
Time Trend and Association of Early-Onset Colorectal Cancer with Diverticular Disease in the United States: 2010–2021

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Database Description
2.2. Study Population
2.3. Statistical Analysis
3. Results
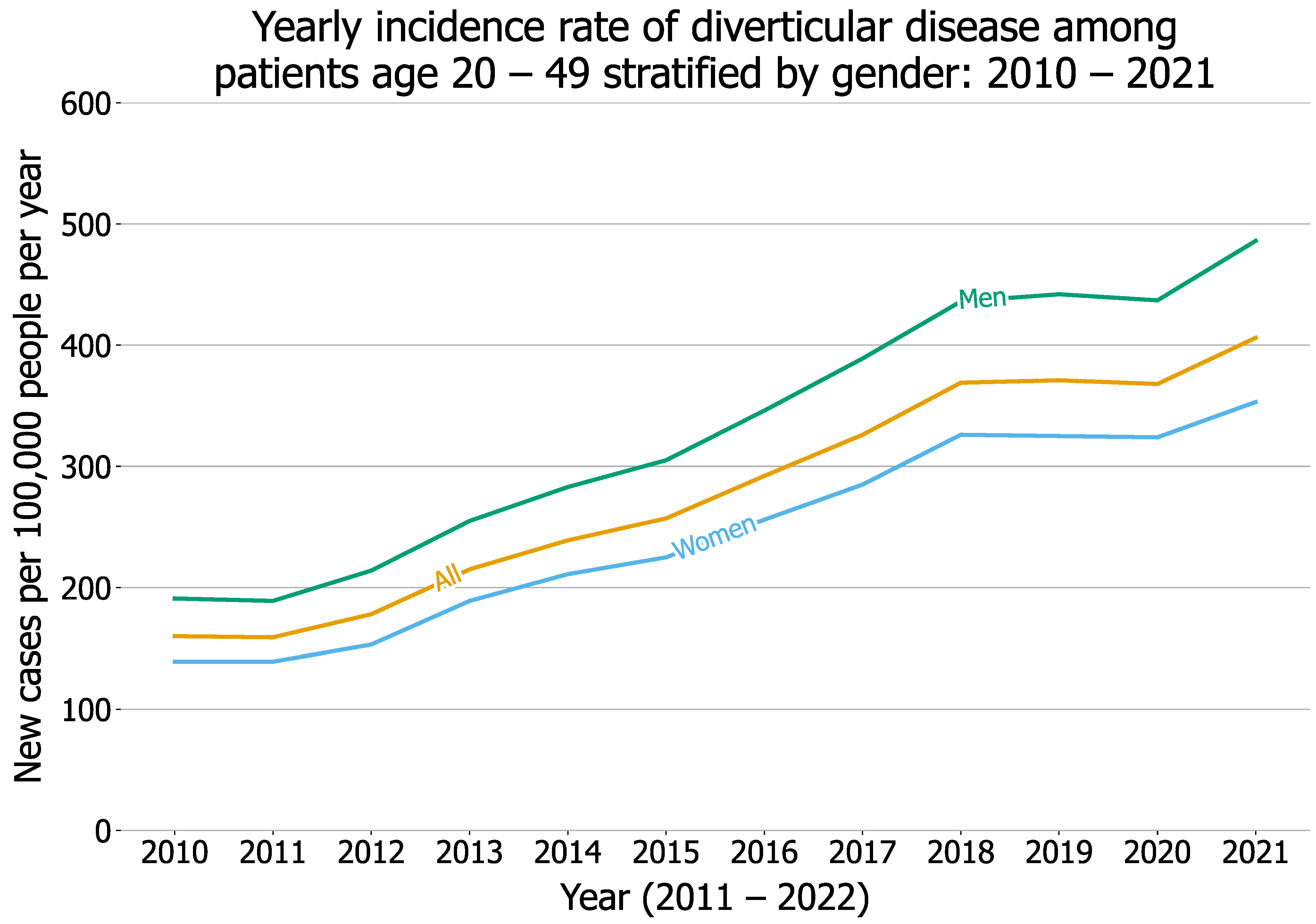
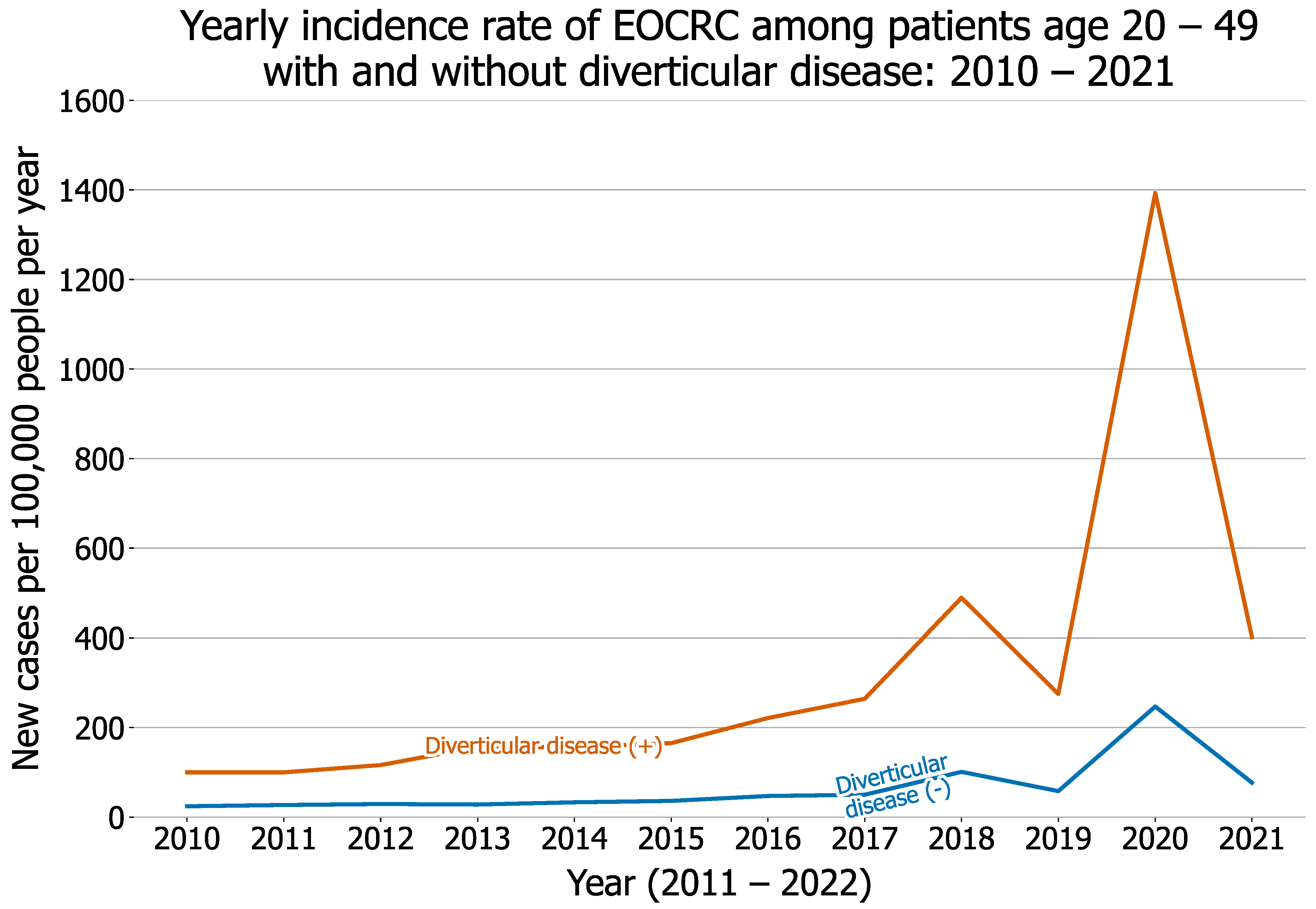
3.1. Yearly Incidence Rate of Diverticular Disease and EOCRC among Young Adults from 2010 through 2021
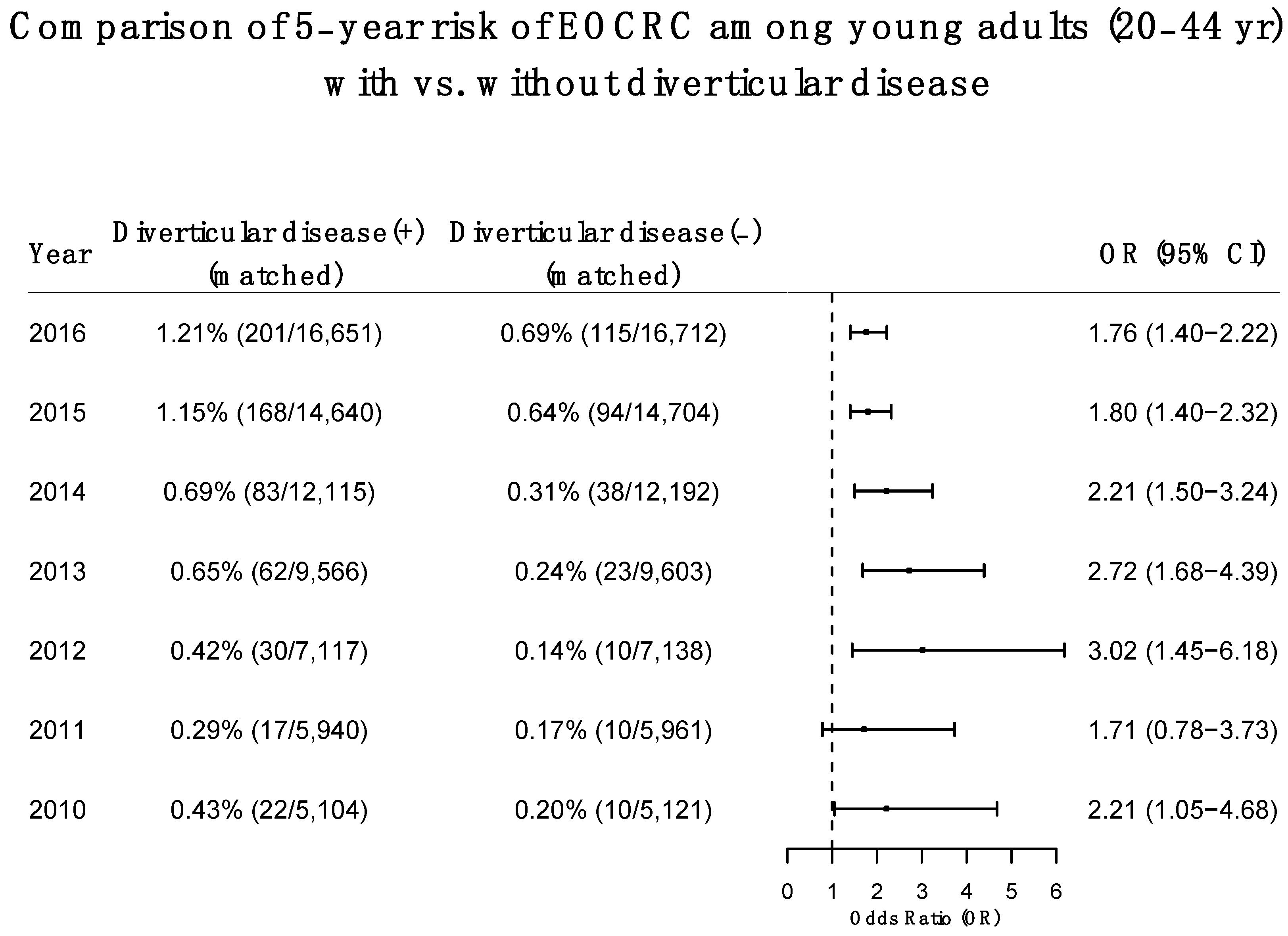
3.2. Increased Risk of EOCRC among Patients with Pre-Existing Diverticular Disease Compared to Propensity-Score-Matched Patients without Diverticular Disease
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Jemal, A.; Ward, E.M. Increase in Incidence of Colorectal Cancer among Young Men and Women in the United States. Cancer Epidemiol. Biom. Prev. 2009, 18, 1695–1698. [Google Scholar] [CrossRef] [Green Version]
- Akimoto, N.; Ugai, T.; Zhong, R.; Hamada, T.; Fujiyoshi, K.; Giannakis, M.; Wu, K.; Cao, Y.; Ng, K.; Ogino, S. Rising incidence of early-onset colorectal cancer—A call to action. Nat. Rev. Clin. Oncol. 2020, 18, 230–243. [Google Scholar] [CrossRef] [PubMed]
- Hofseth, L.J.; Hebert, J.R.; Chanda, A.; Chen, H.; Love, B.L.; Pena, M.M.; Murphy, E.A.; Sajish, M.; Sheth, A.; Buckhaults, P.J.; et al. Early-onset colorectal cancer: Initial clues and current views. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 352–364. [Google Scholar] [CrossRef] [PubMed]
- Bailey, C.E.; Hu, C.-Y.; You, Y.N.; Bednarski, B.K.; Rodriguez-Bigas, M.A.; Skibber, J.M.; Cantor, S.B.; Chang, G.J. Increasing Disparities in the Age-Related Incidences of Colon and Rectal Cancers in the United States, 1975–2010. JAMA Surg. 2015, 150, 17–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feuerstein, J.D.; Falchuk, K.R. Diverticulosis and Diverticulitis. Mayo Clin. Proc. 2016, 91, 1094–1104. [Google Scholar] [CrossRef] [PubMed]
- Violi, A.; Cambiè, G.; Miraglia, C.; Barchi, A.; Nouvenne, A.; Capasso, M.; Leandro, G.; Meschi, T.; De’ Angelis, G.L.; Di Mario, F. Epidemiology and risk factors for diverticular disease. Acta Bio-Med. Atenei Parm. 2018, 89 (Suppl. 9), 107–112. [Google Scholar] [CrossRef]
- Painter, N.S.; Burkitt, D.P. Diverticular disease of the colon: A deficiency disease of Western civilization. BMJ 1971, 2, 450–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- TriNetX. TriNetX. Available online: https://trinetx.com/ (accessed on 4 August 2022).
- Wang, L.; Wang, Q.; Davis, P.B.; Volkow, N.D.; Xu, R. Increased risk for COVID-19 breakthrough infection in fully vaccinated patients with substance use disorders in the United States between December 2020 and August 2021. World Psychiatr. 2021, 21, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Berger, N.A.; Kaelber, D.C.; Davis, P.B.; Volkow, N.D.; Xu, R. Incidence Rates and Clinical Outcomes of SARS-CoV-2 Infection with the Omicron and Delta Variants in Children Younger than 5 Years in the US. JAMA Pediatr. 2022, 176, 811. [Google Scholar] [CrossRef]
- Wang, L.; Davis, P.B.; Kaelber, D.C.; Volkow, N.D.; Xu, R. Comparison of mRNA-1273 and BNT162b2 Vaccines on Breakthrough SARS-CoV-2 Infections, Hospitalizations, and Death during the Delta-Predominant Period. JAMA 2022, 327, 678. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Davis, P.B.; Kaelber, D.C.; Xu, R. COVID-19 breakthrough infections and hospitalizations among vaccinated patients with dementia in the United States between December 2020 and August 2021. Alzheimer Dement. 2022. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Kaelber, D.C.; Xu, R.; Berger, N.A. Breakthrough SARS-CoV-2 Infections, Hospitalizations, and Mortality in Vaccinated Patients with Cancer in the US between December 2020 and November 2021. JAMA Oncol. 2022, 8, 1027. [Google Scholar] [CrossRef]
- Wang, L.; Kaelber, D.C.; Xu, R.; Berger, N.A. COVID-19 breakthrough infections, hospitalizations and mortality in fully vaccinated patients with hematologic malignancies: A clarion call for maintaining mitigation and ramping-up research. Blood Rev. 2022, 54, 100931. [Google Scholar] [CrossRef]
- Wang, L.; Berger, N.A.; Xu, R. Risks of SARS-CoV-2 Breakthrough Infection and Hospitalization in Fully Vaccinated Patients with Multiple Myeloma. JAMA Netw. Open. 2021, 4, e2137575. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Davis, P.B.; Volkow, N.D.; Berger, N.A.; Kaelber, D.C.; Xu, R. Association of COVID-19 with New-Onset Alzheimer’s Disease. J. Alzheimer Dis. 2022, 1, 220717. [Google Scholar] [CrossRef]
- Pan, Y.; Davis, P.B.; Kaebler, D.C.; Blankfield, R.P.; Xu, R. Cardiovascular risk of gabapentin and pregabalin in patients with diabetic neuropathy. Cardiovasc. Diabetol. 2022, 21, 9. [Google Scholar] [CrossRef] [PubMed]
- Austin, P.C. A critical appraisal of propensity-score matching in the medical literature between 1996 and 2003. Stat. Med. 2007, 27, 2037–2049. [Google Scholar] [CrossRef] [PubMed]
- Kuss, O.; Blettner, M.; Börgermann, J. Propensity Score: An Alternative Method of Analyzing Treatment Effects. Dtsch. Ärzteblatt Int. 2016, 113, 597–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.H.; Duster, M.; Roberts, T.; Devinsky, O. United States Dietary Trends Since 1800: Lack of Association Between Saturated Fatty Acid Consumption and Non-communicable Diseases. Front. Nutr. 2022, 8. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention (CDC). Adult Obesity Facts. Centers for Disease Control and Prevention. Published May 19, 2022. Available online: https://www.cdc.gov/obesity/data/adult.html (accessed on 22 July 2022).
- Zhou, Y.; Boudreau, D.M.; Freedman, A.N. Trends in the use of aspirin and nonsteroidal anti-inflammatory drugs in the general U.S. population. Pharmacoepidemiol. Drug Saf. 2013, 23, 43–50. [Google Scholar] [CrossRef] [PubMed]
- National Institute on Alcohol Abuse and Alcoholism (NIAAA). Alcohol Facts and Statistics. Available online: https://www.niaaa.nih.gov/publications/brochures-and-fact-sheets/alcohol-facts-and-statistics (accessed on 22 July 2022).
- CDC Current Cigarette Smoking among Adults in the United States; CDC: Atlanta, GA, USA, 2020. Available online: https://www.cdc.gov/tobacco/data_statistics/fact_sheets/adult_data/cig_smoking/index.htm (accessed on 2 May 2020).
- Peery, A.F.; Keku, T.O.; Galanko, J.A.; Sandler, R.S. Sex and Race Disparities in Diverticulosis Prevalence. Clin. Gastroenterol. Hepatol. 2019, 18, 1980–1986. [Google Scholar] [CrossRef]
- Shah, R.R.; Millien, V.O.; da Costa, W.L., Jr.; Oluyomi, A.O.; Gould Suarez, M.; Thrift, A.P. Trends in the incidence of early-onset colorectal cancer in all 50 United States from 2001 through 2017. Cancer 2022, 128, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Mauri, G.; Sartore-Bianchi, A.; Russo, A.G.; Marsoni, S.; Bardelli, A.; Siena, S. Early-onset colorectal cancer in young individuals. Mol. Oncol. 2018, 13, 109–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Cancer Society. Colorectal Cancer Screening Guidelines. Available online: https://www.cancer.org/health-care-professionals/american-cancer-society-prevention-early-detection-guidelines/colorectal-cancer-screening-guidelines.html (accessed on 25 September 2022).
- Patt, D.; Gordan, L.; Diaz, M.; Okon, T.; Grady, L.; Harmison, M.; Markward, N.; Sullivan, M.; Peng, J.; Zhou, A. Impact of COVID-19 on Cancer Care: How the Pandemic Is Delaying Cancer Diagnosis and Treatment for American Seniors. JCO Clin. Cancer Inform. 2020, 4, 1059–1071. [Google Scholar] [CrossRef]
- Wang, Q.; Berger, N.A.; Xu, R. Analyses of Risk, Racial Disparity, and Outcomes among US Patients with Cancer and COVID-19 Infection. JAMA Oncol. 2021, 7, 220. [Google Scholar] [CrossRef]
- Wang, Q.; Berger, N.A.; Xu, R. When hematologic malignancies meet COVID-19 in the United States: Infections, death and disparities. Blood Rev. 2021, 47, 100775. [Google Scholar] [CrossRef]
- Stefánsson, T.; Ekbom, A.; Sparèn, P.; Påhlman, L. Association between sigmoid diverticulitis and left-sided colon cancer: A nested, population-based, case control study. Scand. J. Gastroenterol. 2004, 39, 743–747. [Google Scholar] [CrossRef]
- Stefansson, T.; Ekbom, A.; Sparen, P.; Pahlman, L. Increased risk of left sided colon cancer in patients with diverticular disease. Gut 1993, 34, 499–502. [Google Scholar] [CrossRef] [Green Version]
- Granlund, J.; Svensson, T.; Granath, F.; Hjern, F.; Ekbom, A.; Blomqvist, P.; Schmidt, P.T. Diverticular disease and the risk of colon cancer—A population-based case-control study. Aliment. Pharmacol. Ther. 2011, 34, 675–681. [Google Scholar] [CrossRef]
- Alvarez, M.D.; Quintana, I.; Terradas, M.; Mur, P.; Balaguer, F.; Valle, L. The Inherited and Familial Component of Early-Onset Colorectal Cancer. Cells 2021, 10, 710. [Google Scholar] [CrossRef] [PubMed]
- Tursi, A.; Elisei, W. Role of Inflammation in the Pathogenesis of Diverticular Disease. Mediat. Inflamm. 2019, 2019, 7. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Before Matching | After Matching | |||||
|---|---|---|---|---|---|---|
| Diverticular Disease (+) Cohort (Year 2016) | Diverticular Disease (−) Cohort (Year 2016) | SMD | Diverticular Disease (+) Cohort (Year 2016) | Diverticular Disease (−) Cohort (Year 2016) | SMD | |
| Total number | 16,782 | 2,991,298 | 16,782 | 16,782 | ||
| Age at index event (years, mean ± SD) | 37.3 ± 5.7 | 32.4 ± 7.1 | 0.76 * | 37.3 ± 5.7 | 37.2 ± 5.7 | 0.003 |
| Sex (%) | ||||||
| Female | 48.3 | 65.5 | 0.35 * | 48.3 | 48.0 | 0.005 |
| Male | 51.7 | 34.5 | 0.35 * | 51.7 | 52.0 | 0.005 |
| Ethnicity (%) | ||||||
| Hispanic/Latinx | 16.9 | 9.3 | 0.23 * | 16.9 | 17.0 | 0.002 |
| Not Hispanic/Latinx | 61.8 | 49.8 | 0.24 * | 61.8 | 61.8 | 0.001 |
| Unknown | 21.3 | 40.9 | 0.43 * | 21.3 | 21.2 | 0.003 |
| Race (%) | ||||||
| Asian | 1.0 | 2.3 | 0.09 | 1.0 | 1.1 | 0.003 |
| Black | 14.4 | 13.5 | 0.03 | 14.4 | 14.2 | 0.005 |
| White | 69.2 | 52.3 | 0.35 * | 69.2 | 70.0 | 0.02 |
| Unknown | 14.4 | 31.4 | 0.41 * | 14.4 | 13.8 | 0.02 |
| Adverse socioeconomic determinants of health and life styles (%) | ||||||
| Health hazards related to socioeconomic and psychosocial circumstances | 3.1 | 2.1 | 0.06 | 3.1 | 2.8 | 0.02 |
| Problems related to lifestyle | 4.7 | 2.3 | 0.13 * | 4.7 | 4.2 | 0.03 |
| Dietary counseling and surveillance | 1.4 | 0.8 | 0.06 | 1.4 | 1.2 | 0.02 |
| Lack of physical exercise | 0.1 | 0.03 | 0.02 | 0.1 | 0.1 | <0.001 |
| Alcohol drinking | 4.5 | 1.9 | 0.15 * | 4.5 | 3.9 | 0.03 |
| Tobacco smoking | 14.8 | 6.5 | 0.27 * | 14.8 | 14.7 | 0.003 |
| Pre-existing medical conditions (%) | ||||||
| Overweight and obesity | 19.6 | 8.4 | 0.33 * | 19.6 | 19.3 | 0.009 |
| Personal history of malignant neoplasm of digestive organs | 0.4 | 0.1 | 0.08 | 0.4 | 0.4 | 0.008 |
| Medications (%) | ||||||
| NSAIDs | 23.4 | 16.4 | 0.17 * | 23.4 | 23.0 | 0.008 |
| Aspirin | 8.9 | 3.7 | 0.22 * | 8.9 | 8.1 | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, L.; Xu, R.; Kaelber, D.C.; Berger, N.A. Time Trend and Association of Early-Onset Colorectal Cancer with Diverticular Disease in the United States: 2010–2021. Cancers 2022, 14, 4948. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14194948
Wang L, Xu R, Kaelber DC, Berger NA. Time Trend and Association of Early-Onset Colorectal Cancer with Diverticular Disease in the United States: 2010–2021. Cancers. 2022; 14(19):4948. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14194948
Chicago/Turabian StyleWang, Lindsey, Rong Xu, David C. Kaelber, and Nathan A. Berger. 2022. "Time Trend and Association of Early-Onset Colorectal Cancer with Diverticular Disease in the United States: 2010–2021" Cancers 14, no. 19: 4948. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14194948