
Blood-Derived Liquid Biopsies Using Foundation One® Liquid CDx for Children and Adolescents with High-Risk Malignancies: A Monocentric Experience

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Genomic Analyses
2.3. Data
3. Results
3.1. Patients
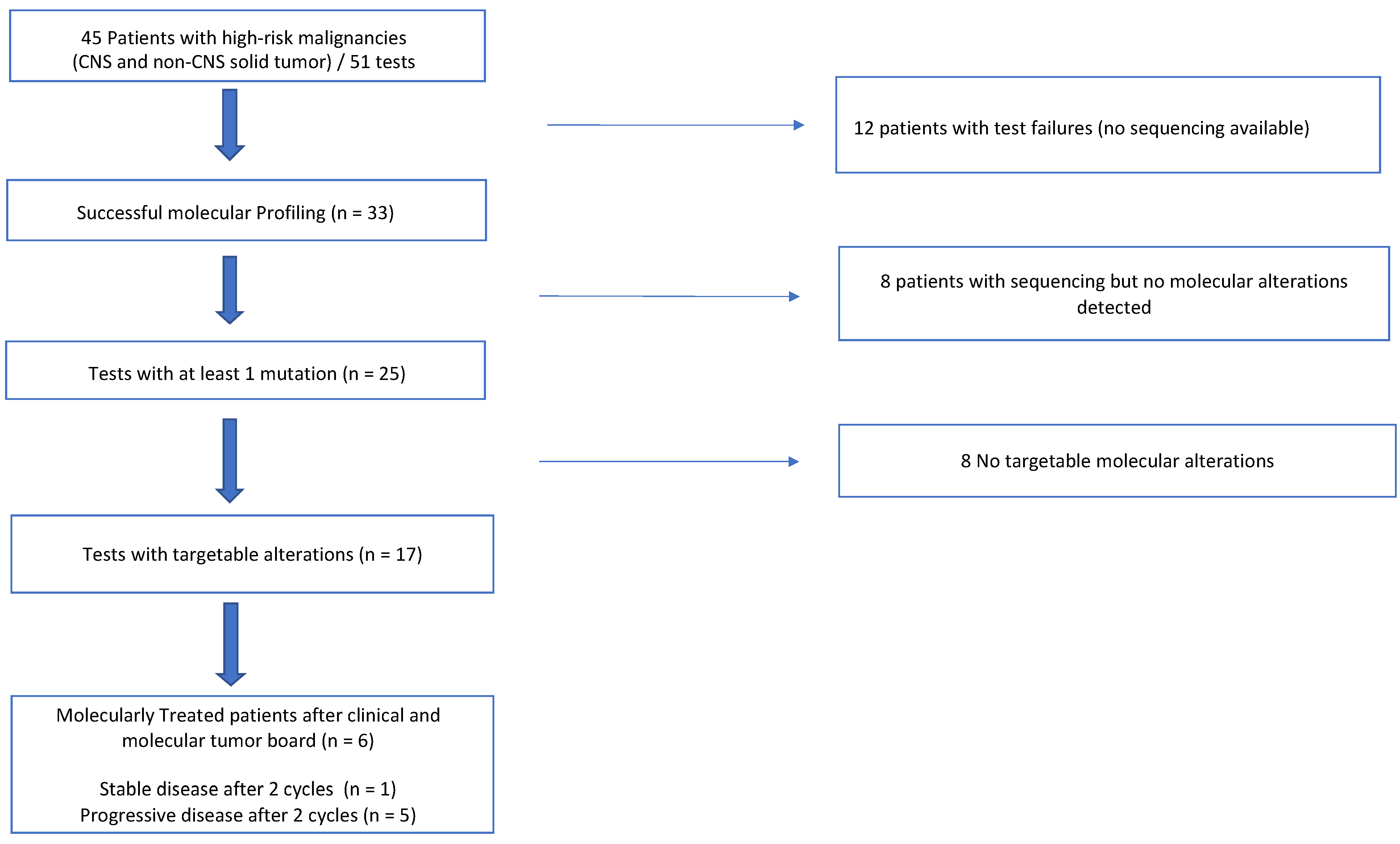
3.2. Feasibility
3.3. Molecular Alterations and Genes Alterations Found with LB
3.4. Molecular Alterations and Genes Alterations Found with Tissue Biopsies
3.5. Clinical Impact for Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.H.; DuBois, S.G.; Bender, J.L.G.; Kim, A.; Crompton, B.D.; Parker, E.; Dumont, I.P.; Hong, A.L.; Guo, D.; Church, A.; et al. Multicenter Feasibility Study of Tumor Molecular Profiling to Inform Therapeutic Decisions in Advanced Pediatric Solid Tumors: The Individualized Cancer Therapy (iCat) Study. JAMA Oncol. 2016, 2, 608–615. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortiz, M.V.; Kobos, R.; Walsh, M.; Slotkin, E.K.; Roberts, S.; Berger, M.F.; Hameed, M.; Solit, D.; Ladanyi, M.; Shukla, N.; et al. Integrating Genomics Into Clinical Pediatric Oncology Using the Molecular Tumor Board at the Memorial Sloan Kettering Cancer Center. Pediatr. Blood Cancer 2016, 63, 1368–1374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mody, R.J.; Prensner, J.R.; Everett, J.; Parsons, D.W.; Chinnaiyan, A.M. Precision medicine in pediatric oncology: Lessons learned and next steps. Pediatr. Blood Cancer 2017, 64, 10–1002. [Google Scholar] [CrossRef] [Green Version]
- Forrest, S.J.; Geoerger, B.; Janeway, K.A. Precision medicine in pediatric oncology. Curr. Opin. Pediatr. 2018, 30, 17–24. [Google Scholar] [CrossRef]
- Khater, F.; Vairy, S.; Langlois, S.; Dumoucel, S.; Sontag, T.; St-Onge, P.; Bittencourt, H.; Soglio, D.D.; Champagne, J.; Duval, M.; et al. Molecular Profiling of Hard-to-Treat Childhood and Adolescent Cancers. JAMA Netw. Open 2019, 2, e192906. [Google Scholar] [CrossRef]
- Langenberg, K.P.S.; Looze, E.J.; Molenaar, J.J. The Landscape of Pediatric Precision Oncology: Program Design, Actionable Alterations, and Clinical Trial Development. Cancers 2021, 13, 4324. [Google Scholar] [CrossRef]
- van Tilburg, C.M.; Pfaff, E.; Pajtler, K.W.; Langenberg, K.P.S.; Fiesel, P.; Jones, B.C.; Balasubramanian, G.P.; Stark, S.; Johann, P.D.; Blattner-Johnson, M.; et al. The Pediatric Precision Oncology INFORM Registry: Clinical Outcome and Benefit for Patients with Very High-Evidence Targets. Cancer Discov. 2021, 11, 2764–2779. [Google Scholar] [CrossRef]
- Berlanga, P.; Pierron, G.; Lacroix, L.; Chicard, M.; de Beaumais, T.A.; Marchais, A.; Harttrampf, A.C.; Iddir, Y.; Larive, A.; Fernandez, A.S.; et al. The European MAPPYACTS trial: Precision Medicine Program in Pediatric and Adolescent Patients with Recurrent Malignancies. Cancer Discov. 2022, 12, 1266–1281. [Google Scholar] [CrossRef]
- Parsons, D.W.; Janeway, K.A.; Patton, D.; Coffey, B.; Williams, P.M.; Hamilton, S.R.; Purkayastha, A.; Tsongalis, G.J.; Routbort, M.; Gastier-Foster, J.M.; et al. Identification of targetable molecular alterations in the NCI-COG Pediatric MATCH trial. J. Clin. Oncol. 2019, 37 (Suppl. 15), 10011. [Google Scholar] [CrossRef]
- Harttrampf, A.C.; Lacroix, L.; Deloger, M.; Deschamps, F.; Puget, S.; Auger, N.; Vielh, P.; Varlet, P.; Balogh, Z.; Abbou, S.; et al. Molecular Screening for Cancer Treatment Optimization (MOSCATO-01) in Pediatric Patients: A Single-Institutional Prospective Molecular Stratification Trial. Clin. Cancer Res. 2017, 23, 6101–6112. [Google Scholar] [CrossRef] [Green Version]
- Rothwell, D.G.; Ayub, M.; Cook, N.; Thistlethwaite, F.; Carter, L.; Dean, E.; Smith, N.; Villa, S.; Dransfield, J.; Clipson, A.; et al. Utility of ctDNA to support patient selection for early phase clinical trials: The TARGET study. Nat. Med. 2019, 25, 738–743. [Google Scholar] [CrossRef] [Green Version]
- Rijavec, E.; Coco, S.; Genova, C.; Rossi, G.; Longo, L.; Grossi, F. Liquid Biopsy in Non-Small Cell Lung Cancer: Highlights and Challenges. Cancers 2019, 12, 17. [Google Scholar] [CrossRef] [Green Version]
- Li, B.T.; Janku, F.; Jung, B.; Hou, C.; Madwani, K.; Alden, R.; Razavi, P.; Reis-Filho, J.S.; Shen, R.; Isbell, J.M.; et al. Ultra-deep next-generation sequencing of plasma cell-free DNA in patients with advanced lung cancers: Results from the Actionable Genome Consortium. Ann. Oncol. 2019, 30, 597–603. [Google Scholar] [CrossRef]
- Klega, K.; Imamovic-Tuco, A.; Ha, G.; Clapp, A.N.; Meyer, S.; Ward, A.; Clinton, C.; Nag, A.; van Allen, E.; Mullen, E.; et al. Detection of Somatic Structural Variants Enables Quantification and Characterization of Circulating Tumor DNA in Children With Solid Tumors. JCO Precis. Oncol. 2018, 2018, PO.17.00285. [Google Scholar] [CrossRef]
- van Paemel, R.; Vlug, R.; de Preter, K.; van Roy, N.; Speleman, F.; Willems, L.; Lammens, T.; Laureys, G.; Schleiermacher, G.; Tytgat, G.A.M.; et al. The pitfalls and promise of liquid biopsies for diagnosing and treating solid tumors in children: A review. Eur. J. Pediatr. 2020, 179, 191–202. [Google Scholar] [CrossRef] [Green Version]
- Stankunaite, R.; George, S.L.; Gallagher, L.; Jamal, S.; Shaikh, R.; Yuan, L.; Hughes, D.; Proszek, P.Z.; Carter, P.; Pietka, G.; et al. Circulating tumour DNA sequencing to determine therapeutic response and identify tumour heterogeneity in patients with paediatric solid tumours. Eur. J. Cancer 2022, 162, 209–220. [Google Scholar] [CrossRef]
- van Paemel, R.; Vandeputte, C.; Raman, L.; van Thorre, J.; Willems, L.; van Dorpe, J.; van der Linden, M.; de Wilde, J.; de Koker, A.; Menten, B.; et al. The feasibility of using liquid biopsies as a complementary assay for copy number aberration profiling in routinely collected paediatric cancer patient samples. Eur. J. Cancer 2022, 160, 12–23. [Google Scholar] [CrossRef]
- Izquierdo, E.; Proszek, P.; Pericoli, G.; Temelso, S.; Clarke, M.; Carvalho, D.M.; Mackay, A.; Marshall, L.V.; Carceller, F.; Hargrave, D.; et al. Droplet digital PCR-based detection of circulating tumor DNA from pediatric high grade and diffuse midline glioma patients. Neuro-Oncol. Adv. 2021, 3, vdab013. [Google Scholar] [CrossRef]
- Pagès, M.; Rotem, D.; Gydush, G.; Reed, S.; Rhoades, J.; Ha, G.; Lo, C.; Fleharty, M.; Duran, M.; Jones, R.; et al. Liquid biopsy detection of genomic alterations in pediatric brain tumors from cell-free DNA in peripheral blood, CSF, and urine. Neuro-Oncol 2022, noab299. [Google Scholar] [CrossRef]
- Research C for DE and FDA Approves Liquid Biopsy NGS Companion Diagnostic Test for Multiple Cancers and Biomarkers. FDA. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-liquid-biopsy-ngs-companion-diagnostic-test-multiple-cancers-and-biomarkers (accessed on 6 January 2022).
- Chakravarty, D.; Gao, J.; Phillips, S.M.; Kundra, R.; Zhang, H.; Wang, J.; Rudolph, J.E.; Yaeger, R.; Soumerai, T.; Nissan, M.H.; et al. OncoKB: A Precision Oncology Knowledge Base. JCO Precis. Oncol. 2017, 2017, PO.17.00011. [Google Scholar] [CrossRef]
- Liu, A.P.Y.; Smith, K.S.; Kumar, R.; Paul, L.; Bihannic, L.; Lin, T.; Maass, K.K.; Pajtler, K.W.; Chintagumpala, M.; Su, J.M.; et al. Serial assessment of measurable residual disease in medulloblastoma liquid biopsies. Cancer Cell 2021, 39, 1519–1530.e4. [Google Scholar] [CrossRef]
- Gröbner, S.N.; Worst, B.C.; Weischenfeldt, J.; Buchhalter, I.; Kleinheinz, K.; Rudneva, V.A.; Johann, P.D.; Balasubramanian, G.P.; Segura-Wang, M.; Brabetz, S.; et al. The landscape of genomic alterations across childhood cancers. Nature 2018, 555, 321–327. [Google Scholar] [CrossRef] [Green Version]
- George, S.L.; Izquierdo, E.; Campbell, J.; Koutroumanidou, E.; Proszek, P.; Jamal, S.; Hughes, D.; Yuan, L.; Marshall, L.V.; Carceller, F.; et al. A tailored molecular profiling programme for children with cancer to identify clinically actionable genetic alterations. Eur. J. Cancer 2019, 121, 224–235. [Google Scholar] [CrossRef]
- Clinical Practice Living Guidelines. Metastatic Non-Small-Cell Lung Cancer: ESMO Clinical Practice Guidelines for diagnosis, Treatment and Follow-Up. Available online: https://www.esmo.org/guidelines/lung-and-chest-tumours/clinical-practice-living-guidelines-metastatic-non-small-cell-lung-cancer (accessed on 16 February 2022).
- Li, W.; Liu, Ji.; Hou, Li.; Yu, F.; Zhang, J.; Wu, W.; Tang, X.; Sun, F.; Lu, H.; Deng, J.; et al. Liquid biopsy in lung cancer: Significance in diagnostics, prediction, and treatment monitoring. Mol. Cancer 2022, 21, 25. [Google Scholar] [CrossRef]
- Gouton, E.; Malissen, N.; André, N.; Jeanson, A.; Pelletier, A.; Testot-Ferry, A.; Gaudy-Marqueste, C.; Dahan, L.; Tabouret, E.; Chevalier, T.; et al. Clinical Impact of High Throughput Sequencing on Liquid Biopsy in Advanced Solid Cancer. Curr. Oncol. 2022, 29, 1902–1918. [Google Scholar] [CrossRef]
- Toutain, G.; Min, V.; Rome, A.; André, N. Trametinib for a BRAF G469A Missense Mutation in a Neuroblastoma Patient Unveiled by Liquid Biopsy. Authorea 2022. [Google Scholar] [CrossRef]
- Eckstein, O.S.; Allen, C.E.; Williams, P.M.; Roy-Chowdhuri, S.; Patton, D.R.; Coffey, B.; Reid, J.M.; Piao, J.; Saguilig, L.; Alonzo, T.A.; et al. Phase II Study of Selumetinib in Children and Young Adults with Tumors Harboring Activating Mitogen-Activated Protein Kinase Pathway Genetic Alterations: Arm E of the NCI-COG Pediatric MATCH Trial. J. Clin. Oncol. 2022, JCO2102840. [Google Scholar] [CrossRef]
- Bautista, F.; Paoletti, X.; Rubino, J.; Brard, C.; Rezai, K.; Nebchi, S.; Andre, N.; Aerts, I.; de Carli, E.; van Eijkelenburg, N.; et al. Phase I or II Study of Ribociclib in Combination With Topotecan-Temozolomide or Everolimus in Children With Advanced Malignancies: Arms A and B of the AcSé-ESMART Trial. J. Clin. Oncol. 2021, 39, 3546–3560. [Google Scholar] [CrossRef]
- Morscher, R.J.; Brard, C.; Berlanga, P.; Marshall, L.V.; André, N.; Rubino, J.; Aerts, I.; de Carli, E.; Corradini, N.; Nebchi, S.; et al. First-in-child phase I/II study of the dual mTORC1/2 inhibitor vistusertib (AZD2014) as monotherapy and in combination with topotecan-temozolomide in children with advanced malignancies: Arms E and F of the AcSé-ESMART trial. Eur. J. Cancer 2021, 157, 268–277. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Values | |
| Age (Years, Median, Range) | 11 (1.5–17) | |
| Gender (M/F) | 27/18 | |
| First line/relapse | 2/45 | |
| Presence of metastasis at the time of LB | 43 | |
| According to Pathology | Number of Patients | Successful LB n (%) |
| Neuroblastoma | 12 | 10 (83%) |
| Bone tumors | 12 | 8 (66%) |
| Ewing’s sarcoma | 5 | 4 (80%) |
| Osteosarcoma | 7 | 4 (57%) |
| Soft Tissue Sarcomas | 9 | 3 (33%) |
| Rhabdomyosarcoma | 3 | 2 |
| DSRCT | 2 | 1 |
| Malignant rhabdoid tumor | 1 | - |
| MPNST | 1 | - |
| BCOR fibromyxoid sarcoma | 1 | - |
| Intra-cardiac sarcoma | 1 | - |
| CNS tumors | 7 | 1 (14%) |
| Medulloblastoma | 4 | 1 |
| Unclassified embryonal tumor | 1 | - |
| High-grade glioma | 2 | - |
| Other tumors | 5 | 3 (60%) |
| Melanoma | 2 | 1 |
| UCNT | 1 | 1 |
| Adenocarcinoma | 1 | 1 |
| Teratoma | 1 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cahn, F.; Revon-Riviere, G.; Min, V.; Rome, A.; Filaine, P.; Pelletier, A.; Abed, S.; Gentet, J.-C.; Verschuur, A.; André, N. Blood-Derived Liquid Biopsies Using Foundation One® Liquid CDx for Children and Adolescents with High-Risk Malignancies: A Monocentric Experience. Cancers 2022, 14, 2774. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14112774
Cahn F, Revon-Riviere G, Min V, Rome A, Filaine P, Pelletier A, Abed S, Gentet J-C, Verschuur A, André N. Blood-Derived Liquid Biopsies Using Foundation One® Liquid CDx for Children and Adolescents with High-Risk Malignancies: A Monocentric Experience. Cancers. 2022; 14(11):2774. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14112774
Chicago/Turabian StyleCahn, Fanny, Gabriel Revon-Riviere, Victoria Min, Angélique Rome, Pauline Filaine, Annick Pelletier, Sylvie Abed, Jean-Claude Gentet, Arnauld Verschuur, and Nicolas André. 2022. "Blood-Derived Liquid Biopsies Using Foundation One® Liquid CDx for Children and Adolescents with High-Risk Malignancies: A Monocentric Experience" Cancers 14, no. 11: 2774. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14112774