
Measuring Walking Speed Failed to Predict Early Death and Toxicity in Elderly Patients with Metastatic Non-Small-Cell Lung Cancer (NSCLC) Selected for Undergoing First-Line Systemic Treatment: An Observational Exploratory Study

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
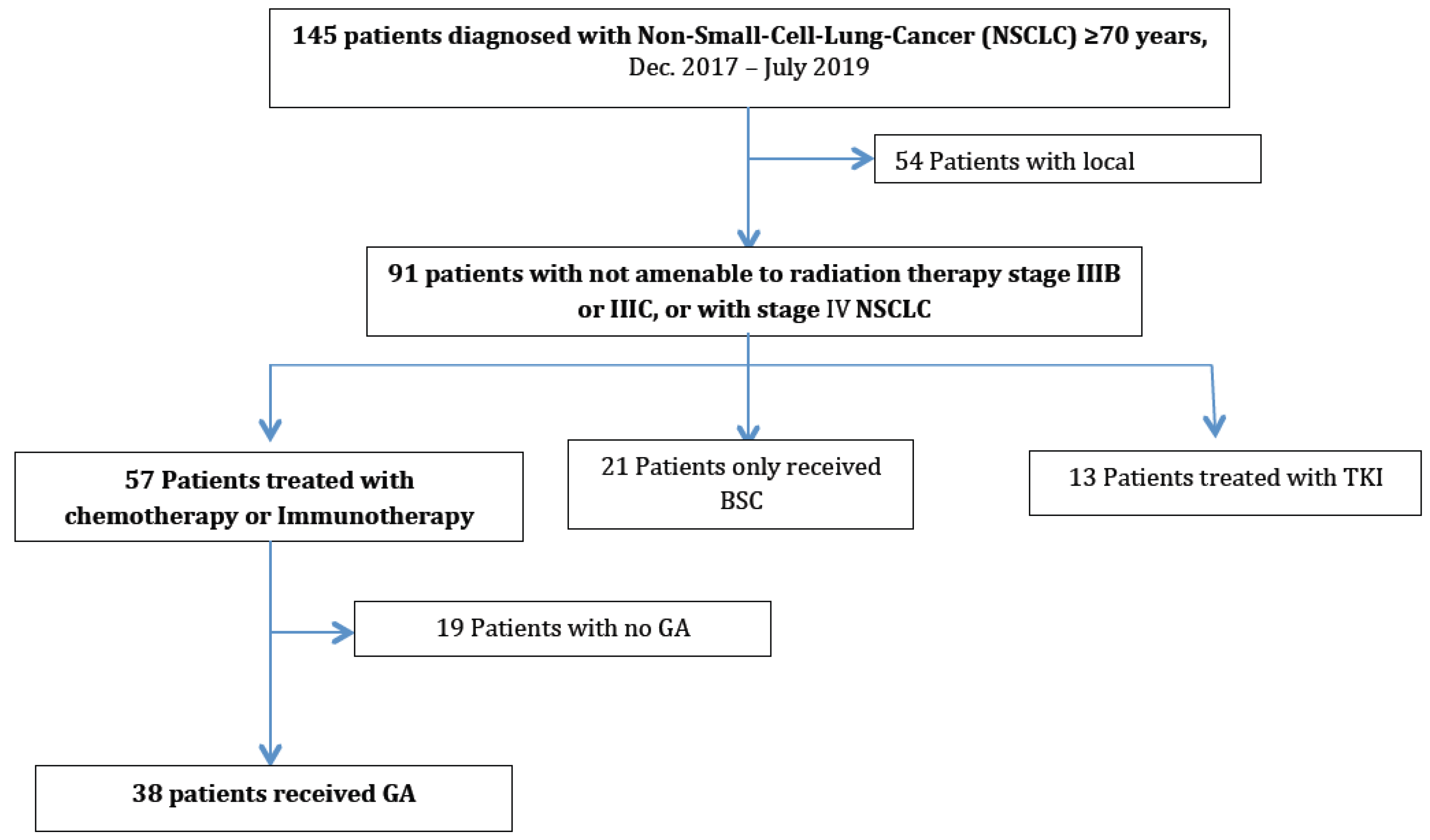
2.1. Study Design and Participants
2.2. Data Collection and Baseline Measurements
2.3. Endpoints
2.4. Statistical Analysis
3. Results
3.1. Patient Baseline Characteristics
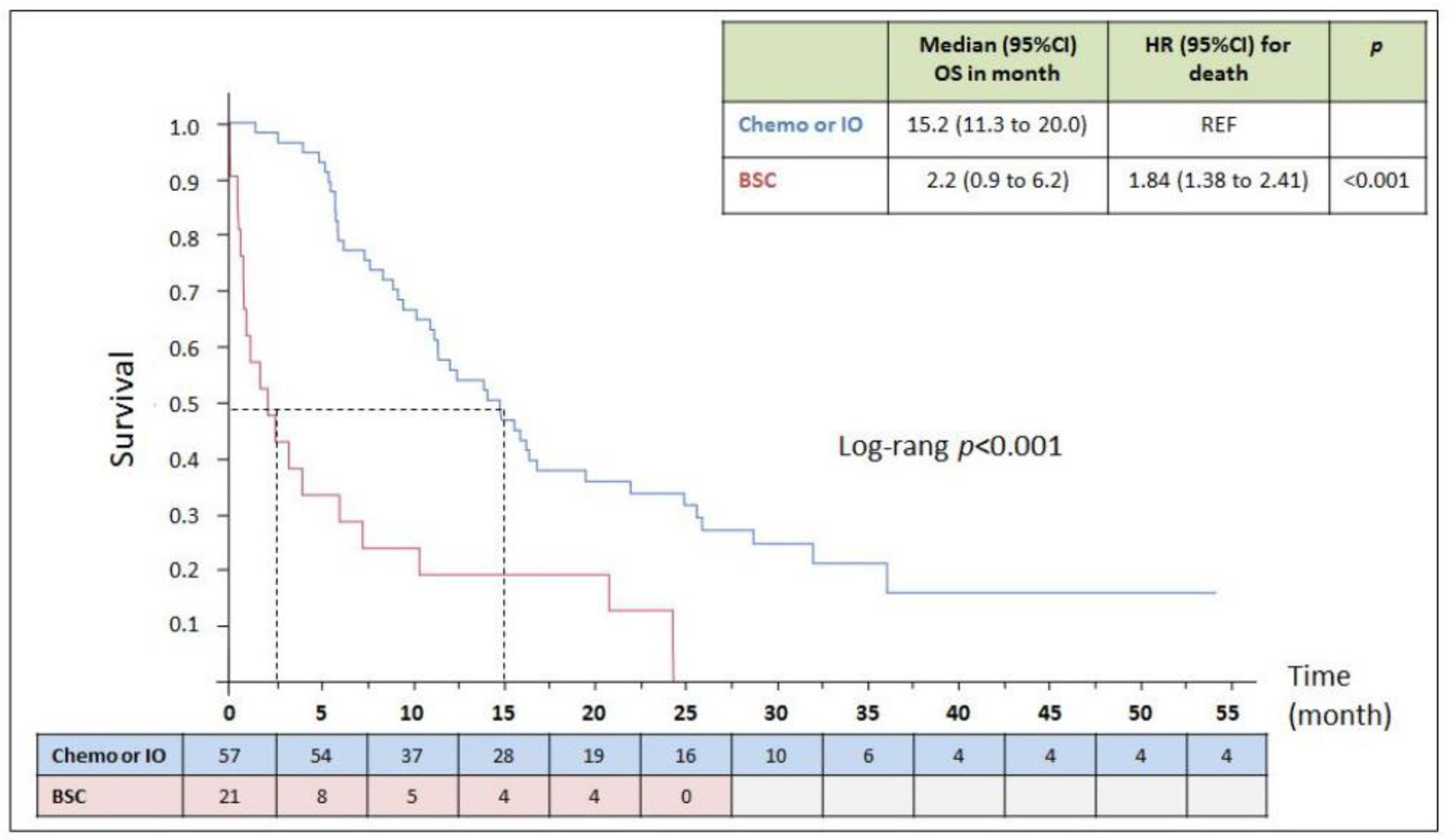
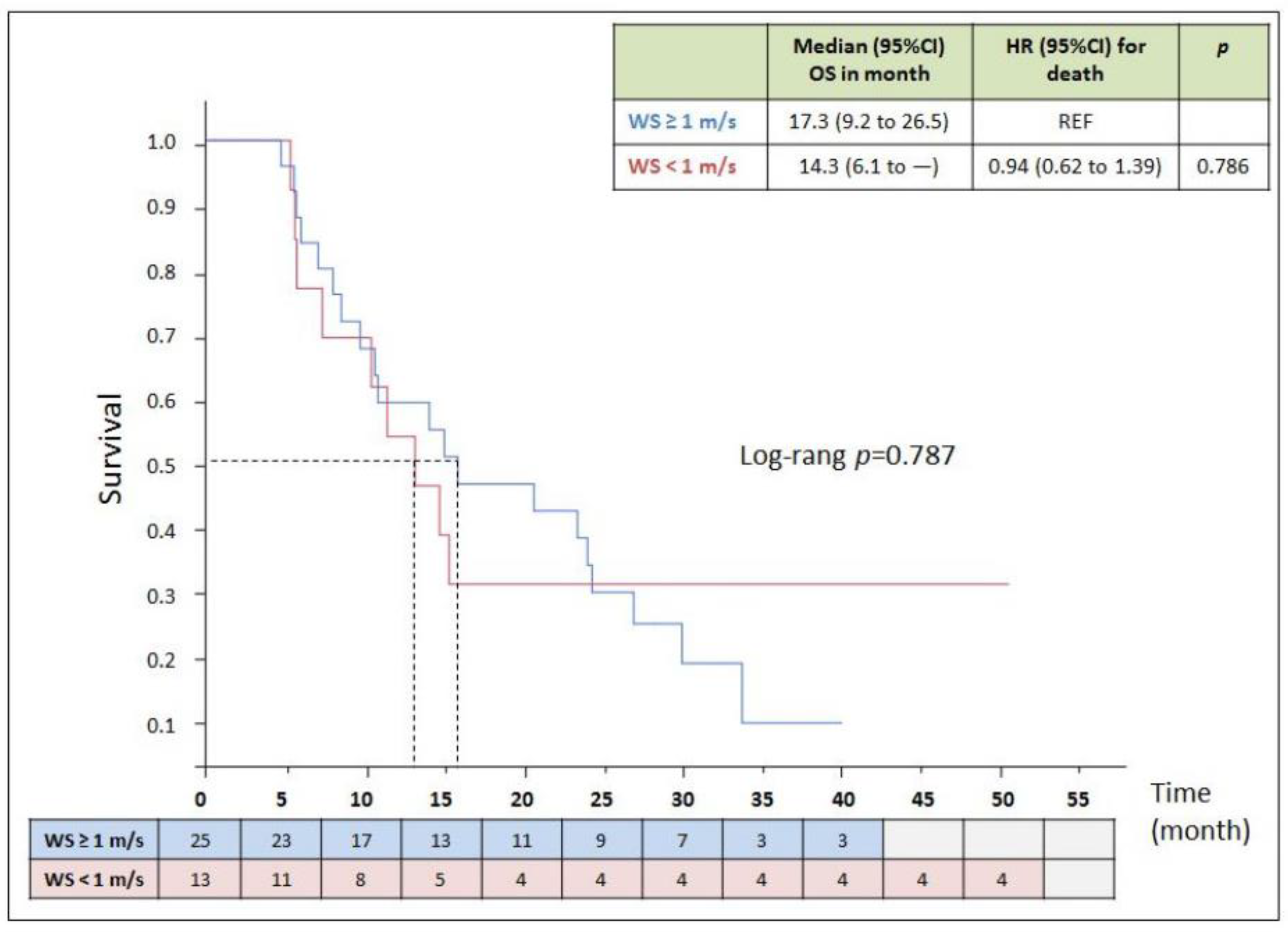
3.2. Overall Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BSC | Best Supportive Care |
| CGA | Comprehensive Geriatric Assessment |
| Chemo | Chemotherapy |
| CIRS-G | Cumulative Illness Rating Scale-Geriatric |
| CT | Computed Tomography |
| GA | Geriatric Assessment |
| IO | Immunotherapy |
| IQR | Interquartile range |
| MNA-SF | Mini Nutritional Assessment-Short Form |
| NR | Not Reached |
| OS | Overall Survival |
| PS | Performance Status |
| PY | Pack years |
| SMI | Skeletal muscle mass index |
| SPPB | Short Physical Performance Battery |
| TKI | Tyrosine Kinase Inhibitor |
| TRAE | Treatment Related Adverse Event |
| TUG | Time Up and Go Test |
| WS | Walking Speed |
References
- Owonikoko, T.K.; Ragin, C.C.; Belani, C.P.; Oton, A.B.; Gooding, W.E.; Taioli, E.; Ramalingam, S.S. Lung Cancer in Elderly Patients: An Analysis of the Surveillance, Epidemiology, and End Results Database. J. Clin. Oncol. 2007, 25, 5570–5577. [Google Scholar] [CrossRef] [PubMed]
- Pilleron, S.; Soto-Perez-de-Celis, E.; Vignat, J.; Ferlay, J.; Soerjomataram, I.; Bray, F.; Sarfati, D. Estimated global cancer inci-dence in the oldest adults in 2018 and projections to 2050. Int. J. Cancer 2021, 148, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33, Erratum in CA Cancer J. Clin. 2021, 71, 359. [Google Scholar] [CrossRef] [PubMed]
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.F.; Faivre-Finn, C.; Mok, T.S.; Reck, M.; Van Schil, P.E.; Hellmann, M.D.; et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29 (Suppl. 4), iv192–iv237. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD-L1–Positive Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sacher, A.G.; Le, L.W.; Leighl, N.B.; Coate, L.E. Elderly Patients with Advanced NSCLC in Phase III Clinical Trials: Are the Elderly Excluded from Practice-Changing Trials in Advanced NSCLC? J. Thorac. Oncol. 2013, 8, 366–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wildiers, H.; Heeren, P.; Puts, M.; Topinkova, E.; Janssen-Heijnen, M.L.; Extermann, M.; Falandry, C.; Artz, A.; Brain, E.; Colloca, G.; et al. International Society of Geriatric Oncology Consensus on Geriatric Assessment in Older Patients with Cancer. J. Clin. Oncol. 2014, 32, 2595–2603. [Google Scholar] [CrossRef] [Green Version]
- Mohile, S.G.; Dale, W.; Somerfield, M.R.; Schonberg, M.A.; Boyd, C.M.; Burhenn, P.; Canin, B.; Cohen, H.J.; Holmes, H.M.; Hopkins, J.O.; et al. Practical Assessment and Management of Vulnerabilities in Older Patients Receiving Chemotherapy: ASCO Guideline for Geriatric Oncology. J. Clin. Oncol. 2018, 36, 2326–2347. [Google Scholar] [CrossRef]
- Ferrat, E.; Paillaud, E.; Laurent, M.; Le Thuaut, A.; Caillet, P.; Tournigand, C.; Lagrange, J.-L.; Canoui-Poitrine, F.; Bastuji-Garin, S.; ELPACA Study Group. Predictors of 1-Year Mortality in a Prospective Cohort of Elderly Patients With Cancer. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2015, 70, 1148–1155. [Google Scholar] [CrossRef]
- Studenski, S.; Perera, S.; Patel, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; Brach, J.; Chandler, J.; Cawthon, P.; Connor, E.B.; et al. Gait Speed and Survival in Older Adults. JAMA 2011, 305, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Cesari, M.; Kritchevsky, S.B.; Penninx, B.W.H.J.; Nicklas, B.J.; Simonsick, E.M.; Newman, A.B.; Tylavsky, F.A.; Brach, J.S.; Satterfield, S.; Bauer, D.C.; et al. Prognostic Value of Usual Gait Speed in Well-Functioning Older People—Results from the Health, Aging and Body Composition Study. J. Am. Geriatr. Soc. 2005, 53, 1675–1680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pamoukdjian, F.; Lévy, V.; Sebbane, G.; Boubaya, M.; Landre, T.; Bloch-Queyrat, C.; Paillaud, E.; Zelek, L. Slow gait speed is an independent predictor of early death in older cancer outpatients: Results from a prospective cohort study. J. Nutr. Health Aging 2016, 21, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Hurria, A.; Togawa, K.; Mohile, S.G.; Owusu, C.; Klepin, H.D.; Gross, C.P.; Lichtman, S.M.; Gajra, A.; Bhatia, S.; Katheria, V.; et al. Predicting Chemotherapy Toxicity in Older Adults With Cancer: A Prospective Multicenter Study. J. Clin. Oncol. 2011, 29, 3457–3465. [Google Scholar] [CrossRef] [Green Version]
- Inoue, A.; Kobayashi, K.; Usui, K.; Maemondo, M.; Okinaga, S.; Mikami, I.; Ando, M.; Yamazaki, K.; Saijo, Y.; Gemma, A.; et al. First-Line Gefitinib for Patients With Advanced Non–Small-Cell Lung Cancer Harboring Epidermal Growth Factor Receptor Mutations Without Indication for Chemotherapy. J. Clin. Oncol. 2009, 27, 1394–1400. [Google Scholar] [CrossRef]
- Pamoukdjian, F.; Canoui-Poitrine, F.; Longelin-Lombard, C.; Aparicio, T.; Ganne, N.; Wind, P.; Martinez-Tapia, C.; Audureau, E.; Sebbane, G.; Zelek, L.; et al. Diagnostic performance of gait speed, G8 and G8 modified indices to screen for vulnerability in older cancer patients: The prospective PF-EC cohort study. Oncotarget 2017, 8, 50393–50402. [Google Scholar] [CrossRef] [Green Version]
- Mourtzakis, M.; Prado, C.M.; Lieffers, J.R.; Reiman, T.; McCargar, L.J.; Baracos, V.E. A practical and precise approach to quantification of body composition in cancer patients using computed tomography images acquired during routine care. Appl. Physiol. Nutr. Metab. 2008, 33, 997–1006. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.K.; Wu, Y.-L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G., Jr.; Srimuninnimit, V.; Laktionov, K.K.; Bondarenko, I.; et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): A randomised, open-label, controlled, phase 3 trial. Lancet 2019, 393, 1819–1830. [Google Scholar] [CrossRef]
- Boulahssass, R.; Gonfrier, S.; Ferrero, J.-M.; Sanchez, M.; Mari, V.; Moranne, O.; Rambaud, C.; Auben, F.; Levi, J.-M.H.; Bereder, J.-M.; et al. Predicting early death in older adults with cancer. Eur. J. Cancer 2018, 100, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Nakano, J.; Fukushima, T.; Tanaka, T.; Fu, J.B.; Morishita, S. Physical function predicts mortality in patients with cancer: A systematic review and meta-analysis of observational studies. Support. Care Cancer 2021, 29, 5623–5634. [Google Scholar] [CrossRef]
- Couderc, A.-L.; Tomasini, P.; Rey, D.; Nouguerède, E.; Correard, F.; Barlesi, F.; Thomas, P.; Villani, P.; Greillier, L. Octogenarians treated for thoracic and lung cancers: Impact of comprehensive geriatric assessment. J. Geriatr. Oncol. 2021, 12, 402–409. [Google Scholar] [CrossRef]
- Corre, R.; Greillier, L.; Le Caër, H.; Audigier-Valette, C.; Baize, N.; Bérard, H.; Falchero, L.; Monnet, I.; Dansin, E.; Vergnenègre, A.; et al. Use of a Comprehensive Geriatric Assessment for the Management of Elderly Patients With Advanced Non–Small-Cell Lung Cancer: The Phase III Randomized ESOGIA-GFPC-GECP 08-02 Study. J. Clin. Oncol. 2016, 34, 1476–1483. [Google Scholar] [CrossRef] [PubMed]
- Quoix, E.; Zalcman, G.; Oster, J.-P.; Westeel, V.; Pichon, E.; Lavolé, A.; Dauba, J.; Debieuvre, D.; Souquet, P.-J.; Bigay-Game, L.; et al. Carboplatin and weekly paclitaxel doublet chemotherapy compared with monotherapy in elderly patients with advanced non-small-cell lung cancer: IFCT-0501 randomised, phase 3 trial. Lancet 2011, 378, 1079–1088. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Overall Patient Population | Patients with Chemotherapy | Patients with Immunotherapy |
|---|---|---|---|
| n = 38 | n = 28 | n = 10 | |
| Age, years (IQR) | 75 (71.8–78.5) | 75 (71.3–79.5) | 76 (71.8–79.5) |
| Male gender, n (%) | 32 (84) | 23 (82) | 9 (90) |
| Performance Status | |||
| 0–1, n (%) | 22 (58) | 16 (57) | 6 (60) |
| 2, n (%) | 16 (42) | 12 (43) | 4 (40) |
| Smokers, n (%) | 34 (90) | 25 (89) | 9 (90) |
| Pack-years (IQR) | 50 (20–80) | 50 (19–80) | 80 (30–120) |
| Histology | |||
| Squamous, n (%) | 9 (24) | 5 (18) | 4 (40) |
| Non-squamous, n (%) | 29 (76) | 23 (82) | 6 (60) |
| Stage | |||
| Stage III, n (%) | 13 (34) | 10 (36) | 3 (30) |
| Stage IV, n (%) | 25 (66) | 18 (64) | 7 (70) |
| Weight, Kg (IQR) | 75 (65.8–85) | 76 (68.8–85) | 72 (49.8–83) |
| Body mass index, Kg/m2 (IQR) | 26.6 (23.5–29.5) | 27.1 (24.1–29.4) | 25.7 (18.4–29.9) |
| Body surface, m2 (IQR) | 1.90 (1.7–2) | 1.90 (1.8–2) | 1.85 (1.31–1.95) |
| Weight loss >3 kg in 1 months, n (%) | 10 (28) | 7 (25) | 3 (38) |
| Loss of appetite, n (%) | 15 (39) | 10 (36) | 5 (50) |
| Plasma Albumin, g/L (IQR) | 39 (33–43) | 37.5 (32.3–43) | 40 (34.5–41.8) |
| MNA-SF score/14 (IQR) | 10 (8–11) | 11 (9–12) | 8 (5–11) |
| MNA-SF categories | |||
| Normal nutritional status (12–14 points), n (%) | 9 (24) | 7 (25) | 2 (20) |
| Risk of malnutrition (8–11 points), n (%) | 20 (52) | 17 (61) | 3 (30) |
| Malnutrition (0–7 points), n (%) | 9 (24) | 4 (14) | 5 (50) |
| CIRS-G, n (%) | 10 (8–12) | 9 (7–12) | 11 (8–13) |
| Skeletal muscle mass index (SMI), cm2/m2 (IQR) | 47.3 (40.5–52.2) | 48.9 (39.3–52.5) | 43.1 (40.5–49.5) |
| Sarcopenia according to SMI *, n (%) | 32 (84) | 24 (86) | 8 (80) |
| Walking speed, m/s (IQR) | 1.09 (0.9–1.31) | 1.13 (0.91–1.29) | 1.06 (0.66–1.35) |
| Walking Speed < 1 m/s, n (%) | 13 (34) | 10 (36) | 3 (30) |
| Characteristics | Outcomes during the First 6 Months of Treatment | ||||
|---|---|---|---|---|---|
| No n = 27 | Yes n = 11 | p | |||
| Grade 3–4 TRAE or Death n = 11 | Alive with Grade 3–4 TRAE n = 5 | Deceased n = 6 | |||
| Age, years (IQR) | 74 (71–78) | 76 (75–82) | 80 (74–81) | 76 (75–80) | 0.034 |
| Male gender, n (%) | 22 (81) | 10 (91) | 5 (100) | 5 (83) | 0.650 |
| Performance status | |||||
| 0–1, n (%) | 16 (59) | 6 (55) | 3 (60) | 3 (50) | 0.790 |
| 2, n (%) | 11 (41) | 5 (45) | 2 (40) | 3 (50) | |
| Pack-years (IQR) | 50 (25–80) | 65 (28–105) | 40 (25–100) | 65 (25–105) | 0.690 |
| Histology | |||||
| Squamous, n (%) | 8 (30) | 1 (9) | 0 (0) | 1 (17) | |
| Non-Squamous, n (%) | 19 (70) | 10 (91) | 5 (100) | 5 (83) | 0.237 |
| Stage | |||||
| Stage III, n (%) | 10 (37) | 3 (27) | 0 (0) | 3 (50) | 0.714 |
| Stage IV, n (%) | 17 (63) | 8 (73) | 5 (100) | 3 (50) | |
| >Weight, Kg (IQR) | 74 (61–85) | 75 (73–80) | 75 (75–78) | 79 (67–90) | 0.675 |
| Body mass index, Kg/m2 (IQR) | 25.6 (21–29.7) | 27.5 (26.2–29.4) | 27.5 (27.1–28.8) | 28.1 (23.4–31.2) | 0.253 |
| Body surface, m2(IQR) | 1.90 (1.70–2.00) | 1.90 (1.80–1.90) | 1.90 (1.90–1.90) | 1.90 (1.70–2.13) | 0.791 |
| Weight loss > 3 kg in 1 month, n (%) | 6 (24) | 4 (36) | 2 (40) | 2 (33) | 0.446 |
| Loss of appetite, n (%) | 8 (30) | 7 (64) | 4 (80) | 3 (50) | 0.052 |
| Plasma albumin, g/L (IQR) | 40 (31–43) | 37 (33–41) | 33 (31–39) | 39 (33–45) | 0.699 |
| MNA-SF (/14), n (IQR) | 10 (8–12) | 10 (7–11) | 11 (7–11) | 9 (7–11) | 0.361 |
| CIRS-G (IQR) | 8 (7–11) | 12 (10–15) | 10 (8–12) | 13 (11–16) | 0.020 |
| Skeletal muscle mass index, cm2/m2 (IQR) | 45.1 (38.8–51) | 52.0 (42.6–53.3) | 52.0 (46.8–56.1) | 47.3 (36.6–53.4) | 0.227 |
| Walking speed, m/s (IQR) | 1.10 (0.95–1.34) | 1.07 (0.68–1.25) | 1.15 (0.83–1.39) | 0.99 (0.63–1.18) | 0.562 |
| Walking speed < 1 m/s, n (%) | 9 (33) | 4 (36) | 1 (20) | 3 (50) | 0.858 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aregui, A.; Pluvy, J.; Sanchez, M.; Israel, T.; Esnault, H.; Guyard, A.; Meyer, M.; Khalil, A.; Zalcman, G.; Raynaud Simon, A.; et al. Measuring Walking Speed Failed to Predict Early Death and Toxicity in Elderly Patients with Metastatic Non-Small-Cell Lung Cancer (NSCLC) Selected for Undergoing First-Line Systemic Treatment: An Observational Exploratory Study. Cancers 2022, 14, 1344. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14051344
Aregui A, Pluvy J, Sanchez M, Israel T, Esnault H, Guyard A, Meyer M, Khalil A, Zalcman G, Raynaud Simon A, et al. Measuring Walking Speed Failed to Predict Early Death and Toxicity in Elderly Patients with Metastatic Non-Small-Cell Lung Cancer (NSCLC) Selected for Undergoing First-Line Systemic Treatment: An Observational Exploratory Study. Cancers. 2022; 14(5):1344. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14051344
Chicago/Turabian StyleAregui, Amélie, Johan Pluvy, Manuel Sanchez, Theresa Israel, Hélène Esnault, Alice Guyard, Marie Meyer, Antoine Khalil, Gérard Zalcman, Agathe Raynaud Simon, and et al. 2022. "Measuring Walking Speed Failed to Predict Early Death and Toxicity in Elderly Patients with Metastatic Non-Small-Cell Lung Cancer (NSCLC) Selected for Undergoing First-Line Systemic Treatment: An Observational Exploratory Study" Cancers 14, no. 5: 1344. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14051344