
Immunophenotypic Analysis of Acute Megakaryoblastic Leukemia: A EuroFlow Study

 , , , , , , and
, , , , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Immunophenotyping
2.3. Data Collection and Evaluation
2.4. Quality Assessment (QA) Procedure
2.5. Data Analysis and Statistics
3. Results
3.1. Patient Characteristics
3.2. Immunophenotypic Profile of AMKL versus Non-AMKL Patients: Univariate Analysis
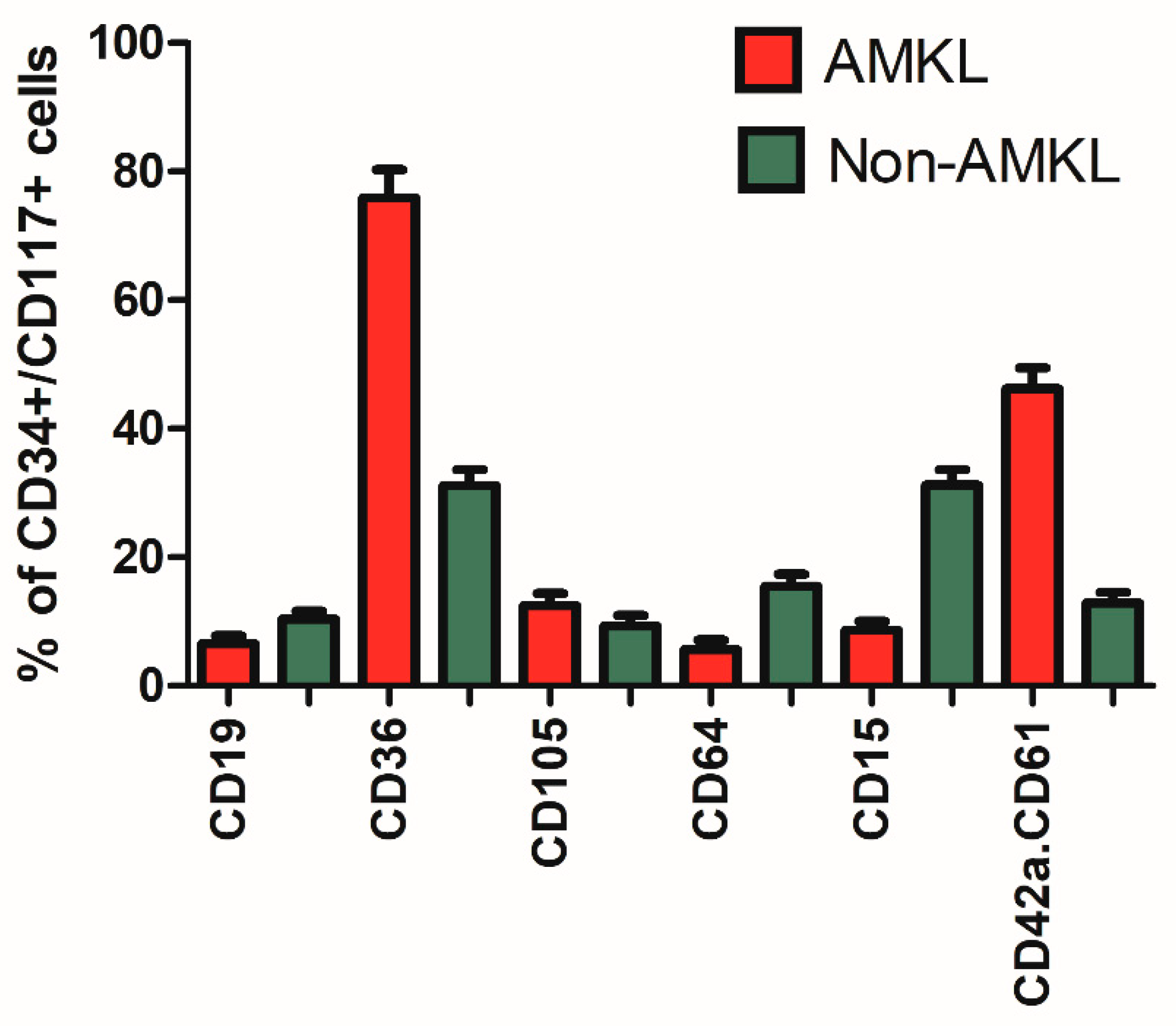
3.3. Expression of Megakaryocytic Markers
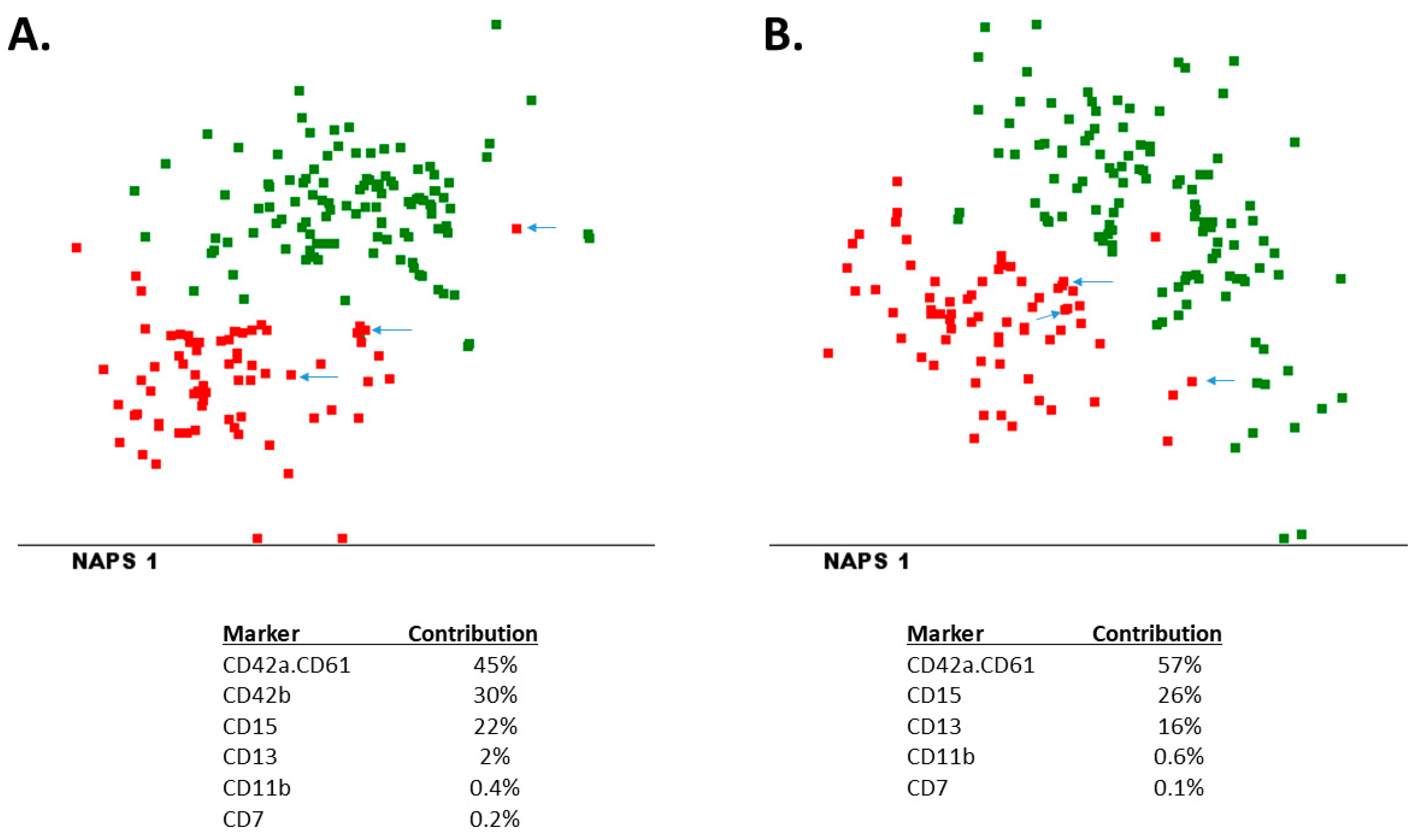
3.4. Immunophenotypic Profile of AMKL versus Non-AMKL: Multivariate Analysis
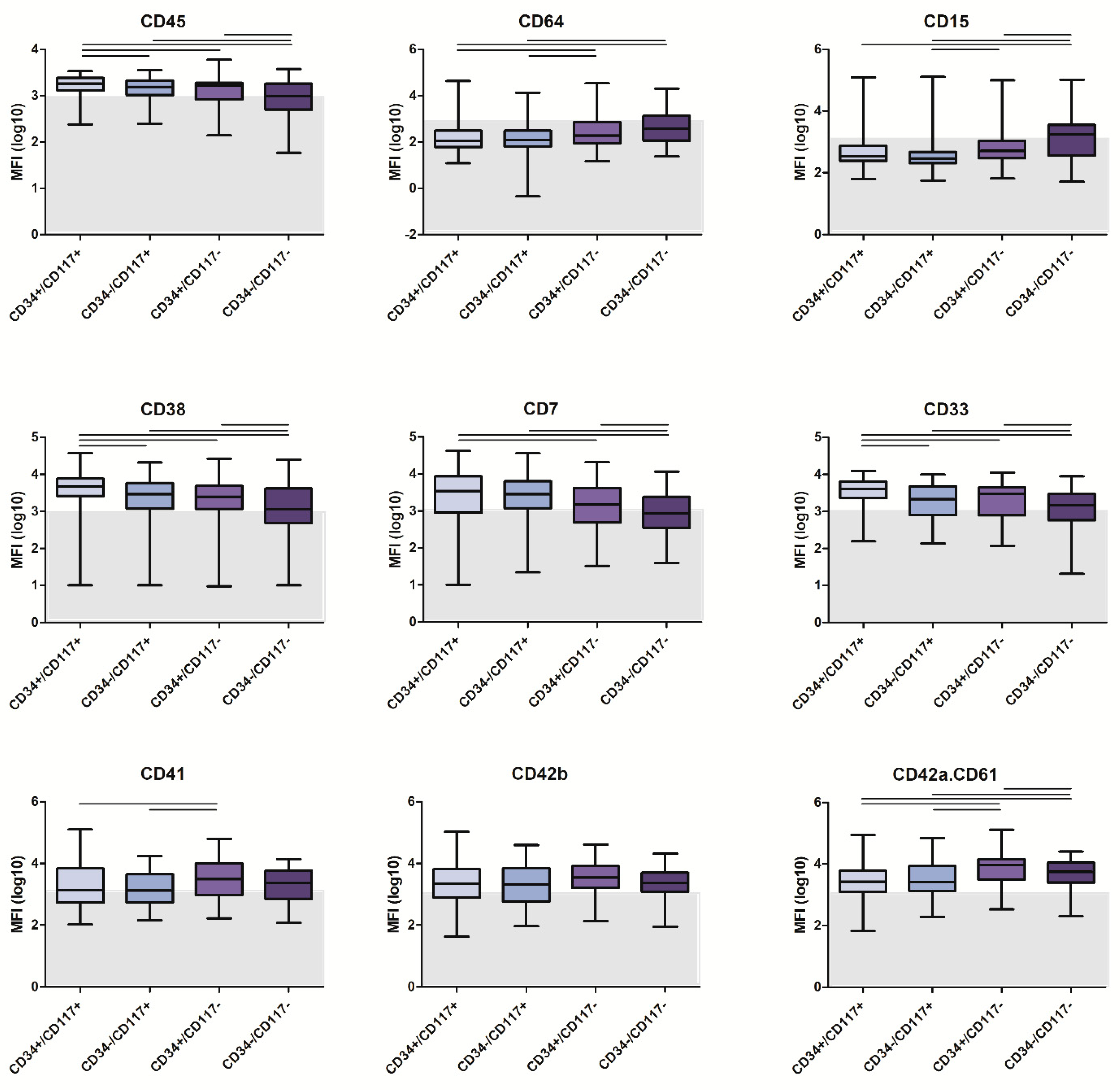
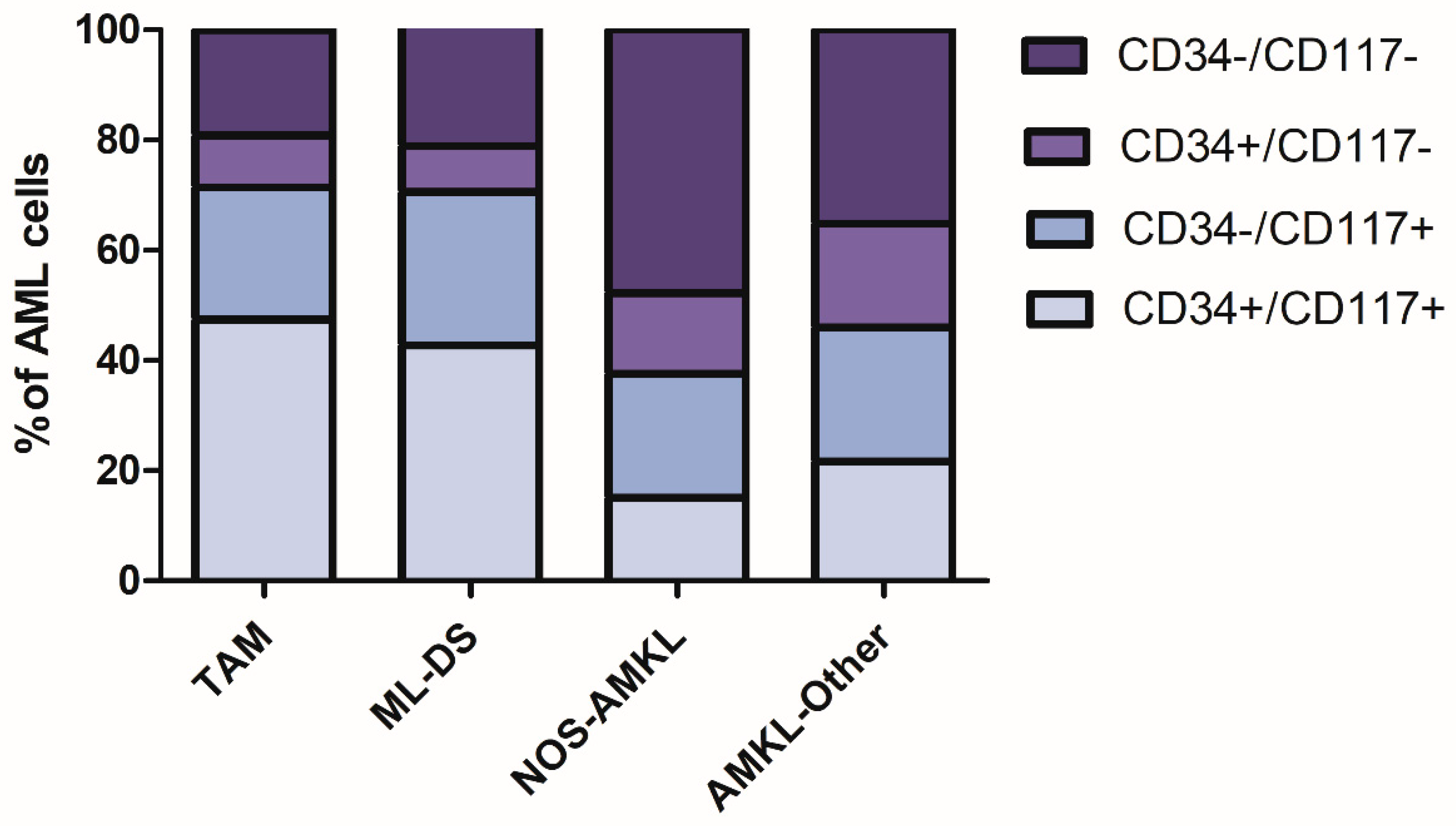
3.5. Maturation-Stage-Related Immunophenotypic Profiles
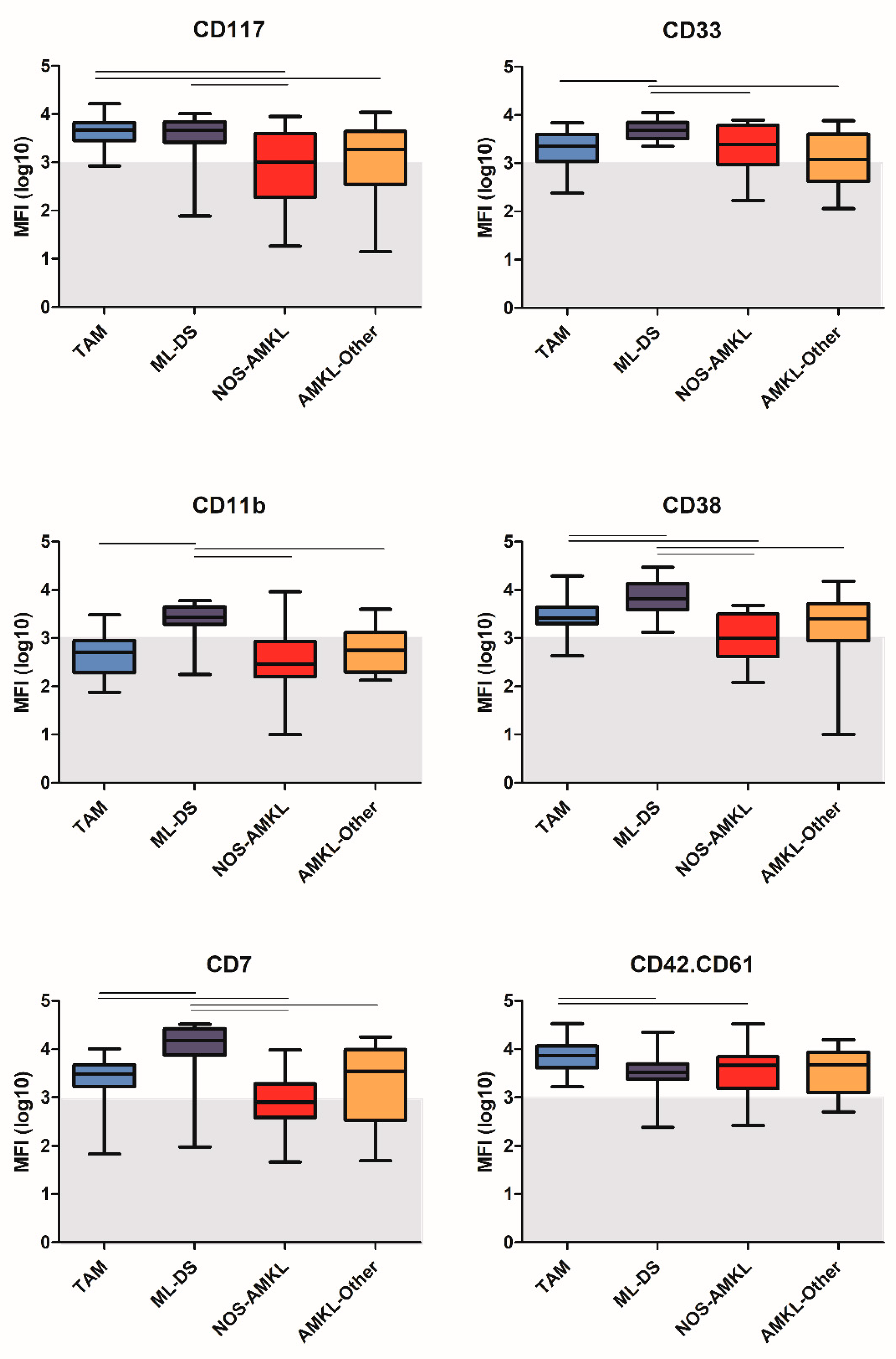
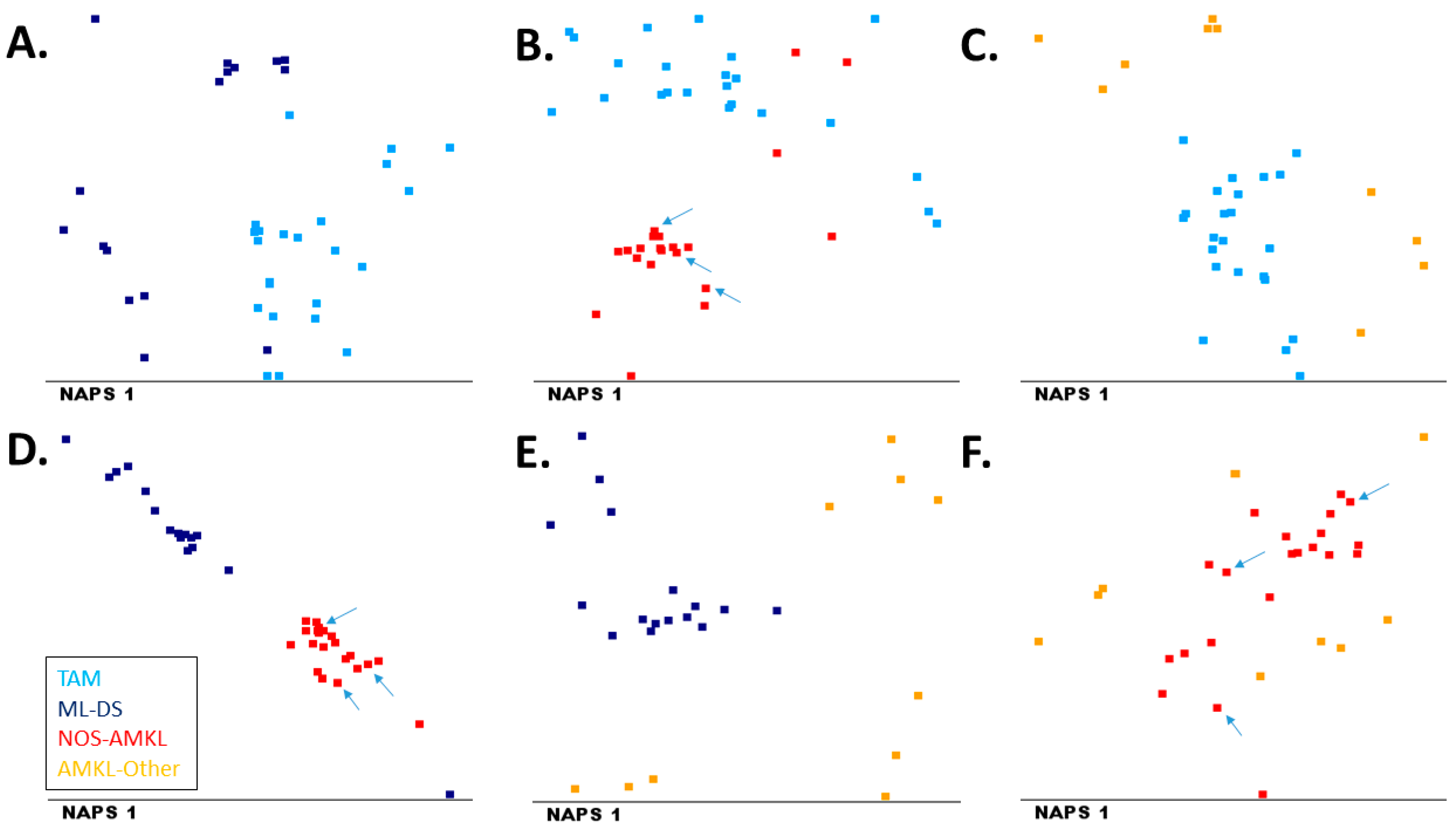
3.6. Immunophenotypic Variability within AMKL
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arber, D.A.; Baumann, I.; Niemeyer, C.; Brunning, R.D.; Porwit, A. Myeloid proliferations associated with Down Syndrome. In WHO Classification of Tumours Iof Haematopoietic and Lymphoid Tissue; International Agency for Research on Cancer: Lyon, France, 2017; pp. 169–171. [Google Scholar]
- Arber, D.A.; Brunning, R.D.; Le Beau, M.M.; Falini, B.; Vardiman, J.W.; Porwit, A.; Thiele, J.; Foucar, K.; Dohner, H.; Bloomfield, C.D. Acute myeloid leukemia with recurrent genetic abnormalities. In WHO Classification of Tumours Iof Haematopoietic and Lymphoid Tissue; International Agency for Research on Cancer: Lyon, France, 2017; pp. 130–149. [Google Scholar]
- Arber, D.A.; Brunning, R.D.; Orazi, A.; Bain, B.J.; Porwit, A.; Le Beau, M.M.; Greenberg, P. Acute myeloid leukemia with myelodysplasia-related changes. In WHO Classification of Tumours Iof Haematopoietic and Lymphoid Tissue; International Agency for Research on Cancer: Lyon, France, 2017; pp. 150–152. [Google Scholar]
- Arber, D.A.; Brunning, R.D.; Orazi, A.; Porwit, A.; Peterson, L.C.; Thiele, J.; Le Beau, M.M.; Hasserjian, R.P. Acute myeloid leukemia, NOS. In WHO Classification of Tumours Iof Haematopoietic and Lymphoid Tissue; International Agency for Research on Cancer: Lyon, France, 2017; pp. 156–166. [Google Scholar]
- Oki, Y.; Kantarjian, H.M.; Zhou, X.; Cortes, J.; Faderl, S.; Verstovsek, S.; O’Brien, S.; Koller, C.; Beran, M.; Bekele, B.N.; et al. Adult acute megakaryocytic leukemia: An analysis of 37 patients treated at M.D. Anderson Cancer Center. Blood 2006, 107, 880–884. [Google Scholar] [CrossRef] [Green Version]
- de Rooij, J.D.; Branstetter, C.; Ma, J.; Li, Y.; Walsh, M.P.; Cheng, J.; Obulkasim, A.; Dang, J.; Easton, J.; Verboon, L.J.; et al. Pediatric non-Down syndrome acute megakaryoblastic leukemia is characterized by distinct genomic subsets with varying outcomes. Nat. Genet. 2017, 49, 451–456. [Google Scholar] [CrossRef] [Green Version]
- Zhao, G.; Wu, W.; Wang, X.; Gu, J. Clinical diagnosis of adult patients with acute megakaryocytic leukemia. Oncol. Lett. 2018, 16, 6988–6997. [Google Scholar] [CrossRef]
- Hahn, A.W.; Li, B.; Prouet, P.; Giri, S.; Pathak, R.; Martin, M.G. Acute megakaryocytic leukemia: What have we learned. Blood Rev. 2016, 30, 49–53. [Google Scholar] [CrossRef]
- Hitzler, J.K.; Zipursky, A. Origins of leukaemia in children with Down syndrome. Nat. Rev. Cancer 2005, 5, 11–20. [Google Scholar] [CrossRef]
- Gamis, A.S.; Smith, F.O. Transient myeloproliferative disorder in children with Down syndrome: Clarity to this enigmatic disorder. Br. J. Haematol. 2012, 159, 277–287. [Google Scholar] [CrossRef]
- Bernstein, J.; Dastugue, N.; Haas, O.A.; Harbott, J.; Heerema, N.A.; Huret, J.L.; Landman-Parker, J.; LeBeau, M.M.; Leonard, C.; Mann, G.; et al. Nineteen cases of the t(1;22)(p13;q13) acute megakaryblastic leukaemia of infants/children and a review of 39 cases: Report from a t(1;22) study group. Leukemia 2000, 14, 216–218. [Google Scholar] [CrossRef] [Green Version]
- McElwaine, S.; Mulligan, C.; Groet, J.; Spinelli, M.; Rinaldi, A.; Denyer, G.; Mensah, A.; Cavani, S.; Baldo, C.; Dagna-Bricarelli, F.; et al. Microarray transcript profiling distinguishes the transient from the acute type of megakaryoblastic leukaemia (M7) in Down’s syndrome, revealing PRAME as a specific discriminating marker. Br. J. Haematol. 2004, 125, 729–742. [Google Scholar] [CrossRef]
- Yamato, G.; Park, M.J.; Sotomatsu, M.; Kaburagi, T.; Maruyama, K.; Kobayashi, T.; Nishi, A.; Sameshima, K.; Ohki, K.; Hayashi, Y. Clinical features of 35 Down syndrome patients with transient abnormal myelopoiesis at a single institution. Int. J. Hematol. 2021, 113, 662–667. [Google Scholar] [CrossRef]
- Athale, U.H.; Razzouk, B.I.; Raimondi, S.C.; Tong, X.; Behm, F.G.; Head, D.R.; Srivastava, D.K.; Rubnitz, J.E.; Bowman, L.; Pui, C.H.; et al. Biology and outcome of childhood acute megakaryoblastic leukemia: A single institution’s experience. Blood 2001, 97, 3727–3732. [Google Scholar] [CrossRef] [Green Version]
- Helleberg, C.; Knudsen, H.; Hansen, P.B.; Nikolajsen, K.; Kjaersgaard, E.; Ralfkiaer, E.; Johnsen, H.E. CD34+ megakaryoblastic leukaemic cells are CD38-, but CD61+ and glycophorin A+: Improved criteria for diagnosis of AML-M7? Leukemia 1997, 11, 830–834. [Google Scholar] [CrossRef] [Green Version]
- Klairmont, M.M.; Hoskoppal, D.; Yadak, N.; Choi, J.K. The Comparative Sensitivity of Immunohistochemical Markers of Megakaryocytic Differentiation in Acute Megakaryoblastic Leukemia. Am. J. Clin. Pathol. 2018, 150, 461–467. [Google Scholar] [CrossRef]
- Langebrake, C.; Creutzig, U.; Reinhardt, D. Immunophenotype of Down syndrome acute myeloid leukemia and transient myeloproliferative disease differs significantly from other diseases with morphologically identical or similar blasts. Klin. Padiatr. 2005, 217, 126–134. [Google Scholar] [CrossRef]
- Lorsbach, R.B. Megakaryoblastic disorders in children. Am. J. Clin. Pathol. 2004, 122, S33–S46. [Google Scholar] [CrossRef]
- van Dongen, J.J.; Lhermitte, L.; Bottcher, S.; Almeida, J.; van der Velden, V.H.; Flores-Montero, J.; Rawstron, A.; Asnafi, V.; Lecrevisse, Q.; Lucio, P.; et al. EuroFlow antibody panels for standardized n-dimensional flow cytometric immunophenotyping of normal, reactive and malignant leukocytes. Leukemia 2012, 26, 1908–1975. [Google Scholar] [CrossRef] [Green Version]
- Kalina, T.; Flores-Montero, J.; Lecrevisse, Q.; Pedreira, C.E.; van der Velden, V.H.; Novakova, M.; Mejstrikova, E.; Hrusak, O.; Bottcher, S.; Karsch, D.; et al. Quality assessment program for EuroFlow protocols: Summary results of four-year (2010–2013) quality assurance rounds. Cytom. A 2015, 87, 145–156. [Google Scholar] [CrossRef]
- Kalina, T.; Flores-Montero, J.; van der Velden, V.H.; Martin-Ayuso, M.; Bottcher, S.; Ritgen, M.; Almeida, J.; Lhermitte, L.; Asnafi, V.; Mendonca, A.; et al. EuroFlow standardization of flow cytometer instrument settings and immunophenotyping protocols. Leukemia 2012, 26, 1986–2010. [Google Scholar] [CrossRef] [Green Version]
- Glier, H.; Novakova, M.; Te Marvelde, J.; Bijkerk, A.; Morf, D.; Thurner, D.; Rejlova, K.; Lange, S.; Finke, J.; van der Sluijs-Gelling, A.; et al. Comments on EuroFlow standard operating procedures for instrument setup and compensation for BD FACS Canto, II., Navios and BD FACS Lyric instruments. J. Immunol. Methods 2019, 475, 112680. [Google Scholar] [CrossRef]
- Bras, A.E.; Beishuizen, A.; Langerak, A.W.; Jongen-Lavrencic, M.; Te Marvelde, J.G.; van den Heuvel-Eibrink, M.M.; Zwaan, C.M.; van Dongen, J.J.M.; van der Velden, V.H.J. CD38 expression in paediatric leukaemia and lymphoma: Implications for antibody targeted therapy. Br. J. Haematol. 2018, 180, 292–296. [Google Scholar] [CrossRef] [Green Version]
- Bras, A.E.; de Haas, V.; van Stigt, A.; Jongen-Lavrencic, M.; Beverloo, H.B.; Te Marvelde, J.G.; Zwaan, C.M.; van Dongen, J.J.M.; Leusen, J.H.W.; van der Velden, V.H.J. CD123 expression levels in 846 acute leukemia patients based on standardized immunophenotyping. Cytom. B Clin. Cytom. 2019, 96, 134–142. [Google Scholar] [CrossRef]
- Bras, A.E.; Osmani, Z.; de Haas, V.; Jongen-Lavrencic, M.; Te Marvelde, J.G.; Zwaan, C.M.; Mejstrikova, E.; Fernandez, P.; Szczepanski, T.; Orfao, A.; et al. Standardised immunophenotypic analysis of myeloperoxidase in acute leukaemia. Br. J. Haematol. 2021, 193, 922–927. [Google Scholar] [CrossRef]
- Bottcher, S.; Engelmann, R.; Grigore, G.; Fernandez, P.C.; Caetano, J.; Flores-Montero, J.; van der Velden, V.H.J.; Novakova, M.; Philippe, J.; Ritgen, M.; et al. Expert-independent classification of mature B-cell neoplasms using standardized flow cytometry: A multicentric study. Blood Adv. 2021, 6, 976–992. [Google Scholar] [CrossRef]
- Yang, W.; Wang, K.; Zuo, W. Neighborhood Component Feature Selection for High-Dimensional Data. J. Comput. 2012, 7, 161–168. [Google Scholar] [CrossRef]
- Salakhutdinov, R.; Hinton, G. Learning a Nonlinear Embedding by Preserving Class Neighbourhood Structure. In Proceedings of the Eleventh International Conference on Artificial Intelligence and Statistics, San Juan, PR, USA, 21–24 March 2007; Volume 2, pp. 409–412. [Google Scholar]
- Della Porta, M.G.; Travaglino, E.; Boveri, E.; Ponzoni, M.; Malcovati, L.; Papaemmanuil, E.; Rigolin, G.M.; Pascutto, C.; Croci, G.; Gianelli, U.; et al. Minimal morphological criteria for defining bone marrow dysplasia: A basis for clinical implementation of WHO classification of myelodysplastic syndromes. Leukemia 2015, 29, 66–75. [Google Scholar] [CrossRef]
- Matsuo, S.; Nishinaka-Arai, Y.; Kazuki, Y.; Oshimura, M.; Nakahata, T.; Niwa, A.; Saito, M.K. Pluripotent stem cell model of early hematopoiesis in Down syndrome reveals quantitative effects of short-form GATA1 protein on lineage specification. PLoS ONE 2021, 16, e0247595. [Google Scholar] [CrossRef]
- Boztug, H.; Schumich, A.; Potschger, U.; Muhlegger, N.; Kolenova, A.; Reinhardt, K.; Dworzak, M. Blast cell deficiency of CD11a as a marker of acute megakaryoblastic leukemia and transient myeloproliferative disease in children with and without Down syndrome. Cytom. B Clin. Cytom. 2013, 84, 370–378. [Google Scholar] [CrossRef]
- Savasan, S.; Buck, S.; Raimondi, S.C.; Becton, D.L.; Weinstein, H.; Chang, M.; Ravindranath, Y. CD36 (thrombospondin receptor) expression in childhood acute megakaryoblastic leukemia: In vitro drug sensitivity and outcome. Leuk Lymphoma 2006, 47, 2076–2083. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AMKL | Non-AMKL | |||||
|---|---|---|---|---|---|---|
| TAM | ML-DS | NOS-AMKL | AMKL-Other | all | ||
| n | 24 | 16 | 22 | 10 | 72 | 114 |
| Age in years (median, range) | 0 (0–0) | 1 (0–4) | 1 (0–89) | 62 (2–86) | 1 (0–89) | 14 (0–93) |
| Gender (M/F) | 12/12 | 8/8 | 13/9 | 6/4 | 39/33 | 60/54 |
| WBC × 109/L (median, range) | 49 (7–179) | 6 (2–35) | 21 (3–94) | 4 (2–16) | 14 (2–179) | 16 (1–441) |
| WHO classification | ||||||
| 3 | 3 | 0 | |||
| 6 | |||||
| 1 | 1 | 9 | |||
| 5 | |||||
| 5 | |||||
| 1 | |||||
| 1 | 1 | 27 | |||
| 5 | |||||
| 6 | 6 | 5 | |||
| 2 | |||||
| 4 | |||||
| 8 | |||||
| 8 | |||||
| 13 | |||||
| 12 | |||||
| 4 | |||||
| 2 | 2 | 0 |
| AMKL | Non-AMKL | Odds Ratio | 95% CI | p | ||||
|---|---|---|---|---|---|---|---|---|
| CD42a.CD61 | 66/72 | 92% | 11/114 | 10% | *# | 103.00 | 36.34 to 291.89 | <0.0001 |
| CD36 | 65/71 | 92% | 68/114 | 60% | *# | 7.32 | 2.93 to 18.32 | <0.0001 |
| CD71 | 65/72 | 90% | 65/114 | 57% | *# | 7.00 | 2.95 to 16.60 | <0.0001 |
| CD42b | 52/64 | 81% | 4/114 | 4% | *# | 119.17 | 36.67 to 387.31 | <0.0001 |
| CD38 | 56/70 | 80% | 97/114 | 85% | 0.70 | 0.32 to 1.53 | 0.3722 | |
| CD33 | 56/71 | 79% | 101/114 | 89% | # | 0.48 | 0.21 to 1.08 | 0.0766 |
| CD41 | 46/64 | 72% | 15/114 | 13% | *# | 15.18 | 7.13 to 32.31 | <0.0001 |
| CD7 | 50/71 | 70% | 36/114 | 32% | *# | 5.16 | 2.71 to 9.83 | <0.0001 |
| CD123 | 42/71 | 59% | 88/114 | 77% | *# | 0.43 | 0.22 to 0.82 | 0.0098 |
| CD11b | 27/70 | 39% | 76/114 | 67% | *# | 0.31 | 0.17 to 0.58 | 0.0002 |
| HLADR | 28/72 | 39% | 87/114 | 76% | *# | 0.20 | 0.10 to 0.37 | <0.0001 |
| CD15 | 25/70 | 36% | 77/114 | 68% | *# | 0.27 | 0.14 to 0.50 | <0.0001 |
| CD13 | 16/70 | 23% | 80/114 | 70% | *# | 0.20 | 0.11 to 0.38 | <0.0001 |
| CD64 | 9/70 | 13% | 46/114 | 40% | *# | 0.22 | 0.10 to 0.48 | 0.0002 |
| CD14 | 6/70 | 9% | 27/114 | 25% | *# | 0.30 | 0.12 to 0.77 | 0.0127 |
| CD105 | 6/71 | 8% | 5/114 | 4% | 2.01 | 0.59 to 6.86 | 0.2636 | |
| CD203c | 2/72 | 3% | 9/114 | 8% | # | 0.33 | 0.07 to 1.59 | 0.1680 |
| CD300e | 2/70 | 3% | 10/114 | 9% | # | 0.31 | 0.07 to 1.44 | 0.1338 |
| NG2 | 1/70 | 1% | 18/114 | 16% | *# | 0.08 | 0.01 to 0.59 | 0.0138 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brouwer, N.; Matarraz, S.; Nierkens, S.; Hofmans, M.; Nováková, M.; da Costa, E.S.; Fernandez, P.; Bras, A.E.; de Mello, F.V.; Mejstrikova, E.; et al. Immunophenotypic Analysis of Acute Megakaryoblastic Leukemia: A EuroFlow Study. Cancers 2022, 14, 1583. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061583
Brouwer N, Matarraz S, Nierkens S, Hofmans M, Nováková M, da Costa ES, Fernandez P, Bras AE, de Mello FV, Mejstrikova E, et al. Immunophenotypic Analysis of Acute Megakaryoblastic Leukemia: A EuroFlow Study. Cancers. 2022; 14(6):1583. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061583
Chicago/Turabian StyleBrouwer, Nienke, Sergio Matarraz, Stefan Nierkens, Mattias Hofmans, Michaela Nováková, Elaine Sobral da Costa, Paula Fernandez, Anne E. Bras, Fabiana Vieira de Mello, Ester Mejstrikova, and et al. 2022. "Immunophenotypic Analysis of Acute Megakaryoblastic Leukemia: A EuroFlow Study" Cancers 14, no. 6: 1583. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14061583