

Comparison of Surgical Resection and Percutaneous Ultrasonographic Guided Radiofrequency Ablation for Initial Recurrence of Hepatocellular Carcinoma in Early Stage following Curative Treatment
 , , , , add
Show full author list
, , , , add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Statistical Analysis
4. Results
4.1. Patient Characteristics
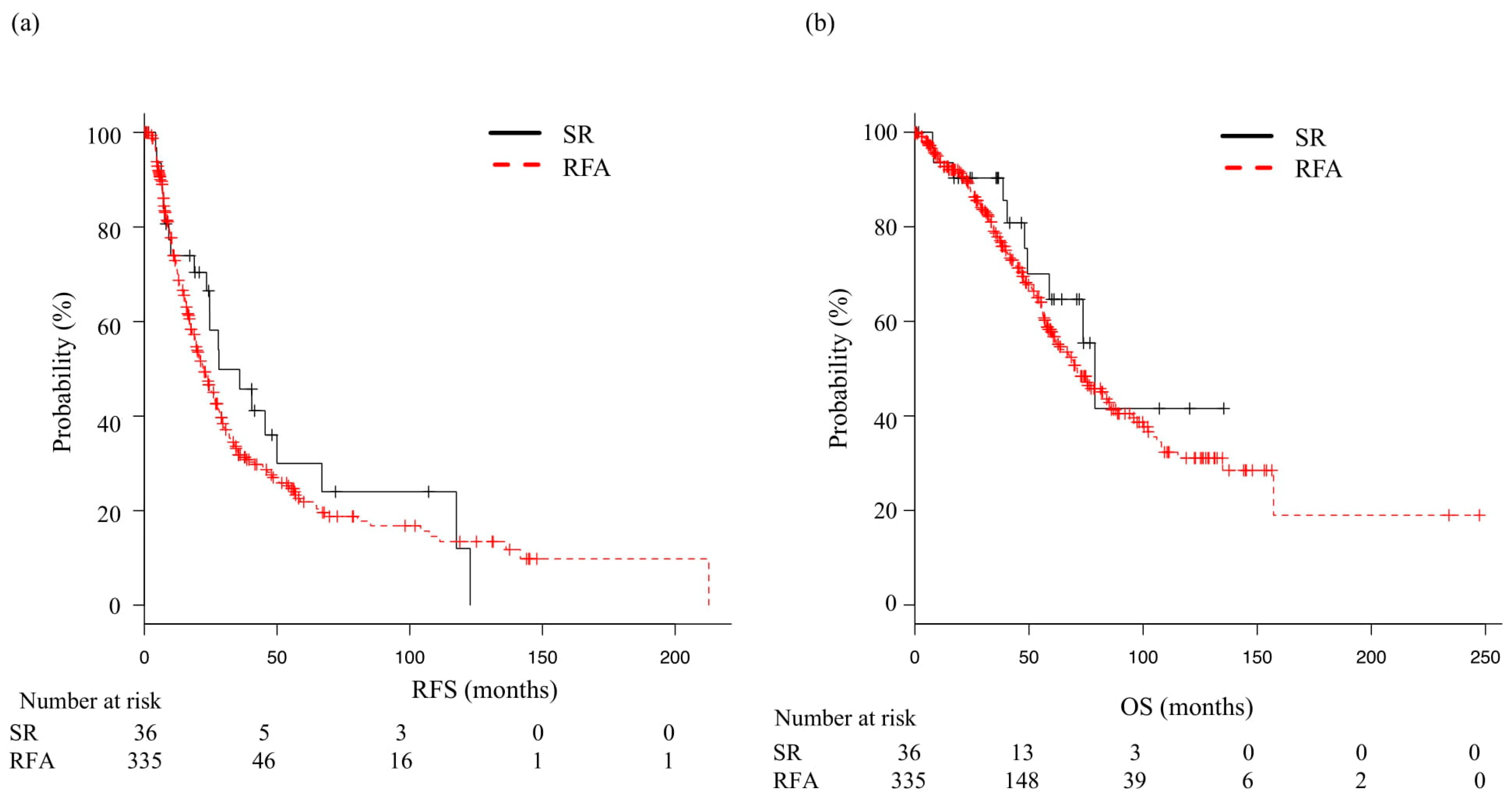
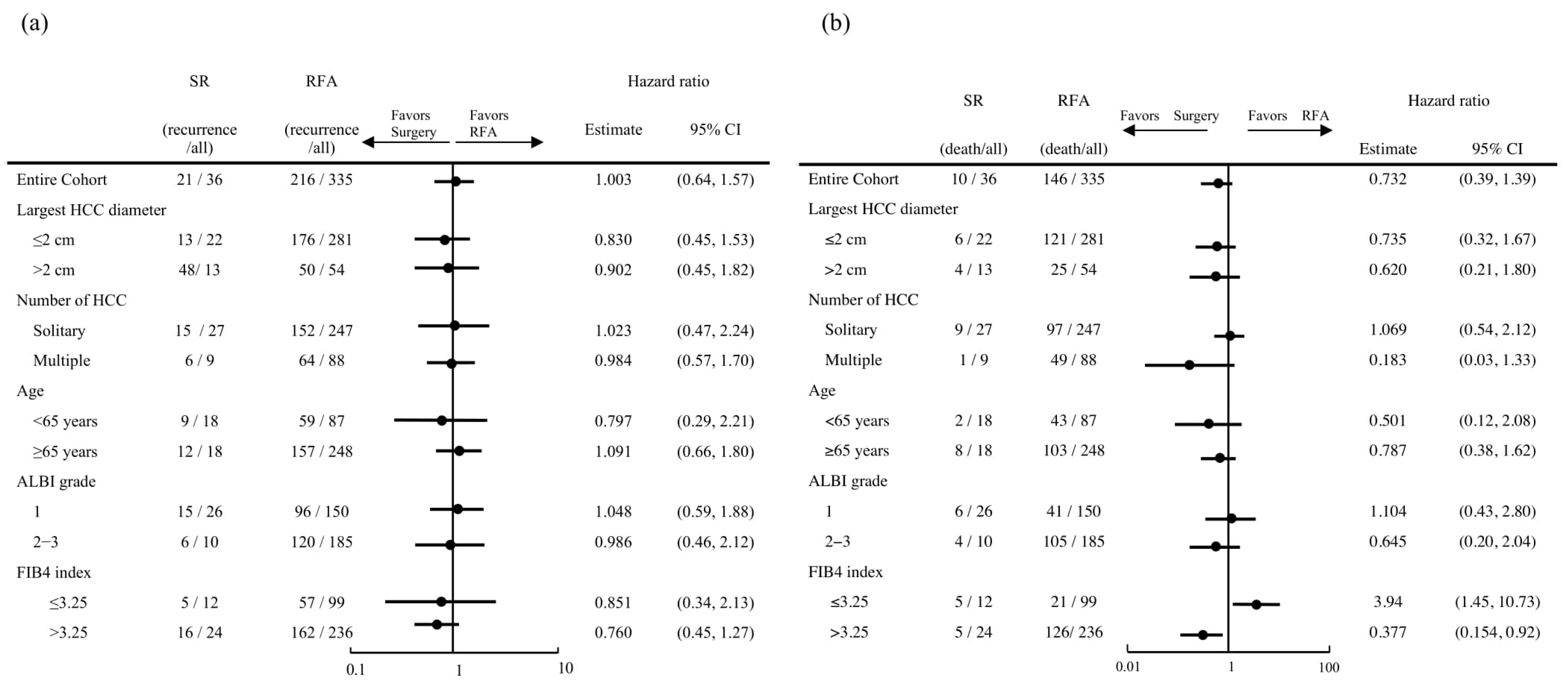
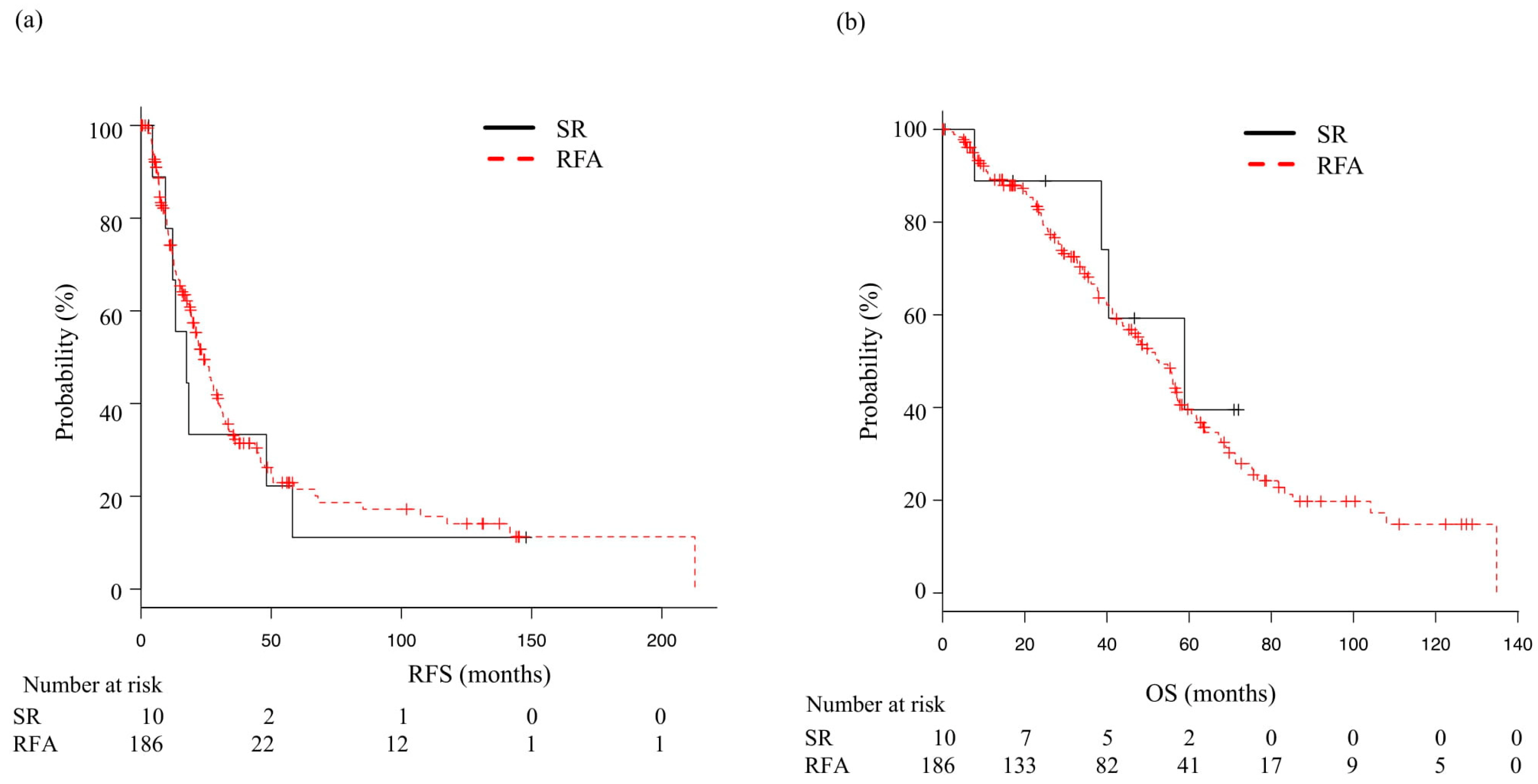
4.2. RFS and OS
4.3. Adverse Events
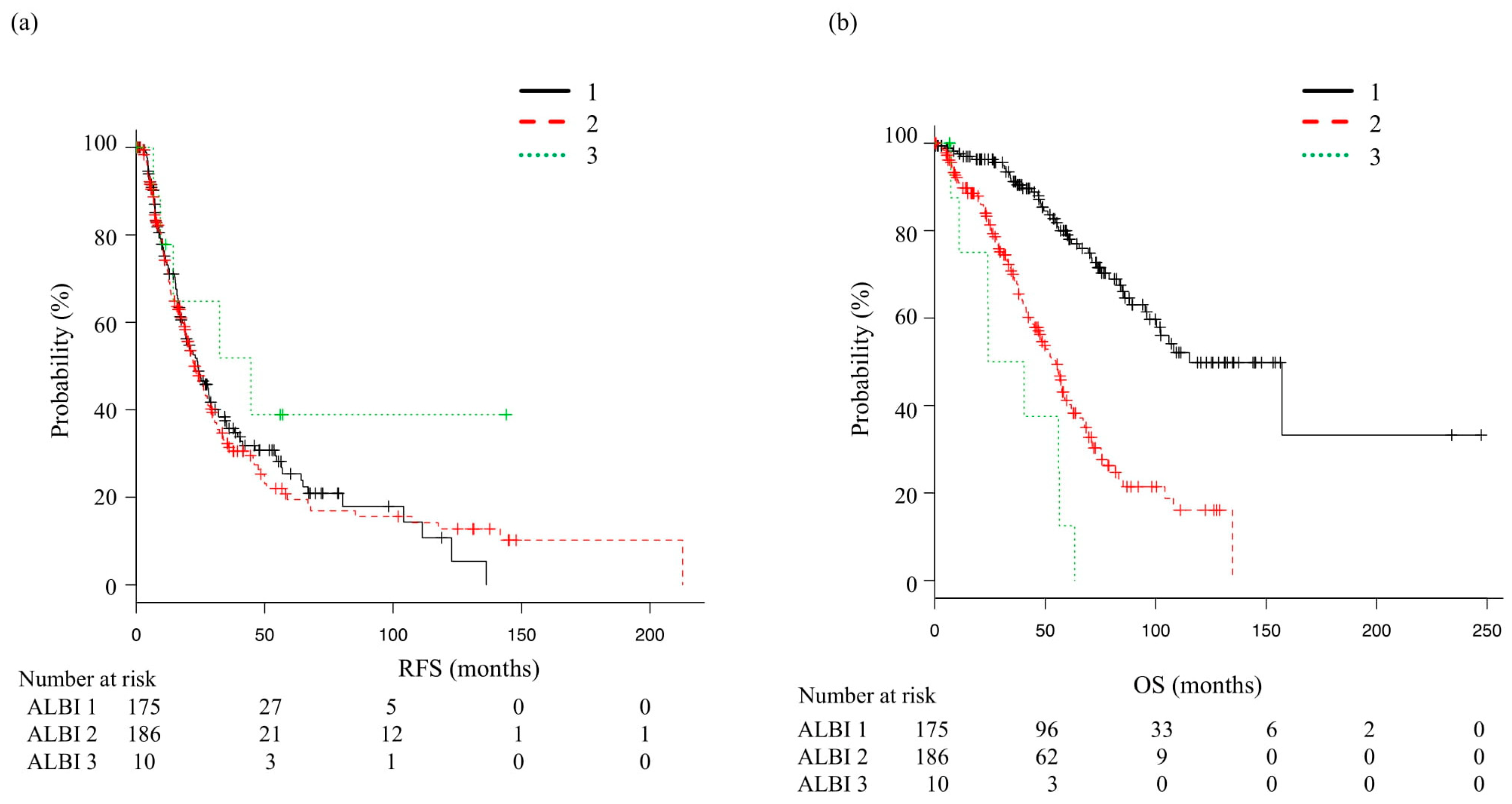
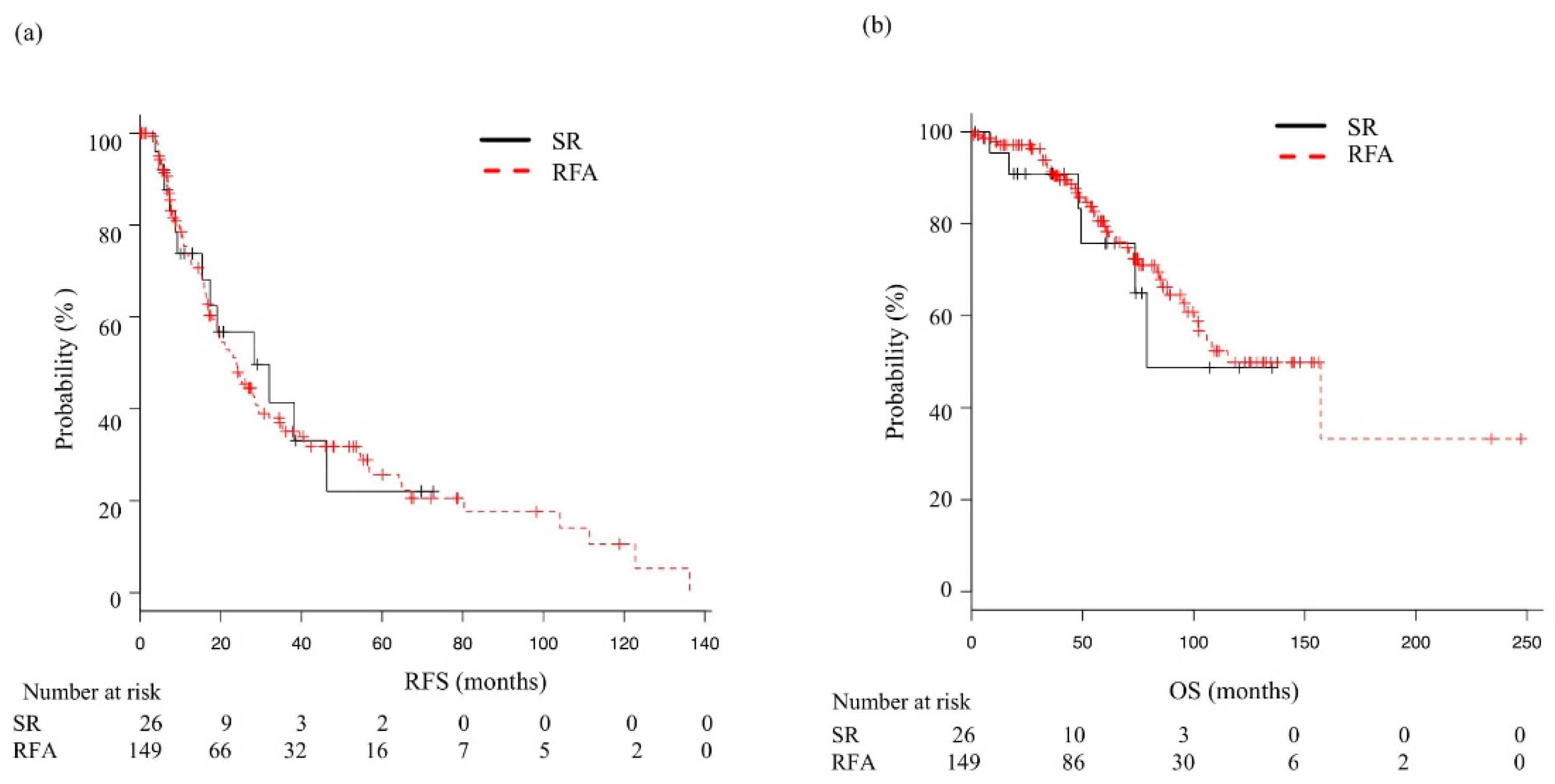
4.4. Sub-Analysis, RFS, and OS for each ALBI Grade
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Taura, K.; Ikai, I.; Hatano, E.; Fujii, H.; Uyama, N.; Shimahara, Y. Implication of frequent local ablation therapy for intrahepatic recurrence in prolonged survival of patients with hepatocellular carcinoma undergoing hepatic resection: An analysis of 610 patients over 16 years old. Ann. Surg. 2006, 244, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Portolani, N.; Coniglio, A.; Ghidoni, S.; Giovanelli, M.; Benetti, A.; Tiberio, G.A.; Giulini, S.M. Early and late recurrence after liver resection for hepatocellular carcinoma: Prognostic and therapeutic implications. Ann. Surg. 2006, 243, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Kokudo, N.; Takemura, N.; Hasegawa, K.; Takayama, T.; Kubo, S.; Shimada, M.; Nagano, H.; Hatano, E.; Izumi, N.; Kaneko, S.; et al. Clinical practice guidelines for hepatocellular carcinoma: The Japan Society of Hepatology 2017 (4th JSH-HCC guidelines) 2019 update. Hepatol. Res. 2019, 49, 1109–1113. [Google Scholar] [CrossRef]
- Takayama, T.; Hasegawa, K.; Izumi, N.; Kudo, M.; Shimada, M.; Yamanaka, N.; Inomata, M.; Kaneko, S.; Nakayama, H.; Kawaguchi, Y.; et al. Surgery Versus Radiofrequency Ablation for Small Hepatocellular Carcinoma: A Randomized Controlled Trial (SURF-Trial). Liver Cancer 2021, 11, 209–218. [Google Scholar] [CrossRef]
- Fan, S.T.; Poon, R.T.; Yeung, C.; Lam, C.M.; Lo, C.M.; Yuen, W.K.; Ng, K.K.; Liu, C.L.; Chan, S.C. Outcome after partial hepatectomy for hepatocellular cancer within the Milan criteria. Br. J. Surg. 2011, 98, 1292–1300. [Google Scholar] [CrossRef]
- Bruix, J.; Sherman, M.; American Association for the Study of Liver, D. Management of hepatocellular carcinoma: An update. Hepatology 2011, 53, 1020–1022. [Google Scholar] [CrossRef] [Green Version]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [Green Version]
- Kudo, M.; Kitano, M.; Sakurai, T.; Nishida, N. General Rules for the Clinical and Pathological Study of Primary Liver Cancer, Nationwide Follow-Up Survey and Clinical Practice Guidelines: The Outstanding Achievements of the Liver Cancer Study Group of Japan. Dig. Dis. 2015, 33, 765–770. [Google Scholar] [CrossRef]
- Pugh, R.N.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the oesophagus for bleeding oesophageal varices. Br. J. Surg. 1973, 60, 646–649. [Google Scholar] [CrossRef]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, A.; Kumada, T.; Michitaka, K.; Toyoda, H.; Tada, T.; Ueki, H.; Kaneto, M.; Aibiki, T.; Okudaira, T.; Kawakami, T.; et al. Usefulness of albumin-bilirubin grade for evaluation of prognosis of 2584 Japanese patients with hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2016, 31, 1031–1036. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, A.; Michitaka, K.; Kumada, T.; Izumi, N.; Kadoya, M.; Kokudo, N.; Kubo, S.; Matsuyama, Y.; Nakashima, O.; Sakamoto, M.; et al. Validation and Potential of Albumin-Bilirubin Grade and Prognostication in a Nationwide Survey of 46,681 Hepatocellular Carcinoma Patients in Japan: The Need for a More Detailed Evaluation of Hepatic Function. Liver Cancer 2017, 6, 325–336. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef] [Green Version]
- Zhu, F.; Chang, Q.; Duan, S.; Leng, W. Efficacy and safety of radiofrequency ablation versus laparoscopic hepatectomy for small hepatocellular carcinoma: A protocol for a randomized controlled trial. Medicine 2021, 100, e23678. [Google Scholar] [CrossRef]
- Kaibori, M.; Hiraoka, A.; Matsui, K.; Matsushima, H.; Kosaka, H.; Yamamoto, H.; Yamaguchi, T.; Yoshida, K.; Sekimoto, M. Predicting Complications following Surgical Resection of Hepatocellular Carcinoma Using Newly Developed Neo-Glasgow Prognostic Score with ALBI Grade: Comparison of Open and Laparoscopic Surgery Cases. Cancers 2022, 14, 1402. [Google Scholar] [CrossRef]
- Cai, W.; Liu, Z.; Xiao, Y.; Zhang, W.; Tang, D.; Cheng, B.; Li, Q. Comparison of clinical outcomes of laparoscopic versus open surgery for recurrent hepatocellular carcinoma: A meta-analysis. Surg. Endosc. 2019, 33, 3550–3557. [Google Scholar] [CrossRef]
- Hirooka, M.; Iuchi, H.; Kumagi, T.; Shigematsu, S.; Hiraoka, A.; Uehara, T.; Kurose, K.; Horiike, N.; Onji, M. Virtual sonographic radiofrequency ablation of hepatocellular carcinoma visualized on CT but not on conventional sonography. AJR Am. J. Roentgenol. 2006, 186, S255–S260. [Google Scholar] [CrossRef]
- Hiraoka, A.; Ichiryu, M.; Tazuya, N.; Ochi, H.; Tanabe, A.; Nakahara, H.; Hidaka, S.; Uehara, T.; Ichikawa, S.; Hasebe, A.; et al. Clinical translation in the treatment of hepatocellular carcinoma following the introduction of contrast-enhanced ultrasonography with Sonazoid. Oncol. Lett. 2010, 1, 57–61. [Google Scholar] [CrossRef] [Green Version]
- Minami, Y.; Kudo, M. Image Guidance in Ablation for Hepatocellular Carcinoma: Contrast-Enhanced Ultrasound and Fusion Imaging. Front. Oncol. 2021, 11, 593636. [Google Scholar] [CrossRef]
- Uehara, T.; Hirooka, M.; Ishida, K.; Hiraoka, A.; Kumagi, T.; Kisaka, Y.; Hiasa, Y.; Onji, M. Percutaneous ultrasound-guided radiofrequency ablation of hepatocellular carcinoma with artificially induced pleural effusion and ascites. J. Gastroenterol. 2007, 42, 306–311. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Liu, G.; Li, J.; Yan, Z.; Xia, Y.; Wan, X.; Ji, Y.; Lau, W.Y.; Wu, M.; Shen, F. Early intrahepatic recurrence of hepatocellular carcinoma after hepatectomy treated with re-hepatectomy, ablation or chemoembolization: A prospective cohort study. Eur. J. Surg. Oncol. 2015, 41, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.C.; Poon, R.T.; Cheung, T.T.; Chok, K.S.; Chan, S.C.; Fan, S.T.; Lo, C.M. Survival analysis of re-resection versus radiofrequency ablation for intrahepatic recurrence after hepatectomy for hepatocellular carcinoma. World J. Surg. 2012, 36, 151–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, S.; Peng, Z.; Xiao, H.; Lin, M.; Chen, Z.; Jiang, C.; Hu, W.; Xie, X.; Liu, L.; Peng, B.; et al. Combined radiofrequency ablation and ethanol injection versus repeat hepatectomy for elderly patients with recurrent hepatocellular carcinoma after initial hepatic surgery. Int. J. Hyperth. 2018, 34, 1029–1037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, K.D.; Lim, H.K.; Rhim, H.; Lee, M.W.; Kim, Y.S.; Lee, W.J.; Paik, Y.H.; Gwak, G.Y.; Kim, J.M.; Kwon, C.H.; et al. Repeated Hepatic Resection versus Radiofrequency Ablation for Recurrent Hepatocellular Carcinoma after Hepatic Resection: A Propensity Score Matching Study. Radiology 2015, 275, 599–608. [Google Scholar] [CrossRef]
- Eisele, R.M.; Chopra, S.S.; Lock, J.F.; Glanemann, M. Treatment of recurrent hepatocellular carcinoma confined to the liver with repeated resection and radiofrequency ablation: A single center experience. Technol. Health Care 2013, 21, 9–18. [Google Scholar] [CrossRef]
- Umeda, Y.; Matsuda, H.; Sadamori, H.; Matsukawa, H.; Yagi, T.; Fujiwara, T. A prognostic model and treatment strategy for intrahepatic recurrence of hepatocellular carcinoma after curative resection. World J. Surg. 2011, 35, 170–177. [Google Scholar] [CrossRef]
- Xia, Y.; Li, J.; Liu, G.; Wang, K.; Qian, G.; Lu, Z.; Yang, T.; Yan, Z.; Lei, Z.; Si, A.; et al. Long-term Effects of Repeat Hepatectomy vs Percutaneous Radiofrequency Ablation Among Patients With Recurrent Hepatocellular Carcinoma: A Randomized Clinical Trial. JAMA Oncol. 2020, 6, 255–263. [Google Scholar] [CrossRef]
- Shiina, S.; Sato, K.; Tateishi, R.; Shimizu, M.; Ohama, H.; Hatanaka, T.; Takawa, M.; Nagamatsu, H.; Imai, Y. Percutaneous Ablation for Hepatocellular Carcinoma: Comparison of Various Ablation Techniques and Surgery. Can. J. Gastroenterol. Hepatol. 2018, 2018, 4756147. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Z.; Lei, J.; Li, B.; Yan, L.; Wang, W.; Wei, Y.; Cheng, K. Liver resection and radiofrequency ablation of very early hepatocellular carcinoma cases (single nodule <2 cm): A single-center study. Eur. J. Gastroenterol. Hepatol. 2014, 26, 339–344. [Google Scholar] [CrossRef]
- Starlinger, P.; Ubl, D.S.; Hackl, H.; Starlinger, J.; Nagorney, D.M.; Smoot, R.L.; Habermann, E.B.; Cleary, S.P. Combined APRI/ALBI score to predict mortality after hepatic resection. BJS Open 2021, 5, zraa043. [Google Scholar] [CrossRef] [PubMed]
- Tamaki, N.; Kurosaki, M.; Yasui, Y.; Mori, N.; Tsuji, K.; Hasebe, C.; Joko, K.; Akahane, T.; Furuta, K.; Kobashi, H.; et al. Change in Fibrosis 4 Index as Predictor of High Risk of Incident Hepatocellular Carcinoma After Eradication of Hepatitis C Virus. Clin. Infect. Dis. 2021, 73, e3349–e3354. [Google Scholar] [CrossRef] [PubMed]
- Kanda, T.; Goto, T.; Hirotsu, Y.; Moriyama, M.; Omata, M. Molecular Mechanisms Driving Progression of Liver Cirrhosis towards Hepatocellular Carcinoma in Chronic Hepatitis B and C Infections: A Review. Int. J. Mol. Sci. 2019, 20, 1358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasaki-Tanaka, R.; Ray, R.; Moriyama, M.; Ray, R.B.; Kanda, T. Molecular Changes in Relation to Alcohol Consumption and Hepatocellular Carcinoma. Int. J. Mol. Sci. 2022, 23, 9679. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SR Group (n = 36) | RFA Group (n = 335) | p-Value | |
|---|---|---|---|
| Age, years * | 71 (65–74) | 72 (64–78) | 0.29 |
| Gender, males:females | 26:10 | 243:92 | 0.97 |
| Etiology, HBV:HCV (SVR):alcohol:others | 4:25 (8):3:4 | 32:226 (32):24:53 | 0.87 |
| ECOG PS, 0:1:2:3 | 36:0:0:0 | 322:11:1:1 | 0.321 |
| AST, U/L * | 28 (23–40) | 42 (29–62) | <0.01 |
| ALT, U/L * | 21 (16–38) | 32 (21–54) | 0.03 |
| Platelets, 104/µL * | 12.3 (9.2–15.1) | 11.3 (7.9–15.6) | 0.39 |
| Total-bilirubin, mg/dL * | 0.8 (0.6–1.0) | 0.7 (0.5–1.0) | 0.87 |
| Albumin, g/dL * | 4.3 (3.9–4.4) | 3.8 (3.5–4.2) | <0.01 |
| Prothrombin time, % * | 90.5 (77.9–101) | 85 (75.3–94) | <0.01 |
| mALBI 1:2a:2b:3 | 25:5:3:1 | 147:9 2: 84:9 | <0.01 |
| FIB4 index * | 3.78 (2.60–4.60) | 4.62 (2.97–7.74) | 0.01 |
| Child–Pugh score A:B | 33:3 | 295:40 | 0.46 |
| AFP, ng/mL * | 9.8 (4.0–103.5) | 9.3 (4.2–29.9) | 0.43 |
| DCP, mAU/mL * | 61 (25–146.5) | 28.5 (19–62.5) | <0.01 |
| Initial curative treatment (SR:RFA) | 20:16 | 112:223 | 0.01 |
| Tumor size (maximum), cm * | 1.6 (1.5–2.5) | 1.5 (1.2–1.9) | 0.03 |
| Tumor number (single:multiple) | 27:9 | 247:88 | 1.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ohama, H.; Hiraoka, A.; Tada, F.; Kato, K.; Fukunishi, Y.; Yanagihara, E.; Kato, M.; Saneto, H.; Izumoto, H.; Ueki, H.; et al. Comparison of Surgical Resection and Percutaneous Ultrasonographic Guided Radiofrequency Ablation for Initial Recurrence of Hepatocellular Carcinoma in Early Stage following Curative Treatment. Cancers 2022, 14, 5524. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14225524
Ohama H, Hiraoka A, Tada F, Kato K, Fukunishi Y, Yanagihara E, Kato M, Saneto H, Izumoto H, Ueki H, et al. Comparison of Surgical Resection and Percutaneous Ultrasonographic Guided Radiofrequency Ablation for Initial Recurrence of Hepatocellular Carcinoma in Early Stage following Curative Treatment. Cancers. 2022; 14(22):5524. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14225524
Chicago/Turabian StyleOhama, Hideko, Atsushi Hiraoka, Fujimasa Tada, Kanako Kato, Yoshiko Fukunishi, Emi Yanagihara, Masaya Kato, Hironobu Saneto, Hirofumi Izumoto, Hidetaro Ueki, and et al. 2022. "Comparison of Surgical Resection and Percutaneous Ultrasonographic Guided Radiofrequency Ablation for Initial Recurrence of Hepatocellular Carcinoma in Early Stage following Curative Treatment" Cancers 14, no. 22: 5524. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14225524