
The Surgical and Therapeutic Activities of Non-Functional Pancreatic Neuroendocrine Tumors at a High-Volume Institution
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
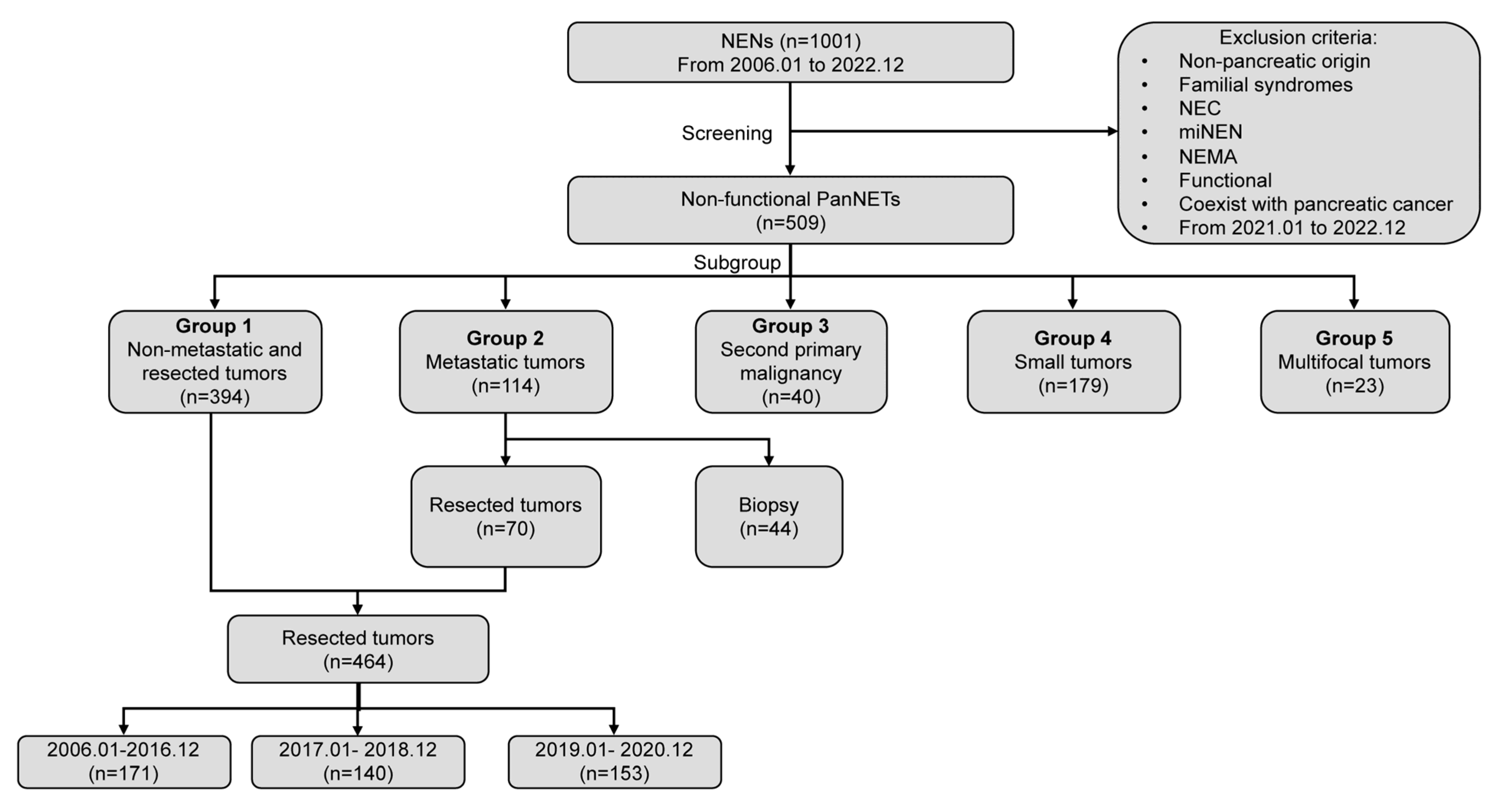
2.1. Patient Population
2.2. Statistical Analyses
3. Results
3.1. Patient Characteristics and Surgical Activities
3.2. Time Trends Analysis
3.3. Non-Metastatic and Resected Tumors
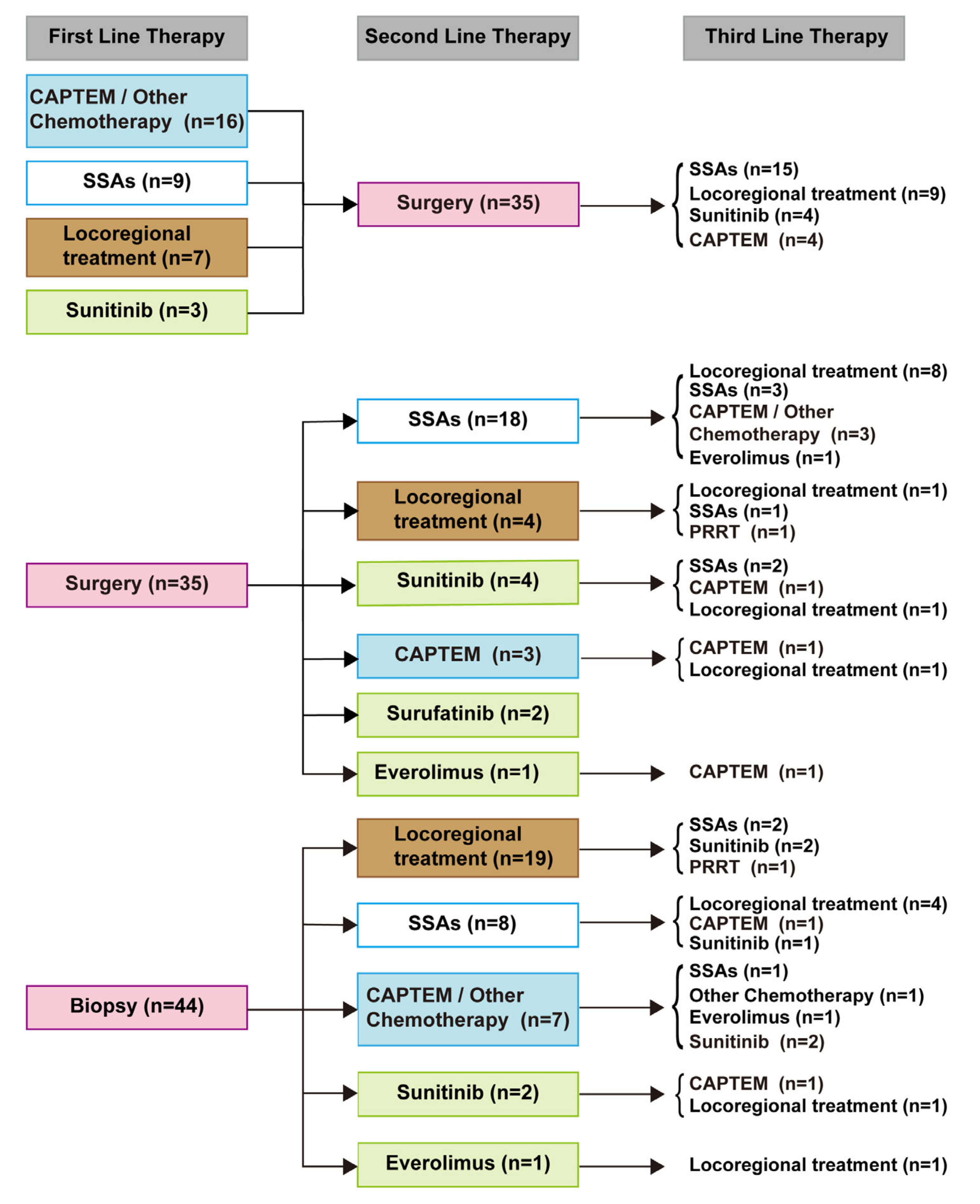
3.4. Metastatic Tumors
3.5. Tumors with Second Primary Malignancy
3.6. Small Tumors ≤2 cm
3.7. Multifocal Tumors
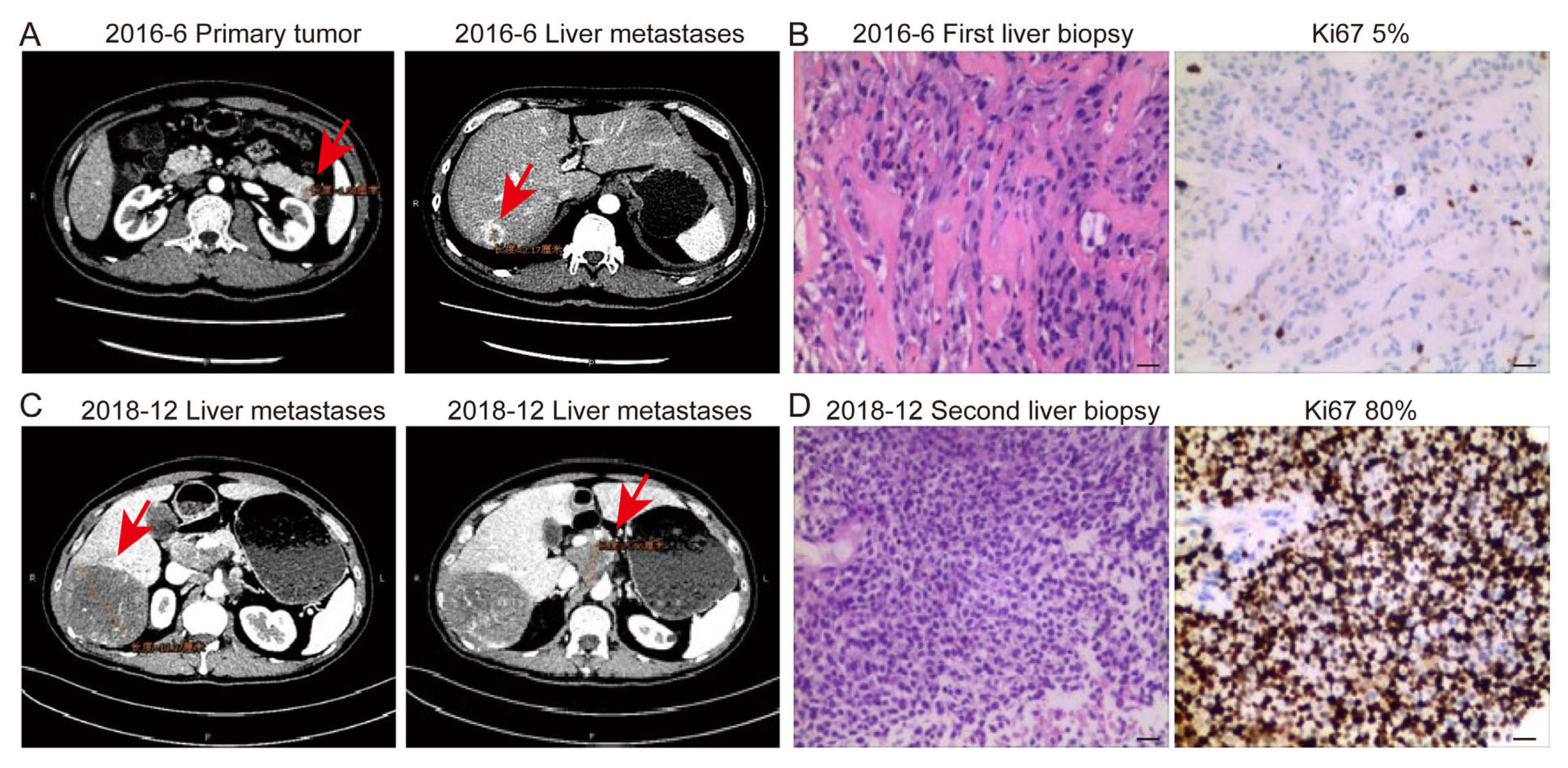
3.8. Transformation from NET to NEC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients With Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Masui, T.; Ito, T.; Komoto, I.; Uemoto, S.; Group, J.P.S. Recent epidemiology of patients with gastro-entero-pancreatic neuroendocrine neoplasms (GEP-NEN) in Japan: A population-based study. BMC Cancer 2020, 20, 1104. [Google Scholar] [CrossRef]
- Zhang, W.H.; Wang, W.Q.; Gao, H.L.; Xu, S.S.; Li, S.; Li, T.J.; Han, X.; Xu, H.X.; Li, H.; Jiang, W.; et al. Tumor-Infiltrating Neutrophils Predict Poor Survival of Non-Functional Pancreatic Neuroendocrine Tumor. J. Clin. Endocrinol. Metab. 2020, 105, 2217–2228. [Google Scholar] [CrossRef]
- Cloyd, J.M.; Poultsides, G.A. Non-functional neuroendocrine tumors of the pancreas: Advances in diagnosis and management. World J. Gastroenterol. 2015, 21, 9512–9525. [Google Scholar] [CrossRef] [PubMed]
- Paik, W.H.; Lee, K.J. Management of Small Nonfunctioning Pancreatic Neuroendocrine Neoplasms: Current Opinion and Controversies. J. Clin. Med. 2023, 12, 251. [Google Scholar] [CrossRef]
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®): Neuroendocrine and Adrenal Tumor, Version 2.2022. Available online: https://www.nccn.org/guidelines (accessed on 29 January 2023).
- Falconi, M.; Eriksson, B.; Kaltsas, G.; Bartsch, D.K.; Capdevila, J.; Caplin, M.; Kos-Kudla, B.; Kwekkeboom, D.; Rindi, G.; Klöppel, G.; et al. ENETS Consensus Guidelines Update for the Management of Patients with Functional Pancreatic Neuroendocrine Tumors and Non-Functional Pancreatic Neuroendocrine Tumors. Neuroendocrinology 2016, 103, 153–171. [Google Scholar] [CrossRef] [Green Version]
- Howe, J.R.; Merchant, N.B.; Conrad, C.; Keutgen, X.M.; Hallet, J.; Drebin, J.A.; Minter, R.M.; Lairmore, T.C.; Tseng, J.F.; Zeh, H.J.; et al. The North American Neuroendocrine Tumor Society Consensus Paper on the Surgical Management of Pancreatic Neuroendocrine Tumors. Pancreas 2020, 49, 1–33. [Google Scholar] [CrossRef] [PubMed]
- Pavel, M.; Öberg, K.; Falconi, M.; Krenning, E.P.; Sundin, A.; Perren, A.; Berruti, A. Gastroenteropancreatic neuroendocrine neoplasms: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 844–860. [Google Scholar] [CrossRef]
- Sharpe, S.M.; In, H.; Winchester, D.J.; Talamonti, M.S.; Baker, M.S. Surgical resection provides an overall survival benefit for patients with small pancreatic neuroendocrine tumors. J. Gastrointest. Surg. 2015, 19, 117–123, discussion 123. [Google Scholar] [CrossRef] [PubMed]
- Gratian, L.; Pura, J.; Dinan, M.; Roman, S.; Reed, S.; Sosa, J.A. Impact of extent of surgery on survival in patients with small nonfunctional pancreatic neuroendocrine tumors in the United States. Ann. Surg. Oncol. 2014, 21, 3515–3521. [Google Scholar] [CrossRef] [Green Version]
- Nanno, Y.; Toyama, H.; Matsumoto, I.; Uemura, J.; Asari, S.; Goto, T.; Lee, D.; Murakami, T.; Komatsu, S.; Yanagimoto, H.; et al. Reappraisal of Malignant Risk Assessment for Small (</=20 mm) Non-functioning Pancreatic Neuroendocrine Tumors. Ann. Surg. Oncol. 2023, online ahead of print. [CrossRef]
- Williams, J.K.; Schwarz, J.L.; Keutgen, X.M. Surgery for metastatic pancreatic neuroendocrine tumors: A narrative review. Hepatobiliary Surg. Nutr. 2023, 12, 69–83. [Google Scholar] [CrossRef] [PubMed]
- Ngongoni, R.; Visser, B. Surgery, Liver Directed Therapy and Peptide Receptor Radionuclide Therapy for Pancreatic Neuroendocrine Tumor Liver Metastases. Cancers 2022, 14, 5103. [Google Scholar] [CrossRef] [PubMed]
- Scott, A.T.; Breheny, P.J.; Keck, K.J.; Bellizzi, A.M.; Dillon, J.S.; O’Dorisio, T.M.; Howe, J.R. Effective cytoreduction can be achieved in patients with numerous neuroendocrine tumor liver metastases (NETLMs). Surgery 2019, 165, 166–175. [Google Scholar] [CrossRef]
- Rindi, G.; Klöppel, G.; Alhman, H.; Caplin, M.; Couvelard, A.; de Herder, W.W.; Erikssson, B.; Falchetti, A.; Falconi, M.; Komminoth, P.; et al. TNM staging of foregut (neuro)endocrine tumors: A consensus proposal including a grading system. Virchows Arch. 2006, 449, 395–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kloppel, G.; La Rosa, S. Ki67 labeling index: Assessment and prognostic role in gastroenteropancreatic neuroendocrine neoplasms. Virchows Arch. 2018, 472, 341–349. [Google Scholar] [CrossRef]
- Rindi, G.; Wiedenmann, B. Neuroendocrine neoplasms of the gut and pancreas: New insights. Nat. Rev. Endocrinol. 2011, 8, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Edge, S.B.; Byrd, D.R.; Compton, C.C.; Fritz, A.G.; Greene, F.L.; Trotti, A. AJCC Cancer Staging Manual, 7th ed.; Springer: Berlin/Heidelberg, Germany, 2010. [Google Scholar]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer: Cham, Switzerland, 2017. [Google Scholar]
- Zhang, W.H.; Gao, H.L.; Liu, W.S.; Qin, Y.; Ye, Z.; Lou, X.; Wang, F.; Zhang, Y.; Chen, X.M.; Chen, J.; et al. A real-life treatment cohort of pancreatic neuroendocrine tumors: High-grade increase in metastases confers poor survival. Front. Endocrinol. 2022, 13, 941210. [Google Scholar] [CrossRef] [PubMed]
- Landoni, L.; Marchegiani, G.; Pollini, T.; Cingarlini, S.; D’Onofrio, M.; Capelli, P.; De Robertis, R.; Davi, M.V.; Amodio, A.; Impellizzeri, H.; et al. The Evolution of Surgical Strategies for Pancreatic Neuroendocrine Tumors (Pan-NENs) Time-trend and Outcome Analysis From 587 Consecutive Resections at a High-volume Institution. Ann. Surg. 2019, 269, 725–732. [Google Scholar] [CrossRef]
- Zheng, J.; Pulvirenti, A.; Javed, A.A.; Michelakos, T.; Paniccia, A.; Lee, K.K.; Ferrone, C.R.; Wei, A.C.; He, J.; Zureikat, A.H.; et al. Minimally Invasive vs Open Pancreatectomy for Pancreatic Neuroendocrine Tumors: Multi-Institutional 10-Year Experience of 1023 Patients. J. Am. Coll. Surg. 2022, 235, 315–330. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Song, K.B.; Hwang, D.W.; Lee, J.H.; Alshammary, S.; Kim, S.C. Time-trend and recurrence analysis of pancreatic neuroendocrine tumors. Endocr. Connect. 2019, 8, 1052–1060. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chouliaras, K.; Newman, N.A.; Shukla, M.; Swett, K.R.; Levine, E.A.; Sham, J.; Mann, G.N.; Shen, P. Analysis of recurrence after the resection of pancreatic neuroendocrine tumors. J. Surg. Oncol. 2018, 118, 416–421. [Google Scholar] [CrossRef]
- Gao, H.; Liu, L.; Wang, W.; Xu, H.; Jin, K.; Wu, C.; Qi, Z.; Zhang, S.; Liu, C.; Xu, J.; et al. Novel recurrence risk stratification of resected pancreatic neuroendocrine tumor. Cancer Lett. 2018, 412, 188–193. [Google Scholar] [CrossRef] [PubMed]
- Dong, D.H.; Zhang, X.F.; Lopez-Aguiar, A.G.; Poultsides, G.; Makris, E.; Rocha, F.; Kanji, Z.; Weber, S.; Fisher, A.; Fields, R.; et al. Resection of pancreatic neuroendocrine tumors: Defining patterns and time course of recurrence. HPB 2020, 22, 215–223. [Google Scholar] [CrossRef]
- Marchegiani, G.; Landoni, L.; Andrianello, S.; Masini, G.; Cingarlini, S.; D’Onofrio, M.; De Robertis, R.; Davì, M.; Capelli, P.; Manfrin, E.; et al. Patterns of Recurrence after Resection for Pancreatic Neuroendocrine Tumors: Who, When, and Where? Neuroendocrinology 2019, 108, 161–171. [Google Scholar] [CrossRef]
- Wang, W.Q.; Zhang, W.H.; Gao, H.L.; Huang, D.; Xu, H.X.; Li, S.; Li, T.J.; Xu, S.S.; Li, H.; Long, J.; et al. A novel risk factor panel predicts early recurrence in resected pancreatic neuroendocrine tumors. J. Gastroenterol. 2021, 56, 395–405. [Google Scholar] [CrossRef] [PubMed]
- Ausania, F.; Senra del Rio, P.; Gomez-Bravo, M.A.; Martin-Perez, E.; Perez-Daga, J.A.; Dorcaratto, D.; Gonzalez-Nicolas, T.; Sanchez-Cabus, S.; Tardio-Baiges, A. Can we predict recurrence in WHO G1-G2 pancreatic neuroendocrine neoplasms? Results from a multi-institutional Spanish study. Pancreatology 2019, 19, 367–371. [Google Scholar] [CrossRef] [PubMed]
- Miller, H.C.; Drymousis, P.; Flora, R.; Goldin, R.; Spalding, D.; Frilling, A. Role of Ki-67 proliferation index in the assessment of patients with neuroendocrine neoplasias regarding the stage of disease. World J. Surg. 2014, 38, 1353–1361. [Google Scholar] [CrossRef] [PubMed]
- Massironi, S.; Campana, D.; Pusceddu, S.; Albertelli, M.; Faggiano, A.; Panzuto, F.; Smiroldo, V.; Andreasi, V.; Rossi, R.E.; Maggio, I.; et al. Second primary neoplasms in patients with lung and gastroenteropancreatic neuroendocrine neoplasms: Data from a retrospective multi-centric study. Dig. Liver Dis. 2021, 53, 367–374. [Google Scholar] [CrossRef]
- Habal, N.; Sims, C.; Bilchik, A.J. Gastrointestinal carcinoid tumors and second primary malignancies. J. Surg. Oncol. 2000, 75, 310–316. [Google Scholar] [CrossRef]
- Finkelstein, P.; Sharma, R.; Picado, O.; Gadde, R.; Stuart, H.; Ripat, C.; Livingstone, A.S.; Sleeman, D.; Merchant, N.; Yakoub, D. Pancreatic Neuroendocrine Tumors (panNETs): Analysis of Overall Survival of Nonsurgical Management Versus Surgical Resection. J. Gastrointest. Surg. 2017, 21, 855–866. [Google Scholar] [CrossRef] [PubMed]
- Kwon, W.; Jang, J.Y.; Song, K.B.; Hwang, D.W.; Kim, S.C.; Heo, J.S.; Choi, D.W.; Hwang, H.K.; Kang, C.M.; Yoon, Y.S.; et al. Risk Factors for Recurrence in Pancreatic Neuroendocrine Tumor and Size as a Surrogate in Determining the Treatment Strategy: A Korean Nationwide Study. Neuroendocrinology 2021, 111, 794–804. [Google Scholar] [CrossRef]
- Partelli, S.; Ramage, J.K.; Massironi, S.; Zerbi, A.; Kim, H.B.; Niccoli, P.; Panzuto, F.; Landoni, L.; Tomazic, A.; Ibrahim, T.; et al. Management of Asymptomatic Sporadic Nonfunctioning Pancreatic Neuroendocrine Neoplasms (ASPEN) ≤2 cm: Study Protocol for a Prospective Observational Study. Front. Med. 2020, 7, 598438. [Google Scholar] [CrossRef]
- Partelli, S.; Massironi, S.; Zerbi, A.; Niccoli, P.; Kwon, W.; Landoni, L.; Panzuto, F.; Tomazic, A.; Bongiovanni, A.; Kaltsas, G.; et al. Management of asymptomatic sporadic non-functioning pancreatic neuroendocrine neoplasms no larger than 2 cm: Interim analysis of prospective ASPEN trial. Br. J. Surg. 2022, 109, 1186–1190. [Google Scholar] [CrossRef] [PubMed]
- Heidsma, C.M.; Engelsman, A.F.; van Dieren, S.; Stommel, M.W.J.; de Hingh, I.; Vriens, M.; Hol, L.; Festen, S.; Mekenkamp, L.; Hoogwater, F.J.H.; et al. Watchful waiting for small non-functional pancreatic neuroendocrine tumours: Nationwide prospective cohort study (PANDORA). Br. J. Surg. 2021, 108, 888–891. [Google Scholar] [CrossRef] [PubMed]
- Pelosi, G.; Bianchi, F.; Dama, E.; Metovic, J.; Barella, M.; Sonzogni, A.; Albini, A.; Papotti, M.; Gong, Y.; Vijayvergia, N. A Subset of Large Cell Neuroendocrine Carcinomas in the Gastroenteropancreatic Tract May Evolve from Pre-existing Well-Differentiated Neuroendocrine Tumors. Endocr. Pathol. 2021, 32, 396–407. [Google Scholar] [CrossRef]
- Yamauchi, Y.; Kodama, Y.; Shiokawa, M.; Kakiuchi, N.; Marui, S.; Kuwada, T.; Sogabe, Y.; Tomono, T.; Mima, A.; Morita, T.; et al. Rb and p53 Execute Distinct Roles in the Development of Pancreatic Neuroendocrine Tumors. Cancer Res. 2020, 80, 3620–3630. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Study Cohort (n = 509) | Group 1 (n = 394) | Group 2 (n = 114) | Group 3 (n = 40) | Group 4 (n = 179) | Group 5 (n = 23) |
|---|---|---|---|---|---|---|
| No. (%) | ||||||
| Gender | ||||||
| Male | 222 (43.6) | 169 (42.9) | 53 (46.5) | 13 (32.5) | 70 (39.1) | 12 (52.2) |
| Female | 287 (56.4) | 225 (57.1) | 61 (53.5) | 27 (67.5) | 109 (60.9) | 11 (47.8) |
| Median Age, years | 54 | 55 | 50.0 | 56.5 | 55.0 | 52.0 |
| Tumor size, cm | ||||||
| Mean (SD) | 3.6 (2.7) | 3.1 (2.4) | 5.4 (3.0) | 3.8 (2.2) | 1.4 (0.4) | 4.1 (3.2) |
| Location | ||||||
| Head | 147 (28.9) | 118 (29.9) | 28 (24.6) | 8 (20.0) | 47 (26.3) | 0 (0.0) |
| Neck | 65 (12.8) | 58 (14.7) | 7 (6.1) | 4 (10.0) | 34 (19.0) | 0 (0.0) |
| Body | 74 (14.5) | 62 (15.7) | 12 (10.5) | 5 (12.5) | 33 (18.4) | 0 (0.0) |
| Tail | 82 (16.1) | 48 (12.2) | 34 (29.8) | 5 (12.5) | 22 (12.3) | 0 (0.0) |
| Body-Tail | 118 (23.2) | 87 (22.1) | 31 (27.2) | 13 (32.2) | 34 (19.0) | 0 (0.0) |
| Multifocal | 23 (4.5) | 21 (5.3) | 2 (1.8) | 5 (12.5) | 9 (5.0) | 23 (100.0) |
| Lymph node positive | n = 470 | n = 76 | n = 176 | n = 22 | ||
| Yes | 98 (20.9) | 55 (14.0) | 43 (56.6) | 9 (22.5) | 12 (6.8) | 6 (27.3) |
| No | 372 (79.1) | 339 (86.0) | 33 (43.4) | 31 (77.5) | 164 (93.2) | 16 (72.7) |
| Perineural invasion | n = 470 | n = 387 | n = 71 | n = 39 | n = 176 | n = 22 |
| Yes | 88 (19.2) | 49 (12.7) | 39 (54.9) | 4 (10.3) | 17 (9.7) | 8 (36.4) |
| No | 370 (80.8) | 338 (87.3) | 32 (45.1) | 35 (89.7) | 159 (90.3) | 14 (63.6) |
| Microvascular invasion | n = 458 | n = 387 | n = 71 | n = 39 | n = 176 | n = 22 |
| Yes | 116 (25.3) | 73 (18.9) | 43 (60.6) | 13 (33.3) | 20 (11.4) | 4 (18.2) |
| No | 342 (74.7) | 314 (81.1) | 28 (39.4) | 26 (66.7) | 156 (88.6) | 18 (81.8) |
| Metastases | n = 114 | n = 5 | n = 11 | n = 2 | ||
| Liver | 111 (97.4) | 0 (0.0) | 111 (97.4) | 5 (100.0) | 11 (100.0) | 2 (100.0) |
| Peritoneum/others | 3 (2.6) | 0 (0.0) | 3 (2.6) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Surgical approach | n = 464 | n = 70 | n = 176 | n = 22 | ||
| Open | 369 (79.5) | 305 (77.4) | 64 (91.4) | 34 (85.0) | 128 (72.7) | 19 (86.4) |
| Minimally invasive | 95 (20.5) | 89 (22.6) | 6 (8.6) | 6 (15.0) | 48 (27.3) | 3 (13.6) |
| Surgical procedure | n = 464 | n = 503 | n = 70 | n = 176 | n = 22 | |
| PD | 141 (30.4) | 129 (32.7) | 12 (17.1) | 12 (30.0) | 52 (29.5) | 8 (36.4) |
| DP | 268 (57.8) | 213 (54.1) | 55 (78.6) | 25 (62.5) | 92 (52.3) | 10 (45.5) |
| TP | 10 (2.2) | 8 (2.0) | 2 (2.9) | 1 (2.5) | 0 (0.0) | 4 (18.2) |
| EN | 36 (7.8) | 35 (8.9) | 1 (1.4) | 1 (2.5) | 26 (14.8) | 0 (0.0) |
| CP | 9 (1.9) | 9 (2.3) | 0 (0.0) | 1 (2.5) | 6 (3.4) | 0 (0.0) |
| Margin status | n = 464 | n = 70 | n = 176 | n = 22 | ||
| R0 | 387 (83.4) | 387 (98.2) | 0 (0.0) | 35 (87.5) | 167 (94.9) | 21 (95.5) |
| R1 | 7 (1.5) | 7 (1.8) | 0 (0.0) | 0 (0.0) | 1 (0.6) | 0 (0.0) |
| R2 | 70 (15.1) | 0 (0.0) | 70 (100.0) | 5 (12.5) | 8 (4.5) | 1 (4.5) |
| AJCC 8th TNM stage | ||||||
| I | 135 (26.5) | 135 (34.3) | 0 (0.0) | 6 (15.0) | 134 (74.9) | 4 (17.4) |
| II | 204 (40.1) | 203 (51.5) | 0 (0.0) | 23 (57.5) | 25 (14.0) | 12 (52.2) |
| III | 56 (11.0) | 56 (14.2) | 0 (0.0) | 6 (15.0) | 9 (5.0) | 5 (21.7) |
| IV | 114 (22.4) | 0 (0.0) | 114 (100.0) | 5 (12.5) | 11 (6.1) | 2 (8.7) |
| WHO classification | ||||||
| G1 | 217 (42.6) | 201 (51.0) | 15 (13.2) | 13 (32.5) | 122 (68.2) | 10 (43.5) |
| G2 | 269 (52.8) | 184 (46.7) | 85 (74.6) | 26 (65.0) | 54 (30.2) | 12 (52.2) |
| G3 | 23 (4.5) | 9 (2.3) | 14 (12.3) | 1 (2.5) | 3 (1.7) | 1 (4.3) |
| Factors | Recurrence-Free Survival | Overall Survival | ||||||
|---|---|---|---|---|---|---|---|---|
| Univariable | Multivariable | Univariable | Multivariable | |||||
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Gender: male vs. female | 0.863 (0.547–1.360) | 0.525 | 1.249 (0.366–4.268) | 0.723 | ||||
| Age: <55 vs. ≥55 years | 1.283 (0.813–2.025) | 0.285 | 1.401 (0.408–4.814) | 0.593 | ||||
| Tumor size: <2.5 vs. ≥2.5 cm | 6.120 (3.142–11.919) | <0.001 | 4.975 (2.538–9.752) | <0.001 | 7.662 (0.974–60.291) | 0.053 | ||
| Tumor location: head vs. neck/body/tail | 1.069 (0. 657–1.738) | 0.789 | 1.281 (0.340–4.831) | 0.714 | ||||
| Lymph node positive: no vs. yes | 4.448 (2.745–7.206) | <0.001 | 2.818 (1.628–4.879) | <0.001 | 5.284 (1.605–17.398) | 0.006 | ||
| Perineural invasion: no vs. yes | 2.608 (1.527–4.455) | 0.001 | 3.446 (0.861–13.782) | 0.080 | ||||
| Microvascular invasion: no vs. yes | 3.317 (2.058–5.345) | <0.001 | 4.958 (1.425–17.250) | 0.012 | 4.395 (1.215–15.905) | 0.024 | ||
| Margin status: R0 vs. R1 | 4.963 (1.997–12.331) | 0.001 | 4.794 (0.606–37.939) | 0.138 | ||||
| Adjuvant treatment: no vs. yes | 3.643 (2.178–6.093) | <0.001 | 1.840 (1.004–3.373) | 0.048 | 4.587 (1.338–15.730) | 0.015 | ||
| WHO classification: G1/G2 vs. G3 | 12.357 (5.810–26.280) | <0.001 | 6.904 (2.994–15.916) | <0.001 | 16.665 (4.225–65.732) | <0.001 | 7.718 (1.543–38.602) | 0.013 |
| Characteristics | SPM Cohort (n = 40) |
|---|---|
| No. (%) | |
| Site | |
| Gynecological tumors | 7 (17.5) |
| Colorectal | 6 (15.0) |
| Gastrointestinal stromal tumor | 6 (15.0) |
| Breast | 4 (10.0) |
| Thyroid | 4 (10.0) |
| Endocrine system | 4 (10.0) |
| Lung | 2 (5.0) |
| Liver | 2 (5.0) |
| Esophagus | 1 (2.5) |
| Stomach | 1 (2.5) |
| Prostate | 1 (2.5) |
| Testis | 1 (2.5) |
| Breast + lung | 1 (2.5) |
| Timing | |
| Synchronous | 17 (42.5) |
| Metachronous Antecedent | 10 (25.0) 13 (32.5) |
| Previous therapy for PanNETs in metachronous SPM | n = 10 |
| SSAs | 2 (20.0) |
| CAPTEM | 1 (10.0) |
| No | 7 (70.0) |
| Therapy for antecedent SPM administered before PanNETs occurrence | n = 13 |
| Chemotherapy | 5 (38.5) |
| Chemotherapy + Targeted therapy | 2 (15.4) |
| No | 6 (46.1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, W.-H.; Xu, J.-F.; Hu, Y.-H.; Qin, Y.; Chen, J.; Yu, X.-J.; Xu, X.-W.; Ji, S.-R. The Surgical and Therapeutic Activities of Non-Functional Pancreatic Neuroendocrine Tumors at a High-Volume Institution. Cancers 2023, 15, 1955. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15071955
Zhang W-H, Xu J-F, Hu Y-H, Qin Y, Chen J, Yu X-J, Xu X-W, Ji S-R. The Surgical and Therapeutic Activities of Non-Functional Pancreatic Neuroendocrine Tumors at a High-Volume Institution. Cancers. 2023; 15(7):1955. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15071955
Chicago/Turabian StyleZhang, Wu-Hu, Jun-Feng Xu, Yu-Heng Hu, Yi Qin, Jie Chen, Xian-Jun Yu, Xiao-Wu Xu, and Shun-Rong Ji. 2023. "The Surgical and Therapeutic Activities of Non-Functional Pancreatic Neuroendocrine Tumors at a High-Volume Institution" Cancers 15, no. 7: 1955. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15071955