
Benchmarking Safety Indicators of Surgical Treatment of Brain Metastases Combined with Intraoperative Radiotherapy: Results of Prospective Observational Study with Comparative Matched-Pair Analysis

 , , , , ,
, , , , ,  ,
,  , , and
, , and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Matching Procedure
2.3. Statistics
3. Results
3.1. Patient Baseline Characteristics
3.2. Perioperative Complications
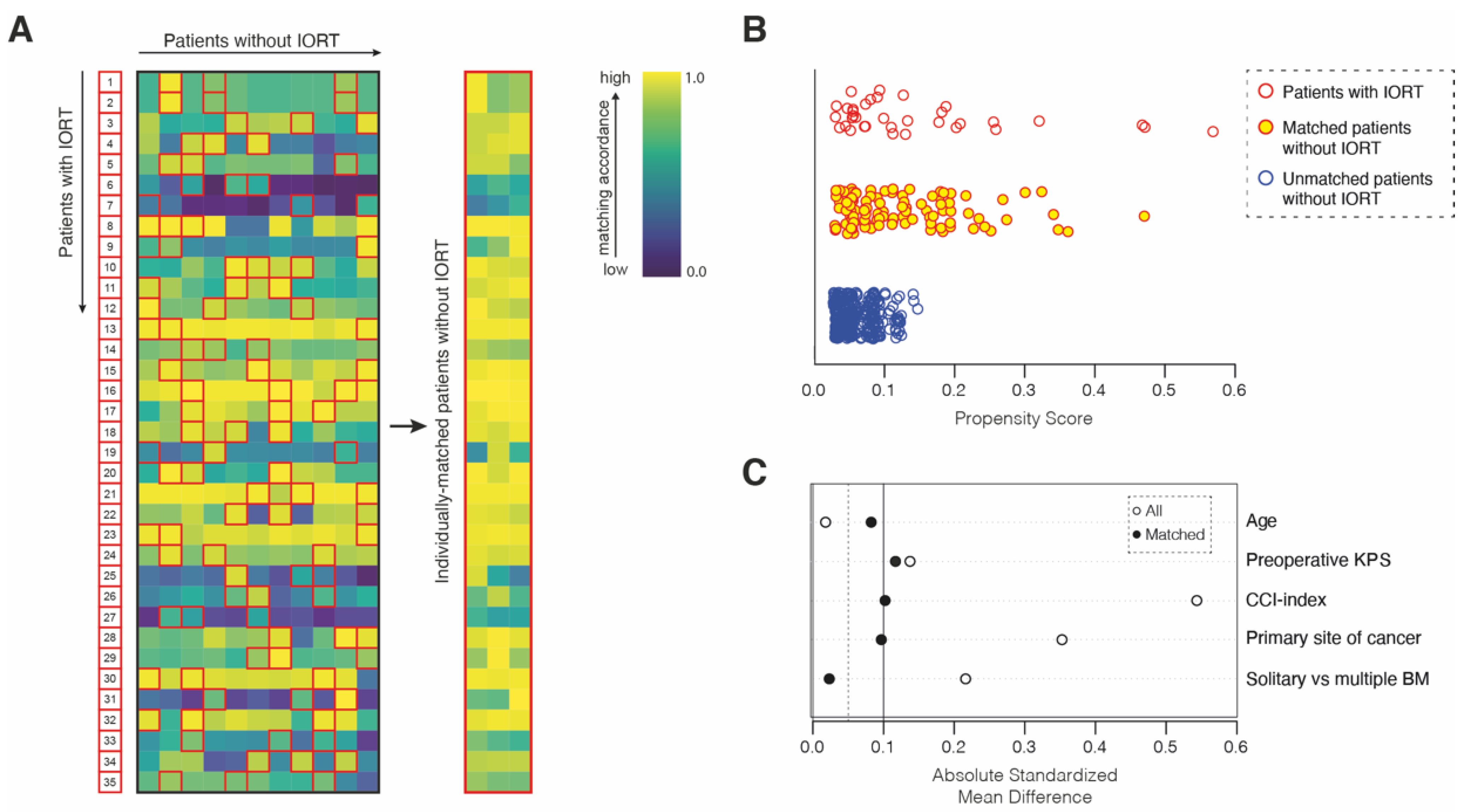
3.3. Safety-Metric Profiling for IORT in a Comparative Matched-Pair Analysis
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nahed, B.V.; Alvarez-Breckenridge, C.; Brastianos, P.K.; Shih, H.; Sloan, A.; Ammirati, M.; Kuo, J.S.; Ryken, T.C.; Kalkanis, S.N.; Olson, J.J. Congress of Neurological Surgeons Systematic Review and Evidence-Based Guidelines on the Role of Surgery in the Management of Adults With Metastatic Brain Tumors. Neurosurgery 2019, 84, E152–E155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kocher, M.; Soffietti, R.; Abacioglu, U.; Villa, S.; Fauchon, F.; Baumert, B.G.; Fariselli, L.; Tzuk-Shina, T.; Kortmann, R.D.; Carrie, C.; et al. Adjuvant whole-brain radiotherapy versus observation after radiosurgery or surgical resection of one to three cerebral metastases: Results of the EORTC 22952-26001 study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29, 134–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vargo, J.A.; Sparks, K.M.; Singh, R.; Jacobson, G.M.; Hack, J.D.; Cifarelli, C.P. Feasibility of dose escalation using intraoperative radiotherapy following resection of large brain metastases compared to post-operative stereotactic radiosurgery. J. Neuro-Oncol. 2018, 140, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Weil, R.J.; Mavinkurve, G.G.; Chao, S.T.; Vogelbaum, M.A.; Suh, J.H.; Kolar, M.; Toms, S.A. Intraoperative radiotherapy to treat newly diagnosed solitary brain metastasis: Initial experience and long-term outcomes. J. Neurosurg. 2015, 122, 825–832. [Google Scholar] [CrossRef] [PubMed]
- Raleigh, D.R.; Seymour, Z.A.; Tomlin, B.; Theodosopoulos, P.V.; Berger, M.S.; Aghi, M.K.; Geneser, S.E.; Krishnamurthy, D.; Fogh, S.E.; Sneed, P.K.; et al. Resection and brain brachytherapy with permanent iodine-125 sources for brain metastasis. J. Neurosurg. 2017, 126, 1749–1755. [Google Scholar] [CrossRef] [Green Version]
- Kalapurakal, J.A.; Goldman, S.; Stellpflug, W.; Curran, J.; Sathiaseelan, V.; Marymont, M.H.; Tomita, T. Phase I study of intraoperative radiotherapy with photon radiosurgery system in children with recurrent brain tumors: Preliminary report of first dose level (10 Gy). Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 800–808. [Google Scholar] [CrossRef] [PubMed]
- Sarria, G.R.; Smalec, Z.; Muedder, T.; Holz, J.A.; Scafa, D.; Koch, D.; Garbe, S.; Schneider, M.; Hamed, M.; Vatter, H.; et al. Dosimetric Comparison of Upfront Boosting With Stereotactic Radiosurgery Versus Intraoperative Radiotherapy for Glioblastoma. Front. Oncol. 2021, 11, 759873. [Google Scholar] [CrossRef] [PubMed]
- Sarria, G.R.; Sperk, E.; Han, X.; Sarria, G.J.; Wenz, F.; Brehmer, S.; Fu, B.; Min, S.; Zhang, H.; Qin, S.; et al. Intraoperative radiotherapy for glioblastoma: An international pooled analysis. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2020, 142, 162–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giordano, F.A.; Brehmer, S.; Murle, B.; Welzel, G.; Sperk, E.; Keller, A.; Abo-Madyan, Y.; Scherzinger, E.; Clausen, S.; Schneider, F.; et al. Intraoperative Radiotherapy in Newly Diagnosed Glioblastoma (INTRAGO): An Open-Label, Dose-Escalation Phase I/II Trial. Neurosurgery 2019, 84, 41–49. [Google Scholar] [CrossRef]
- Cifarelli, C.P.; Brehmer, S.; Vargo, J.A.; Hack, J.D.; Kahl, K.H.; Sarria-Vargas, G.; Giordano, F.A. Intraoperative radiotherapy (IORT) for surgically resected brain metastases: Outcome analysis of an international cooperative study. J. Neuro-Oncol. 2019, 145, 391–397. [Google Scholar] [CrossRef]
- Kahl, K.H.; Balagiannis, N.; Hock, M.; Schill, S.; Roushan, Z.; Shiban, E.; Muller, H.; Grossert, U.; Konietzko, I.; Sommer, B.; et al. Intraoperative radiotherapy with low-energy x-rays after neurosurgical resection of brain metastases-an Augsburg University Medical Center experience. Strahlenther. Onkol. 2021, 197, 1124–1130. [Google Scholar] [CrossRef] [PubMed]
- Schuss, P.; Lehmann, F.; Schäfer, N.; Bode, C.; Scharnböck, E.; Schaub, C.; Heimann, M.; Potthoff, A.L.; Weller, J.; Güresir, E.; et al. Postoperative Prolonged Mechanical Ventilation in Patients With Newly Diagnosed Glioblastoma-An Unrecognized Prognostic Factor. Front. Oncol. 2020, 10, 607557. [Google Scholar] [CrossRef] [PubMed]
- Schuss, P.; Schäfer, N.; Bode, C.; Borger, V.; Eichhorn, L.; Giordano, F.A.; Güresir, E.; Heimann, M.; Ko, Y.D.; Landsberg, J.; et al. The Impact of Prolonged Mechanical Ventilation on Overall Survival in Patients With Surgically Treated Brain Metastases. Front. Oncol. 2021, 11, 658949. [Google Scholar] [CrossRef]
- Sundararajan, V.; Henderson, T.; Perry, C.; Muggivan, A.; Quan, H.; Ghali, W.A. New ICD-10 version of the Charlson comorbidity index predicted in-hospital mortality. J. Clin. Epidemiol. 2004, 57, 1288–1294. [Google Scholar] [CrossRef]
- Peus, D.; Newcomb, N.; Hofer, S. Appraisal of the Karnofsky Performance Status and proposal of a simple algorithmic system for its evaluation. BMC Med. Inf. Decis. Mak. 2013, 13, 72. [Google Scholar] [CrossRef] [Green Version]
- Marks, L.B.; Yorke, E.D.; Jackson, A.; Ten Haken, R.K.; Constine, L.S.; Eisbruch, A.; Bentzen, S.M.; Nam, J.; Deasy, J.O. Use of normal tissue complication probability models in the clinic. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, S10–S19. [Google Scholar] [CrossRef] [Green Version]
- Agency for Healthcare Research and Quality. Patient Safety Indicators; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2015. [Google Scholar]
- U.S. Centers for Medicare & Medicaid Services. Hospital-Acquired Conditions; U.S. Centers for Medicare & Medicaid Services: Baltimore, MD, USA, 2020.
- Schneider, M.; Heimann, M.; Schaub, C.; Eichhorn, L.; Potthoff, A.L.; Giordano, F.A.; Güresir, E.; Ko, Y.D.; Landsberg, J.; Lehmann, F.; et al. Comorbidity Burden and Presence of Multiple Intracranial Lesions Are Associated with Adverse Events after Surgical Treatment of Patients with Brain Metastases. Cancers 2020, 12, 3209. [Google Scholar] [CrossRef] [PubMed]
- Schneider, M.; Ilic, I.; Potthoff, A.L.; Hamed, M.; Schäfer, N.; Velten, M.; Güresir, E.; Herrlinger, U.; Borger, V.; Vatter, H.; et al. Safety metric profiling in surgery for temporal glioblastoma: Lobectomy as a supra-total resection regime preserves perioperative standard quality rates. J. Neuro-Oncol. 2020, 149, 455–461. [Google Scholar] [CrossRef]
- Heimann, M.; Schäfer, N.; Bode, C.; Borger, V.; Eichhorn, L.; Giordano, F.A.; Güresir, E.; Jacobs, A.H.; Ko, Y.D.; Landsberg, J.; et al. Outcome of Elderly Patients With Surgically Treated Brain Metastases. Front. Oncol. 2021, 11, 713965. [Google Scholar] [CrossRef]
- Ilic, I.; Faron, A.; Heimann, M.; Potthoff, A.L.; Schäfer, N.; Bode, C.; Borger, V.; Eichhorn, L.; Giordano, F.A.; Güresir, E.; et al. Combined Assessment of Preoperative Frailty and Sarcopenia Allows the Prediction of Overall Survival in Patients with Lung Cancer (NSCLC) and Surgically Treated Brain Metastasis. Cancers 2021, 13, 3353. [Google Scholar] [CrossRef]
- Pilar, A.; Gupta, M.; Ghosh Laskar, S.; Laskar, S. Intraoperative radiotherapy: Review of techniques and results. Ecancermedicalscience 2017, 11, 750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barker, H.E.; Paget, J.T.; Khan, A.A.; Harrington, K.J. The tumour microenvironment after radiotherapy: Mechanisms of resistance and recurrence. Nat. Rev. Cancer 2015, 15, 409–425. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Dawood, H.; Giantini Larsen, A.; Fandino, L.; Knelson, E.H.; Smith, T.R.; Lee, E.Q.; Aizer, A.; Dunn, I.F.; Bi, W.L. Surgical and Peri-Operative Considerations for Brain Metastases. Front. Oncol. 2021, 11, 662943. [Google Scholar] [CrossRef] [PubMed]
- Schneider, M.; Borger, V.; Grigutsch, D.; Güresir, Á.; Potthoff, A.L.; Velten, M.; Vatter, H.; Güresir, E.; Schuss, P. Elevated body mass index facilitates early postoperative complications after surgery for intracranial meningioma. Neurosurg. Rev. 2021, 44, 1023–1029. [Google Scholar] [CrossRef] [PubMed]
- Cifarelli, C.P.; Jacobson, G.M. Intraoperative Radiotherapy in Brain Malignancies: Indications and Outcomes in Primary and Metastatic Brain Tumors. Front. Oncol. 2021, 11, 768168. [Google Scholar] [CrossRef]


{kind=link}
| Baseline Characteristics | n |
|---|---|
| Female sex | 18 (51%) |
| Median age (IQR) (in years) | 63 (54–71) |
| Primary site of cancer | |
| Lung | 21 (60%) |
| Melanoma | 4 (11%) |
| Breast | 2 (6%) |
| Others | 8 (23%) |
| Multiple BMs | 15 (43%) |
| Preoperative KPS ≥ 70 | 25 (71%) |
| Median CCI (IQR) | 10 (8–11) |
| ASA ≥ 3 | 24 (69%) |
| Median duration of surgery (IQR) | 272 (187–250) |
| Median dose of IORT (in Gy) | 30 (16–30) |
| Median duration of IORT (IQR) (in min) | 20 (17–21) |
| Perioperative complications | 4 (11%) |
| 30-day mortality | 2 (6%) |
| No. of Patients with IORT | n = 35 |
|---|---|
| No. of complications | 4 (11) |
| PSIs | |
| Postoperative hemorrhage | 1 (3) |
| Postoperative pulmonary embolism | 1 (3) |
| Postoperative sepsis (urinary tract infection) | 1 (3) |
| HACs | |
| Pneumonia | 1 (3) |
| Specific CSCs | 0 (0) |
| Variables | Surgery with IORT n = 35 | Surgery without IORT n = 105 | p-Value |
|---|---|---|---|
| Matching variables | |||
| Age (years) | 63 (54–71) † | 65 (56–73) † | 0.69 |
| Preoperative KPS | 80 (60–90) † | 80 (70–90) † | 0.73 |
| CCI | 10 (8–11) † | 9 (8–11) † | 0.74 |
| Primary site of cancer | 0.70 | ||
| Lung cancer | 21 (60) | 58 (55) | |
| Others | 14 (40) | 47 (45) | |
| Solitary versus multiple BM | 1.0 | ||
| Multiple BM | 15 (43) | 46 (44) | |
| Solitary BM | 20 (57) | 59 (56) | |
| Perioperative complications | 4 (11) | 19 (18) | 0.44 |
| PSIs | 3 (9) | 12 (11) | n.s. |
| HACs | 1 (3) | 3 (3) | n.s. |
| Specific CSCs | 0 (0) | 4 (4) | 0.04 |
| 30-day mortality | 2 (6) | 8 (8%) | 0.73 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamed, M.; Potthoff, A.-L.; Layer, J.P.; Koch, D.; Borger, V.; Heimann, M.; Scafa, D.; Sarria, G.R.; Holz, J.A.; Schmeel, F.C.; et al. Benchmarking Safety Indicators of Surgical Treatment of Brain Metastases Combined with Intraoperative Radiotherapy: Results of Prospective Observational Study with Comparative Matched-Pair Analysis. Cancers 2022, 14, 1515. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061515
Hamed M, Potthoff A-L, Layer JP, Koch D, Borger V, Heimann M, Scafa D, Sarria GR, Holz JA, Schmeel FC, et al. Benchmarking Safety Indicators of Surgical Treatment of Brain Metastases Combined with Intraoperative Radiotherapy: Results of Prospective Observational Study with Comparative Matched-Pair Analysis. Cancers. 2022; 14(6):1515. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061515
Chicago/Turabian StyleHamed, Motaz, Anna-Laura Potthoff, Julian P. Layer, David Koch, Valeri Borger, Muriel Heimann, Davide Scafa, Gustavo R. Sarria, Jasmin A. Holz, Frederic Carsten Schmeel, and et al. 2022. "Benchmarking Safety Indicators of Surgical Treatment of Brain Metastases Combined with Intraoperative Radiotherapy: Results of Prospective Observational Study with Comparative Matched-Pair Analysis" Cancers 14, no. 6: 1515. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061515