
Central Nervous System Progression in Primary Vitreoretinal Lymphoma with Bilateral and Unilateral Involvement: A Systematic Review and Meta-Analysis

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
Objectives
2. Methods
2.1. Search Strategy and Study Selection
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Risk of Bias Assessment
2.5. Statistical Analysis/Meta-Analysis
3. Results
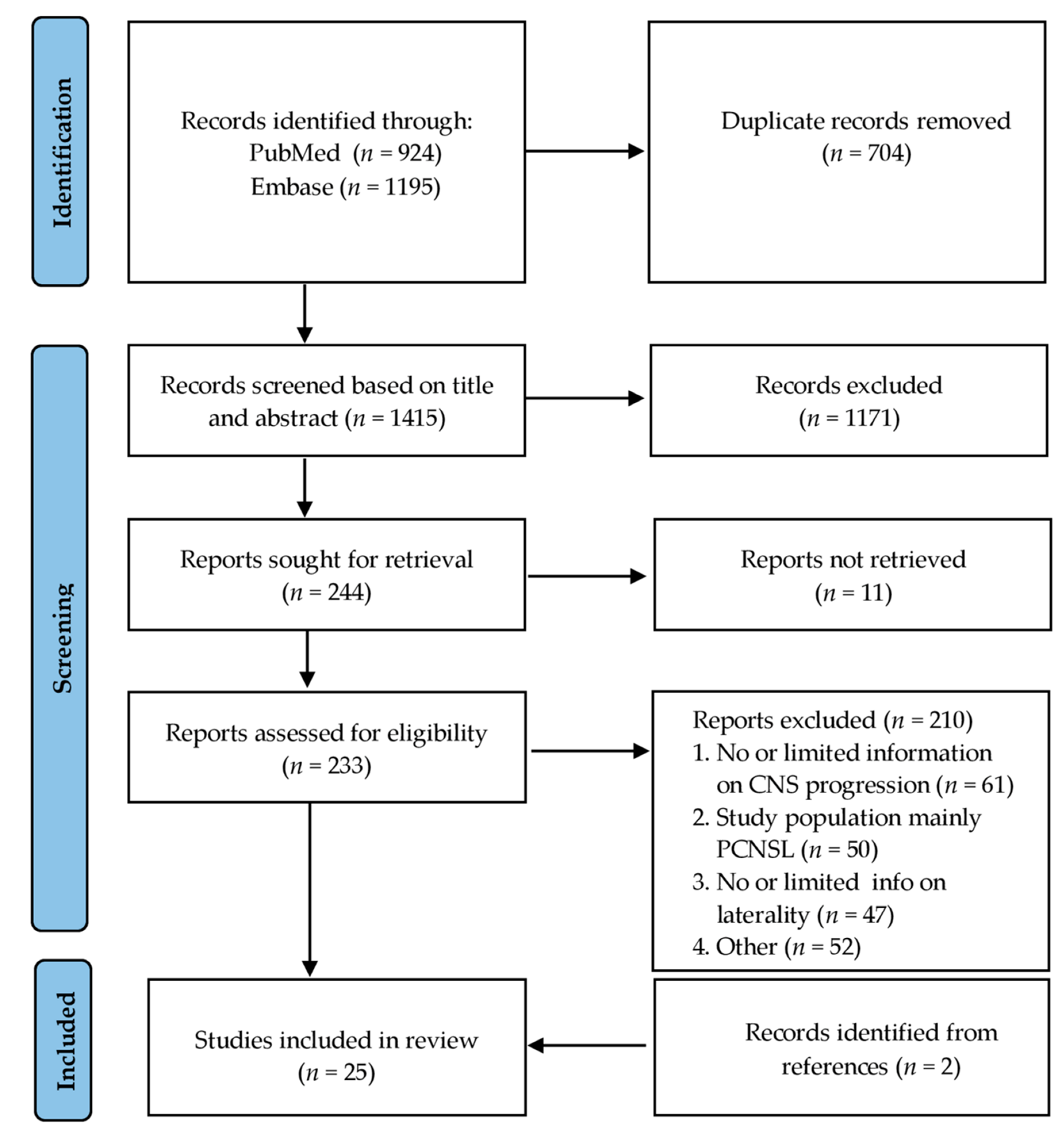
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias
3.4. CNS Progression in PVRL
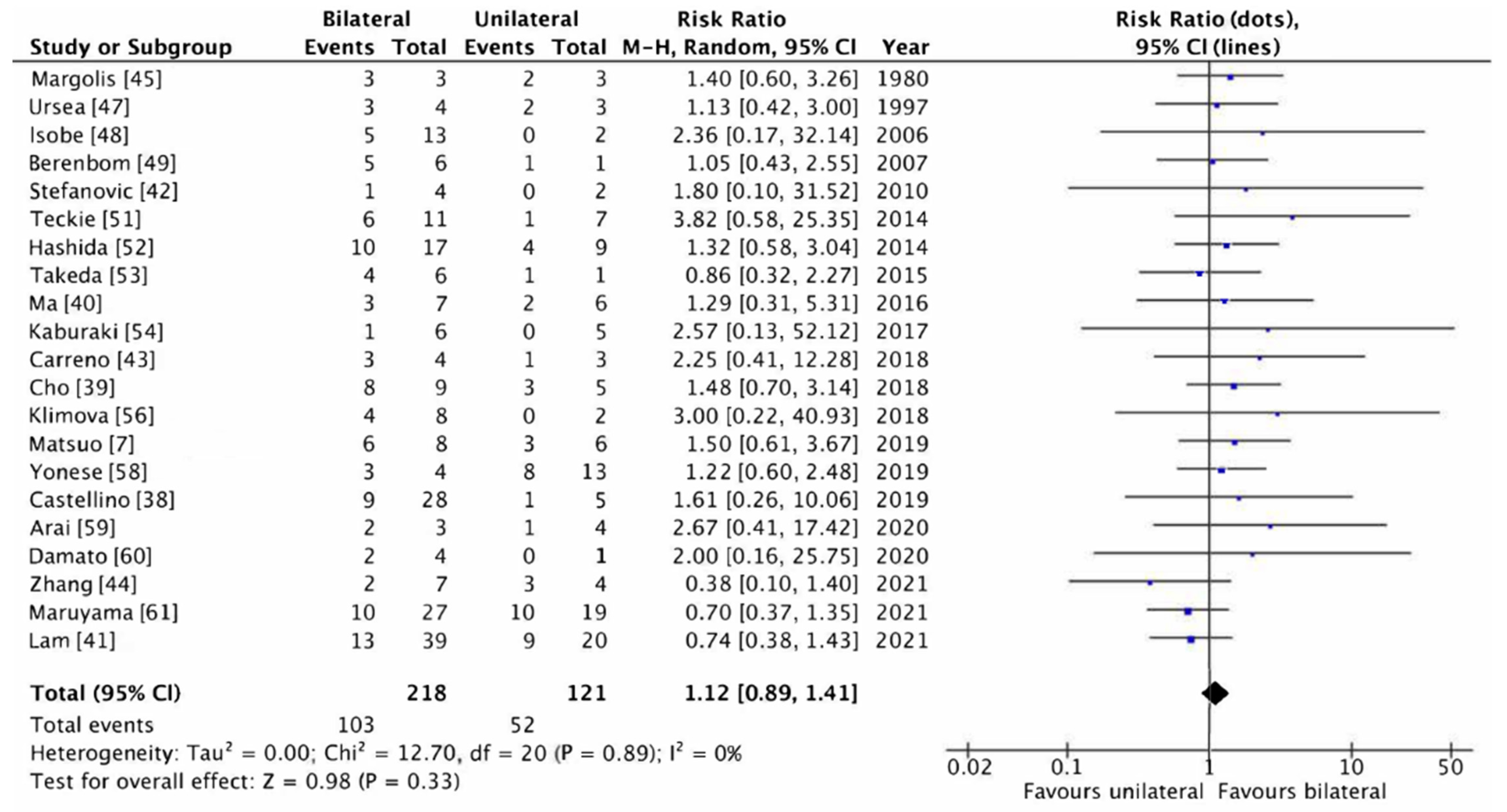
3.5. Meta-Analysis
4. Discussion
4.1. Strengths
4.2. Limitations
4.3. Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hormigo, A.; DeAngelis, L.M. Primary ocular lymphoma: Clinical features, diagnosis, and treatment. Clin. Lymphoma 2003, 4, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Gill, M.K.; Jampol, L.M. Variations in the presentation of primary intraocular lymphoma: Case reports and a review. Surv. Ophthalmol. 2001, 45, 463–471. [Google Scholar] [CrossRef]
- Choi, J.Y.; Kafkala, C.; Foster, C.S. Primary intraocular lymphoma: A review. Semin. Ophthalmol. 2006, 21, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Grimm, S.A.; Pulido, J.S.; Jahnke, K.; Schiff, D.; Hall, A.J.; Shenkier, T.N.; Siegal, T.; Doolittle, N.D.; Batchelor, T.; Herrlinger, U.; et al. Primary intraocular lymphoma: An International Primary Central Nervous System Lymphoma Collaborative Group Report. Ann. Oncol. 2007, 18, 1851–1855. [Google Scholar] [CrossRef]
- Kimura, K.; Usui, Y.; Goto, H.; Japanese Intraocular Lymphoma Study Group. Clinical features and diagnostic significance of the intraocular fluid of 217 patients with intraocular lymphoma. Jpn. J. Ophthalmol. 2012, 56, 383–389. [Google Scholar] [CrossRef]
- Char, D.H.; Ljung, B.M.; Miller, T.; Phillips, T. Primary intraocular lymphoma (ocular reticulum cell sarcoma) diagnosis and management. Ophthalmology 1988, 95, 625–630. [Google Scholar] [CrossRef]
- Matsuo, T.; Tanaka, T. Are there primary intraocular lymphomas that do not develop into central nervous system lymphomas? J. Clin. Exp. Hematop 2019, 59, 168–174. [Google Scholar] [CrossRef] [Green Version]
- Tang, L.J.; Gu, C.L.; Zhang, P. Intraocular lymphoma. Int. J. Ophthalmol. 2017, 10, 1301–1307. [Google Scholar] [CrossRef]
- Chan, C.C.; Sen, H.N. Current concepts in diagnosing and managing primary vitreoretinal (intraocular) lymphoma. Discov. Med. 2013, 15, 93–100. [Google Scholar]
- Coupland, S.E.; Heimann, H.; Bechrakis, N.E. Primary intraocular lymphoma: A review of the clinical, histopathological and molecular biological features. Graefes Arch. Clin. Exp. Ophthalmol. 2004, 242, 901–913. [Google Scholar] [CrossRef]
- Riemens, A.; Bromberg, J.; Touitou, V.; Sobolewska, B.; Missotten, T.; Baarsma, S.; Hoyng, C.; Cordero-Coma, M.; Tomkins-Netzer, O.; Rozalski, A.; et al. Treatment strategies in primary vitreoretinal lymphoma: A 17-center European collaborative study. JAMA Ophthalmol. 2015, 133, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayden, J.A.; van der Windt, D.A.; Cartwright, J.L.; Côté, P.; Bombardier, C. Assessing bias in studies of prognostic factors. Ann. Intern. Med. 2013, 158, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Review Manager (RevMan) [Computer Program]; Version 5.4; The Cochrane Collaboration: London, UK, 2020.
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Giuffrè, C.; Cicinelli, M.V.; Marchese, A.; Modorati, G.M.; Brambati, M.; Ferreri, A.J.M.; Calimeri, T.; Ponzoni, M.; Bandello, F.; Miserocchi, E. Clinical Experience in a Large Cohort of Patients with Vitreoretinal Lymphoma in a Single Center. Ocul. Immunol. Inflamm. 2021, 29, 472–478. [Google Scholar] [CrossRef]
- Lavine, J.A.; Singh, A.D.; Sharma, S.; Baynes, K.; Lowder, C.Y.; Srivastava, S.K. Ultra-Widefield Multimodal Imaging of Primary Vitreoretinal Lymphoma. Retina 2019, 39, 1861–1871. [Google Scholar] [CrossRef]
- Abu Samra, K.; Oray, M.; Ebrahimiadib, N.; Lee, S.; Anesi, S.; Foster, C.S. Intraocular Lymphoma: Descriptive Data of 26 Patients Including Clinico-pathologic Features, Vitreous Findings, and Treatment Outcomes. Ocul. Immunol. Inflamm. 2018, 26, 347–352. [Google Scholar] [CrossRef]
- Hashida, N.; Ohguro, N.; Nishida, K. Efficacy and Complications of Intravitreal Rituximab Injection for Treating Primary Vitreoretinal Lymphoma. Transl. Vis. Sci. Technol. 2012, 1, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raparia, K.; Chang, C.C.; Chévez-Barrios, P. Intraocular lymphoma: Diagnostic approach and immunophenotypic findings in vitrectomy specimens. Arch. Pathol Lab. Med. 2009, 133, 1233–1237. [Google Scholar] [CrossRef]
- Jahnke, K.; Korfel, A.; Komm, J.; Bechrakis, N.E.; Stein, H.; Thiel, E.; Coupland, S.E. Intraocular lymphoma 2000–2005: Results of a retrospective multicentre trial. Graefes Arch. Clin. Exp. Ophthalmol. 2006, 244, 663–669. [Google Scholar] [CrossRef]
- Coupland, S.E.; Bechrakis, N.E.; Anastassiou, G.; Foerster, A.M.; Heiligenhaus, A.; Pleyer, U.; Hummel, M.; Stein, H. Evaluation of vitrectomy specimens and chorioretinal biopsies in the diagnosis of primary intraocular lymphoma in patients with Masquerade syndrome. Graefes Arch. Clin. Exp. Ophthalmol. 2003, 241, 860–870. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, P.M.; McKelvie, P.; Hall, A.J.; Stawell, R.J.; Santamaria, J.D. Intraocular lymphoma: A series of 14 patients with clinicopathological features and treatment outcomes. Eye 2003, 17, 513–521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cassoux, N.; Merle-Beral, H.; Leblond, V.; Bodaghi, B.; Miléa, D.; Gerber, S.; Fardeau, C.; Reux, I.; Xuan, K.H.; Chan, C.C.; et al. Ocular and central nervous system lymphoma: Clinical features and diagnosis. Ocul. Immunol. Inflamm. 2000, 8, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Akpek, E.K.; Ahmed, I.; Hochberg, F.H.; Soheilian, M.; Dryja, T.P.; Jakobiec, F.A.; Foster, C.S. Intraocular-central nervous system lymphoma: Clinical features, diagnosis, and outcomes. Ophthalmology 1999, 106, 1805–1810. [Google Scholar] [CrossRef]
- Minezaki, T.; Usui, Y.; Asakage, M.; Takanashi, M.; Shimizu, H.; Nezu, N.; Narimatsu, A.; Tsubota, K.; Umazume, K.; Yamakawa, N.; et al. High-Throughput MicroRNA Profiling of Vitreoretinal Lymphoma: Vitreous and Serum MicroRNA Profiles Distinct from Uveitis. J. Clin. Med. 2020, 9, 1844. [Google Scholar] [CrossRef] [PubMed]
- Cheah, C.Y.; Milgrom, S.; Chihara, D.; Gombos, D.S.; Pinnix, C.C.; Dabaja, B.S.; Fowler, N.H. Intensive chemoimmunotherapy and bilateral globe irradiation as initial therapy for primary intraocular lymphoma. Neuro Oncol. 2016, 18, 575–581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.; Kim, M.J.; Kim, J.S.; Oh, S.Y.; Kim, S.J.; Kwon, Y.H.; Chung, I.Y.; Kang, J.H.; Yang, D.H.; Kang, H.J.; et al. Intraocular lymphoma in Korea: The Consortium for Improving Survival of Lymphoma (CISL) study. Blood Res. 2015, 50, 242–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Sato-Otsubo, A.; Sugita, S.; Takase, H.; Mochizuki, M.; Usui, Y.; Goto, H.; Koyama, T.; Akiyama, H.; Miura, O.; et al. High-resolution genomic copy number profiling of primary intraocular lymphoma by single nucleotide polymorphism microarrays. Cancer Sci. 2014, 105, 592–599. [Google Scholar] [CrossRef] [Green Version]
- Levasseur, S.D.; Wittenberg, L.A.; White, V.A. Vitreoretinal lymphoma: A 20-year review of incidence, clinical and cytologic features, treatment, and outcomes. JAMA Ophthalmol. 2013, 131, 505. [Google Scholar] [CrossRef] [Green Version]
- Wallace, D.J.; Shen, D.; Reed, G.F.; Miyanaga, M.; Mochizuki, M.; Sen, H.N.; Dahr, S.S.; Buggage, R.R.; Nussenblatt, R.B.; Chan, C.C. Detection of the bcl-2 t(14;18) translocation and proto-oncogene expression in primary intraocular lymphoma. Investig. Ophthalmol. Vis. Sci. 2006, 47, 2750–2756. [Google Scholar] [CrossRef] [Green Version]
- Baehring, J.M.; Androudi, S.; Longtine, J.J.; Betensky, R.A.; Sklar, J.; Foster, C.S.; Hochberg, F.H. Analysis of clonal immunoglobulin heavy chain rearrangements in ocular lymphoma. Cancer 2005, 104, 591–597. [Google Scholar] [CrossRef]
- Kim, M.M.; Dabaja, B.S.; Medeiros, J.; Kim, S.; Allen, P.; Chevez-Barrios, P.; Gombos, D.S.; Fowler, N. Survival Outcomes of Primary Intraocular Lymphoma: A Single-institution Experience. Am. J. Clin. Oncol. 2016, 39, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Mikami, R.; Nakayama, H.; Goto, H.; Kimura, K.; Usui, Y.; Nogi, S.; Tajima, Y.; Okubo, M.; Kanesaka, N.; Sugahara, S.; et al. Preliminary results of radiotherapy for primary intraocular non-Hodgkin lymphoma. Leuk. Lymphoma 2013, 54, 2181–2184. [Google Scholar] [CrossRef] [PubMed]
- Hormigo, A.; Abrey, L.; Heinemann, M.H.; DeAngelis, L.M. Ocular presentation of primary central nervous system lymphoma: Diagnosis and treatment. Br. J. Haematol. 2004, 126, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Peterson, K.; Gordon, K.B.; Heinemann, M.H.; DeAngelis, L.M. The clinical spectrum of ocular lymphoma. Cancer 1993, 72, 843–849. [Google Scholar] [CrossRef]
- Castellino, A.; Pulido, J.S.; Johnston, P.B.; Ristow, K.M.; Nora Bennani, N.; Inwards, D.J.; Macon, W.R.; Micallef, I.N.M.; King, R.L.; Salomao, D.R.; et al. Role of systemic high-dose methotrexate and combined approaches in the management of vitreoretinal lymphoma: A single center experience 1990–2018. Am. J. Hematol. 2019, 94, 291–298. [Google Scholar] [CrossRef]
- Cho, B.J.; Kim, D.Y.; Park, U.C.; Lee, J.Y.; Yoon, Y.H.; Yu, H.G. Clinical Features and Treatment Outcomes of Vitreoretinal Lymphoma according to Its Association with CNS Lymphoma. Ocul. Immunol. Inflamm. 2018, 26, 365–371. [Google Scholar] [CrossRef]
- Ma, W.L.; Hou, H.A.; Hsu, Y.J.; Chen, Y.K.; Tang, J.L.; Tsay, W.; Yeh, P.T.; Yang, C.M.; Lin, C.P.; Tien, H.F. Clinical outcomes of primary intraocular lymphoma patients treated with front-line systemic high-dose methotrexate and intravitreal methotrexate injection. Ann. Hematol. 2016, 95, 593–601. [Google Scholar] [CrossRef]
- Lam, M.; Touitou, V.; Choquet, S.; Cassoux, N.; Ghesquières, H.; Kodjikian, L.; Schmitt, A.; Gattoussi, S.; Tabouret, É.; Sampo, M.; et al. Intravenous high-dose methotrexate based systemic therapy in the treatment of isolated primary vitreoretinal lymphoma: A LOC network study. Am. J. Hematol. 2021, 96, 823–833. [Google Scholar] [CrossRef]
- Stefanovic, A.; Davis, J.; Murray, T.; Markoe, A.; Lossos, I.S. Treatment of isolated primary intraocular lymphoma with high-dose methotrexate-based chemotherapy and binocular radiation therapy: A single-institution experience. Br. J. Haematol. 2010, 151, 103–106. [Google Scholar] [CrossRef] [Green Version]
- Carreno, E.; Clench, T.; Steeples, L.R.; Salvatore, S.; Lee, R.W.J.; Dick, A.D.; Pawade, J. Clinical spectrum of vitreoretinal lymphoma and its association with MyD88 L265P mutation. Acta Ophthalmol. 2019, 97, 138–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Zhang, X.; Zou, D.; Yin, J.; Zhang, L.; Wang, X.; Jia, C.; Wang, W.; Zhao, D.; Zhou, D.; et al. Lenalidomide and Rituximab Regimen Combined with Intravitreal Methotrexate Followed by Lenalidomide Maintenance for Primary Vitreoretinal Lymphoma: A Prospective Phase II Study. Front. Oncol. 2021, 11, 701507. [Google Scholar] [CrossRef] [PubMed]
- Margolis, L.; Fraser, R.; Lichter, A.; Char, D.H. The role of radiation therapy in the management of ocular reticulum cell sarcoma. Cancer 1980, 45, 688–692. [Google Scholar] [CrossRef]
- Soussain, C.; Merle-Béral, H.; Reux, I.; Sutton, L.; Fardeau, C.; Gerber, S.; Ben Othman, T.; Binet, J.L.; Lehoang, P.; Leblond, V. A single-center study of 11 patients with intraocular lymphoma treated with conventional chemotherapy followed by high-dose chemotherapy and autologous bone marrow transplantation in 5 cases. Leuk. Lymphoma 1996, 23, 339–345. [Google Scholar] [CrossRef]
- Ursea, R.; Heinemann, M.H.; Silverman, R.H.; Deangelis, L.M.; Daly, S.W.; Coleman, D.J. Ophthalmic, ultrasonographic findings in primary central nervous system lymphoma with ocular involvement. Retina 1997, 17, 118–123. [Google Scholar] [CrossRef]
- Isobe, K.; Ejima, Y.; Tokumaru, S.; Shikama, N.; Suzuki, G.; Takemoto, M.; Tsuchida, E.; Nomura, M.; Shibamoto, Y.; Hayabuchi, N. Treatment of primary intraocular lymphoma with radiation therapy: A multi-institutional survey in Japan. Leuk Lymphoma 2006, 47, 1800–1805. [Google Scholar] [CrossRef]
- Berenbom, A.; Davila, R.M.; Lin, H.S.; Harbour, J.W. Treatment outcomes for primary intraocular lymphoma: Implications for external beam radiotherapy. Eye 2007, 21, 1198–1201. [Google Scholar] [CrossRef] [Green Version]
- Karma, A.; von Willebrand, E.O.; Tommila, P.V.; Paetau, A.E.; Oskala, P.S.; Immonen, I.J. Primary intraocular lymphoma: Improving the diagnostic procedure. Ophthalmology 2007, 114, 1372–1377. [Google Scholar] [CrossRef]
- Teckie, S.; Yahalom, J. Primary intraocular lymphoma: Treatment outcomes with ocular radiation therapy alone. Leuk Lymphoma 2014, 55, 795–801. [Google Scholar] [CrossRef]
- Hashida, N.; Nakai, K.; Saitoh, N.; Nishida, K. Association between ocular findings and preventive therapy with onset of central nervous system involvement in patients with primary vitreoretinal lymphoma. Graefes Arch. Clin. Exp. Ophthalmol. 2014, 252, 687–693. [Google Scholar] [CrossRef]
- Takeda, A.; Yoshikawa, H.; Fukuhara, T.; Hikita, S.; Hijioka, K.; Otomo, T.; Arita, R.; Hisatomi, T.; Kimura, K.; Yoshida, S.; et al. Distinct Profiles of Soluble Cytokine Receptors Between B-Cell Vitreoretinal Lymphoma and Uveitis. Investig. Ophthalmol. Vis. Sci. 2015, 56, 7516–7523. [Google Scholar] [CrossRef] [PubMed]
- Kaburaki, T.; Taoka, K.; Matsuda, J.; Yamashita, H.; Matsuda, I.; Tsuji, H.; Tanaka, R.; Nakazaki, K.; Nakamura, F.; Kamiya, K.; et al. Combined intravitreal methotrexate and immunochemotherapy followed by reduced-dose whole-brain radiotherapy for newly diagnosed B-cell primary intraocular lymphoma. Br. J. Haematol. 2017, 179, 246–255. [Google Scholar] [CrossRef] [PubMed]
- Mahajan, S.; Nijhawan, R.; Rajwanshi, A.; Karkhur, S.; Mulkutar, S.; Dogra, M.; Lal, V.; Gupta, V.; Gupta, A. Clinical characteristics of primary vitreoretinal lymphoma in an Indian population. Ocul. Immunol. Inflamm. 2017, 25, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Klimova, A.; Heissigerova, J.; Rihova, E.; Brichova, M.; Pytlik, R.; Spicka, I.; Mrazova, K.; Karolova, J.; Svozilkova, P. Combined treatment of primary vitreoretinal lymphomas significantly prolongs the time to first relapse. Br. J. Ophthalmol. 2018, 102, 1579–1585. [Google Scholar] [CrossRef] [PubMed]
- de la Fuente, M.I.; Alderuccio, J.P.; Reis, I.M.; Omuro, A.; Markoe, A.; Echegaray, J.J.; Davis, J.L.; Harbour, J.W.; Lossos, I.S. Bilateral radiation therapy followed by methotrexate-based chemotherapy for primary vitreoretinal lymphoma. Am. J. Hematol. 2019, 94, 455–460. [Google Scholar] [CrossRef]
- Yonese, I.; Takase, H.; Yoshimori, M.; Onozawa, E.; Tsuzura, A.; Miki, T.; Mochizuki, M.; Miura, O.; Arai, A. CD79B mutations in primary vitreoretinal lymphoma: Diagnostic and prognostic potential. Eur. J. Haematol. 2019, 102, 191–196. [Google Scholar] [CrossRef]
- Arai, A.; Takase, H.; Yoshimori, M.; Yamamoto, K.; Mochizuki, M.; Miura, O. Gene expression profiling of primary vitreoretinal lymphoma. Cancer Sci. 2020, 111, 1417–1421. [Google Scholar] [CrossRef]
- Damato, B.; Bever, G.J.; Kim, D.J.; Afshar, A.R.; Rubenstein, J.L. An audit of retinal lymphoma treatment at the University of California San Francisco. Eye 2020, 34, 515–522. [Google Scholar] [CrossRef]
- Maruyama, K.; Iwahashi, C.; Hashida, N.; Ohguro, N.; Nishida, K. Relationship between vitreoretinal lymphoma and the site of lymphoma development in the central nervous system. Jpn. J. Ophthalmol. 2021, 66, 142–150. [Google Scholar] [CrossRef]
- Wang, Y.; Shen, D.; Wang, V.M.; Sen, H.N.; Chan, C.C. Molecular biomarkers for the diagnosis of primary vitreoretinal lymphoma. Int. J. Mol. Sci. 2011, 12, 5684–5697. [Google Scholar] [CrossRef] [Green Version]
- Chan, C.C.; Rubenstein, J.L.; Coupland, S.E.; Davis, J.L.; Harbour, J.W.; Johnston, P.B.; Cassoux, N.; Touitou, V.; Smith, J.R.; Batchelor, T.T.; et al. Primary vitreoretinal lymphoma: A report from an International Primary Central Nervous System Lymphoma Collaborative Group symposium. Oncologist 2011, 16, 1589–1599. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study | Period (Years) | Study Design | Total Number of Patients with PVRL | CNS Progression for Patients with PVRL (%) | Laterality of PVRL | Time to CNS Progression: Mean (Range); in Months | Follow-Up Period: Median (Range); in Months | Initial Treatment Strategy |
|---|---|---|---|---|---|---|---|---|
| Margolis 1980 [45] | 1968–1974 | R | 6 | 5/6 (83%) | 3 B, 3 U | 34 (14–54) | 11 (5–39) | ORT, BRT, ChT, IT MTX |
| Soussain 1996 [46] | 1992–1995 | P | 5 | 0/5 (0%) | 5 B | n/a | 21 (13–27) | ORT, BRT, ChT, ASCT |
| Ursea 1997 [47] | 1997 | R | 7 | 5/7 (71%) | 4 B, 3 U | Unknown (1–86) | 39 (10–126) | Unknown |
| Isobe 2006 [48] | 1990–2005 | R | 15 | 5/15 (33%) | 13 B, 2 U | Unknown | 19 (7–73) | BRT, ChT |
| Berenbom 2007 [49] | 1995–2003 | R | 7 | 6/7 (86%) | 6 B, 1 U | 16 (Unknown) | 12 (4–58) | BRT, ChT |
| Karma 2007 [50] | 2000–2005 | P | 8 | 5/8 (63%) | 8 B | Unknown | 30 (10–49) | Unknown |
| Stefanovic 2010 [42] | 2005 | P | 6 | 1/6 (17%) | 4 B, 2 U | 21 (n/a) | 44 (10–51) | ORT, ChT |
| Teckie 2014 [51] | 1999–2011 | R | 18 | 7/18 (39%) | 11 B, 7 U | 18 (2–42) | 25 (2–150) | ORT, ChT |
| Hashida 2014 [52] | 2001–2011 | R | 26 | 14/26 (54%) | 17 B, 9 U | 24 (8–65) | 51 (27–81) | ChT, IT MTX, IVM, IVR |
| Takeda 2015 [53] | 2008–2015 | R | 7 | 5/7 (71%) | 6 B, 1 U | 21 (4–48) | Unknown | Unknown |
| Ma 2016 [40] | 2003–2013 | R | 13 | 5/13 (38%) | 7 B, 6 U | Unknown | 40 (4–123) * | ChT, IVM |
| Kaburaki 2017 [54] | 2008–2015 | P | 11 | 1/11 (9%) | 6 B, 5 U | 9 (n/a) | 49 (15–95) * | BRT, ChT, IVM |
| Mahajan 2017 [55] | 2004–2015 | R | 7 | 5/7 (71%) | 7 B | Unknown (4–36) | 13 (6–64) | IVM |
| Carreno 2018 [43] | Unknown | R | 7 | 4/7 (57%) | 4 B, 3 U | 15 (6–27) | 7 (1–27) | Unknown |
| Cho 2018 [39] | 2000–2014 | R | 14 | 11/14 (79%) | 9 B, 5 U | 17 (1–82) | Mean 39 (12–95) | BRT, ORT, ChT, IVM |
| Klimova 2018 [56] | 2004–2016 | R | 10 | 4/10 (40%) | 8 B, 2 U | 34 (25–40) | 53 (14–166) | ChT, IVM, BMT |
| DeLaFuente 2019 [57] | 2005–2018 | R | 12 | 4/12 (33%) | 12 B | Unknown | 68 (17–154) | ORT, ChT, IVM |
| Matsuo 2019 [7] | 2005–2019 | R | 14 | 9/14 (64%) | 8 B, 6 U | 15 (1–60) | 31 (7–132) | BRT, ORT, ChT, ASCT, none |
| Yonese 2019 [58] | 2007–2016 | R | 17 | 11/17 (63%) | 4 B, 13 U | 29 (11–67) | 33 (11–103) | ChT, IVM |
| Castellino 2019 [38] | 1990–2018 | R | 33 | 10/33 (30%) | 28 B, 5 U | Unknown | 36 (Unknown) | BRT, ORT, ChT, ASCT, IVM, IVR |
| Arai 2020 [59] | 2011–2018 | R | 7 | 3/7 (43%) | 3 B, 4 U | 18 (11–24) | 36 (21–67) | ChT, IVM |
| Damato 2020 [60] | 2013–2018 | P | 5 | 2/5 (40%) | 4 B, 1 U | 8 (4 –13) | 44 (30–50) | ChT, sR |
| Maruyama 2021 [61] | 2004–2020 | R | 46 | 20/46 (43%) | 27 B, 19 U | 22 (1–55) | Unknown | BRT, Cht, IT MTX, IVM, IVR, sR, none |
| Zhang 2021 [44] | 2018–2020 | P | 11 | 5/11 (45%) | 7 B, 4 U | 9 (1–25) | 18 (11–28) | ChT, IVM, sR, lenalidomide |
| Lam 2021 [41] | 2011–2018 | R | 59 | 22/59 (37%) | 39 B, 20 U | Unknown | 61 (Unknown) | ORT, ChT, ASCT, IVM, sR |
| Risk of Bias | |||||||
|---|---|---|---|---|---|---|---|
| Study | Study Participation | Study Attrition | Prognostic Factor | Outcome | Study Confounding | Statistical Analysis and Reporting | Overall |
| Margolis [45] | ● | ● | ● | ● | ● | ● | ● |
| Soussain [46] | ● | ● | ● | ● | ● | ● | ● |
| Ursea [47] | ● | ● | ● | ● | ● | ● | ● |
| Isobe [48] | ● | ● | ● | ● | ● | ● | ● |
| Berenbom [49] | ● | ● | ● | ● | ● | ● | ● |
| Karma [50] | ● | ● | ● | ● | ● | ● | ● |
| Stefanovic [42] | ● | ● | ● | ● | ● | ● | ● |
| Teckie [51] | ● | ● | ● | ● | ● | ● | ● |
| Hashida [52] | ● | ● | ● | ● | ● | ● | ● |
| Takeda [53] | ● | ● | ● | ● | ● | ● | ● |
| Ma [40] | ● | ● | ● | ● | ● | ● | ● |
| Kaburaki [54] | ● | ● | ● | ● | ● | ● | ● |
| Mahajan [55] | ● | ● | ● | ● | ● | ● | ● |
| Carreno [43] | ● | ● | ● | ● | ● | ● | ● |
| Cho [39] | ● | ● | ● | ● | ● | ● | ● |
| Klimova [56] | ● | ● | ● | ● | ● | ● | ● |
| DeLaFuente [57] | ● | ● | ● | ● | ● | ● | ● |
| Matsuo [7] | ● | ● | ● | ● | ● | ● | ● |
| Yonese [58] | ● | ● | ● | ● | ● | ● | ● |
| Castellino [38] | ● | ● | ● | ● | ● | ● | ● |
| Arai [59] | ● | ● | ● | ● | ● | ● | ● |
| Damato [60] | ● | ● | ● | ● | ● | ● | ● |
| Maruyama [61] | ● | ● | ● | ● | ● | ● | ● |
| Zhang [44] | ● | ● | ● | ● | ● | ● | ● |
| Lam [41] | ● | ● | ● | ● | ● | ● | ● |
| Study | Bilateral–CNS Progression | Bilateral–No CNS Progression | Unilateral–CNS Progression | Unilateral–No CNS Progression | Relative Risk | 95% CI |
|---|---|---|---|---|---|---|
| Margolis [45] | 3/3 (100%) | 0/3 (0%) | 2/3 (67%) | 1/3 (33%) | 1.40 | [0.60, 3.26] |
| Soussain [46] | 0/5 (0%) | 5/5 (100%) | - | - | - | - |
| Ursea [47] | 3/4 (75%) | 1/4 (25%) | 2/3 (67%) | 1/3 (33%) | 1.13 | [0.42, 3.00] |
| Isobe [48] | 5/13 (38%) | 8/13 (62%) | 0/2 (0%) | 2/2 (100%) | 2.36 | [0.17, 32.14] |
| Berenbom [49] | 5/6 (83%) | 1/6 (17%) | 1/1 (100%) | 0/1 (0%) | 1.05 | [0.43, 2.55] |
| Karma [50] | 5/8 (63%) | 3/8 (38%) | - | - | - | - |
| Stefanovic [42] | 1/4 (25%) | 3/4 (75%) | 0/2 (0%) | 2/2 (100%) | 1.80 | [0.10, 31.52] |
| Teckie [51] | 6/11 (55%) | 5/11 (45%) | 1/7 (14%) | 6/7 (86%) | 3.82 | [0.58, 25.35] |
| Hashida [52] | 10/17 (59%) | 7/17 (41%) | 4/9 (44%) | 5/9 (56%) | 1.32 | [0.58, 3.04] |
| Takeda [53] | 4/6 (67%) | 2/6 (33%) | 1/1 (100%) | 0/1 (0%) | 0.86 | [0.32, 2.27] |
| Ma [40] | 3/7 (43%) | 4/7 (57%) | 2/6 (33%) | 4/6 (67%) | 1.29 | [0.31, 5.31] |
| Kaburaki [54] | 1/6 (17%) | 5/6 (83%) | 0/5 (0%) | 5/5 (100%) | 2.57 | [0.13, 52,12] |
| Mahajan [55] | 5/7 (71%) | 2/7 (29%) | - | - | - | - |
| Carreno [43] | 3/4 (75%) | 1/4 (25%) | 1/3 (33%) | 2/3 (67%) | 2.25 | [0.41, 12.28] |
| Cho [39] | 8/9 (89%) | 1/9 (11%) | 3/5 (60%) | 2/5 (40%) | 1.48 | [0.70, 3.14] |
| Klimova [56] | 4/8 (50%) | 4/8 (50%) | 0/2 (0%) | 2/2 (100%) | 3.00 | [0.22, 40,93] |
| DeLaFuente [57] | 4/12 (33%) | 8/12 (67%) | - | - | - | - |
| Matsuo [7] | 6/8 (75%) | 2/8 (25%) | 3/6 (50%) | 3/6 (50%) | 1.50 | [0.61, 3.67] |
| Yonese [58] | 3/4 (75%) | 1/4 (25%) | 8/13 (62%) | 5/13 (38%) | 1.22 | [0.60, 2.48] |
| Castellino [38] | 9/28 (32%) | 19/28 (68%) | 1/5 (20%) | 4/5 (80%) | 1.61 | [0.26, 10.06] |
| Arai [59] | 2/3 (67%) | 1/3 (33%) | 1/4 (25%) | 3/4 (75%) | 2.67 | [0.41, 17.42] |
| Damato [60] | 2/4 (50%) | 2/4 (50%) | 0/1 (0%) | 1/1 (100%) | 2.00 | [0.16, 25,75] |
| Maruyama [61] | 10/27 (37%) | 17/27 (63%) | 10/19 (53%) | 9/19 (47%) | 0.70 | [0.37, 1.35] |
| Zhang [44] | 2/7 (29%) | 5/7 (71%) | 3/4 (75%) | 1/4 (25%) | 0.38 | [0.10, 1.40] |
| Lam [41] | 13/39 (33%) | 26/39 (67%) | 9/20 (45%) | 11/20 (55%) | 0.74 | [0.38, 1,43] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Rooij, J.L.M.; Tokarska, K.A.; ten Dam-van Loon, N.H.; Wessels, P.H.; Seute, T.; Minnema, M.C.; Snijders, T.J. Central Nervous System Progression in Primary Vitreoretinal Lymphoma with Bilateral and Unilateral Involvement: A Systematic Review and Meta-Analysis. Cancers 2022, 14, 2967. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14122967
van Rooij JLM, Tokarska KA, ten Dam-van Loon NH, Wessels PH, Seute T, Minnema MC, Snijders TJ. Central Nervous System Progression in Primary Vitreoretinal Lymphoma with Bilateral and Unilateral Involvement: A Systematic Review and Meta-Analysis. Cancers. 2022; 14(12):2967. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14122967
Chicago/Turabian Stylevan Rooij, Josephus L. M., Klaudia A. Tokarska, Ninette H. ten Dam-van Loon, Peter H. Wessels, Tatjana Seute, Monique C. Minnema, and Tom J. Snijders. 2022. "Central Nervous System Progression in Primary Vitreoretinal Lymphoma with Bilateral and Unilateral Involvement: A Systematic Review and Meta-Analysis" Cancers 14, no. 12: 2967. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14122967