
Effect of Neoadjuvant Chemotherapy on Complications, in-Hospital Mortality, Length of Stay and Total Hospital Costs in Bladder Cancer Patients Undergoing Radical Cystectomy

 ,
,  , ,
, ,  , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Data Source
2.2. Study Population
2.3. Outcomes of Interest
2.4. Patient and Hospital Characteristics
2.5. Statistical Analyses
3. Results
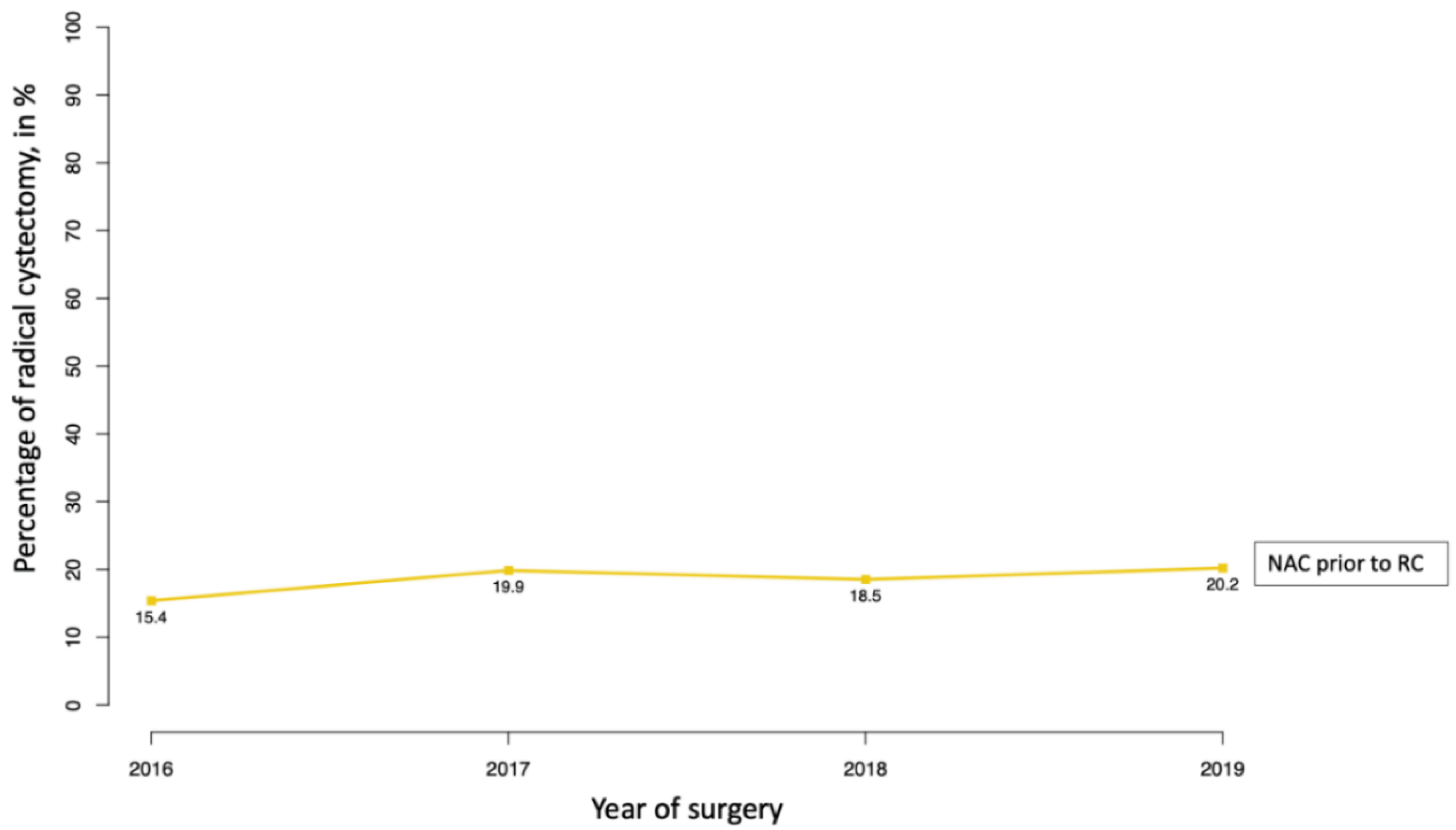
3.1. Patients’ Characteristics and Temporal Trends
3.2. Crude Rates of Outcomes of Interest
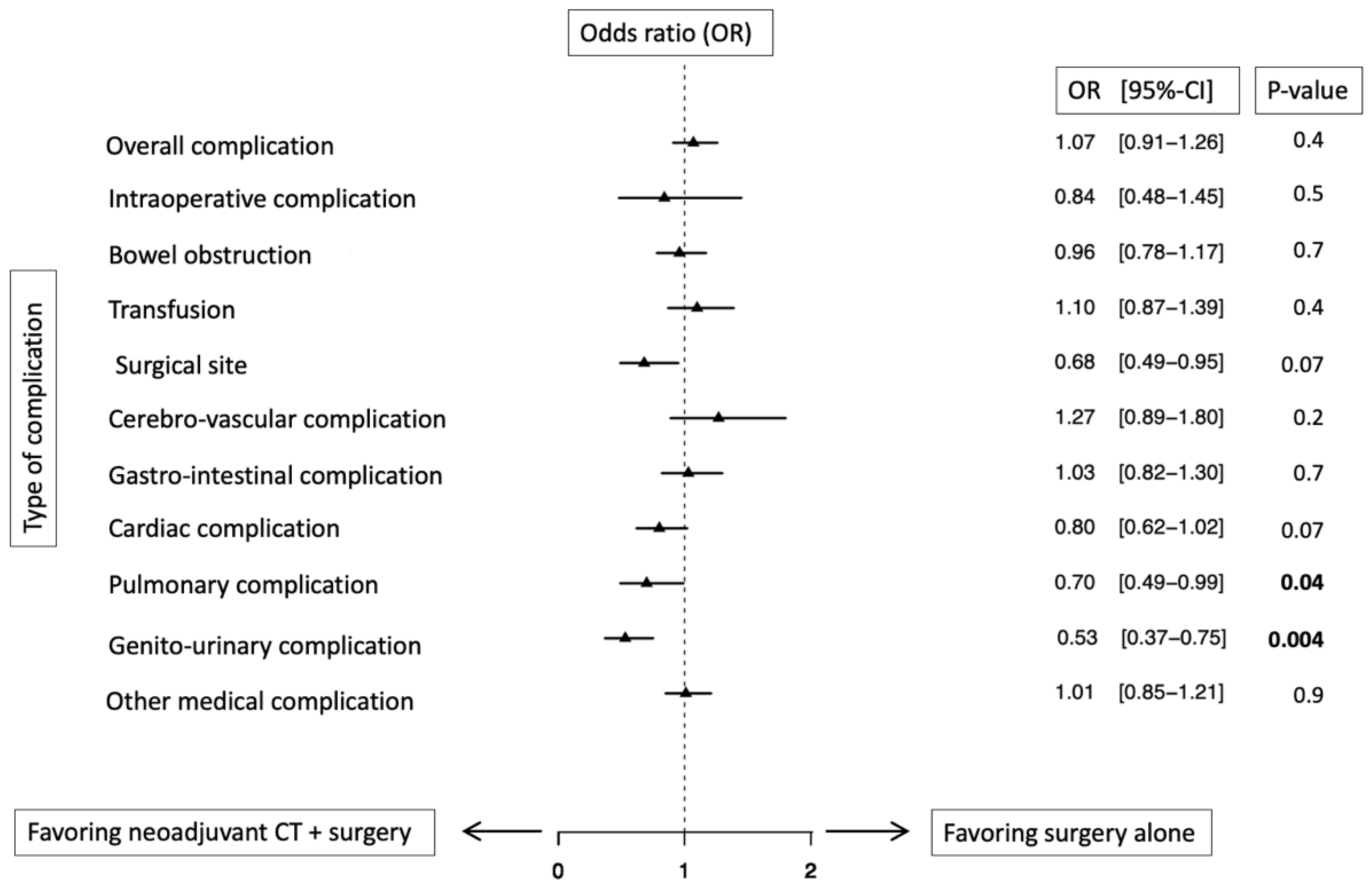
3.3. Multivariable Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Witjes, J.A.; Bruins, H.M.; Cathomas, R.; Compérat, E.; Cowan, N.C.; Efstathiou, J.A.; Fietkau, R.; Gakis, G.; Hernández, V.; Lorch, A.; et al. Muscle-invasive and Metastatic Bladder Cancer. EAU Guidelines. Edn. Presented at the EAU Annual Congress, Milan, Italy, 9–13 July 2021; ISBN 978-94-92671-13-4. [Google Scholar]
- NCCN Guidelines Version 5.2021 Bladder Cancer. Available online: http://www.nccn.org/professionals/physician_gls/pdf/bladdercancer.pdf (accessed on 10 November 2021).
- Grossman, H.B.; Natale, R.B.; Tangen, C.M.; Speights, V.O.; Vogelzang, N.J.; Trump, D.L.; de Vere White, R.W.; Sarosdy, M.F.; Wood, D.P.; Raghavan, D.; et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Eng. J. Med. 2003, 349, 859–866. [Google Scholar] [CrossRef] [PubMed]
- International Collaboration of Trialists on behalf of the Medical Research Council Advanced Bladder Cancer Working Party (Now the National Cancer Research Institute Bladder Cancer Clinical Studies Group); The European Organisation for Research and Treatment of Cancer Genito-Urinary Tract Cancer Group; The Australian Bladder Cancer Study Group; The National Cancer Institute of Canada Clinical Trials Group; Finnbladder, Norwegian Bladder Cancer Study Group. Club Urologico Espanol de Tratamiento Oncologic International Phase III Trial Assessing Neoadjuvant Cisplatin, Methotrexate, and Vinblastine Chemotherapy for Muscle-Invasive Bladder Cancer: Long-Term Results of the BA06 30894 Trial. JCO 2011, 29, 2171–2177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, M.; Joshi, M.; Meijer, R.P.; Glantz, M.; Holder, S.; Harvey, H.A.; Kaag, M.; Fransen van de Putte, E.E.; Horenblas, S.; Drabick, J.J. Neoadjuvant Chemotherapy for Muscle-Invasive Bladder Cancer: A Systematic Review and Two-Step Meta-Analysis. Oncologist 2016, 21, 708–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Advanced Bladder Cancer Meta-analysis Collaboration Neoadjuvant chemotherapy in invasive bladder cancer: A systematic review and meta-analysis. Lancet 2003, 361, 1927–1934. [CrossRef]
- Winquist, E.; Kirchner, T.S.; Segal, R.; Chin, J.; Lukka, H.; Genitourinary Cancer Disease Site Group, Cancer Care Ontario Program in Evidence-based Care Practice Guidelines Initiative. Neoadjuvant chemotherapy for transitional cell carcinoma of the bladder: A systematic review and meta-analysis. J. Urol. 2004, 171, 561–569. [Google Scholar] [CrossRef]
- Pfister, C.; Gravis, G.; Fléchon, A.; Soulié, M.; Guy, L.; Laguerre, B.; Mottet, N.; Joly, F.; Allory, Y.; Harter, V.; et al. Randomized Phase III Trial of Dose-dense Methotrexate, Vinblastine, Doxorubicin, and Cisplatin, or Gemcitabine and Cisplatin as Perioperative Chemotherapy for Patients with Muscle-invasive Bladder Cancer. Analysis of the GETUG/AFU V05 VESPER Trial Secondary Endpoints: Chemotherapy Toxicity and Pathological Responses. Eur. Urol. 2021, 79, 214–221. [Google Scholar]
- Johnson, D.C.; Nielsen, M.E.; Matthews, J.; Woods, M.E.; Wallen, E.M.; Pruthi, R.S.; Milowsky, M.I.; Smith, A.B. Neoadjuvant chemotherapy for bladder cancer does not increase risk of perioperative morbidity: Neoadjuvant chemotherapy utilization and perioperative morbidity. BJU Int. 2014, 114, 221–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gandaglia, G.; Popa, I.; Abdollah, F.; Schiffmann, J.; Shariat, S.F.; Briganti, A.; Montorsi, F.; Trinh, Q.-D.; Karakiewicz, P.I.; Sun, M. The Effect of Neoadjuvant Chemotherapy on Perioperative Outcomes in Patients Who Have Bladder Cancer Treated with Radical Cystectomy: A Population-based Study. Eur. Urol. 2014, 66, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Jerlström, T.; Chen, R.; Liedberg, F.; Andrén, O.; Ströck, V.; Aljabery, F.A.S.; Hosseini, A.; Sherif, A.; Malmström, P.-U.; Ullén, A.; et al. No increased risk of short-term complications after radical cystectomy for muscle-invasive bladder cancer among patients treated with preoperative chemotherapy: A nation-wide register-based study. World J. Urol. 2020, 38, 381–388. [Google Scholar] [CrossRef] [Green Version]
- Salminen, A.P.; Koskinen, I.; Perez, I.M.; Hurme, S.; Murtola, T.J.; Vaarala, M.H.; Nykopp, T.K.; Seppänen, M.; Isotalo, T.; Marttila, T.; et al. Neoadjuvant Chemotherapy Does Not Increase the Morbidity of Radical Cystectomy: A 10-year Retrospective Nationwide Study. Eur. Urol. Oncol. 2018, 1, 525–530. [Google Scholar] [CrossRef] [PubMed]
- Agency for Healthcare Research and Quality; Rockville, M.D. HCUP National Inpatient Sample (NIS). Healthcare Cost and Utilization Project (HCUP); Agency for Healthcare Research and Quality: Rockville, MD, USA, 2012. Available online: www.hcup-us.ahrq.gov/nisoverview.jsp (accessed on 1 February 2022).
- Lyon, T.D.; Faraj, K.S.; Brennan, E.; Tyson, M.D.; Boorjian, S.A.; Spaulding, A.C. Defining radical cystectomy using the ICD-10 procedure coding system. Urol. Oncol. Semin. Orig. Investig. 2021. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, C.; Knipper, S.; Pecoraro, A.; Rosiello, G.; Luzzago, S.; Deuker, M.; Tian, Z.; Shariat, S.F.; Simeone, C.; Briganti, A.; et al. Patient frailty predicts worse perioperative outcomes and higher cost after radical cystectomy. Surg. Oncol. 2020, 32, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Mazzone, E.; Preisser, F.; Nazzani, S.; Tian, Z.; Zaffuto, E.; Gallina, A.; Tilki, D.; Montorsi, F.; Shariat, S.F.; Saad, F.; et al. The effect of age and comorbidities on early postoperative complications after radical cystectomy: A contemporary population-based analysis. J. Geriatr. Oncol. 2019, 10, 623–631. [Google Scholar] [CrossRef] [PubMed]
- Preisser, F.; Nazzani, S.; Mazzone, E.; Marchioni, M.; Bandini, M.; Tian, Z.; Haese, A.; Saad, F.; Zorn, K.; Montorsi, F.; et al. Comparison of Open Versus Robotically Assisted Cytoreductive Radical Prostatectomy for Metastatic Prostate Cancer. Clin. Genitourin. Cancer 2019, 17, e939–e945. [Google Scholar] [CrossRef] [PubMed]
- Storesund, A.; Haugen, A.S.; Hjortås, M.; Nortvedt, M.W.; Flaatten, H.; Eide, G.E.; Boermeester, M.A.; Sevdalis, N.; Søfteland, E. Accuracy of surgical complication rate estimation using ICD-10 codes. Br. J. Surg. 2019, 106, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Bhanvadia, R.; Ashbrook, C.; Gahan, J.; Mauck, R.; Bagrodia, A.; Margulis, V.; Lotan, Y.; Roehrborn, C.; Woldu, S. Perioperative outcomes and cost of robotic vs open simple prostatectomy in the modern robotic era: Results from the National Inpatient Sample. BJU Int. 2021, 128, 168–177. [Google Scholar] [CrossRef] [PubMed]
- United States Department of Labor; U.S. Bureau of Labor Statistics. Consumer Price Index. Available online: https://www.bls.gov/cpi/ (accessed on 10 October 2021).
- Deyo, R. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J. Clin. Epidemiol. 1992, 45, 613–619. [Google Scholar] [CrossRef]
- Glasheen, W.P.; Cordier, T.; Gumpina, R.; Haugh, G.; Davis, J.; Renda, A. Charlson Comorbidity Index: ICD-9 Update and ICD-10 Translation. Am. Health Drug Benefits 2019, 12, 188–197. [Google Scholar] [PubMed]
- Preisser, F.; Nazzani, S.; Mazzone, E.; Knipper, S.; Bandini, M.; Tian, Z.; Haese, A.; Saad, F.; Zorn, K.C.; Montorsi, F.; et al. Regional differences in total hospital charges between open and robotically assisted radical prostatectomy in the United States. World J. Urol. 2019, 37, 1305–1313. [Google Scholar] [CrossRef] [PubMed]
- Hoeh, B.; Preisser, F.; Mandel, P.; Wenzel, M.; Humke, C.; Welte, M.-N.; Müller, M.; Köllermann, J.; Wild, P.; Kluth, L.A.; et al. Inverse Stage Migration in Radical Prostatectomy-A Sustaining Phenomenon. Front. Surg. 2021, 8, 612813. [Google Scholar] [CrossRef] [PubMed]
- RCT. R: A Language and Environment for Statistical Computing. Available online: https://wwwr-projectorg2017 (accessed on 1 February 2022).
- McFerrin, C.; Davaro, F.; May, A.; Raza, S.; Siddiqui, S.; Hamilton, Z. Trends in utilization of neoadjuvant and adjuvant chemotherapy for muscle invasive bladder cancer. Investig. Clin. Urol. 2020, 61, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Patafio, F.M.; Mackillop, W.J.; Feldman-Stewart, D.; Siemens, D.R.; Booth, C.M. Why is perioperative chemotherapy for bladder cancer underutilized? Urol. Oncol. 2014, 32, 391–395. [Google Scholar] [CrossRef] [PubMed]
- Hanna, N.; Trinh, Q.-D.; Seisen, T.; Vetterlein, M.W.; Sammon, J.; Preston, M.A.; Lipsitz, S.R.; Bellmunt, J.; Menon, M.; Choueiri, T.K.; et al. Effectiveness of Neoadjuvant Chemotherapy for Muscle-invasive Bladder Cancer in the Current Real World Setting in the USA. Eur. Urol. Oncol. 2018, 1, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Gray, P.J.; Fedewa, S.A.; Shipley, W.U.; Efstathiou, J.A.; Lin, C.C.; Zietman, A.L.; Virgo, K.S. Use of Potentially Curative Therapies for Muscle-invasive Bladder Cancer in the United States: Results from the National Cancer Data Base. Eur. Urol. 2013, 63, 823–829. [Google Scholar] [CrossRef]
- National Cancer Database. Available online: http://ncdbpuf.facs.org/ (accessed on 5 July 2021).
- Batista Rodríguez, G.; Balla, A.; Fernández-Ananín, S.; Balagué, C.; Targarona, E.M. The Era of the Large Databases: Outcomes After Gastroesophageal Surgery According to NSQIP, NIS, and NCDB Databases. Systematic Literature Review. Surg. Innov. 2018, 25, 400–412. [Google Scholar] [CrossRef] [PubMed]
- Vetterlein, M.W.; Meyer, C.P.; Leyh-Bannurah, S.-R.; Mayr, R.; Gierth, M.; Fritsche, H.-M.; Burger, M.; Keck, B.; Wullich, B.; Martini, T.; et al. Effect of Hospital and Surgeon Case Volume on Perioperative Quality of Care and Short-term Outcomes After Radical Cystectomy for Muscle-invasive Bladder Cancer: Results from a European Tertiary Care Center Cohort. Clin. Genitourin. Cancer 2017, 15, e809–e817. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Overall, N = 4347 | Surgery, N = 3542 (81%) | Neoadjuvant CT + Surgery, N = 805 (19%) | p-Value | |
|---|---|---|---|---|
| Age in years, Median (IQR) | 69 (62, 75) | 70 (63, 76) | 67 (61, 73) | <0.001 |
| Gender, n (%) | <0.001 | |||
| Female | 936 (22%) | 725 (20%) | 211 (26%) | |
| Male | 3411 (78%) | 2817 (80%) | 594 (74%) | |
| Modified Charlson-Comorbidity Index, n (%) | <0.001 | |||
| 0-1 | 3698 (85%) | 2976 (84%) | 722 (90%) | |
| ≥2 | 649 (15%) | 566 (16%) | 83 (10%) | |
| History of smoking, n (%) | 1656 (38%) | 1292 (36%) | 364 (45%) | <0.001 |
| Race/Ethnicity, n (%) | 0.6 | |||
| Caucasian | 3506 (81%) | 2855 (81%) | 651 (81%) | |
| African-American | 256 (5.9%) | 204 (5.8%) | 52 (6.5%) | |
| Others | 585 (13%) | 483 (14%) | 102 (13%) | |
| Surgical approach, n (%) | 0.8 | |||
| Open | 2622 (60%) | 2140 (60%) | 482 (60%) | |
| Minimal-invasive | 1725 (40%) | 1402 (40%) | 323 (40%) | |
| Lymph-node dissection, n (%) | 3968 (91%) | 3213 (91%) | 755 (94%) | 0.005 |
| Type of diversion, n (%) | 0.007 | |||
| Incontinent | 4078 (94%) | 3335 (94%) | 743 (92%) | |
| Continent | 239 (5.3%) | 179 (5%) | 60 (7%) | |
| Other/Unkown | 30 (0.7%) | * | <11 (<1.3%) * | |
| Year of surgery, n (%) | 0.005 | |||
| 2016 | 1091 (25%) | 923 (26%) | 168 (21%) | |
| 2017 | 1148 (26%) | 920 (26%) | 228 (28%) | |
| 2018 | 1015 (23%) | 827 (23%) | 188 (23%) | |
| 2019 | 1093 (25%) | 872 (25%) | 221 (27%) | |
| Hospital bed size, n (%) | 0.14 | |||
| Small | 491 (11%) | 397 (11%) | 94 (12%) | |
| Medium | 922 (21%) | 772 (22%) | 150 (19%) | |
| Large | 2934 (67%) | 2373 (67%) | 561 (70%) | |
| Teaching hospital, n (%) | 3911 (90%) | 3174 (90%) | 737 (92%) | 0.1 |
| Region, n (%) | 0.6 | |||
| Midwest | 1176 (27%) | 954 (27%) | 222 (28%) | |
| Northeast | 851 (20%) | 706 (20%) | 145 (18%) | |
| South | 1530 (35%) | 1257 (35%) | 273 (34%) | |
| West | 790 (18%) | 625 (18%) | 165 (20%) | |
| Income, n (%) | 0.1 | |||
| 0-25-percentile | 981 (23%) | 815 (23%) | 166 (21%) | |
| 26-50-percentile | 1153 (27%) | 950 (27%) | 203 (25%) | |
| 51-75-percentile | 1160 (27%) | 923 (26%) | 237 (29%) | |
| 76-100-percentile | 991 (23%) | 800 (23%) | 191 (24%) | |
| Other/Unknown | 62 (1.4%) | * | <11 (<1.3%) * | |
| Insurance provider, n (%) | <0.001 | |||
| Medicare | 2717 (63%) | 2284 (64%) | 433 (54%) | |
| Private | 1203 (28%) | 908 (26%) | 295 (37%) | |
| Medicaid | 258 (5.9%) | 210 (5.9%) | 48 (6.0%) | |
| Others | 169 (3.9%) | 140 (4.0%) | 29 (3.6%) |
| Overall, N = 4347 | Surgery, N = 3542 (81%) | Neoadjuvant CT + Surgery, N = 805 (19%) | p-Value | |
|---|---|---|---|---|
| Overall complication n (%) | 2813 (65%) | 2306 (65%) | 507 (63%) | 0.3 |
| Intraoperative n (%) | 100 (2.3%) | 85 (2.4%) | 15 (1.9%) | 0.4 |
| Bowel obstruction n (%) | 914 (21%) | 760 (21%) | 154 (19%) | 0.4 |
| Transfusion n (%) | 543 (12%) | 439 (12%) | 104 (13%) | 0.7 |
| Surgical site n (%) | 379 (8.7%) | 333 (9.4%) | 46 (5.7%) | <0.001 |
| Cerebro-vascular n (%) | 248 (5.7%) | 202 (5.7%) | 46 (5.7%) | 0.9 |
| Gastro-intestinal n (%) | 638 (15%) | 523 (15%) | 115 (14%) | 0.7 |
| Cardiac n (%) | 743 (17%) | 647 (18%) | 96 (12%) | <0.001 |
| Pulmonary n (%) | 380 (8.7%) | 337 (9.5%) | 43 (5.3%) | <0.001 |
| Genito-urinary n (%) | 372 (8.6%) | 332 (9.4%) | 40 (5.0%) | 0.002 |
| Other medical n (%) | 1650 (38%) | 1363 (38%) | 287 (36%) | 0.1 |
| In-hospital mortality, n (%) | 66 (1.5%) | * | <11 (<1.4%) | 0.02 |
| Length of stay, Median (IQR) | 6 (5, 9) | 7 (5, 9) | 6 (5, 8) | <0.001 |
| Total hospital costs in $#, Median (IQR) | 28,494 (21,639, 39,387) | 28,367 (21,505, 39,397) | 29,073 (22,178, 39,337) | 0.2 |
| Heading | Overall Complications 1 | In-Hospital Mortality 1 | Length of Stay 2 | Total Hospital Costs 3 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Treatment Modality | OR | 95%-CI | p-Value | OR | 95%-CI | p-Value | Risk Ratio | 95%-CI | p-Value | OR | 95%-CI | p-Value |
| RC | Ref. | Ref. | Ref. | Ref. | ||||||||
| RC + neoadjuvant chemotherapy | 1.07 | 0.91–1.26 | 0.4 | 0.47 | 0.19–1.15 | 0.1 | 0.86 | 0.83–0.90 | <0.001 | 1858 4 | 690–3026 | 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoeh, B.; Flammia, R.S.; Hohenhorst, L.; Sorce, G.; Chierigo, F.; Panunzio, A.; Tian, Z.; Saad, F.; Gallucci, M.; Briganti, A.; et al. Effect of Neoadjuvant Chemotherapy on Complications, in-Hospital Mortality, Length of Stay and Total Hospital Costs in Bladder Cancer Patients Undergoing Radical Cystectomy. Cancers 2022, 14, 1222. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14051222
Hoeh B, Flammia RS, Hohenhorst L, Sorce G, Chierigo F, Panunzio A, Tian Z, Saad F, Gallucci M, Briganti A, et al. Effect of Neoadjuvant Chemotherapy on Complications, in-Hospital Mortality, Length of Stay and Total Hospital Costs in Bladder Cancer Patients Undergoing Radical Cystectomy. Cancers. 2022; 14(5):1222. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14051222
Chicago/Turabian StyleHoeh, Benedikt, Rocco Simone Flammia, Lukas Hohenhorst, Gabriele Sorce, Francesco Chierigo, Andrea Panunzio, Zhe Tian, Fred Saad, Michele Gallucci, Alberto Briganti, and et al. 2022. "Effect of Neoadjuvant Chemotherapy on Complications, in-Hospital Mortality, Length of Stay and Total Hospital Costs in Bladder Cancer Patients Undergoing Radical Cystectomy" Cancers 14, no. 5: 1222. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14051222