4) |
| Variable | ECOG PS 0–1 N = 807 | ECOG PS 2 N = 237 |
|---|---|---|
| Theoretical follow-up, median (range), mo 1 | 34.1 (12.0–52.7) | 33.5 (12.2–52.7) |
| Patient follow-up, median (range), mo 1 | 17.4 (<0.1–52.6) | 5.7 (<0.1–51.5) |
| Discontinued pembrolizumab, n (%) | 628 (77.8) | 207 (87.3) |
| rwToT, median (95% CI), mo | 7.4 (6.3–8.1) | 2.1 (1.4–2.8) |
| Restricted mean rwToT (95% CI), mo | ||
| Restricted to 12 months | 7.0 (6.7–7.3) | 4.3 (3.7–5.0) |
| Restricted to 24 months | 10.3 (9.7–11.0) | 5.9 (4.9–7.0) (Lognormal) |
| Restricted to 36 months | 12.4 (11.5–13.3) (Weibull) | 7.4 (6.0–9.0) (Lognormal) |
| Restricted to 48 months | 13.6 (12.6–14.8) (Weibull) | 8.5 (6.9–10.6) (Lognormal) |
| On-treatment rate, % (95% CI) 2 | ||
| At 12 months | 36.0 (32.6–39.3) | 20.8 (15.7–26.3) |
| At 24 months | 22.1 (19.1–25.3) | 9.9 (6.1–14.6) |
| At 36 months | 13.7 (10.9–16.9) | 6.1 (2.8–11.1) |
| At 48 months | 9.8 (6.7–13.6) | n/a |
| Variable | All Nonsquamous N = 544 | KRAS Positive N = 164 | KRAS Wild-Type N = 166 | KRAS Unknown N = 214 |
|---|---|---|---|---|
| Pembrolizumab rwToT | ||||
| Discontinued pembrolizumab, n (%) | 410 (75.4) | 126 (76.8) | 131 (78.9) | 153 (71.5) |
| rwToT, median (95% CI), mo | 7.6 (6.3–8.8) | 7.6 (6.3–10.6) | 7.0 (5.3–9.3) | 7.9 (4.8–10.8) |
| Restricted mean rwToT (95% CI), mo | ||||
| Restricted to 12 months | 7.1 (6.7–7.5) | 7.4 (6.7–8.1) | 6.9 (6.3–7.7) | 7.0 (6.3–7.7) |
| Restricted to 24 months | 10.7 (9.9–11.5) | 11.3 (9.9–12.8) | 10.3 (9.0–11.8) | 10.5 (9.3–11.8) |
| Restricted to 36 months | 13.0 (11.9–14.1) (Weibull) | 13.5 (11.6–15.6) (Weibull) | 12.2 (10.4–14.3) (Weibull) | 13.2 (11.4–15.2) (Weibull) |
| Restricted to 48 months | 14.5 (13.1–16.0) (Weibull) | 14.9 (12.6–17.7) (Weibull) | 13.4 (11.2–16.0) (Weibull) | 15.0 (12.7–17.6) (Weibull) |
| On-treatment rate, % (95% CI) 1 | ||||
| At 12 months | 37.1 (33.0–41.3) | 38.3 (30.8–45.8) | 35.1 (27.8–42.5) | 37.9 (31.2–44.7) |
| At 24 months | 24.6 (20.7–28.6) | 25.7 (18.8–33.1) | 23.0 (16.4–30.3) | 25.1 (18.9–31.7) |
| At 36 months | 16.5 (12.8–20.6) | 17.7 (11.2–25.4) | 12.5 (6.9–19.8) | 19.1 (13.2–26.0) |
| At 48 months | 10.6 (6.5–15.8) | n/a | 9.4 (4.4–16.6) | 17.5 (11.5–24.6) |
| Regimen by Treatment Line 1 | ECOG 0–1 N = 807 | ECOG 2 N = 237 |
|---|---|---|
| Systemic Therapy Line 2 | 263 (32.6) | 39 (16.5) |
| Anti-PD-1/PD-L1-based therapies | 105 (39.9) | 11 (28.2) |
| Anti-PD-1/PD-L1 monotherapy | 36 (34.3) | 3 (27.3) |
| Anti-PD-1/PD-L1 combination therapy | 69 (65.7) | 8 (72.7) |
| Anti-VEGF-based therapies | 25 (9.5) | 4 (10.3) |
| Platinum-based chemotherapy combinations | 88 (33.5) | 17 (43.6) |
| Nonplatinum-based chemotherapy combinations | 3 (1.1) | 0 |
| Single-agent chemotherapy | 29 (11.0) | 6 (15.4) |
| Other therapy | 13 (4.9) | 1 (2.6) |
| Systemic Therapy Line 3 | 91 (11.3) | 10 (4.2) |
| Anti-PD-1/PD-L1-based therapies | 34 (37.4) | 4 (40.0) |
| Anti-PD-1/PD-L1 monotherapy | 15 (44.1) | 2 (50.0) |
| Anti-PD-1/PD-L1 combination therapy | 19 (55.9) | 2 (50.0) |
| Anti-VEGF-based therapies | 12 (13.2) | 2 (20.0) |
| Platinum-based chemotherapy combinations | 13 (14.3) | 0 |
| Nonplatinum-based chemotherapy combinations | 1 (1.1) | 0 |
| Single-agent chemotherapy | 24 (26.4) | 3 (30.0) |
| Other therapy | 7 (7.7) | 1 (10.0) |
| Systemic Therapy Line 4 | 24 (3.0) | 4 (1.7) |
| Anti-PD-1/PD-L1-based therapies | 5 (20.8) | 1 (25.0) |
| Anti-PD-1/PD-L1 monotherapy | 1 (20.0) | 0 |
| Anti-PD-1/PD-L1 combination therapy | 4 (80.0) | 1 (100) |
| Anti-VEGF-based therapies | 4 (16.7) | 0 |
| Platinum-based chemotherapy combinations | 5 (20.8) | 0 |
| Single-agent chemotherapy | 8 (33.3) | 1 (25.0) |
| Other therapy | 2 (8.3) | 2 (50.0) |
| Systemic Therapy Line 5 | 7 (0.9) 2 | 1 (0.4) 3 |
| Anti-PD-1/PD-L1-based therapies | 3 (42.9) | 0 |
| Anti-PD-1/PD-L1 monotherapy | 2 (66.7) | 0 |
| Anti-PD-1/PD-L1 combination therapy | 1 (33.3) | 0 |
| Anti-VEGF-based therapies | 1 (14.3) | 0 |
| Platinum-based chemotherapy combinations | 1 (14.3) | 0 |
| Single-agent chemotherapy | 1 (14.3) | 1 (100) |
| Other therapy | 1 (14.3) | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Velcheti, V.; Hu, X.; Li, Y.; El-Osta, H.; Pietanza, M.C.; Burke, T. Real-World Time on Treatment with First-Line Pembrolizumab Monotherapy for Advanced NSCLC with PD-L1 Expression ≥ 50%: 3-Year Follow-Up Data. Cancers 2022, 14, 1041. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14041041
Velcheti V, Hu X, Li Y, El-Osta H, Pietanza MC, Burke T. Real-World Time on Treatment with First-Line Pembrolizumab Monotherapy for Advanced NSCLC with PD-L1 Expression ≥ 50%: 3-Year Follow-Up Data. Cancers. 2022; 14(4):1041. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14041041
Chicago/Turabian StyleVelcheti, Vamsidhar, Xiaohan Hu, Yeran Li, Hazem El-Osta, M. Catherine Pietanza, and Thomas Burke. 2022. "Real-World Time on Treatment with First-Line Pembrolizumab Monotherapy for Advanced NSCLC with PD-L1 Expression ≥ 50%: 3-Year Follow-Up Data" Cancers 14, no. 4: 1041. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14041041