
Hotspot on 18F-FET PET/CT to Predict Aggressive Tumor Areas for Radiotherapy Dose Escalation Guiding in High-Grade Glioma

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
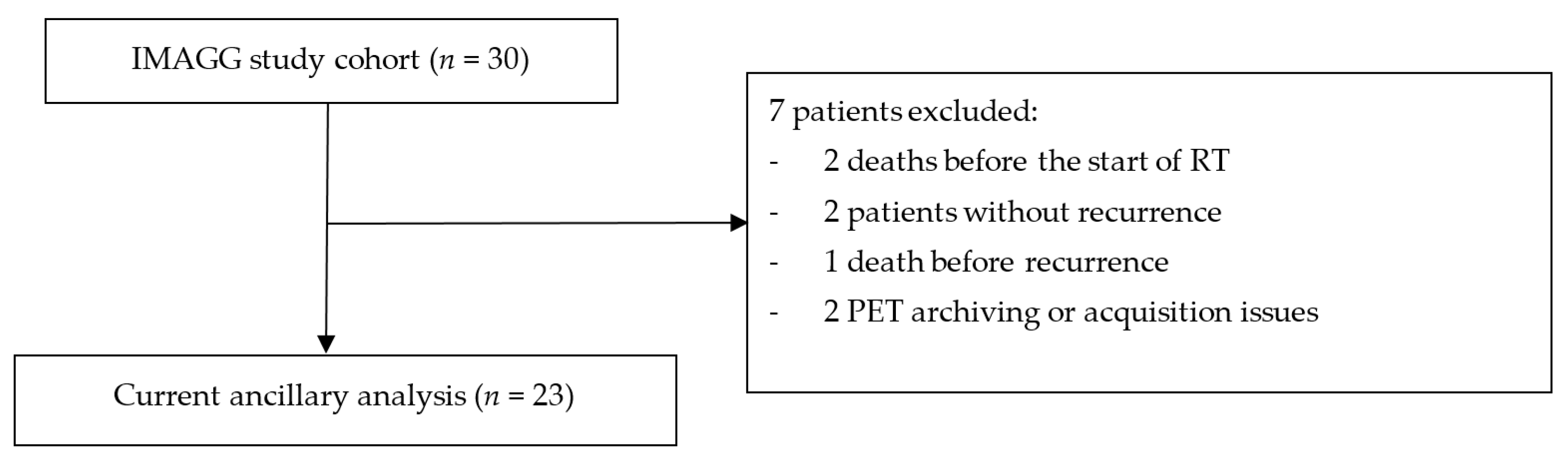
2.1. Population
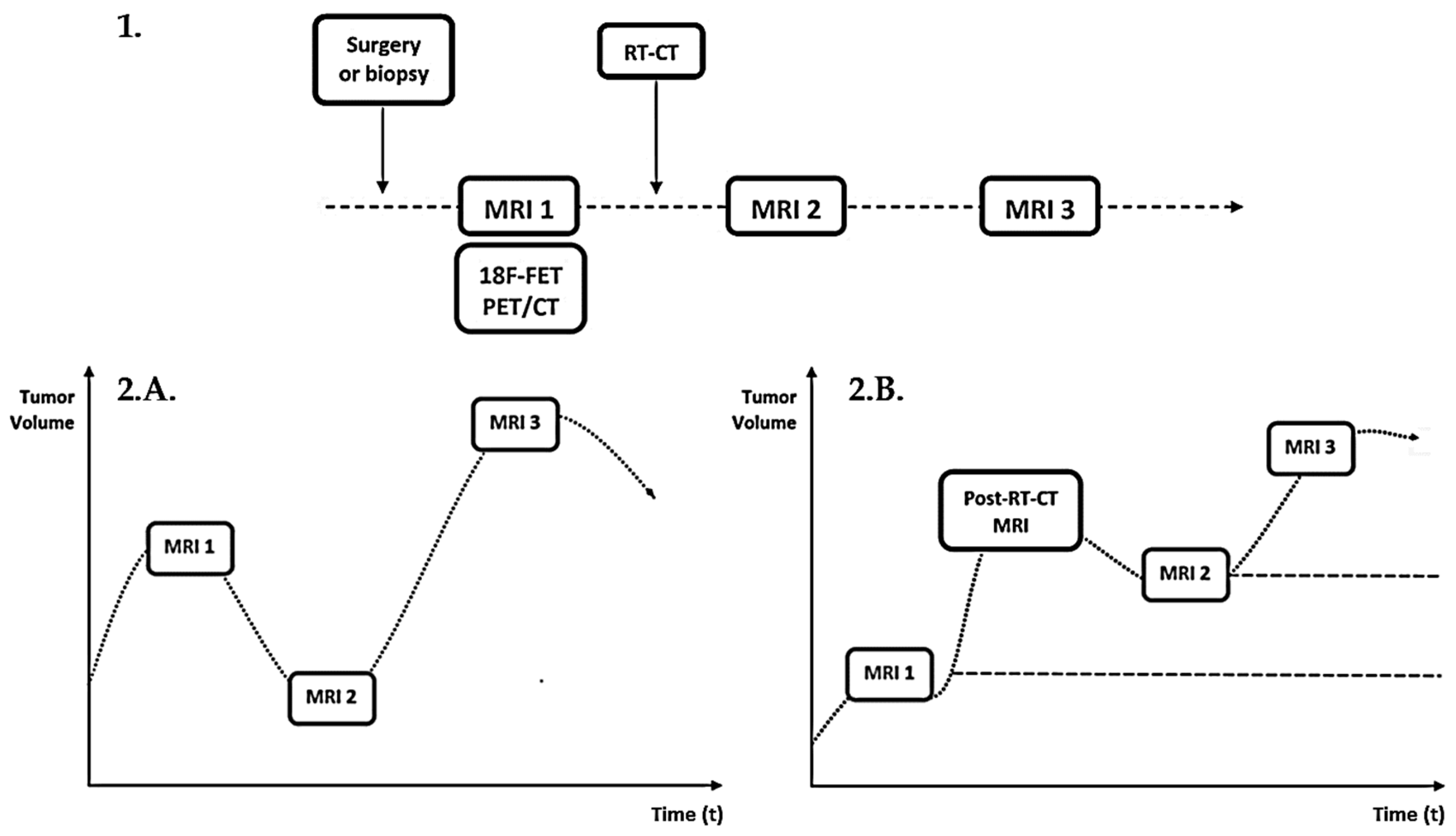
2.2. Imaging Protocol
2.2.1. MRI
2.2.2. FET PET
2.3. Target Volume Delineation on MRI
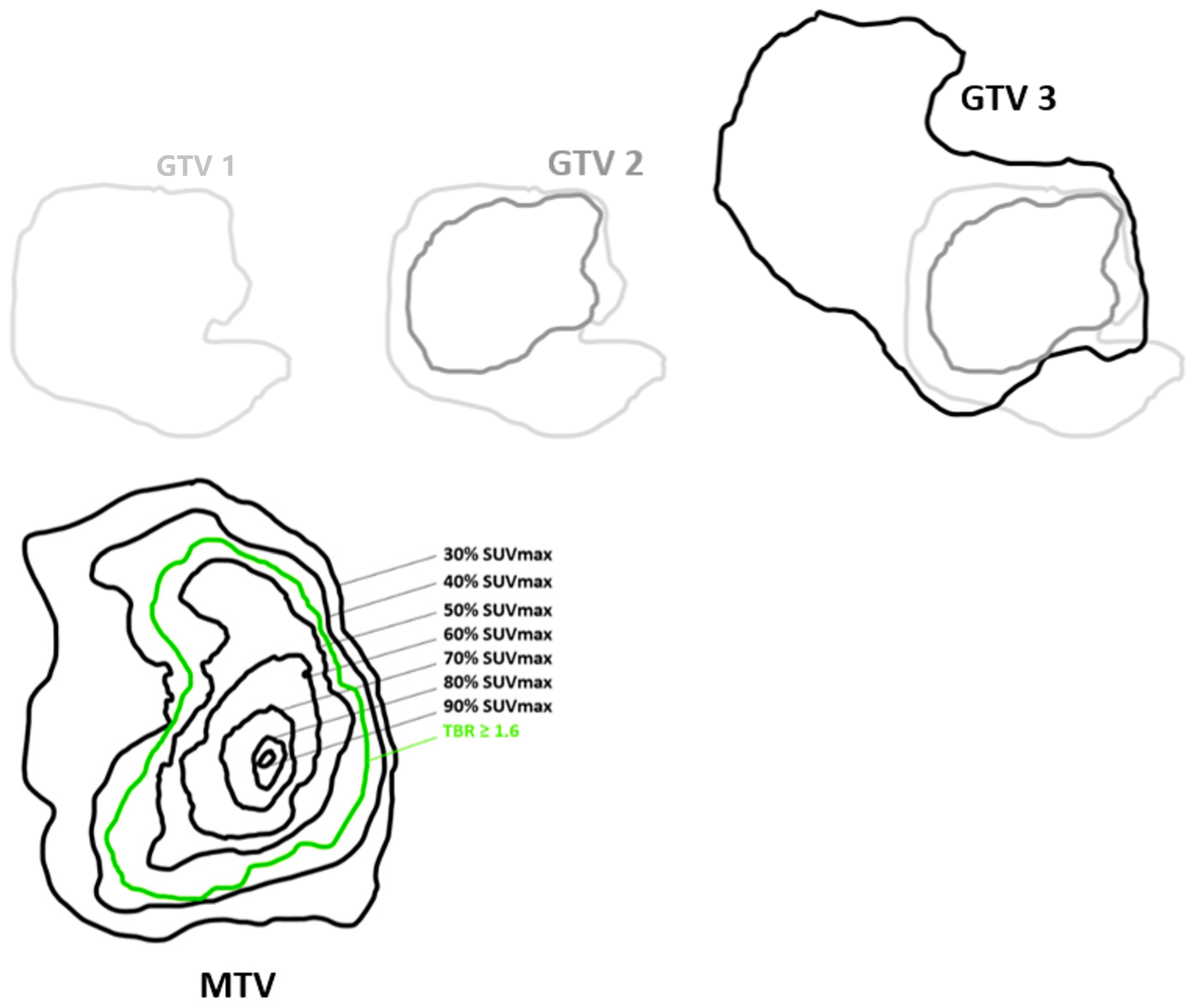
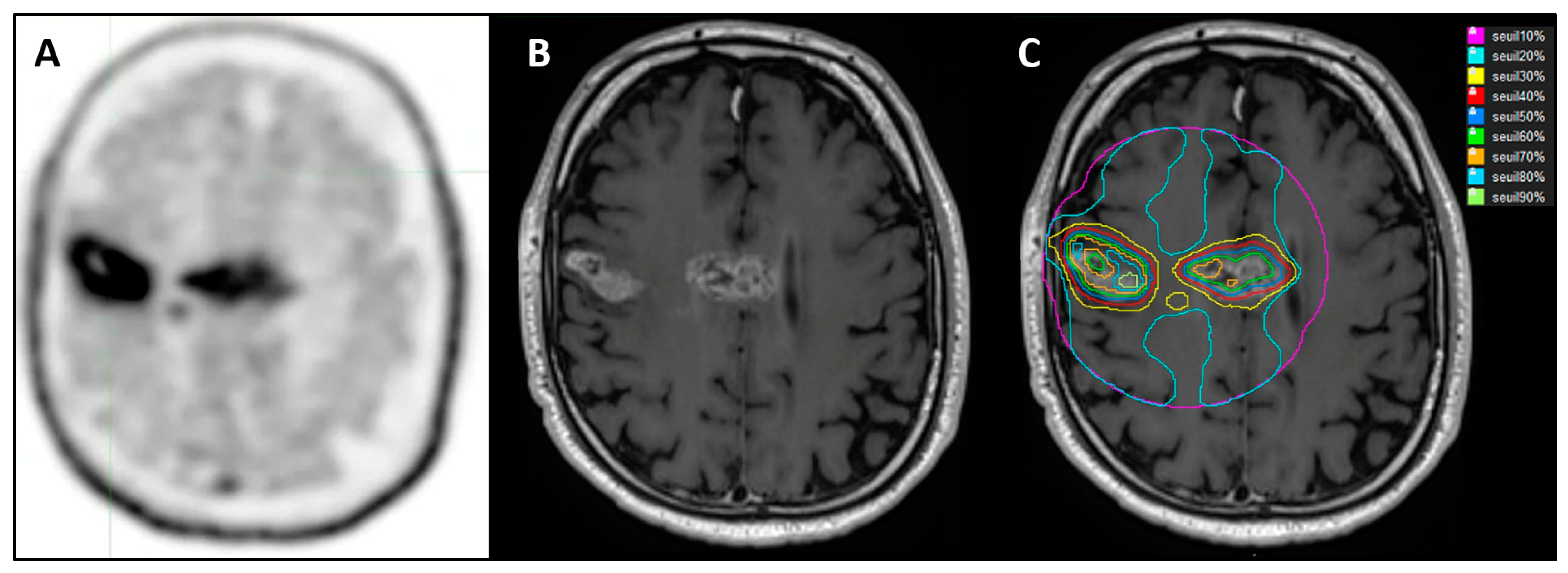
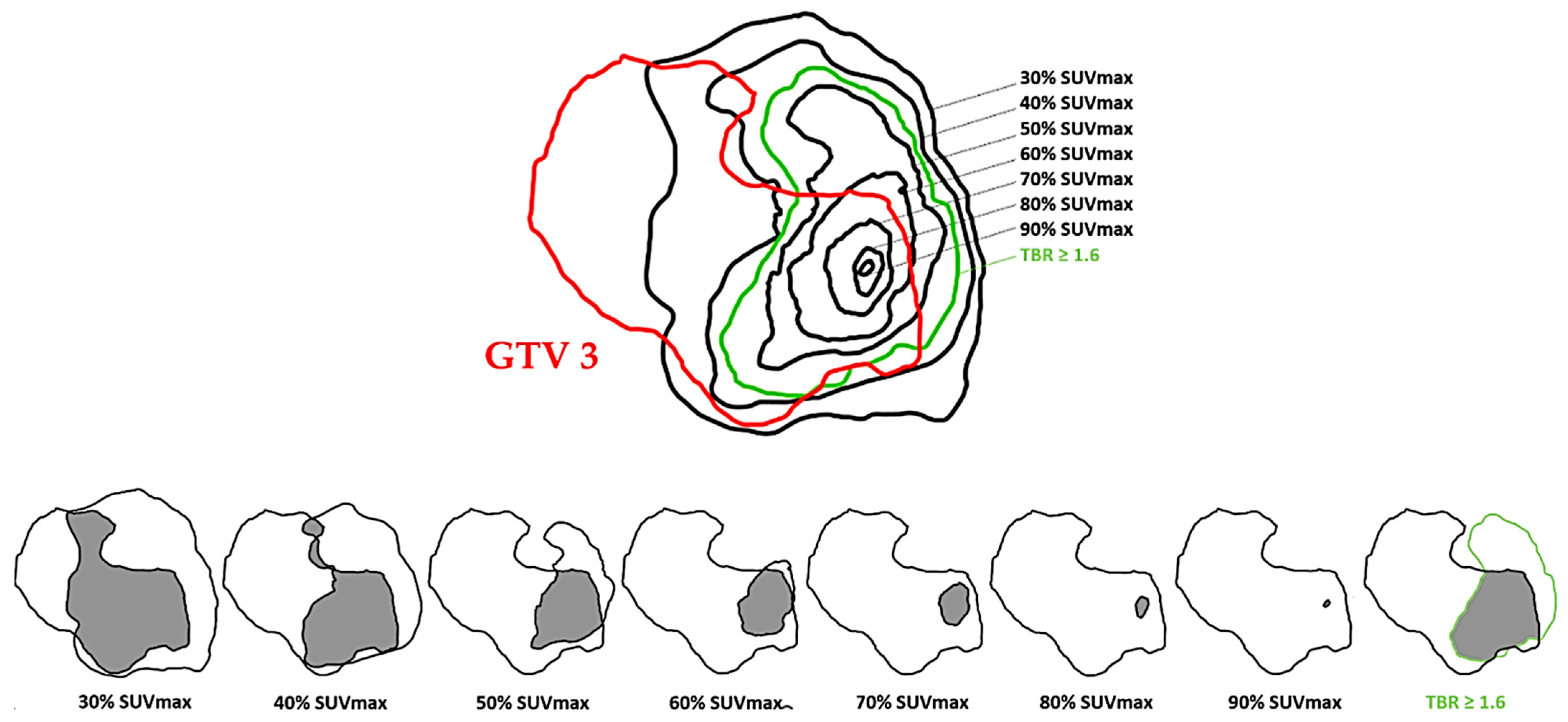
2.4. Target Volume Delineation on FET PET
2.5. Co-Registration
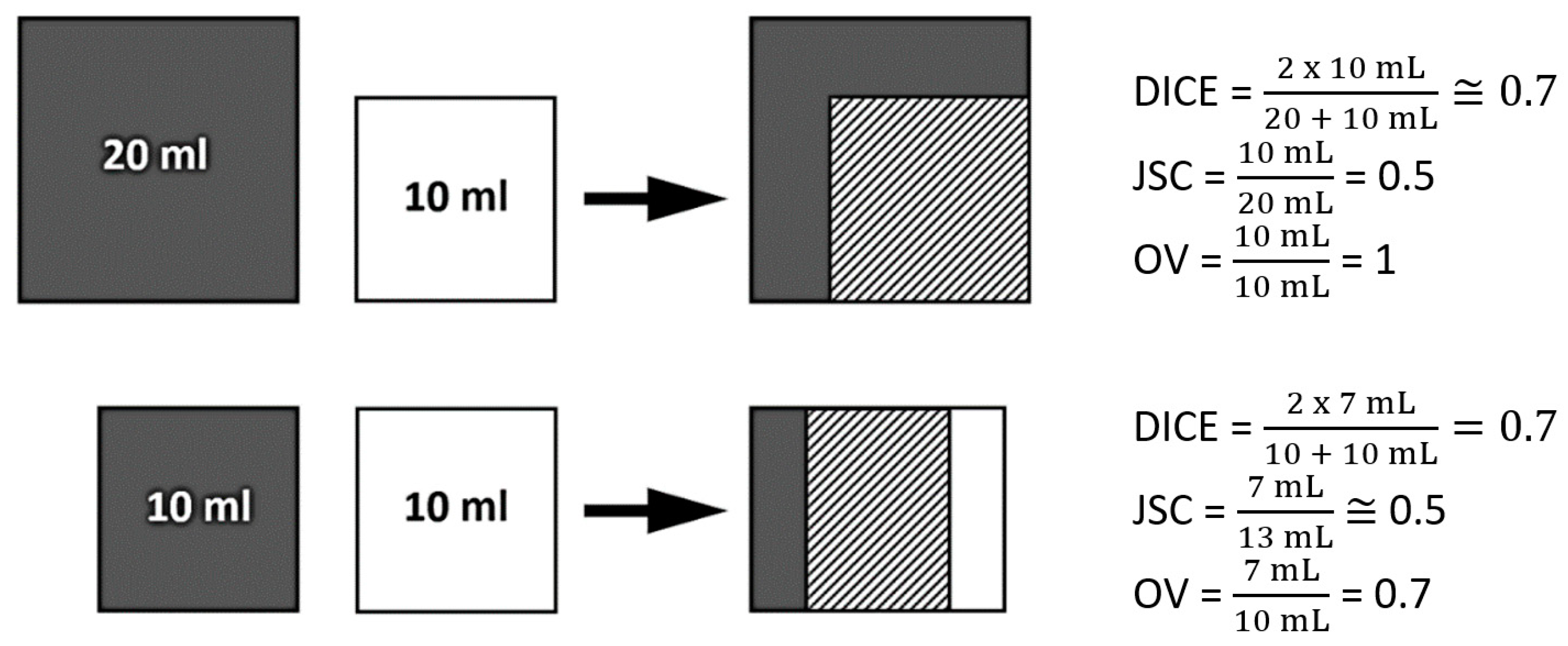
2.6. Spatial Similarity Coefficients
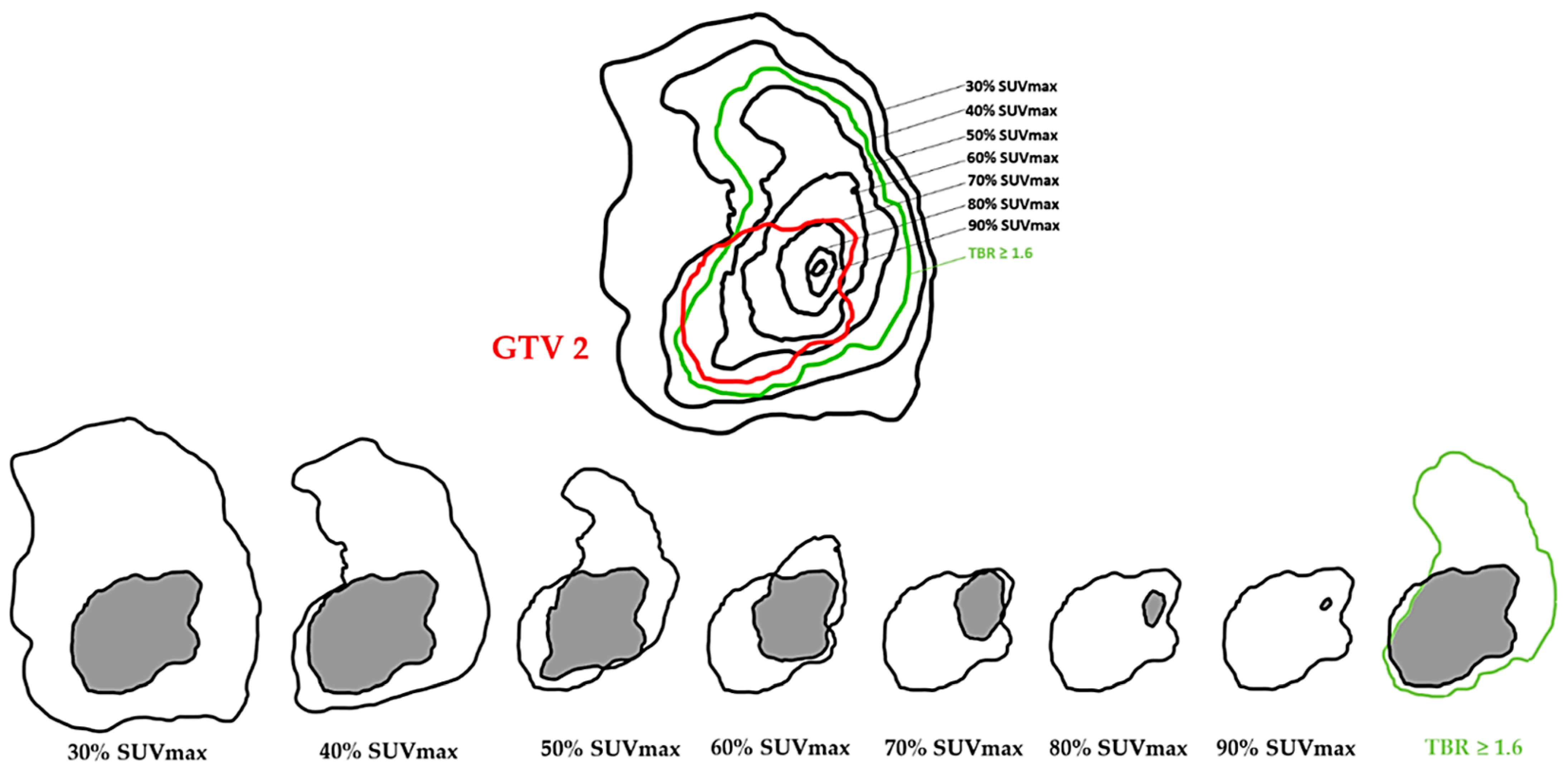
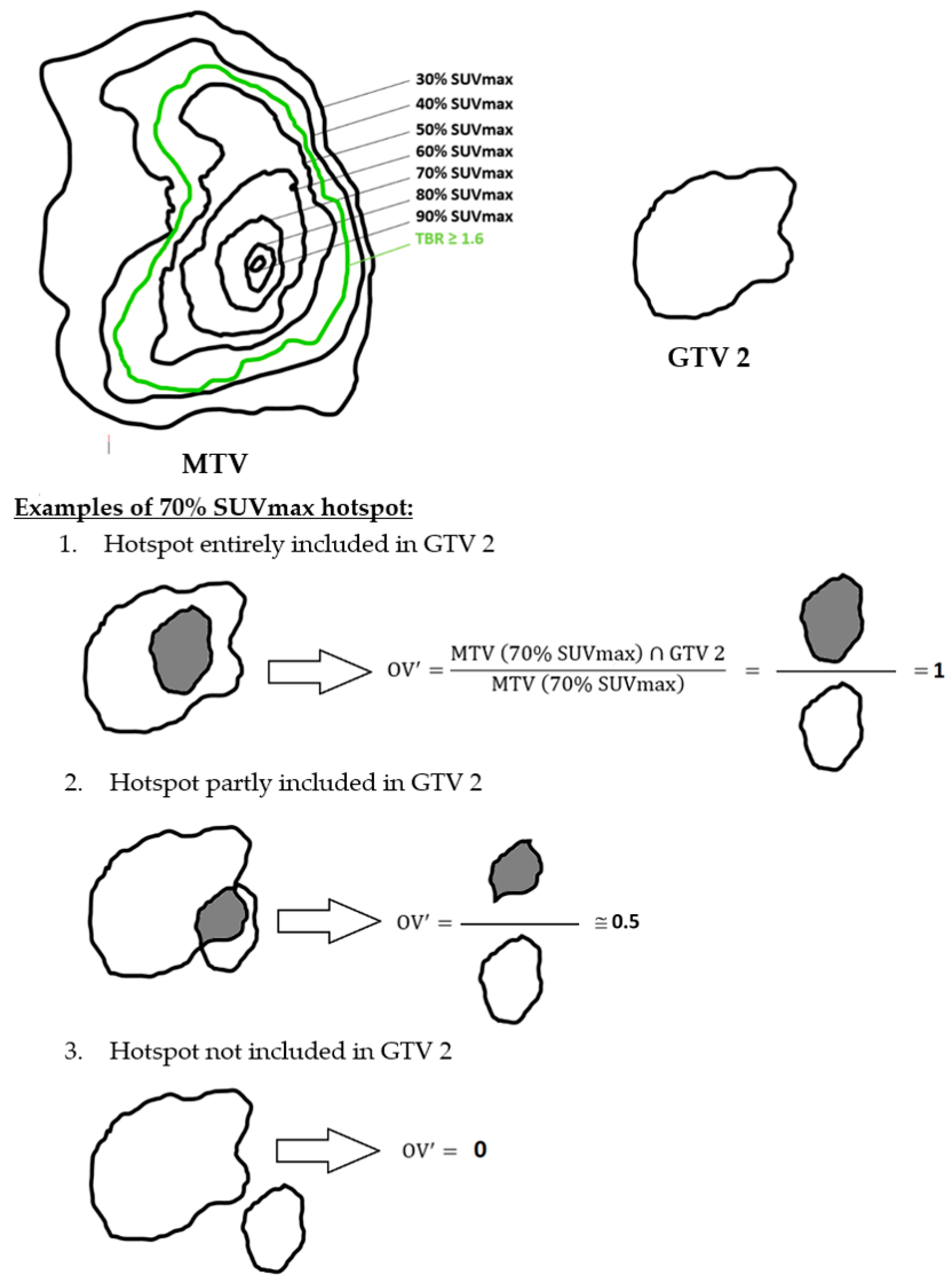
2.7. Hotspot Concept
2.8. Statistical Test
3. Results
3.1. Patient Characteristics
3.2. Impact of Radio-Chemotherapy
3.3. Spatial Similarity between PET (MTV) and MRI Tumor Volumes (GTV)
3.4. Hotspot Concept
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Woehrer, A.; Bauchet, L.; Barnholtz-Sloan, J.S. Glioblastoma survival: Has it improved? Evidence from population-based studies. Curr. Opin. Neurol. 2014, 27, 666–674. [Google Scholar] [CrossRef] [PubMed]
- Ostrom, Q.T.; Cioffi, G.; Waite, K.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2014–2018. Neuro Oncol. 2021, 23, iii1–iii105. [Google Scholar] [CrossRef]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.B.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, K.D.; Ostrom, Q.T.; Kruchko, C.; Patil, N.; Tihan, T.; Cioffi, G.; Fuchs, H.E.; Waite, K.A.; Jemal, A.; Siegel, R.L.; et al. Brain and other central nervous system tumor statistics, 2021. CA Cancer J. Clin. 2021, 71, 381–406. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, Y.R.; Li, X.A.; el Naqa, I.; Hahn, C.A.; Marks, L.B.; Merchant, T.E.; Dicker, A.P. Radiation dose-volume effects in the brain. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, S20–S27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minniti, G.; Amelio, D.; Amichetti, M.; Salvati, M.; Muni, R.; Bozzao, A.; Lanzetta, G.; Scarpino, S.; Arcella, A.; Enrici, R.M. Patterns of failure and comparison of different target volume delineations in patients with glioblastoma treated with conformal radiotherapy plus concomitant and adjuvant temozolomide. Radiother. Oncol. 2010, 97, 377–381. [Google Scholar] [CrossRef]
- Tanaka, M.; Ino, Y.; Nakagawa, K.; Tago, M.; Todo, T. High-dose conformal radiotherapy for supratentorial malignant glioma: A historical comparison. Lancet Oncol. 2005, 6, 953–960. [Google Scholar] [CrossRef]
- Iuchi, T.; Hatano, K.; Narita, Y.; Kodama, T.; Yamaki, T.; Osato, K. Hypofractionated high-dose irradiation for the treatment of malignant astrocytomas using simultaneous integrated boost technique by IMRT. Int. J. Radiat. Oncol. Biol. Phys. 2006, 64, 1317–1324. [Google Scholar] [CrossRef]
- Fitzek, M.M.; Thornton, A.F.; Rabinov, J.D.; Lev, M.H.; Pardo, F.S.; Munzenrider, J.E.; Okunieff, P.; Bussière, M.; Braun, I.; Hochberg, F.H.; et al. Accelerated fractionated proton/photon irradiation to 90 cobalt gray equivalent for glioblastoma multiforme: Results of a phase II prospective trial. J. Neurosurg. 1999, 91, 251–260. [Google Scholar] [CrossRef] [Green Version]
- Shieh, L.-T.; Guo, H.-R.; Ho, C.-H.; Lin, L.-C.; Chang, C.-H.; Ho, S.-Y. Survival of glioblastoma treated with a moderately escalated radiation dose-Results of a retrospective analysis. PLoS ONE 2020, 15, e0233188. [Google Scholar] [CrossRef]
- Laack, N.N.; Pafundi, D.; Anderson, S.K.; Kaufmann, T.; Lowe, V.; Hunt, C.; Vogen, D.; Yan, E.; Sarkaria, J.; Brown, P.; et al. Initial Results of a Phase 2 Trial of 18F-DOPA PET-Guided Dose-Escalated Radiation Therapy for Glioblastoma. Int. J. Radiat. Oncol. Biol. Phys. 2021, 110, 1383–1395. [Google Scholar] [CrossRef] [PubMed]
- Miwa, K.; Matsuo, M.; Ogawa, S.; Shinoda, J.; Asano, Y.; Ito, T.; Yokoyama, K.; Yamada, J.; Yano, H.; Iwama, T. Hypofractionated High-Dose Irradiation with Positron Emission Tomography Data for the Treatment of Glioblastoma Multiforme. Biomed. Res. Int. 2014, 2014, 407026. [Google Scholar] [CrossRef] [Green Version]
- Matsuda, M.; Yamamoto, T.; Ishikawa, E.; Nakai, K.; Zaboronok, A.; Takano, S.; Matsumura, A. Prognostic factors in glioblastoma multiforme patients receiving high-dose particle radiotherapy or conventional radiotherapy. Br. J. Radiol. 2011, 84, S54–S60. [Google Scholar] [CrossRef] [Green Version]
- Claes, A.; Idema, A.J.; Wesseling, P. Diffuse glioma growth: A guerilla war. Acta Neuropathol. 2007, 114, 443–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abgral, R.; Bourhis, D.; Calais, J.; Lucia, F.; Leclère, J.-C.; Salaün, P.-Y.; Vera, P.; Schick, U. Correlation between fluorodeoxyglucose hotspots on preradiotherapy PET/CT and areas of cancer local relapse: Systematic review of literature. Cancer Radiother. 2020, 24, 444–452. [Google Scholar] [CrossRef] [PubMed]
- Langen, K.-J.; Hamacher, K.; Weckesser, M.; Floeth, F.; Stoffels, G.; Bauer, D.; Coenen, H.H.; Pauleit, D. O-(2-[18F]fluoroethyl)-L-tyrosine: Uptake mechanisms and clinical applications. Nucl. Med. Biol. 2006, 33, 287–294. [Google Scholar] [CrossRef]
- Verger, A.; Arbizu, J.; Law, I. Role of amino-acid PET in high-grade gliomas: Limitations and perspectives. Q. J. Nucl. Med. Mol. Imaging 2018, 62, 254–266. [Google Scholar] [CrossRef]
- Galldiks, N.; Law, I.; Pope, W.B.; Arbizu, J.; Langen, K.-J. The use of amino acid PET and conventional MRI for monitoring of brain tumor therapy. Neuroimage Clin. 2017, 13, 386–394. [Google Scholar] [CrossRef] [Green Version]
- Langen, K.-J.; Stoffels, G.; Filss, C.; Heinzel, A.; Stegmayr, C.; Lohmann, P.; Willuweit, A.; Neumaier, B.; Mottaghy, F.M.; Galldiks, N. Imaging of amino acid transport in brain tumours: Positron emission tomography with O-(2-[18F]fluoroethyl)-L-tyrosine (FET). Methods 2017, 130, 124–134. [Google Scholar] [CrossRef]
- Dissaux, G.; Dissaux, B.; Kabbaj, O.E.; Gujral, D.M.; Pradier, O.; Salaün, P.-Y.; Seizeur, R.; Bourhis, D.; Ben Salem, D.; Querellou, S.; et al. Radiotherapy target volume definition in newly diagnosed high grade glioma using 18F-FET PET imaging and multiparametric perfusion MRI: A prospective study (IMAGG). Radiother. Oncol. 2020, 150, 164–171. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestler, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, P.Y.; Macdonald, D.R.; Reardon, D.A.; Cloughesy, T.F.; Sorensen, A.G.; Galanis, E.; Degroot, J.; Wick, W.; Gilbert, M.R.; Lassman, A.B.; et al. Updated response assessment criteria for high-grade gliomas: Response assessment in neuro-oncology working group. J. Clin. Oncol. 2010, 28, 1963–1972. [Google Scholar] [CrossRef] [PubMed]
- Law, I.; Albert, N.L.; Arbizu, J.; Boellaard, R.; Drzezga, A.; Galldiks, N.; la Fougère, C.; Langen, K.-J.; Lopci, E.; Lowe, V.; et al. Joint EANM/EANO/RANO practice guidelines/SNMMI procedure standards for imaging of gliomas using PET with radiolabelled amino acids and [18F]FDG: Version 1.0. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 540–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pauleit, D.; Floeth, F.; Hamacher, K.; Riemenschneider, M.J.; Reifenberger, G.; Müller, H.-W.; Zilles, K.; Coenen, H.H.; Langen, K.-J. O-(2-[18F]fluoroethyl)-L-tyrosine PET combined with MRI improves the diagnostic assessment of cerebral gliomas. Brain 2005, 128, 678–687. [Google Scholar] [CrossRef] [Green Version]
- Unterrainer, M.; Vettermann, F.; Brendel, M.; Holzgreve, A.; Lifschitz, M.; Zähringer, M.; Suchorska, B.; Wenter, V.; Illigens, B.M.; Bartenstein, P.; et al. Towards standardization of 18F-FET PET imaging: Do we need a consistent method of background activity assessment? EJNMMI Res. 2017, 7, 48. [Google Scholar] [CrossRef]
- Nelson, A.; Duchateau, M.; Piper, J.; Verellen, D.; Ridder, M.D. SU-E-J-198: Evaluation of a Free-Form Intensity-Based Deformable Registration Method Using the POPI Model. Med. Phys. 2014, 41, 202. [Google Scholar] [CrossRef]
- Hanna, G.G.; Hounsell, A.R.; O’Sullivan, J.M. Geometrical analysis of radiotherapy target volume delineation: A systematic review of reported comparison methods. Clin. Oncol. (R. Coll. Radiol.) 2010, 22, 515–525. [Google Scholar] [CrossRef]
- Lohmann, P.; Stavrinou, P.; Lipke, K.; Bauer, E.K.; Ceccon, G.; Werner, J.-M.; Neumaier, B.; Fink, G.R.; Shah, N.J.; Langen, K.-J.; et al. FET PET reveals considerable spatial differences in tumour burden compared to conventional MRI in newly diagnosed glioblastoma. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 591–602. [Google Scholar] [CrossRef] [Green Version]
- Thureau, S.; Chaumet-Riffaud, P.; Modzelewski, R.; Fernandez, P.; Tessonnier, L.; Vervueren, L.; Cachin, F.; Berriolo-Riedinger, A.; Olivier, P.; Kolesnikov-Gauthier, H.; et al. Interobserver agreement of qualitative analysis and tumor delineation of 18F-fluoromisonidazole and 3′-deoxy-3′-18F-fluorothymidine PET images in lung cancer. J. Nucl. Med. 2013, 54, 1543–1550. [Google Scholar] [CrossRef] [Green Version]
- Jansen, E.P.; Dewit, L.G.; van Herk, M.; Bartelink, H. Target volumes in radiotherapy for high-grade malignant glioma of the brain. Radiother. Oncol. 2000, 56, 151–156. [Google Scholar] [CrossRef]
- Lemée, J.-M.; Clavreul, A.; Aubry, M.; Com, E.; de Tayrac, M.; Eliat, P.-A.; Henry, C.; Rousseau, A.; Mosser, J.; Menei, P. Characterizing the peritumoral brain zone in glioblastoma: A multidisciplinary analysis. J. Neurooncol. 2015, 122, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Stegmayr, C.; Stoffels, G.; Filß, C.; Heinzel, A.; Lohmann, P.; Willuweit, A.; Ermert, J.; Coenen, H.H.; Mottaghy, F.M.; Galldiks, N.; et al. Current trends in the use of O-(2-[18F]fluoroethyl)-L-tyrosine ([18F]FET) in neurooncology. Nucl. Med. Biol. 2021, 92, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Dunet, V.; Pomoni, A.; Hottinger, A.; Nicod-Lalonde, M.; Prior, J.O. Performance of 18F-FET versus 18F-FDG-PET for the diagnosis and grading of brain tumors: Systematic review and meta-analysis. Neuro. Oncol. 2016, 18, 426–434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiepers, C.; Chen, W.; Cloughesy, T.; Dahlbom, M.; Huang, S.-C. 18F-FDOPA kinetics in brain tumors. J. Nucl. Med. 2007, 48, 1651–1661. [Google Scholar] [CrossRef] [Green Version]
- Lapa, C.; Linsenmann, T.; Monoranu, C.M.; Samnick, S.; Buck, A.K.; Bluemel, C.; Czernin, J.; Kessler, A.F.; Homola, G.A.; Ernestus, R.-I.; et al. Comparison of the amino acid tracers 18F-FET and 18F-DOPA in high-grade glioma patients. J. Nucl. Med. 2014, 55, 1611–1616. [Google Scholar] [CrossRef] [Green Version]
- Nioche, C.; Soret, M.; Gontier, E.; Lahutte, M.; Dutertre, G.; Dulou, R.; Capelle, L.; Guillevin, R.; Foehrenbach, H.; Buvat, I. Evaluation of quantitative criteria for glioma grading with static and dynamic 18F-FDopa PET/CT. Clin. Nucl. Med. 2013, 38, 81–87. [Google Scholar] [CrossRef]
- Cicone, F.; Filss, C.P.; Minniti, G.; Rossi-Espagnet, C.; Papa, A.; Scaringi, C.; Galldiks, N.; Bozzao, A.; Shah, N.J.; Scopinaro, F.; et al. Volumetric assessment of recurrent or progressive gliomas: Comparison between F-DOPA PET and perfusion-weighted MRI. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 905–915. [Google Scholar] [CrossRef] [PubMed]
- Suchorska, B.; Jansen, N.L.; Linn, J.; Kretzschmar, H.; Janssen, H.; Eigenbrod, S.; Simon, M.; Pöpperl, G.; Kreth, F.W.; la Fougere, C.; et al. Biological tumor volume in 18FET-PET before radiochemotherapy correlates with survival in GBM. Neurology 2015, 84, 710–719. [Google Scholar] [CrossRef] [Green Version]
- Piroth, M.D.; Galldiks, N.; Pinkawa, M.; Holy, R.; Stoffels, G.; Ermert, J.; Mottaghy, F.M.; Shah, N.J.; Langen, K.-J.; Eble, M.J. Relapse patterns after radiochemotherapy of glioblastoma with FET PET-guided boost irradiation and simulation to optimize radiation target volume. Radiat. Oncol. 2016, 11, 87. [Google Scholar] [CrossRef] [Green Version]
- Girard, A.; Le Reste, P.-J.; Metais, A.; Carsin Nicol, B.; Chiforeanu, D.C.; Bannier, E.; Campillo-Gimenez, B.; Devillers, A.; Palard-Novello, X.; Le Jeune, F. Combining 18F-DOPA PET and MRI with perfusion-weighted imaging improves delineation of high-grade subregions in enhancing and non-enhancing gliomas prior treatment: A biopsy-controlled study. J. Neurooncol. 2021, 155, 287–295. [Google Scholar] [CrossRef]
- Song, S.; Cheng, Y.; Ma, J.; Wang, L.; Dong, C.; Wei, Y.; Xu, G.; An, Y.; Qi, Z.; Lin, Q.; et al. Simultaneous FET-PET and contrast-enhanced MRI based on hybrid PET/MR improves delineation of tumor spatial biodistribution in gliomas: A biopsy validation study. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1458–1467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filss, C.P.; Galldiks, N.; Stoffels, G.; Sabel, M.; Wittsack, H.J.; Turowski, B.; Antoch, G.; Zhang, K.; Fink, G.R.; Coenen, H.H.; et al. Comparison of 18F-FET PET and perfusion-weighted MR imaging: A PET/MR imaging hybrid study in patients with brain tumors. J. Nucl. Med. 2014, 55, 540–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piroth, M.D.; Holy, R.; Pinkawa, M.; Stoffels, G.; Kaiser, H.J.; Galldiks, N.; Herzog, H.; Coenen, H.H.; Eble, M.J.; Langen, K.J. Prognostic impact of postoperative, pre-irradiation (18)F-fluoroethyl-l-tyrosine uptake in glioblastoma patients treated with radiochemotherapy. Radiother. Oncol. 2011, 99, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Lundemann, M.; Munck Af Rosenschöld, P.; Muhic, A.; Larsen, V.A.; Poulsen, H.S.; Engelholm, S.-A.; Andersen, F.L.; Kjær, A.; Larsson, H.B.W.; Law, I.; et al. Feasibility of multi-parametric PET and MRI for prediction of tumour recurrence in patients with glioblastoma. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 603–613. [Google Scholar] [CrossRef]
- Chaput, A.; Calais, J.; Robin, P.; Thureau, S.; Bourhis, D.; Modzelewski, R.; Schick, U.; Vera, P.; Salaün, P.-Y.; Abgral, R. Correlation between fluorodeoxyglucose hotspots on pretreatment positron emission tomography/CT and preferential sites of local relapse after chemoradiotherapy for head and neck squamous cell carcinoma. Head Neck 2017, 39, 1155–1165. [Google Scholar] [CrossRef]
- Truffault, B.; Bourhis, D.; Chaput, A.; Calais, J.; Robin, P.; Le Pennec, R.; Lucia, F.; Leclère, J.-C.; Gujral, D.M.; Vera, P.; et al. Correlation Between FDG Hotspots on Pre-radiotherapy PET/CT and Areas of HNSCC Local Relapse: Impact of Treatment Position and Images Registration Method. Front. Med. 2020, 7, 218. [Google Scholar] [CrossRef]
- Guezennec, C.; Bourhis, D.; Orlhac, F.; Robin, P.; Corre, J.-B.; Delcroix, O.; Gobel, Y.; Schick, U.; Salaün, P.-Y.; Abgral, R. Inter-observer and segmentation method variability of textural analysis in pre-therapeutic FDG PET/CT in head and neck cancer. PLoS ONE 2019, 14, e0214299. [Google Scholar] [CrossRef]
- Dissaux, B.; Mazouz Fatmi, D.; Ognard, J.; Allard, B.; Keromnes, N.; Latreche, A.; Lepeuve, A.; Schick, U.; Bourbonne, V.; Ben Salem, D.; et al. Radiotherapy Target Volume Definition in Newly Diagnosed High-Grade Glioma Using 18F-FET PET Imaging and Multiparametric MRI: An Inter Observer Agreement Study. Tomography 2022, 8, 2030–2041. [Google Scholar] [CrossRef]
- Byun, J.; Kim, Y.-H.; Nam, S.J.; Park, J.E.; Cho, Y.H.; Kim, H.S.; Hong, S.H.; Kim, J.H.; Kim, S.J.; Kim, C.J. Comparison of Survival Outcomes Between Partial Resection and Biopsy for Primary Glioblastoma: A Propensity Score-Matched Study. World Neurosurg. 2019, 121, e858–e866. [Google Scholar] [CrossRef]
- Ellingson, B.M.; Wen, P.Y.; Cloughesy, T.F. Modified Criteria for Radiographic Response Assessment in Glioblastoma Clinical Trials. Neurotherapeutics 2017, 14, 307–320. [Google Scholar] [CrossRef]
- Wen, P.Y.; Chang, S.M.; Van den Bent, M.J.; Vogelbaum, M.A.; Macdonald, D.R.; Lee, E.Q. Response Assessment in Neuro-Oncology Clinical Trials. J. Clin. Oncol. 2017, 35, 2439–2449. [Google Scholar] [CrossRef] [PubMed]
- Smeraldo, A.; Ponsiglione, A.M.; Soricelli, A.; Netti, P.A.; Torino, E. Update on the Use of PET/MRI Contrast Agents and Tracers in Brain Oncology: A Systematic Review. Int. J. Nanomed. 2022, 17, 3343–3359. [Google Scholar] [CrossRef] [PubMed]
- Verger, A.; Filss, C.P.; Lohmann, P.; Stoffels, G.; Sabel, M.; Wittsack, H.J.; Kops, E.R.; Galldiks, N.; Fink, G.R.; Shah, N.J.; et al. Comparison of 18F-FET PET and perfusion-weighted MRI for glioma grading: A hybrid PET/MR study. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 2257–2265. [Google Scholar] [CrossRef]
- Souhami, L.; Seiferheld, W.; Brachman, D.; Podgorsak, E.B.; Werner-Wasik, M.; Lustig, R.; Schultz, C.J.; Sause, W.; Okunieff, P.; Buckner, J.; et al. Randomized comparison of stereotactic radiosurgery followed by conventional radiotherapy with carmustine to conventional radiotherapy with carmustine for patients with glioblastoma multiforme: Report of Radiation Therapy Oncology Group 93-05 protocol. Int. J. Radiat. Oncol. Biol. Phys. 2004, 60, 853–860. [Google Scholar] [CrossRef]
- Chan, J.L.; Lee, S.W.; Fraass, B.A.; Normolle, D.P.; Greenberg, H.S.; Junck, L.R.; Gebarski, S.S.; Sandler, H.M. Survival and failure patterns of high-grade gliomas after three-dimensional conformal radiotherapy. J. Clin. Oncol. 2002, 20, 1635–1642. [Google Scholar] [CrossRef]
- Pafundi, D.H.; Laack, N.N.; Youland, R.S.; Parney, I.F.; Lowe, V.J.; Giannini, C.; Kemp, B.J.; Grams, M.P.; Morris, J.M.; Hoover, J.M.; et al. Biopsy validation of 18F-DOPA PET and biodistribution in gliomas for neurosurgical planning and radiotherapy target delineation: Results of a prospective pilot study. Neuro. Oncol. 2013, 15, 1058–1067. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean/Number | Percentage/ Range | |
|---|---|---|
| Age at diagnosis | 59 | 38–74 |
| Sex | ||
| Male Female | 14 9 | 60.9% 39.1% |
| Cell origin | ||
| Astrocytoma Oligodendroglioma | 23 0 | 100% 0% |
| Histology | ||
| Grade III Grade IV | 3 20 | 13% 87% |
| Neurosurgical intervention before inclusion: | ||
| Total surgery (G2) Subtotal surgery (G2) Partial surgery (G1) Biopsy alone (G1) | 8 3 3 9 | 34.8% 13% 13% 39.1% |
| Time between MRI 1 and MRI 2 | 255 | 71–938 |
| Time between MRI 1 and MRI 3 | 330 | 48–1033 |
| Molecular biology: | ||
| IDH mutation Co-deletion 1p/19q MGMT methylation | 0 0 13 | 0% 0% 57% |
| N° | Age | Gender | Surgery * (Group) | Histology | Ki67 | GTV 1 mL | GTV 2 Ml | Residual tumor (%) | Variation (%) |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 45 | M | 3 (G2) | IV | 20% | 6.6 | 3.8 | 57.6 | −42.4 |
| 2 | 65 | M | 3 (G2) | IV | 0.1% | 21.7 | NA | NA | NA |
| 3 | 56 | M | 1 (G1) | IV | 30% | 23.6 | 2.2 | 9.3 | −90.7 |
| 4 | 70 | M | 0 (G1) | IV | 30% | 53.0 | 51.7 | 97.5 | −2.5 |
| 5 | 49 | M | 0 (G1) | IV | 20% | 62.5 | NA | NA | NA |
| 6 | 70 | F | 3 (G2) | IV | 15% | 11.4 | 5.4 | 47,4 | −52.6 |
| 7 | 57 | F | 2 (G2) | IV | 30% | 3.0 | 0.1 | 3.3 | −96.7 |
| 8 | 63 | M | 3 (G2) | IV | 0.7% | 13.7 | 12.1 | 88.3 | −11.7 |
| 9 | 70 | M | 0 (G1) | IV | 20% | 38.8 | NA | NA | NA |
| 10 | 64 | M | 1 (G1) | III | 10% | 0.9 | 0.95 | 105.6 | +5.6 |
| 11 | 61 | F | 3 (G2) | IV | 0.3% | 6.4 | 0.1 | 1.6 | −98.4 |
| 12 | 74 | M | 0 (G1) | IV | 20% | 18.6 | 5.4 | 29.0 | −71.0 |
| 13 | 53 | F | 3 (G2) | IV | 5% | 5.9 | 3.1 | 52.5 | −47.5 |
| 14 | 61 | F | 3 (G2) | IV | 20% | 10.5 | 21.0 | 200.0 | +100.0 |
| 15 | 64 | M | 0 (G1) | IV | 10% | 31.6 | 32.3 | 102.2 | +2.2 |
| 16 | 47 | F | 3 (G2) | IV | 15% | 0.5 | 0.3 | 60.0 | −40.0 |
| 17 | 44 | M | 1 (G1) | IV | 0.2% | 2.0 | NA | NA | NA |
| 18 | 49 | M | 0 (G1) | III | 20% | 37.9 | 26.0 | 68.6 | −31.4 |
| 19 | 68 | M | 0 (G1) | IV | 10% | 7.5 | 8.5 | 113.3 | +13.3 |
| 20 | 38 | M | 2 (G2) | IV | 30% | 6.5 | 10.1 | 155.4 | +55.4 |
| 21 | 63 | F | 2 (G2) | IV | 60% | 16.5 | 1.1 | 6.7 | −93.3 |
| 22 | 58 | F | 0 (G1) | III | 35% | 1.4 | NA | NA | NA |
| 23 | 69 | F | 0 (G1) | IV | 40% | 38.7 | 37.3 | 96.4 | −3.6 |
| G1 = Biopsy or Partial Surgery (n = 8) | G2 = Total or Subtotal Surgery (n = 10) | Difference between G1 and G2 (p=) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| DICE | JSC | OV | DICE | JSC | OV | DICE | JSC | OV | |
| 30% SUVmax | 0.362 | 0.243 | 0.781 | 0.138 | 0.079 | 0.684 | 0.01 * | 0.008 * | 0.223 |
| 40% SUVmax | 0.397 | 0.270 | 0.722 | 0.173 | 0.103 | 0.570 | 0.015 * | 0.013 * | 0.120 |
| 50% SUVmax | 0.368 | 0.246 | 0.676 | 0.193 | 0.125 | 0.462 | 0.057 | 0.076 | 0.047 * |
| 60% SUVmax | 0.288 | 0.181 | 0.632 | 0.176 | 0.114 | 0.358 | 0.131 | 0.188 | 0.028 * |
| 70% SUVmax | 0.196 | 0.114 | 0.596 | 0.136 | 0.083 | 0.344 | 0.225 | 0.270 | 0.051 |
| 80% SUVmax | 0.114 | 0.068 | 0.592 | 0.100 | 0.060 | 0.325 | 0.428 | 0.432 | 0.059 |
| 90% SUVmax | 0.032 | 0.026 | 0.670 | 0.019 | 0.017 | 0.379 | 0.644 | 0.658 | 0.068 |
| TBR ≥ 1.6 | 0.418 | 0.287 | 0.735 | 0.207 | 0.127 | 0.477 | 0.024 * | 0.019 * | 0.012 * |
| G1 = Biopsy or Partial Surgery (n = 10) | G2 = Total or Subtotal Surgery (n = 7) | Difference between G1 and G2 (p=) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| DICE | JSC | OV | DICE | JSC | OV | DICE | JSC | OV | |
| 30% SUVmax | 0.465 | 0.321 | 0.755 | 0.215 | 0.132 | 0.551 | 0.009 * | 0.010 * | 0.046 * |
| 40% SUVmax | 0.483 | 0.331 | 0.707 | 0.199 | 0.126 | 0.451 | 0.004 * | 0.006 * | 0.019 * |
| 50% SUVmax | 0.445 | 0.300 | 0.670 | 0.173 | 0.112 | 0.400 | 0.006 * | 0.012 * | 0.022 * |
| 60% SUVmax | 0.338 | 0.213 | 0.670 | 0.141 | 0.087 | 0.370 | 0.018 * | 0.028 * | 0.021 * |
| 70% SUVmax | 0.196 | 0.113 | 0.701 | 0.105 | 0.061 | 0.353 | 0.094 | 0.113 | 0.012 * |
| 80% SUVmax | 0.078 | 0.045 | 0.717 | 0.078 | 0.042 | 0.362 | 0.503 | 0.545 | 0.016 * |
| 90% SUVmax | 0.019 | 0.010 | 0.681 | 0.018 | 0.009 | 0.367 | 0.470 | 0.473 | 0.061 |
| TBR ≥ 1.6 | 0.488 | 0.339 | 0.757 | 0.233 | 0.144 | 0.434 | 0.008 * | 0.007 * | 0.003 * |
| OV’ (MTV; GTV 2) | OV’ (MTV; GTV 3) | |||||
|---|---|---|---|---|---|---|
| G1 (n = 8) | G2 (n = 10) | Difference (p=) | G1 (n = 10) | G2 (n = 7) | Difference (p=) | |
| 30% SUVmax | 0.31 | 0.09 | 0.019 * | 0.41 | 0.17 | 0.017 * |
| 40% SUVmax | 0.4 | 0.14 | 0.014 * | 0.51 | 0.21 | 0.007 * |
| 50% SUVmax | 0.46 | 0.19 | 0.021 * | 0.60 | 0.24 | 0.004 * |
| 60% SUVmax | 0.5 | 0.23 | 0.034 * | 0.66 | 0.25 | 0.003 * |
| 70% SUVmax | 0.54 | 0.26 | 0.043 * | 0.70 | 0.28 | 0.003 * |
| 80% SUVmax | 0.59 | 0.31 | 0.053 | 0.72 | 0.35 | 0.014 * |
| 90% SUVmax | 0.67 | 0.38 | 0.068 | 0.68 | 0.37 | 0.061 |
| TBR ≥ 1.6 | 0.33 | 0.153 | 0.027 * | 0.41 | 0.21 | 0.022 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Allard, B.; Dissaux, B.; Bourhis, D.; Dissaux, G.; Schick, U.; Salaün, P.-Y.; Abgral, R.; Querellou, S. Hotspot on 18F-FET PET/CT to Predict Aggressive Tumor Areas for Radiotherapy Dose Escalation Guiding in High-Grade Glioma. Cancers 2023, 15, 98. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15010098
Allard B, Dissaux B, Bourhis D, Dissaux G, Schick U, Salaün P-Y, Abgral R, Querellou S. Hotspot on 18F-FET PET/CT to Predict Aggressive Tumor Areas for Radiotherapy Dose Escalation Guiding in High-Grade Glioma. Cancers. 2023; 15(1):98. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15010098
Chicago/Turabian StyleAllard, Bastien, Brieg Dissaux, David Bourhis, Gurvan Dissaux, Ulrike Schick, Pierre-Yves Salaün, Ronan Abgral, and Solène Querellou. 2023. "Hotspot on 18F-FET PET/CT to Predict Aggressive Tumor Areas for Radiotherapy Dose Escalation Guiding in High-Grade Glioma" Cancers 15, no. 1: 98. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15010098