
Association of Physical Activity Intensity with All-Cause Mortality in Cancer Survivors: A National Prospective Cohort Study

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
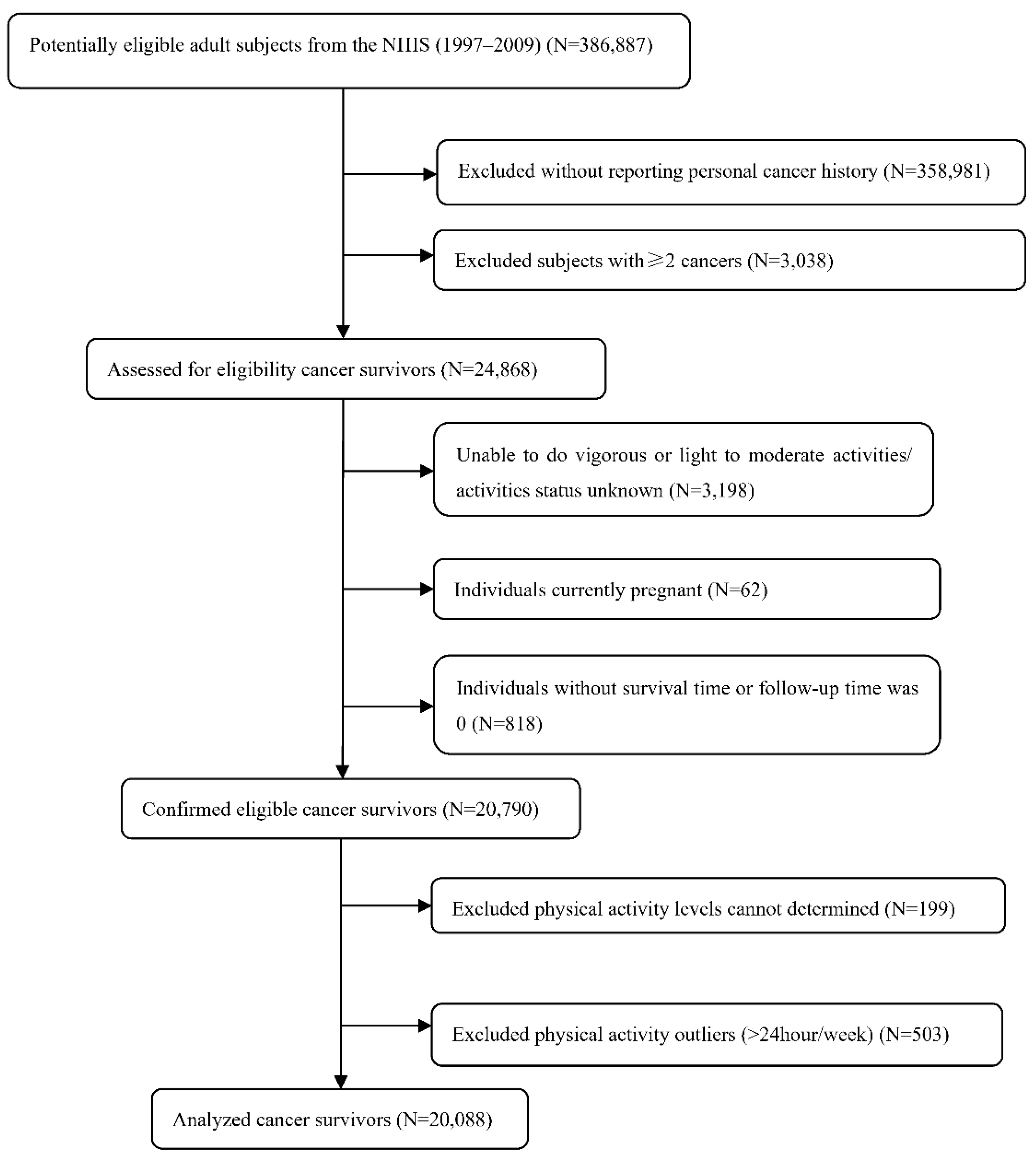
2.1. Study Design and Population
2.2. Study Outcome
2.3. Study Exposure
2.4. Study Covariates
2.5. Statistical Analysis
3. Results
3.1. Population Characteristics
3.2. The Relationship between PA and Cancer Survivors’ Mortality
3.3. Subgroup Analyses
3.4. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arem, H.; Moore, S.C.; Patel, A.; Hartge, P.; De Gonzalez, A.B.; Visvanathan, K.; Campbell, P.T.; Freedman, M.; Weiderpass, E.; Adami, H.O.; et al. Leisure Time Physical Activity and Mortality: A detailed pooled analysis of the dose-response relationship. JAMA Intern. Med. 2015, 175, 959–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, M.; Veeranki, S.P.; Li, S.; Steffen, L.M.; Xi, B. Beneficial associations of low and large doses of leisure time physical activity with all-cause, cardiovascular disease and cancer mortality: A national cohort study of 88,140 US adults. Br. J. Sports Med. 2019, 53, 1405–1411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Nie, J.; Ferrari, G.; Rey-Lopez, J.P.; Rezende, L.F.M. Association of Physical Activity Intensity with Mortality. JAMA Intern. Med. 2021, 181, 203. [Google Scholar] [CrossRef] [PubMed]
- Stamatakis, E.; Gale, J.; Bauman, A.; Ekelund, U.; Hamer, M.; Ding, D. Sitting Time, Physical Activity, and Risk of Mortality in Adults. J. Am. Coll. Cardiol. 2019, 73, 2062–2072. [Google Scholar] [CrossRef]
- Lee, I.-M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T.; Lancet Physical Activity Series Working Group. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Kyu, H.H.; Bachman, V.F.; Alexander, L.T.; Mumford, J.E.; Afshin, A.; Estep, K.; Veerman, J.L.; Delwiche, K.; Iannarone, M.L.; Moyer, M.L.; et al. Physical activity and risk of breast cancer, colon cancer, diabetes, ischemic heart disease, and ischemic stroke events: Systematic review and dose-response meta-analysis for the Global Burden of Disease Study 2013. BMJ 2016, 354, i3857. [Google Scholar] [CrossRef] [Green Version]
- Ekelund, U.; Tarp, J.; Steene-Johannessen, J.; Hansen, B.H.; Jefferis, B.; Fagerland, M.W.; Whincup, P.; Diaz, K.M.; Hooker, S.P.; Chernofsky, A.; et al. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: Systematic review and harmonised meta-analysis. BMJ 2019, 366, l4570. [Google Scholar] [CrossRef] [Green Version]
- Jeong, S.-W.; Kim, S.-H.; Kang, S.-H.; Kim, H.-J.; Yoon, C.-H.; Youn, T.-J.; Chae, I.-H. Mortality reduction with physical activity in patients with and without cardiovascular disease. Eur. Heart J. 2019, 40, 3547–3555. [Google Scholar] [CrossRef] [Green Version]
- Cao, C.; Friedenreich, C.M.; Yang, L. Association of Daily Sitting Time and Leisure-Time Physical Activity With Survival Among US Cancer Survivors. JAMA Oncol. 2022, 8, 395. [Google Scholar] [CrossRef]
- Friedenreich, C.M.; Stone, C.R.; Cheung, W.Y.; Hayes, S.C. Physical Activity and Mortality in Cancer Survivors: A Systematic Review and Meta-Analysis. JNCI Cancer Spectr. 2019, 4, pkz080. [Google Scholar] [CrossRef]
- Holmes, M.D.; Chen, W.; Feskanich, D.; Kroenke, C.; Colditz, G. Physical Activity and Survival After Breast Cancer Diagnosis. JAMA J. Am. Med. Assoc. 2005, 293, 2479–2486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cannioto, R.A.; Dighe, S.; Mahoney, M.C.; Moysich, K.B.; Sen, A.; Hulme, K.; McCann, S.E.; Ambrosone, C.B. Habitual recreational physical activity is associated with significantly improved survival in cancer patients: Evidence from the Roswell Park Data Bank and BioRepository. Cancer Causes Control 2018, 30, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Simon, T.G.; Na Kim, M.; Luo, X.; Yang, W.; Ma, Y.; Chong, D.Q.; Fuchs, C.S.; Meyerhardt, J.A.; Corey, K.E.; Chung, R.T.; et al. Physical activity compared to adiposity and risk of liver-related mortality: Results from two prospective, nationwide cohorts. J. Hepatol. 2020, 72, 1062–1069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Moor, J.S.; Mariotto, A.B.; Parry, C.; Alfano, C.M.; Padgett, L.; Kent, E.E.; Forsythe, L.; Scoppa, S.; Hachey, M.; Rowland, J.H. Cancer Survivors in the United States: Prevalence across the Survivorship Trajectory and Implications for Care. Cancer Epidemiol. Biomark. Prev. 2013, 22, 561–570. [Google Scholar] [CrossRef] [Green Version]
- DeSantis, C.E.; Lin, C.C.; Mariotto, A.B.; Siegel, R.L.; Stein, K.D.; Kramer, J.L.; Alteri, R.; Robbins, A.S.; Jemal, A. Cancer treatment and survivorship statistics, 2014. CA: A Cancer J. Clin. 2014, 64, 252–271. [Google Scholar] [CrossRef] [PubMed]
- Parsons, V.L.; Moriarity, C.; Jonas, K.; Moore, T.F.; Davis, E.K.; Tompkins, L. Design and estimation for the national health interview survey, 2006–2015. Vital-Health Stat. Ser. 2 Data Eval. Methods Res. 2014, 165, 1–53. [Google Scholar]
- Lochner, K.; Hummer, R.A.; Bartee, S.; Wheatcroft, G.; Cox, C. The Public-Use National Health Interview Survey Linked Mortality Files: Methods of Reidentification Risk Avoidance and Comparative Analysis. Am. J. Epidemiol. 2008, 168, 336–344. [Google Scholar] [CrossRef] [Green Version]
- Committee, P.A.G.A. Physical Activity Guidelines for Americans. 2018. Available online: http://www.health.gov/PAGuidelines (accessed on 20 October 2018).
- VanderWeele, T.J.; Ding, P. Sensitivity Analysis in Observational Research: Introducing the E-Value. Ann. Intern. Med. 2017, 167, 268–274. [Google Scholar] [CrossRef] [Green Version]
- Marzorati, C.; Riva, S.; Pravettoni, G. Who Is a Cancer Survivor? A Systematic Review of Published Definitions. J. Cancer Educ. 2016, 32, 228–237. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics. CA Cancer J. Clin. 2021, 71, 7–33, Erratum in CA Cancer J. Clin. 2021, 71, 359. [Google Scholar] [CrossRef]
- Miller, K.D.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Alfano, C.M.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer treatment and survivorship statistics. CA Cancer J. Clin. 2019, 69, 363–385. [Google Scholar] [CrossRef] [PubMed]
- Campbell, K.L.; Winters-Stone, K.M.; Wiskemann, J.; May, A.M.; Schwartz, A.L.; Courneya, K.S.; Zucker, D.S.; Matthews, C.E.; Ligibel, J.A.; Gerber, L.H.; et al. Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Med. Sci. Sports Exerc. 2019, 51, 2375–2390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedenreich, C.M.; Neilson, H.K.; Farris, M.S.; Courneya, K.S. Physical Activity and Cancer Outcomes: A Precision Medicine Approach. Clin. Cancer Res. 2016, 22, 4766–4775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmitz, K.H.; Courneya, K.S.; Matthews, C.; Demark-Wahnefried, W.; Galvão, D.A.; Pinto, B.M.; Irwin, M.L.; Wolin, K.Y.; Segal, R.J.; Lucia, A.; et al. American College of Sports Medicine Roundtable on Exercise Guidelines for Cancer Survivors. Med. Sci. Sports Exerc. 2010, 42, 1409–1426. [Google Scholar] [CrossRef] [PubMed]
- Rock, C.L.; Doyle, C.; Demark-Wahnefried, W.; Meyerhardt, J.; Courneya, K.S.; Schwartz, A.L.; Bandera, E.V.; Hamilton, K.K.; Grant, B.; McCullough, M.; et al. Nutrition and physical activity guidelines for cancer survivors. CA A Cancer J. Clin. 2012, 62, 242–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, A.V.; Friedenreich, C.M.; Moore, S.C.; Hayes, S.C.; Silver, J.K.; Campbell, K.L.; Winters-Stone, K.; Gerber, L.H.; George, S.M.; Fulton, J.E.; et al. American College of Sports Medicine Roundtable Report on Physical Activity, Sedentary Behavior, and Cancer Prevention and Control. Med. Sci. Sports Exerc. 2019, 51, 2391–2402. [Google Scholar] [CrossRef] [Green Version]
- Hirko, K.A.; Dorn, J.M.; Dearing, J.W.; Alfano, C.M.; Wigton, A.; Schmitz, K.H. Implementation of Physical Activity Programs for Rural Cancer Survivors: Challenges and Opportunities. Int. J. Environ. Res. Public Health 2021, 18, 12909. [Google Scholar] [CrossRef]
- Chung, J.Y.; Lee, D.H.; Park, J.-H.; Lee, M.K.; Kang, D.-W.; Min, J.; Kim, D.-I.; Jeong, D.H.; Kim, N.-K.; Meyerhardt, J.A.; et al. Patterns of physical activity participation across the cancer trajectory in colorectal cancer survivors. Support. Care Cancer 2013, 21, 1605–1612. [Google Scholar] [CrossRef]
- Hair, B.Y.; Hayes, S.; Tse, C.-K.; Bell, M.B.; Olshan, A.F. Racial differences in physical activity among breast cancer survivors: Implications for breast cancer care. Cancer 2014, 120, 2174–2182. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, M.E.G.; Green, J.; Reeves, G.K.; Beral, V.; Cairns, B. Frequent Physical Activity May Not Reduce Vascular Disease Risk as Much as Moderate Activity. Circulation 2015, 131, 721–729. [Google Scholar] [CrossRef] [Green Version]
- Schnohr, P.; O’Keefe, J.H.; Marott, J.L.; Lange, P.; Jensen, G.B. Dose of Jogging and Long-Term Mortality. J. Am. Coll. Cardiol. 2015, 65, 411–419. [Google Scholar] [CrossRef]
- Noone, A.-M.; Cronin, K.A.; Altekruse, S.F.; Howlader, N.; Lewis, D.R.; Petkov, V.I.; Penberthy, L. Cancer Incidence and Survival Trends by Subtype Using Data from the Surveillance Epidemiology and End Results Program, 1992–2013. Cancer Epidemiol. Biomark. Prev. 2017, 26, 632–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eschke, R.-C.K.-R.; Lampit, A.; Schenk, A.; Javelle, F.; Steindorf, K.; Diel, P.; Bloch, W.; Zimmer, P. Impact of Physical Exercise on Growth and Progression of Cancer in Rodents—A Systematic Review and Meta-Analysis. Front. Oncol. 2019, 9, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Ashcraft, K.A.; Peace, R.M.; Betof, A.S.; Dewhirst, M.W.; Jones, L.W. Efficacy and Mechanisms of Aerobic Exercise on Cancer Initiation, Progression, and Metastasis: A Critical Systematic Review of In Vivo Preclinical Data. Cancer Res. 2016, 76, 4032–4050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hojman, P.; Gehl, J.; Christensen, J.F.; Pedersen, B.K. Molecular Mechanisms Linking Exercise to Cancer Prevention and Treatment. Cell Metab. 2018, 27, 10–21. [Google Scholar] [CrossRef] [Green Version]
- Bland, K.A.; Zadravec, K.; Landry, T.; Weller, S.; Meyers, L.; Campbell, K.L. Impact of exercise on chemotherapy completion rate: A systematic review of the evidence and recommendations for future exercise oncology research. Crit. Rev. Oncol. 2019, 136, 79–85. [Google Scholar] [CrossRef]
- Yang, L.; Morielli, A.R.; Heer, E.; Kirkham, A.A.; Cheung, W.Y.; Usmani, N.; Friedenreich, C.M.; Courneya, K.S. Effects of Exercise on Cancer Treatment Efficacy: A Systematic Review of Preclinical and Clinical Studies. Cancer Res. 2021, 81, 4889–4895. [Google Scholar] [CrossRef]
- Albrecht, T.A.; Taylor, A.G. Physical Activity in Patients with Advanced-Stage Cancer: A Systematic Review of the Literature. Clin. J. Oncol. Nurs. 2012, 16, 293–300. [Google Scholar] [CrossRef] [Green Version]
- Dogra, S.; Wolf, M.; Jeffrey, M.P.; Foley, R.C.A.; Logan-Sprenger, H.; Jones-Taggart, H.; Green-Johnson, J.M. Disrupting prolonged sitting reduces IL-8 and lower leg swell in active young adults. BMC Sports Sci. Med. Rehabil. 2019, 11, 23–27. [Google Scholar] [CrossRef]
- Dunstan, D.W.; Dogra, S.; Carter, S.E.; Owen, N. Sit less and move more for cardiovascular health: Emerging insights and opportunities. Nat. Rev. Cardiol. 2021, 18, 637–648. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Leisure Time PA Level, Minutes/Week | |||||||
|---|---|---|---|---|---|---|---|
| 0 | 10 min–1 h | 1–2.5 h | 2.5–5 h | 5–7.5 h | 7.5–13.3 h | 13.3–24 h | |
| Sex, % | |||||||
| Female | 5718 (64.71%) | 764 (67.37%) | 1959 (65.52%) | 1661 (60.84%) | 1076 (60.35%) | 869 (53.74%) | 493 (49.45%) |
| Male | 3119 (35.29%) | 370 (32.63%) | 1031 (34.48%) | 1069 (39.16%) | 707 (39.65%) | 748 (46.26%) | 504 (50.55%) |
| Age, years, % | |||||||
| <40 | 690 (7.81%) | 111 (9.79%) | 281 (9.40%) | 278 (10.18%) | 240 (13.46%) | 259 (16.02%) | 158 (15.85%) |
| 40–59 | 2227 (25.20%) | 388 (34.22%) | 928 (31.04%) | 928 (33.99%) | 629 (35.28%) | 620 (38.34%) | 328 (32.90%) |
| ≥60 | 5920 (66.99%) | 635 (56.00%) | 1781 (59.57%) | 1524 (55.82%) | 914 (51.26%) | 738 (45.64%) | 511 (51.25%) |
| Body mass index, kg/m2, % | |||||||
| <18.5 | 267 (3.12%) | 23 (2.10%) | 68 (2.33%) | 41 (1.53%) | 25 (1.42%) | 22 (1.38%) | 16 (1.63%) |
| 18.5–24.9 | 2997 (35.00%) | 349 (31.84%) | 1083 (37.04%) | 1078 (40.34%) | 744 (42.27%) | 671 (42.15%) | 408 (41.68%) |
| 25–29.9 | 2983 (34.83%) | 385 (35.13%) | 1068 (36.53%) | 1031 (38.59%) | 650 (36.93%) | 621 (39.01%) | 362 (36.98%) |
| ≥30 | 2317 (27.06%) | 339 (30.93%) | 705 (24.11%) | 522 (19.54%) | 341 (19.38%) | 278 (17.46%) | 193 (19.71%) |
| Race/ethnicity, % | |||||||
| White | 7645 (86.51%) | 979 (86.33%) | 2706 (90.50%) | 2503 (91.68%) | 1640 (91.98%) | 1495 (92.46%) | 900 (90.27%) |
| Black | 957 (10.83%) | 118 (10.41%) | 201 (6.72%) | 168 (6.15%) | 87 (4.88%) | 79 (4.89%) | 60 (6.02%) |
| Other | 235 (2.66%) | 37 (3.26%) | 83 (2.78%) | 59 (2.16%) | 56 (3.14%) | 43 (2.66%) | 37 (3.71%) |
| Marital status, % | |||||||
| Married/Living with partner | 4074 (46.18%) | 582 (51.41%) | 1592 (53.30%) | 1539 (56.46%) | 1028 (57.69%) | 975 (60.30%) | 572 (57.49%) |
| Divorced/separated/widowed | 4062 (46.04%) | 453 (40.02%) | 1152 (38.57%) | 923 (33.86%) | 578 (32.44%) | 472 (29.19%) | 324 (32.56%) |
| Never married | 686 (7.78%) | 97 (8.57%) | 243 (8.14%) | 264 (9.68%) | 176 (9.88%) | 170 (10.51%) | 99 (9.95%) |
| Alcohol drinking, % | |||||||
| Lifetime abstainer | 2630 (37.20%) | 213 (26.30%) | 550 (25.87%) | 427 (22.71%) | 232 (19.46%) | 174 (16.84%) | 145 (21.71%) |
| Former drinker | 1864 (26.37%) | 206 (25.43%) | 512 (24.08%) | 432 (22.98%) | 252 (21.14%) | 194 (18.78%) | 150 (22.46%) |
| Current drinker | 2575 (36.43%) | 391 (48.27%) | 1064 (50.05%) | 1021 (54.31%) | 708 (59.40%) | 665 (64.38%) | 373 (55.84%) |
| Smoking status, % | |||||||
| Never | 1806 (20.50%) | 191 (16.84%) | 464 (15.54%) | 357 (13.09%) | 269 (15.10%) | 211 (13.07%) | 162 (16.27%) |
| Former | 1750 (19.86%) | 209 (18.43%) | 607 (20.34%) | 592 (21.71%) | 368 (20.65%) | 358 (22.18%) | 214 (21.49%) |
| Current | 3510 (39.84%) | 472 (41.62%) | 1241 (41.57%) | 1133 (41.55%) | 748 (41.98%) | 667 (41.33%) | 399 (40.06%) |
| Smoker, current status unknown | 1745 (19.80%) | 262 (23.10%) | 673 (22.55%) | 645 (23.65%) | 397 (22.28%) | 378 (23.42%) | 221 (22.19%) |
| Diabetes, % | |||||||
| No | 7228 (81.83%) | 969 (85.45%) | 2578 (86.28%) | 2377 (87.07%) | 1574 (88.28%) | 1468 (90.79%) | 904 (90.67%) |
| Yes | 1462 (16.55%) | 150 (13.23%) | 354 (11.85%) | 300 (10.99%) | 176 (9.87%) | 130 (8.04%) | 77 (7.72%) |
| Borderline | 143 (1.62%) | 15 (1.32%) | 56 (1.87%) | 53 (1.94%) | 33 (1.85%) | 19 (1.18%) | 16 (1.60%) |
| Hypertension, % | |||||||
| No | 4178 (47.32%) | 572 (50.49%) | 1610 (53.90%) | 1579 (57.86%) | 1064 (59.74%) | 1060 (65.55%) | 606 (60.84%) |
| Yes | 4652 (52.68%) | 561 (49.51%) | 1377 (46.10%) | 1150 (42.14%) | 717 (40.26%) | 557 (34.45%) | 390 (39.16%) |
| Coronary heart disease, % | |||||||
| No | 7763 (88.10%) | 1026 (90.72%) | 2711 (90.97%) | 2485 (91.16%) | 1640 (92.24%) | 1501 (92.88%) | 916 (92.06%) |
| Yes | 1049 (11.90%) | 105 (9.28%) | 269 (9.03%) | 241 (8.84%) | 138 (7.76%) | 115 (7.12%) | 79 (7.94%) |
| Angina, % | |||||||
| No | 8145 (92.41%) | 1070 (94.52%) | 2793 (93.69%) | 2590 (94.98%) | 1691 (95.05%) | 1543 (95.48%) | 959 (96.29%) |
| Yes | 669 (7.59%) | 62 (5.48%) | 188 (6.31%) | 137 (5.02%) | 88 (4.95%) | 73 (4.52%) | 37 (3.71%) |
| Myocardial infarction, % | |||||||
| No | 7879 (89.34%) | 1048 (92.50%) | 2778 (93.07%) | 2544 (93.29%) | 1688 (94.78%) | 1523 (94.25%) | 945 (94.78%) |
| Yes | 940 (10.66%) | 85 (7.50%) | 207 (6.93%) | 183 (6.71%) | 93 (5.22%) | 93 (5.75%) | 52 (5.22%) |
| Stroke, % | |||||||
| No | 8036 (91.12%) | 1071 (94.69%) | 2853 (95.42%) | 2621 (96.08%) | 1721 (96.74%) | 1580 (97.71%) | 957 (95.99%) |
| Yes | 783 (8.88%) | 60 (5.31%) | 137 (4.58%) | 107 (3.92%) | 58 (3.26%) | 37 (2.29%) | 40 (4.01%) |
| Asthma, % | |||||||
| No | 7618 (86.31%) | 981 (86.74%) | 2623 (87.84%) | 2409 (88.34%) | 1578 (88.65%) | 1425 (88.13%) | 889 (89.17%) |
| Yes | 1208 (13.69%) | 150 (13.26%) | 363 (12.16%) | 318 (11.66%) | 202 (11.35%) | 192 (11.87%) | 108 (10.83%) |
| Non-Adjusted | Adjust I | Adjust II | |
|---|---|---|---|
| All-cause mortality | |||
| PA(Continuous) | 0.92 (0.91, 0.92) < 0.0001 | 0.94 (0.93, 0.95) < 0.0001 | 0.95 (0.95, 0.96) < 0.0001 |
| PA level | |||
| 0 | 1 (Reference) | 1 (Reference) | 1 (Reference) |
| 10 min–1 h | 0.60 (0.54, 0.67) < 0.0001 | 0.71 (0.64, 0.79) < 0.0001 | 0.75 (0.67, 0.85) < 0.0001 |
| 1–2.5 h | 0.60 (0.56, 0.64) < 0.0001 | 0.67 (0.63, 0.72) < 0.0001 | 0.72 (0.67, 0.78) < 0.0001 |
| 2.5–5 h | 0.48 (0.45, 0.52) < 0.0001 | 0.58 (0.54, 0.63) < 0.0001 | 0.66 (0.60, 0.72) < 0.0001 |
| 5–7.5 h | 0.43 (0.39, 0.48) < 0.0001 | 0.55 (0.50, 0.61) < 0.0001 | 0.63 (0.56, 0.70) < 0.0001 |
| 7.5–13.3 h | 0.35 (0.32, 0.40) < 0.0001 | 0.48 (0.42, 0.53) < 0.0001 | 0.53 (0.47, 0.61) < 0.0001 |
| 13.3–24 h | 0.39 (0.34, 0.45) < 0.0001 | 0.50 (0.43, 0.57) < 0.0001 | 0.57 (0.49, 0.66) < 0.0001 |
| p for trend | <0.001 | <0.001 | <0.001 |
| Cancer mortality | |||
| PA(Continuous) | 0.89 (0.83, 0.96) 0.0027 | 0.91 (0.85, 0.98) 0.0114 | 0.90 (0.83, 0.98) 0.0115 |
| PA level | |||
| 0 | 1 (Reference) | 1 (Reference) | 1 (Reference) |
| 10 min–1 h | 0.64 (0.26, 1.58) 0.3328 | 0.70 (0.28, 1.73) 0.4362 | 0.86 (0.35, 2.15) 0.7535 |
| 1–2.5 h | 0.25 (0.11, 0.58) 0.0011 | 0.28 (0.12, 0.64) 0.0025 | 0.23 (0.08, 0.64) 0.0046 |
| 2.5–5 h | 0.48 (0.24, 0.96) 0.0371 | 0.55 (0.27, 1.10) 0.0884 | 0.61 (0.29, 1.30) 0.2007 |
| 5–7.5 h | 0.31 (0.11, 0.84) 0.0212 | 0.36 (0.13, 0.98) 0.0461 | 0.42 (0.15, 1.17) 0.0986 |
| 7.5–13.3 h | 0.29 (0.09, 0.93) 0.0365 | 0.34 (0.11, 1.09) 0.0701 | 0.29 (0.07, 1.20) 0.0872 |
| 13.3–24 h | 0.45 (0.14, 1.43) 0.1771 | 0.48 (0.15, 1.55) 0.2208 | 0.37 (0.09, 1.51) 0.1646 |
| p for trend | 0.003 | 0.011 | 0.011 |
| Cardiovascular disease mortality | |||
| PA(Continuous) | 0.96 (0.93, 0.99) 0.0084 | 0.96 (0.93, 0.99) 0.0083 | 0.95 (0.91, 0.98) 0.0052 |
| PA level | |||
| 0 | 1 (Reference) | 1 (Reference) | 1 (Reference) |
| 10 min–1 h | 1.24 (0.79, 1.92) 0.3478 | 1.32 (0.85, 2.05) 0.2222 | 1.39 (0.88, 2.20) 0.1632 |
| 1–2.5 h | 0.83 (0.60, 1.14) 0.2530 | 0.88 (0.63, 1.22) 0.4368 | 0.84 (0.59, 1.22) 0.3674 |
| 2.5–5 h | 0.80 (0.55, 1.15) 0.2232 | 0.84 (0.58, 1.22) 0.3643 | 0.69 (0.45, 1.06) 0.0906 |
| 5–7.5 h | 0.89 (0.59, 1.34) 0.5828 | 0.90 (0.60, 1.36) 0.6229 | 0.87 (0.55, 1.37) 0.5429 |
| 7.5–13.3 h | 0.68 (0.41, 1.14) 0.1412 | 0.71 (0.43, 1.19) 0.1979 | 0.60 (0.32, 1.11) 0.1027 |
| 13.3–24 h | 0.46 (0.22, 0.98) 0.0447 | 0.40 (0.18, 0.91) 0.0294 | 0.40 (0.16, 0.99) 0.0470 |
| p for trend | 0.008 | 0.003 | 0.005 |
| Inflection Point | Group | HR (95% CI) | p Value | p for Log Likelihood Ratio Test | |
|---|---|---|---|---|---|
| Physical activity | 1 h/week | ≤1 | 0.70 (0.66, 0.75) | <0.001 | <0.001 |
| >1 | 0.98 (0.97, 0.99) | <0.001 |
| Variable | Participants, No. | 0 | 10 min–1 h | 1–2.5 h | 2.5–5 h | 5–7.5 h | 7.5–13.3 h | 13.3–24 h | p Value for Interaction |
|---|---|---|---|---|---|---|---|---|---|
| Age, y | 0.7287 | ||||||||
| <40 | 2017 | 1 [Reference] | 0.77 (0.33, 1.83) 0.5598 | 0.78 (0.44, 1.40) 0.4113 | 0.40 (0.19, 0.84) 0.0155 | 0.64 (0.32, 1.28) 0.2076 | 0.61 (0.31, 1.21) 0.1573 | 0.51 (0.20, 1.29) 0.1561 | |
| 40–59 | 6048 | 1 [Reference] | 0.88 (0.65, 1.19) 0.4071 | 0.70 (0.56, 0.89) 0.0029 | 0.57 (0.44, 0.73) < 0.0001 | 0.66 (0.50, 0.88) 0.0041 | 0.53 (0.38, 0.73) < 0.0001 | 0.45 (0.29, 0.68) 0.0002 | |
| ≥60 | 12023 | 1 [Reference] | 0.70 (0.61, 0.80) < 0.0001 | 0.68 (0.62, 0.74) < 0.0001 | 0.59 (0.54, 0.65) < 0.0001 | 0.56 (0.49, 0.63) < 0.0001 | 0.44 (0.38, 0.51) < 0.0001 | 0.50 (0.42, 0.59) < 0.0001 | |
| Sex | 0.603 | ||||||||
| Female | 12540 | 1 [Reference] | 0.77 (0.66, 0.91) 0.0016 | 0.70 (0.63, 0.78) < 0.0001 | 0.66 (0.58, 0.75) < 0.0001 | 0.64 (0.55, 0.75) < 0.0001 | 0.52 (0.42, 0.64) < 0.0001 | 0.49 (0.38, 0.64) < 0.0001 | |
| Male | 7548 | 1 [Reference] | 0.72 (0.60, 0.87) 0.0008 | 0.76 (0.67, 0.86) < 0.0001 | 0.65 (0.57, 0.74) < 0.0001 | 0.62 (0.53, 0.73) < 0.0001 | 0.54 (0.45, 0.64) < 0.0001 | 0.62 (0.51, 0.74) < 0.0001 | |
| BMI, Kg/m2 | 0.1238 | ||||||||
| <18.5 | 462 | 1 [Reference] | 0.76 (0.32, 1.80) 0.5259 | 0.69 (0.44, 1.07) 0.0951 | 0.42 (0.23, 0.79) 0.0068 | 0.33 (0.14, 0.80) 0.0140 | 0.44 (0.13, 1.47) 0.1815 | 0.53 (0.16, 1.71) 0.2851 | |
| 18.5–24.9 | 7330 | 1 [Reference] | 0.76 (0.32, 1.80) 0.5259 | 0.69 (0.44, 1.07) 0.0951 | 0.42 (0.23, 0.79) 0.0068 | 0.33 (0.14, 0.80) 0.0140 | 0.44 (0.13, 1.47) 0.1815 | 0.53 (0.16, 1.71) 0.2851 | |
| 25–29.9 | 7100 | 1 [Reference] | 0.73 (0.59, 0.90) 0.0034 | 0.78 (0.68, 0.89) 0.0002 | 0.71 (0.62, 0.82) < 0.0001 | 0.74 (0.62, 0.89) 0.0012 | 0.62 (0.50, 0.75) < 0.0001 | 0.57 (0.44, 0.74) < 0.0001 | |
| ≥30 | 4695 | 1 [Reference] | 0.82 (0.64, 1.04) 0.0937 | 0.63 (0.53, 0.77) < 0.0001 | 0.65 (0.52, 0.80) < 0.0001 | 0.50 (0.38, 0.67) < 0.0001 | 0.56 (0.41, 0.77) 0.0004 | 0.82 (0.60, 1.12) 0.2066 | |
| Race/ethnicity | 0.5269 | ||||||||
| White | 17868 | 1 [Reference] | 0.75 (0.66, 0.86) < 0.0001 | 0.72 (0.66, 0.78) < 0.0001 | 0.67 (0.61, 0.73) < 0.0001 | 0.65 (0.58, 0.73) < 0.0001 | 0.54 (0.47, 0.62) < 0.0001 | 0.57 (0.49, 0.67) < 0.0001 | |
| Black | 1670 | 1 [Reference] | 0.69 (0.46, 1.02) 0.0640 | 0.72 (0.54, 0.96) 0.0229 | 0.54 (0.38, 0.77) 0.0006 | 0.55 (0.35, 0.86) 0.0093 | 0.59 (0.33, 1.02) 0.0606 | 0.80 (0.47, 1.38) 0.4282 | |
| Other | 550 | 1 [Reference] | 1.12 (0.59, 2.12) 0.7376 | 0.61 (0.30, 1.27) 0.1906 | 0.80 (0.42, 1.53) 0.5025 | 0.37 (0.15, 0.90) 0.0287 | 0.32 (0.11, 0.93) 0.0360 | 0.16 (0.02, 1.15) 0.0678 | |
| Marital status | 0.907 | ||||||||
| Married/Living with partner | 10362 | 1 [Reference] | 0.75 (0.62, 0.90) 0.0018 | 0.69 (0.61, 0.78) < 0.0001 | 0.67 (0.59, 0.76) < 0.0001 | 0.62 (0.53, 0.73) < 0.0001 | 0.54 (0.45, 0.65) < 0.0001 | 0.55 (0.44, 0.68) < 0.0001 | |
| Divorced/separated/widowed | 7964 | 1 [Reference] | 0.73 (0.61, 0.87) 0.0004 | 0.74 (0.67, 0.83) < 0.0001 | 0.64 (0.56, 0.73) < 0.0001 | 0.66 (0.56, 0.78) < 0.0001 | 0.51 (0.41, 0.63) < 0.0001 | 0.58 (0.46, 0.73) < 0.0001 | |
| Never married | 1735 | 1 [Reference] | 1.11 (0.69, 1.77) 0.6709 | 0.72 (0.51, 1.01) 0.0605 | 0.67 (0.45, 0.98) 0.0403 | 0.52 (0.32, 0.85) 0.0082 | 0.68 (0.42, 1.11) 0.1247 | 0.62 (0.34, 1.13) 0.1195 | |
| Alcohol drinking | 0.941 | ||||||||
| Lifetime abstainer | 4371 | 1 [Reference] | 0.80 (0.64, 1.00) 0.0540 | 0.70 (0.60, 0.82) < 0.0001 | 0.68 (0.57, 0.82) < 0.0001 | 0.60 (0.47, 0.76) < 0.0001 | 0.52 (0.38, 0.71) < 0.0001 | 0.61 (0.45, 0.84) 0.0025 | |
| Former drinker | 3610 | 1 [Reference] | 0.78 (0.63, 0.96) 0.0218 | 0.69 (0.60, 0.80) < 0.0001 | 0.60 (0.51, 0.71) < 0.0001 | 0.61 (0.49, 0.75) < 0.0001 | 0.48 (0.36, 0.64) < 0.0001 | 0.62 (0.47, 0.82) 0.0007 | |
| Current drinker | 6797 | 1 [Reference] | 0.71 (0.59, 0.86) 0.0006 | 0.75 (0.66, 0.85) < 0.0001 | 0.69 (0.61, 0.79) < 0.0001 | 0.67 (0.57, 0.78) < 0.0001 | 0.57 (0.48, 0.68) < 0.0001 | 0.54 (0.43, 0.67) < 0.0001 | |
| Smoking status | 0.032 | ||||||||
| Never | 3460 | 1 [Reference] | 0.99 (0.74, 1.34) 0.9635 | 0.74 (0.60, 0.92) 0.0054 | 0.54 (0.41, 0.71) < 0.0001 | 0.78 (0.60, 1.03) 0.0807 | 0.80 (0.59, 1.09) 0.1512 | 0.60 (0.41, 0.88) 0.0079 | |
| Former | 4089 | 1 [Reference] | 0.74 (0.60, 0.92) 0.0066 | 0.73 (0.64, 0.83) < 0.0001 | 0.69 (0.60, 0.80) < 0.0001 | 0.70 (0.59, 0.85) 0.0002 | 0.54 (0.44, 0.66) < 0.0001 | 0.60 (0.48, 0.76) < 0.0001 | |
| Current | 8170 | 1 [Reference] | 0.64 (0.52, 0.77) < 0.0001 | 0.68 (0.60, 0.77) < 0.0001 | 0.64 (0.56, 0.74) < 0.0001 | 0.54 (0.45, 0.65) < 0.0001 | 0.44 (0.35, 0.55) < 0.0001 | 0.50 (0.39, 0.65) < 0.0001 | |
| Diabetes | 0.9089 | ||||||||
| No | 17098 | 1 [Reference] | 0.74 (0.65, 0.85) < 0.0001 | 0.72 (0.66, 0.79) < 0.0001 | 0.65 (0.59, 0.72) < 0.0001 | 0.63 (0.55, 0.71) < 0.0001 | 0.50 (0.43, 0.58) < 0.0001 | 0.55 (0.47, 0.65) < 0.0001 | |
| Yes | 2649 | 1 [Reference] | 0.80 (0.60, 1.05) 0.1086 | 0.68 (0.56, 0.83) 0.0002 | 0.67 (0.54, 0.82) 0.0002 | 0.67 (0.51, 0.88) 0.0041 | 0.70 (0.52, 0.95) 0.0215 | 0.77 (0.51, 1.15) 0.1979 | |
| Hypertension | 0.0435 | ||||||||
| No | 10669 | 1 [Reference] | 0.69 (0.57, 0.84) 0.0002 | 0.77 (0.68, 0.86) < 0.0001 | 0.65 (0.57, 0.74) < 0.0001 | 0.59 (0.50, 0.70) < 0.0001 | 0.47 (0.39, 0.57) < 0.0001 | 0.49 (0.39, 0.62) < 0.0001 | |
| Yes | 9404 | 1 [Reference] | 0.80 (0.68, 0.93) 0.0046 | 0.68 (0.61, 0.76) < 0.0001 | 0.66 (0.58, 0.74) < 0.0001 | 0.66 (0.57, 0.77) < 0.0001 | 0.60 (0.50, 0.72) < 0.0001 | 0.64 (0.53, 0.79) < 0.0001 | |
| Coronary heart disease | 0.0428 | ||||||||
| No | 18042 | 1 [Reference] | 0.75 (0.66, 0.86) < 0.0001 | 0.73 (0.67, 0.79) < 0.0001 | 0.63 (0.57, 0.69) < 0.0001 | 0.61 (0.54, 0.69) < 0.0001 | 0.53 (0.46, 0.61) < 0.0001 | 0.53 (0.44, 0.62) < 0.0001 | |
| Yes | 1996 | 1 [Reference] | 0.76 (0.55, 1.05) 0.0944 | 0.70 (0.56, 0.86) 0.0007 | 0.81 (0.65, 1.01) 0.0560 | 0.77 (0.58, 1.02) 0.0661 | 0.53 (0.37, 0.75) 0.0003 | 0.88 (0.62, 1.25) 0.4626 | |
| Angina | 0.2168 | ||||||||
| No | 18791 | 1 [Reference] | 0.76 (0.67, 0.86) < 0.0001 | 0.72 (0.66, 0.78) < 0.0001 | 0.64 (0.58, 0.70) < 0.0001 | 0.60 (0.54, 0.68) < 0.0001 | 0.54 (0.47, 0.62) < 0.0001 | 0.57 (0.49, 0.67) < 0.0001 | |
| Yes | 1254 | 1 [Reference] | 0.67 (0.45, 1.01) 0.0585 | 0.72 (0.57, 0.92) 0.0081 | 0.80 (0.61, 1.04) 0.0992 | 0.93 (0.66, 1.30) 0.6648 | 0.50 (0.33, 0.76) 0.0013 | 0.51 (0.28, 0.92) 0.0258 | |
| Myocardial infarction | 0.3738 | ||||||||
| No | 18405 | 1 [Reference] | 0.77 (0.67, 0.87) < 0.0001 | 0.72 (0.66, 0.78) < 0.0001 | 0.63 (0.58, 0.70) < 0.0001 | 0.62 (0.55, 0.70) < 0.0001 | 0.54 (0.47, 0.61) < 0.0001 | 0.57 (0.48, 0.67) < 0.0001 | |
| Yes | 1653 | 1 [Reference] | 0.62 (0.44, 0.88) 0.0066 | 0.69 (0.55, 0.86) 0.0012 | 0.80 (0.63, 1.01) 0.0571 | 0.66 (0.47, 0.92) 0.0149 | 0.49 (0.32, 0.73) 0.0005 | 0.57 (0.35, 0.92) 0.0218 | |
| Stroke | 0.0876 | ||||||||
| No | 18839 | 1 [Reference] | 0.79 (0.70, 0.90) 0.0003 | 0.73 (0.67, 0.79) < 0.0001 | 0.66 (0.60, 0.72) < 0.0001 | 0.63 (0.56, 0.70) < 0.0001 | 0.53 (0.46, 0.61) < 0.0001 | 0.55 (0.47, 0.65) < 0.0001 | |
| Yes | 1222 | 1 [Reference] | 0.43 (0.27, 0.69) 0.0004 | 0.66 (0.51, 0.86) 0.0018 | 0.66 (0.48, 0.91) 0.0102 | 0.62 (0.41, 0.95) 0.0264 | 0.50 (0.27, 0.92) 0.0249 | 0.95 (0.56, 1.61) 0.8575 | |
| Asthma | 0.7195 | ||||||||
| No | 17523 | 1 [Reference] | 0.76 (0.67, 0.87) < 0.0001 | 0.72 (0.66, 0.79) < 0.0001 | 0.66 (0.61, 0.73) < 0.0001 | 0.63 (0.56, 0.70) < 0.0001 | 0.54 (0.47, 0.62) < 0.0001 | 0.56 (0.48, 0.65) < 0.0001 | |
| Yes | 2541 | 1 [Reference] | 0.74 (0.52, 1.04) 0.0853 | 0.71 (0.56, 0.91) 0.0073 | 0.61 (0.46, 0.81) 0.0006 | 0.64 (0.44, 0.94) 0.0241 | 0.44 (0.27, 0.71) 0.0009 | 0.78 (0.44, 1.36) 0.3772 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Q.; Pan, X.; Li, X.; Huang, W. Association of Physical Activity Intensity with All-Cause Mortality in Cancer Survivors: A National Prospective Cohort Study. Cancers 2022, 14, 5760. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14235760
Li Q, Pan X, Li X, Huang W. Association of Physical Activity Intensity with All-Cause Mortality in Cancer Survivors: A National Prospective Cohort Study. Cancers. 2022; 14(23):5760. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14235760
Chicago/Turabian StyleLi, Qiguang, Xueqiang Pan, Xiao Li, and Wei Huang. 2022. "Association of Physical Activity Intensity with All-Cause Mortality in Cancer Survivors: A National Prospective Cohort Study" Cancers 14, no. 23: 5760. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers14235760