
Image-Guided Localization Techniques for Metastatic Axillary Lymph Nodes in Breast Cancer; What Radiologists Should Know
 , , , , and
, , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Axillary Localization Techniques
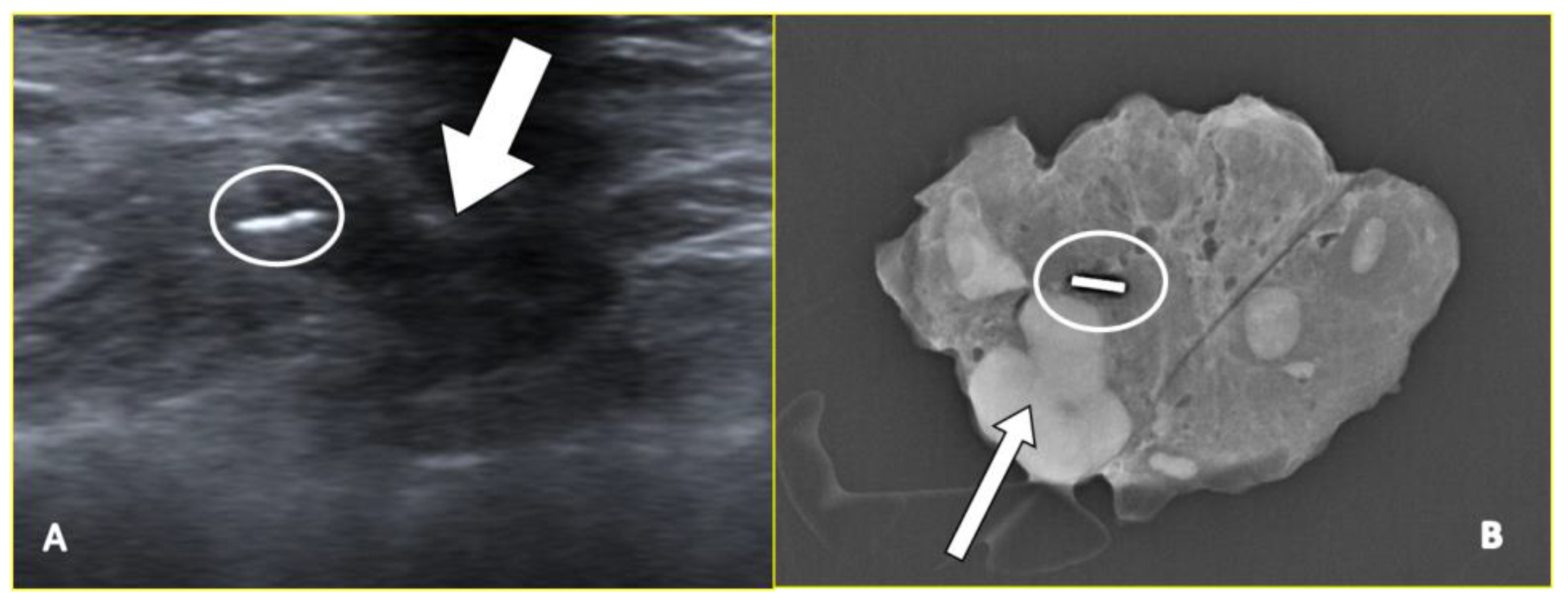
2.1. Marker Clips and Intraoperative Ultrasonography
2.2. Carbon Suspension-Based Localization
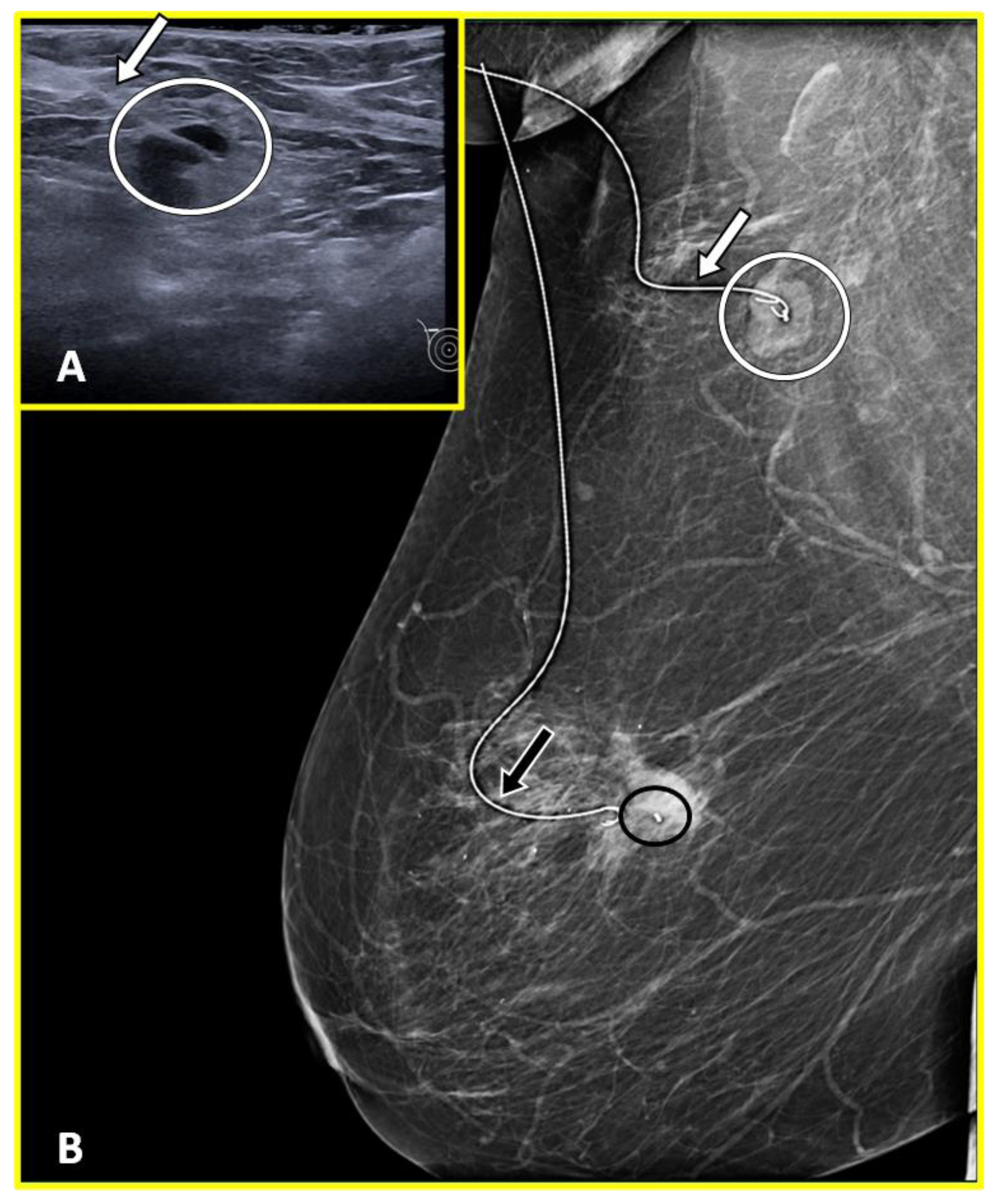
2.3. Metal Wires
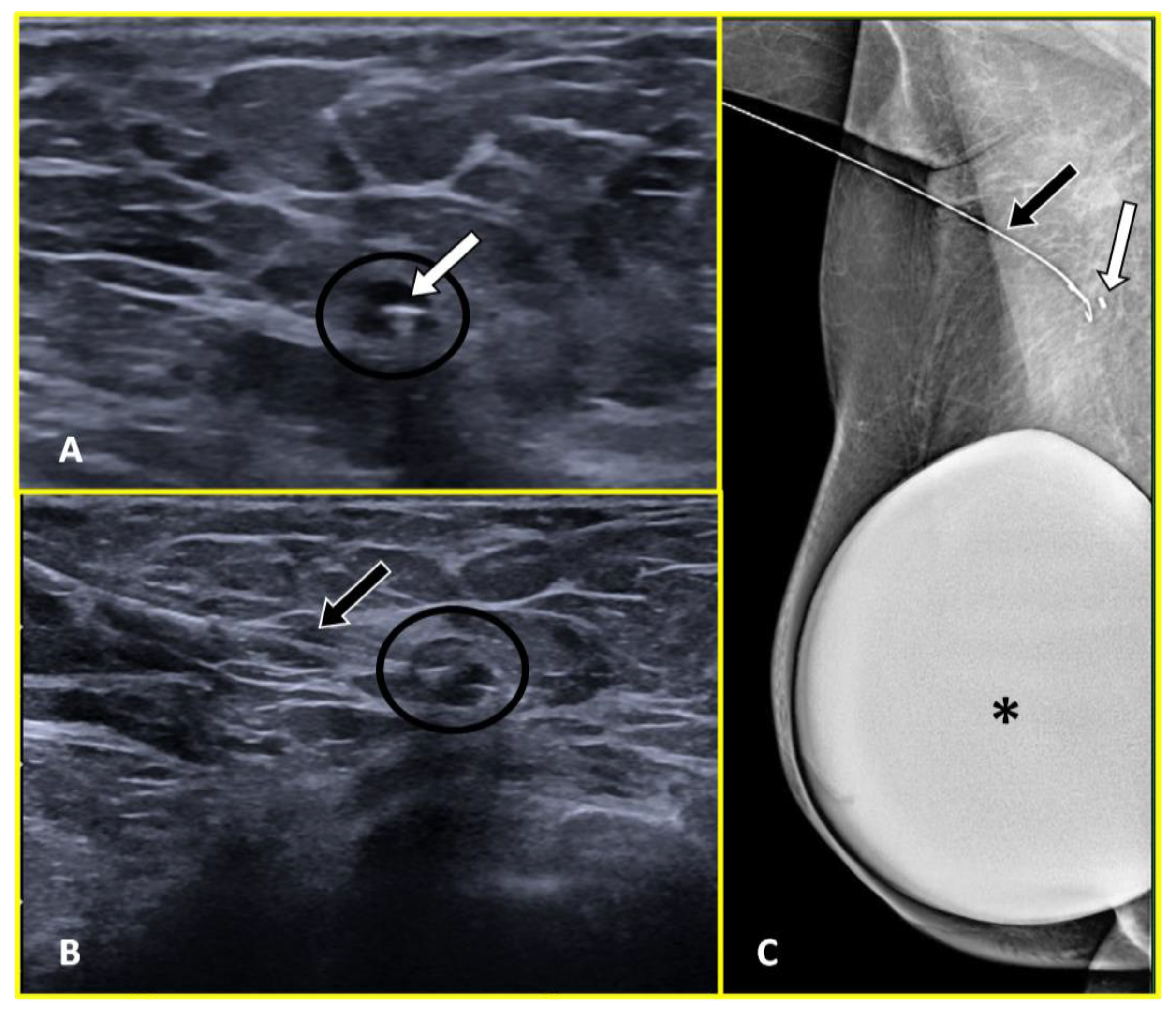
2.4. Magnetic Seed
2.5. Radar and Infrared Light
2.6. Radioactive Tracer-Based Localization
2.6.1. Radioactive Seed Localization
2.6.2. Radioguided Occult Lesion Localization (ROLL)
2.7. Radiofrequency Identification Devices
3. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Panico, C.; Ferrara, F.; Woitek, R.; D’Angelo, A.; Di Paola, V.; Bufi, E.; Conti, M.; Palma, S.; Cicero, S.L.; Cimino, G.; et al. Staging Breast Cancer with MRI, the T. A Key Role in the Neoadjuvant Setting. Cancers 2022, 14, 5786. [Google Scholar] [CrossRef]
- Sivridis, E.; Giatromanolaki, A.; Galazios, G.; Koukourakis, M.I. Node-Related Factors and Survival in Node-Positive Breast Carcinomas. Breast 2006, 15, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Cirocchi, R.; Amabile, M.I.; De Luca, A.; Frusone, F.; Tripodi, D.; Gentile, P.; Tabola, R.; Pironi, D.; Forte, F.; Monti, M.; et al. New Classifications of Axillary Lymph Nodes and Their Anatomical-Clinical Correlations in Breast Surgery. World J. Surg. Oncol. 2021, 19, 93. [Google Scholar] [CrossRef] [PubMed]
- Clough, K.B.; Nasr, R.; Nos, C.; Vieira, M.; Inguenault, C.; Poulet, B. New Anatomical Classification of the Axilla with Implications for Sentinel Node Biopsy. Br. J. Surg. 2010, 97, 1659–1665. [Google Scholar] [CrossRef]
- Ma, X.; Wen, S.; Liu, B.; Li, D.; Wang, X.; Kong, X.; Ma, T.; Jiang, L.; Yang, Q. Relationship between Upper Extremity Lymphatic Drainage and Sentinel Lymph Nodes in Patients with Breast Cancer. J. Oncol. 2019, 2019, 8637895. [Google Scholar] [CrossRef] [PubMed]
- Di Paola, V.; Mazzotta, G.; Pignatelli, V.; Bufi, E.; D’Angelo, A.; Conti, M.; Panico, C.; Fiorentino, V.; Pierconti, F.; Kilburn-Toppin, F.; et al. Beyond N Staging in Breast Cancer: Importance of MRI and Ultrasound-Based Imaging. Cancers 2022, 14, 4270. [Google Scholar] [CrossRef]
- Green, M.; Neamonitou, F.; Vidya, R. Conservative Management of Positive Axilla After Neoadjuvant Systemic Therapy—The Need for, and Review of, Techniques Used for Lymph Node Localization. Clin. Breast Cancer 2018, 18, e739–e742. [Google Scholar] [CrossRef]
- Boughey, J.C.; Suman, V.J.; Mittendorf, E.A.; Ahrendt, G.M.; Wilke, L.G.; Taback, B.; Leitch, A.M.; Kuerer, H.M.; Bowling, M.; Flippo-Morton, T.S.; et al. Alliance for Clinical Trials in Oncology. Sentinel Lymph Node Surgery after Neoadjuvant Chemotherapy in Patients with Node-Positive Breast Cancer: The ACOSOG Z1071 (Alliance) Clinical Trial. JAMA 2013, 310, 1455–1461. [Google Scholar] [CrossRef] [Green Version]
- Staubach, P.; Scharl, A.; Ignatov, A.; Ortmann, O.; Inwald, E.C.; Hildebrandt, T.; Gerken, M.; Klinkhammer-Schalke, M.; Scharl, S.; Papathemelis, T. Sentinel Lymph Node Detection by Means of Indocyanine Green Using the Karl Storz VITOM® Fluorescence Camera: A Comparison between Primary Sentinel Lymph Node Biopsy versus Sentinel Lymph Node Biopsy after Neoadjuvant Chemotherapy. J. Cancer Res. Clin. Oncol. 2021, 147, 1813–1823. [Google Scholar] [CrossRef]
- Pelc, Z.; Skórzewska, M.; Kurylcio, M.; Nowikiewicz, T.; Mlak, R.; Sędłak, K.; Gęca, K.; Rawicz-Pruszyński, K.; Zegarski, W.; Polkowski, W.P.; et al. A Propensity Score Matched Analysis of Superparamagnetic Iron Oxide versus Radioisotope Sentinel Node Biopsy in Breast Cancer Patients after Neoadjuvant Chemotherapy. Cancers 2022, 14, 676. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.T.; Zackrisson, S.; Senkus, E. Early Breast Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2019, 30, 1194–1220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gradishar, W.J.; Moran, M.S.; Abraham, J.; Aft, R.; Agnese, D.; Allison, K.H.; Anderson, B.; Burstein, H.J.; Chew, H.; Dang, C.; et al. Breast Cancer, Version 3.2022, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. JNCCN 2022, 20, 691–722. [Google Scholar] [CrossRef]
- Kahler-Ribeiro-Fontana, S.; Pagan, E.; Magnoni, F.; Vicini, E.; Morigi, C.; Corso, G.; Intra, M.; Canegallo, F.; Ratini, S.; Leonardi, M.C.; et al. Long-Term Standard Sentinel Node Biopsy after Neoadjuvant Treatment in Breast Cancer: A Single Institution Ten-Year Follow-Up. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2021, 47, 804–812. [Google Scholar] [CrossRef]
- Classe, J.-M.; Loaec, C.; Gimbergues, P.; Alran, S.; de Lara, C.T.; Dupre, P.F.; Rouzier, R.; Faure, C.; Paillocher, N.; Chauvet, M.P.; et al. Sentinel Lymph Node Biopsy without Axillary Lymphadenectomy after Neoadjuvant Chemotherapy Is Accurate and Safe for Selected Patients: The GANEA 2 Study. Breast Cancer Res. Treat. 2019, 173, 343–352. [Google Scholar] [CrossRef]
- Dominici, L.S.; Negron Gonzalez, V.M.; Buzdar, A.U.; Lucci, A.; Mittendorf, E.A.; Le-Petross, H.T.; Babiera, G.V.; Meric-Bernstam, F.; Hunt, K.K.; Kuerer, H.M. Cytologically Proven Axillary Lymph Node Metastases Are Eradicated in Patients Receiving Preoperative Chemotherapy with Concurrent Trastuzumab for HER2-Positive Breast Cancer. Cancer 2010, 116, 2884–2889. [Google Scholar] [CrossRef]
- Buzdar, A.U.; Ibrahim, N.K.; Francis, D.; Booser, D.J.; Thomas, E.S.; Theriault, R.L.; Pusztai, L.; Green, M.C.; Arun, B.K.; Giordano, S.H.; et al. Significantly Higher Pathologic Complete Remission Rate after Neoadjuvant Therapy with Trastuzumab, Paclitaxel, and Epirubicin Chemotherapy: Results of a Randomized Trial in Human Epidermal Growth Factor Receptor 2-Positive Operable Breast Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2005, 23, 3676–3685. [Google Scholar] [CrossRef] [PubMed]
- Alvarado, R.; Yi, M.; Le-Petross, H.; Gilcrease, M.; Mittendorf, E.A.; Bedrosian, I.; Hwang, R.F.; Caudle, A.S.; Babiera, G.V.; Akins, J.S.; et al. The Role for Sentinel Lymph Node Dissection after Neoadjuvant Chemotherapy in Patients Who Present with Node-Positive Breast Cancer. Ann. Surg. Oncol. 2012, 19, 3177–3184. [Google Scholar] [CrossRef]
- Kuehn, T.; Bauerfeind, I.; Fehm, T.; Fleige, B.; Hausschild, M.; Helms, G.; Lebeau, A.; Liedtke, C.; von Minckwitz, G.; Nekljudova, V.; et al. Sentinel-Lymph-Node Biopsy in Patients with Breast Cancer before and after Neoadjuvant Chemotherapy (SENTINA): A Prospective, Multicentre Cohort Study. Lancet Oncol. 2013, 14, 609–618. [Google Scholar] [CrossRef]
- Boileau, J.-F.; Poirier, B.; Basik, M.; Holloway, C.M.B.; Gaboury, L.; Sideris, L.; Meterissian, S.; Arnaout, A.; Brackstone, M.; McCready, D.R.; et al. Sentinel Node Biopsy after Neoadjuvant Chemotherapy in Biopsy-Proven Node-Positive Breast Cancer: The SN FNAC Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2015, 33, 258–264. [Google Scholar] [CrossRef]
- Cohen, L.F.; Breslin, T.M.; Kuerer, H.M.; Ross, M.I.; Hunt, K.K.; Sahin, A.A. Identification and Evaluation of Axillary Sentinel Lymph Nodes in Patients with Breast Carcinoma Treated with Neoadjuvant Chemotherapy. Am. J. Surg. Pathol. 2000, 24, 1266–1272. [Google Scholar] [CrossRef]
- Goyal, A.; Newcombe, R.G.; Chhabra, A.; Mansel, R.E.; on behalf of the ALMANAC Trialists Group. Factors Affecting Failed Localisation and False-Negative Rates of Sentinel Node Biopsy in Breast Cancer—Results of the ALMANAC Validation Phase. Breast Cancer Res. Treat. 2006, 99, 203–208. [Google Scholar] [CrossRef]
- King, T.A.; Morrow, M. Surgical Issues in Patients with Breast Cancer Receiving Neoadjuvant Chemotherapy. Nat. Rev. Clin. Oncol. 2015, 12, 335–343. [Google Scholar] [CrossRef]
- Boughey, J.C.; Ballman, K.V.; Le-Petross, H.T.; McCall, L.M.; Mittendorf, E.A.; Ahrendt, G.M.; Wilke, L.G.; Taback, B.; Feliberti, E.C.; Hunt, K.K. Identification and Resection of Clipped Node Decreases the False-Negative Rate of Sentinel Lymph Node Surgery in Patients Presenting With Node-Positive Breast Cancer (T0-T4, N1-N2) Who Receive Neoadjuvant Chemotherapy: Results From ACOSOG Z1071 (Alliance). Ann. Surg. 2016, 263, 802–807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caudle, A.S.; Yang, W.T.; Krishnamurthy, S.; Mittendorf, E.A.; Black, D.M.; Gilcrease, M.Z.; Bedrosian, I.; Hobbs, B.P.; DeSnyder, S.M.; Hwang, R.F.; et al. Improved Axillary Evaluation Following Neoadjuvant Therapy for Patients With Node-Positive Breast Cancer Using Selective Evaluation of Clipped Nodes: Implementation of Targeted Axillary Dissection. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2016, 34, 1072–1078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caudle, A.S.; Yang, W.T.; Mittendorf, E.A.; Black, D.M.; Hwang, R.; Hobbs, B.; Hunt, K.K.; Krishnamurthy, S.; Kuerer, H.M. Selective Surgical Localization of Axillary Lymph Nodes Containing Metastases in Patients with Breast Cancer: A Prospective Feasibility Trial. JAMA Surg. 2015, 150, 137–143. [Google Scholar] [CrossRef] [Green Version]
- Krivorotko, P.; Emelyanov, A.; Komyahov, A.; Zhiltsova, E.; Gigolaeva, L.; Tabagua, T.; Nikolaev, K.; Pesotskiy, R.; Gukova, V.; Amirov, N.; et al. Axillary Surgery after Neoadjuvant Chemotherapy in Breast Cancer Patients Downstaging from CN+ to YcN0. J. Clin. Oncol. 2022, 40 (Suppl. S16), e12580. [Google Scholar] [CrossRef]
- Kuemmel, S.; Heil, J.; Rueland, A.; Seiberling, C.; Harrach, H.; Schindowski, D.; Lubitz, J.; Hellerhoff, K.; Ankel, C.; Graßhoff, S.-T.; et al. A Prospective, Multicenter Registry Study to Evaluate the Clinical Feasibility of Targeted Axillary Dissection (TAD) in Node-Positive Breast Cancer Patients. Ann. Surg. 2022, 276, e553–e562. [Google Scholar] [CrossRef]
- Mariscal Martínez, A.; Vives Roselló, I.; Salazar Gómez, A.; Catanese, A.; Pérez Molina, M.; Solà Suarez, M.; Pascual Miguel, I.; Blay Aulina, L.; Ríos Gozálvez, C.; Julián Ibáñez, J.F.; et al. Advantages of Preoperative Localization and Surgical Resection of Metastatic Axillary Lymph Nodes Using Magnetic Seeds after Neoadjuvant Chemotherapy in Breast Cancer. Surg. Oncol. 2021, 36, 28–33. [Google Scholar] [CrossRef]
- Simons, J.M.; van Nijnatten, T.J.A.; van der Pol, C.C.; van Diest, P.J.; Jager, A.; van Klaveren, D.; Kam, B.L.R.; Lobbes, M.B.I.; de Boer, M.; Verhoef, C.; et al. Diagnostic Accuracy of Radioactive Iodine Seed Placement in the Axilla With Sentinel Lymph Node Biopsy After Neoadjuvant Chemotherapy in Node-Positive Breast Cancer. JAMA Surg. 2022, 157, 991–999. [Google Scholar] [CrossRef] [PubMed]
- Swarnkar, P.K.; Tayeh, S.; Michell, M.J.; Mokbel, K. The Evolving Role of Marked Lymph Node Biopsy (MLNB) and Targeted Axillary Dissection (TAD) after Neoadjuvant Chemotherapy (NACT) for Node-Positive Breast Cancer: Systematic Review and Pooled Analysis. Cancers 2021, 13, 1539. [Google Scholar] [CrossRef]
- Siso, C.; de Torres, J.; Esgueva-Colmenarejo, A.; Espinosa-Bravo, M.; Rus, N.; Cordoba, O.; Rodriguez, R.; Peg, V.; Rubio, I.T. Intraoperative Ultrasound-Guided Excision of Axillary Clip in Patients with Node-Positive Breast Cancer Treated with Neoadjuvant Therapy (ILINA Trial): A New Tool to Guide the Excision of the Clipped Node After Neoadjuvant Treatment. Ann. Surg. Oncol. 2018, 25, 784–791. [Google Scholar] [CrossRef]
- Aragón-Sánchez, S.; Ciruelos-Gil, E.; López-Marín, L.; Galindo, A.; Tabuenca-Mateos, M.J.; Jiménez-Arranz, S.; Colmenero-Hernández, M.; Oliver-Pérez, M.R. Feasibility of Targeted Axillary Dissection for De-Escalation of Surgical Treatment after Neoadjuvant Chemotherapy in Breast Cancer. Surg. Oncol. 2022, 44, 101823. [Google Scholar] [CrossRef] [PubMed]
- Burstein, H.J.; Curigliano, G.; Thürlimann, B.; Weber, W.P.; Poortmans, P.; Regan, M.M.; Senn, H.J.; Winer, E.P.; Gnant, M.; Panelists of the St Gallen Consensus Conference. Customizing Local and Systemic Therapies for Women with Early Breast Cancer: The St. Gallen International Consensus Guidelines for Treatment of Early Breast Cancer 2021. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2021, 32, 1216–1235. [Google Scholar] [CrossRef] [PubMed]
- Brackstone, M.; Baldassarre, F.G.; Perera, F.E.; Cil, T.; Chavez Mac Gregor, M.; Dayes, I.S.; Engel, J.; Horton, J.K.; King, T.A.; Kornecki, A.; et al. Management of the Axilla in Early-Stage Breast Cancer: Ontario Health (Cancer Care Ontario) and ASCO Guideline. J. Clin. Oncol. 2021, 39, 3056–3082. [Google Scholar] [CrossRef] [PubMed]
- Ditsch, N.; Wöcke, A.; Untch, M.; Jackisch, C.; Albert, U.-S.; Banys-Paluchowski, M.; Bauerfeind, I.; Blohmer, J.-U.; Budach, W.; Dall, P.; et al. AGO Recommendations for the Diagnosis and Treatment of Patients with Early Breast Cancer: Update 2022. Breast Care 2022, 17, 403–420. [Google Scholar] [CrossRef]
- Consensus Statement on Axillary Management for Patients with In-Situ and Invasive Breast Cancer: A Concise Overview; The American Society of Breast Surgeons: Boston, MA, USA, 2022.
- Thomassin-Naggara, I.; Lalonde, L.; David, J.; Darai, E.; Uzan, S.; Trop, I. A Plea for the Biopsy Marker: How, Why and Why Not Clipping after Breast Biopsy? Breast Cancer Res. Treat. 2012, 132, 881–893. [Google Scholar] [CrossRef]
- Guenin, M.A. Clip Placement during Sonographically Guided Large-Core Breast Biopsy for Mammographic-Sonographic Correlation. AJR Am. J. Roentgenol. 2000, 175, 1053–1055. [Google Scholar] [CrossRef]
- Liberman, L.; Dershaw, D.D.; Morris, E.A.; Abramson, A.F.; Thornton, C.M.; Rosen, P.P. Clip Placement after Stereotactic Vacuum-Assisted Breast Biopsy. Radiology 1997, 205, 417–422. [Google Scholar] [CrossRef]
- Perlet, C.; Sittek, H.; Reiser, M.; Heywang-Köbrunner, S.H. Clip marker placement following MR-guided vacuum biopsy of the breast. Radiol. 2005, 45, 230–236. [Google Scholar] [CrossRef]
- Corsi, F.; Sorrentino, L.; Sartani, A.; Bossi, D.; Amadori, R.; Nebuloni, M.; Truffi, M.; Bonzini, M.; Foschi, D. Localization of Nonpalpable Breast Lesions with Sonographically Visible Clip: Optimizing Tailored Resection and Clear Margins. Am. J. Surg. 2015, 209, 950–958. [Google Scholar] [CrossRef] [PubMed]
- Murthy, V.; Young, J.; Tokumaru, Y.; Quinn, M.; Edge, S.B.; Takabe, K. Options to Determine Pathological Response of Axillary Lymph Node Metastasis after Neoadjuvant Chemotherapy in Advanced Breast Cancer. Cancers 2021, 13, 4167. [Google Scholar] [CrossRef] [PubMed]
- Gittleman, M.A. Single-Step Ultrasound Localization of Breast Lesions and Lumpectomy Procedure. Am. J. Surg. 2003, 186, 386–390. [Google Scholar] [CrossRef] [PubMed]
- Eby, P.R.; Calhoun, K.E.; Kurland, B.F.; Demartini, W.B.; Gutierrez, R.L.; Peacock, S.; Anderson, B.O.; Byrd, D.R.; Mann, G.N.; Lehman, C.D. Preoperative and Intraoperative Sonographic Visibility of Collagen-Based Breast Biopsy Marker Clips. Acad. Radiol. 2010, 17, 340–347. [Google Scholar] [CrossRef]
- Klein, R.L.; Mook, J.A.; Euhus, D.M.; Rao, R.; Wynn, R.T.; Eastman, A.B.; Leitch, A.M. Evaluation of a Hydrogel Based Breast Biopsy Marker (HydroMARK®) as an Alternative to Wire and Radioactive Seed Localization for Non-Palpable Breast Lesions. J. Surg. Oncol. 2012, 105, 591–594. [Google Scholar] [CrossRef]
- Ahmed, M.; Abdullah, N.; Cawthorn, S.; Usiskin, S.I.; Douek, M. Why Should Breast Surgeons Use Ultrasound? Breast Cancer Res. Treat. 2014, 145, 1–4. [Google Scholar] [CrossRef]
- Carmon, M.; Olsha, O.; Gekhtman, D.; Nikitin, I.; Cohen, Y.; Messing, M.; Lioubashevsky, N.; Abu Dalo, R.; Hadar, T.; Golomb, E. Detectability of Hygroscopic Clips Used in Breast Cancer Surgery. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2017, 36, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Blumencranz, P.W.; Ellis, D.; Barlowe, K. Use of Hydrogel Breast Biopsy Tissue Markers Reduces the Need for Wire Localization. Ann. Surg. Oncol. 2014, 21, 3273–3277. [Google Scholar] [CrossRef]
- Hartmann, S.; Stachs, A.; Kühn, T.; de Boniface, J.; Banys-Paluchowski, M.; Reimer, T. Targeted Removal of Axillary Lymph Nodes After Carbon Marking in Patients with Breast Cancer Treated with Primary Chemotherapy. Geburtshilfe Frauenheilkd. 2021, 81, 1121–1127. [Google Scholar] [CrossRef]
- Ruiz-Delgado, M.L.; López-Ruiz, J.A.; Sáiz-López, A. Abnormal Mammography and Sonography Associated with Foreign-Body Giant-Cell Reaction after Stereotactic Vacuum-Assisted Breast Biopsy with Carbon Marking. Acta Radiol. Stockh. Swed. 1987 2008, 49, 1112–1118. [Google Scholar] [CrossRef]
- Hartmann, S.; Kühn, T.; de Boniface, J.; Stachs, A.; Winckelmann, A.; Frisell, J.; Wiklander-Bråkenhielm, I.; Stubert, J.; Gerber, B.; Reimer, T. Carbon Tattooing for Targeted Lymph Node Biopsy after Primary Systemic Therapy in Breast Cancer: Prospective Multicentre TATTOO Trial. Br. J. Surg. 2021, 108, 302–307. [Google Scholar] [CrossRef]
- Khallaf, E.; Wessam, R.; Abdoon, M. Targeted Axillary Dissection of Carbon-Tattooed Metastatic Lymph Nodes in Combination with Post-Neo-Adjuvant Sentinel Lymph Node Biopsy Using 1% Methylene Blue in Breast Cancer Patients. Breast J. 2020, 26, 1061–1063. [Google Scholar] [CrossRef] [PubMed]
- Choy, N.; Lipson, J.; Porter, C.; Ozawa, M.; Kieryn, A.; Pal, S.; Kao, J.; Trinh, L.; Wheeler, A.; Ikeda, D.; et al. Initial Results with Preoperative Tattooing of Biopsied Axillary Lymph Nodes and Correlation to Sentinel Lymph Nodes in Breast Cancer Patients. Ann. Surg. Oncol. 2015, 22, 377–382. [Google Scholar] [CrossRef]
- Hartmann, S.; Stachs, A.; Kühn, T.; Winckelmann, A.; de Boniface, J.; Gerber, B.; Reimer, T. Target Lymph Node Biopsy (TLNB) nach Kohlenstoffmarkierung bei Mammakarzinom-Patientinnen im Rahmen der primären Systemtherapie—Ergebnisse der TATTOO-Studie. In Geburtshilfe und Frauenheilkunde; Thieme: Leipzig, Germany, 2020; Volume 80, p. 61. [Google Scholar] [CrossRef]
- Natsiopoulos, I.; Intzes, S.; Liappis, T.; Zarampoukas, K.; Zarampoukas, T.; Zacharopoulou, V.; Papazisis, K. Axillary Lymph Node Tattooing and Targeted Axillary Dissection in Breast Cancer Patients Who Presented as CN+ Before Neoadjuvant Chemotherapy and Became CN0 After Treatment. Clin. Breast Cancer 2019, 19, 208–215. [Google Scholar] [CrossRef]
- Trinh, L.; Miyake, K.K.; Dirbas, F.M.; Kothary, N.; Horst, K.C.; Lipson, J.A.; Carpenter, C.; Thompson, A.C.; Ikeda, D.M. CT-Guided Wire Localization for Involved Axillary Lymph Nodes After Neo-Adjuvant Chemotherapy in Patients With Initially Node-Positive Breast Cancer. Breast J. 2016, 22, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Woods, R.W.; Camp, M.S.; Durr, N.J.; Harvey, S.C. A Review of Options for Localization of Axillary Lymph Nodes in the Treatment of Invasive Breast Cancer. Acad. Radiol. 2019, 26, 805–819. [Google Scholar] [CrossRef] [PubMed]
- Hayes, M.K. Update on Preoperative Breast Localization. Radiol. Clin. North Am. 2017, 55, 591–603. [Google Scholar] [CrossRef]
- Ahmed, M.; Douek, M. Radioactive Seed Localisation (RSL) in the Treatment of Non-Palpable Breast Cancers: Systematic Review and Meta-Analysis. Breast 2013, 22, 383–388. [Google Scholar] [CrossRef] [PubMed]
- van Susante, J.L.C.; Barendregt, W.B.; Bruggink, E.D.M. Migration of the Guide-Wire into the Pleural Cavity after Needle Localization of Breast Lesions. Eur. J. Surg. Oncol. EJSO 1998, 24, 446–448. [Google Scholar] [CrossRef]
- Davis, P.S.; Wechsler, R.J.; Feig, S.A.; March, D.E. Migration of Breast Biopsy Localization Wire. AJR Am. J. Roentgenol. 1988, 150, 787–788. [Google Scholar] [CrossRef]
- Martinez, S.R.; Gelfand, M.; Hourani, H.S.; Sorrento, J.J.; Mohan, E.P. Cardiac Injury during Needle Localized Surgical Breast Biopsy. J. Surg. Oncol. 2003, 82, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Bristol, J.B.; Jones, P.A. Transgression of Localizing Wire into the Pleural Cavity Prior to Mammography. Br. J. Radiol. 1981, 54, 139–140. [Google Scholar] [CrossRef] [PubMed]
- Mj, H. Transection of the Localization Hooked Wire during Breast Biopsy. AJR Am. J. Roentgenol. 1983, 141, 5. [Google Scholar] [CrossRef]
- Harvey, J.R.; Lim, Y.; Murphy, J.; Howe, M.; Morris, J.; Goyal, A.; Maxwell, A.J. Safety and Feasibility of Breast Lesion Localization Using Magnetic Seeds (Magseed): A Multi-Centre, Open-Label Cohort Study. Breast Cancer Res. Treat. 2018, 169, 531–536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Price, E.R.; Khoury, A.L.; Esserman, L.J.; Joe, B.N.; Alvarado, M.D. Initial Clinical Experience With an Inducible Magnetic Seed System for Preoperative Breast Lesion Localization. AJR Am. J. Roentgenol. 2018, 210, 913–917. [Google Scholar] [CrossRef]
- Mammotome: Massima Efficienza, Cure Ottimizzate. Available online: https://it.mammotome.com (accessed on 24 February 2023).
- Schermers, B.; van der Hage, J.A.; Loo, C.E.; Peeters, M.V.; Winter-Warnars, H.A.O.; van Duijnhoven, F.; Ten Haken, B.; Muller, S.H.; Ruers, T.J.M. Feasibility of Magnetic Marker Localisation for Non-Palpable Breast Cancer. Breast 2017, 33, 50–56. [Google Scholar] [CrossRef]
- Merit Oncology. Merit Medical. Available online: https://www.merit.com/merit-oncology/ (accessed on 24 February 2023).
- Jeffries, D.O.; Dossett, L.A.; Jorns, J.M. Localization for Breast Surgery: The Next Generation. Arch. Pathol. Lab. Med. 2017, 141, 1324–1329. [Google Scholar] [CrossRef] [Green Version]
- Cox, C.E.; Russell, S.; Prowler, V.; Carter, E.; Beard, A.; Mehindru, A.; Blumencranz, P.; Allen, K.; Portillo, M.; Whitworth, P.; et al. A Prospective, Single Arm, Multi-Site, Clinical Evaluation of a Nonradioactive Surgical Guidance Technology for the Location of Nonpalpable Breast Lesions during Excision. Ann. Surg. Oncol. 2016, 23, 3168–3174. [Google Scholar] [CrossRef]
- Mango, V.; Ha, R.; Gomberawalla, A.; Wynn, R.; Feldman, S. Evaluation of the SAVI SCOUT Surgical Guidance System for Localization and Excision of Nonpalpable Breast Lesions: A Feasibility Study. AJR Am. J. Roentgenol. 2016, 207, W69–W72. [Google Scholar] [CrossRef] [Green Version]
- Mango, V.L.; Wynn, R.T.; Feldman, S.; Friedlander, L.; Desperito, E.; Patel, S.N.; Gomberawalla, A.; Ha, R. Beyond Wires and Seeds: Reflector-Guided Breast Lesion Localization and Excision. Radiology 2017, 284, 365–371. [Google Scholar] [CrossRef]
- Reicher, J.J.; Reicher, M.A.; Thomas, M.; Petcavich, R. Radiofrequency Identification Tags for Preoperative Tumor Localization: Proof of Concept. AJR Am. J. Roentgenol. 2008, 191, 1359–1365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharek, D.; Zuley, M.L.; Zhang, J.Y.; Soran, A.; Ahrendt, G.M.; Ganott, M.A. Radioactive Seed Localization versus Wire Localization for Lumpectomies: A Comparison of Outcomes. AJR Am. J. Roentgenol. 2015, 204, 872–877. [Google Scholar] [CrossRef] [PubMed]
- Janssen, N.N.Y.; Nijkamp, J.; Alderliesten, T.; Loo, C.E.; Rutgers, E.J.T.; Sonke, J.-J.; Vrancken Peeters, M.T.F.D. Radioactive Seed Localization in Breast Cancer Treatment. Br. J. Surg. 2016, 103, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Hylenius, S.; Uldall, W.; Qvamme, G.; Kroman, N. Radioactive Seed Localization of Foreign Body. Acta Radiol. Open 2022, 11, 20584601221088920. [Google Scholar] [CrossRef]
- Banys-Paluchowski, M.; Kühn, T.; Masannat, Y.; Rubio, I.; de Boniface, J.; Ditsch, N.; Karadeniz Cakmak, G.; Karakatsanis, A.; Dave, R.; Hahn, M.; et al. Localization Techniques for Non-Palpable Breast Lesions: Current Status, Knowledge Gaps, and Rationale for the MELODY Study (EUBREAST-4/IBRA-NET, NCT 05559411). Cancers 2023, 15, 1173. [Google Scholar] [CrossRef]
- Diego, E.J.; McAuliffe, P.F.; Soran, A.; McGuire, K.P.; Johnson, R.R.; Bonaventura, M.; Ahrendt, G.M. Axillary Staging After Neoadjuvant Chemotherapy for Breast Cancer: A Pilot Study Combining Sentinel Lymph Node Biopsy with Radioactive Seed Localization of Pre-Treatment Positive Axillary Lymph Nodes. Ann. Surg. Oncol. 2016, 23, 1549–1553. [Google Scholar] [CrossRef] [PubMed]
- Barros, A.; Cardoso, M.; Sheng, P.; Costa, P.; Pelizon, C. Radioguided Localisation of Non-Palpable Breast Lesions and Simultaneous Sentinel Lymph Node Mapping. Eur. J. Nucl. Med. Mol. Imaging 2002, 29, 1561–1565. [Google Scholar] [CrossRef]
- Thind, C.R.; Desmond, S.; Harris, O.; Nadeem, R.; Chagla, L.S.; Audisio, R.A. Radio-Guided Localization of Clinically Occult Breast Lesions (ROLL): A DGH Experience. Clin. Radiol. 2005, 60, 681–686. [Google Scholar] [CrossRef]
- Nadeem, R.; Chagla, L.S.; Harris, O.; Desmond, S.; Thind, R.; Titterrell, C.; Audisio, R.A. Occult Breast Lesions: A Comparison between Radioguided Occult Lesion Localisation (ROLL) vs. Wire-Guided Lumpectomy (WGL). Breast 2005, 14, 283–289. [Google Scholar] [CrossRef]
- De Cicco, C.; Pizzamiglio, M.; Trifirò, G.; Luini, A.; Ferrari, M.; Prisco, G.; Galimberti, V.; Cassano, E.; Viale, G.; Intra, M.; et al. Radioguided Occult Lesion Localisation (ROLL) and Surgical Biopsy in Breast Cancer. Technical Aspects. Q. J. Nucl. Med. Off. Publ. Ital. Assoc. Nucl. Med. AIMN Int. Assoc. Radiopharmacol. IAR 2002, 46, 145–151. [Google Scholar]
- Rampaul, R.S.; Dudley, N.J.; Thompson, J.Z.; Burrell, H.; Evans, A.J.; Wilson, A.R.M.; Macmillan, R.D. Radioisotope for Occult Lesion Localisation (ROLL) of the Breast Does Not Require Extra Radiation Protection Procedures. Breast 2003, 12, 150–152. [Google Scholar] [CrossRef]
- Aydogan, F.; Ozben, V.; Celik, V.; Uras, C.; Tahan, G.; Gazioglu, E.; Cengiz, A.; Ferahman, M.; Cercel, A.; Yilmaz, M.H.; et al. Radioguided Occult Lesion Localization (ROLL) for Non-Palpable Breast Cancer: A Comparison between Day-before and Same-Day Protocols. Breast 2010, 19, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Seok, J.W.; Kim, I.J.; Heo, Y.-J.; Yang, Y.J.; Choi, Y.S.; Kim, B.G.; Park, S.J. Comparison of Subareolar Injection Lymphoscintigraphy with the 1-Day and the 2-Day Protocols for the Detection of Sentinel Lymph Nodes in Patients with Breast Cancer. Ann. Nucl. Med. 2009, 23, 465–469. [Google Scholar] [CrossRef] [PubMed]
- Medina-Franco, H.; Abarca-Pérez, L.; Ulloa-Gómez, J.L.; Romero, C. Radioguided Localization of Clinically Occult Breast Lesions (ROLL): A Pilot Study. Breast J. 2007, 13, 401–405. [Google Scholar] [CrossRef]
- Ramesh, H.S.J.; Anguille, S.; Chagla, L.S.; Harris, O.; Desmond, S.; Thind, R.; Audisio, R.A. Recurrence after ROLL Lumpectomy for Invasive Breast Cancer. Breast 2008, 17, 637–639. [Google Scholar] [CrossRef] [PubMed]
- van Rijk, M.C.; Tanis, P.J.; Nieweg, O.E.; Loo, C.E.; Olmos, R.A.V.; Oldenburg, H.S.A.; Rutgers, E.J.T.; Hoefnagel, C.A.; Kroon, B.B.R. Sentinel Node Biopsy and Concomitant Probe-Guided Tumor Excision of Nonpalpable Breast Cancer. Ann. Surg. Oncol. 2007, 14, 627–632. [Google Scholar] [CrossRef]
- Besic, N.; Kramaric, A.; Podnar, B.; Perhavec, A.; Music, M.; Grazio-Frkovic, S.; Zgajnar, J. Factors Correlated to Successful Surgical Treatment of 181 Non-Palpable Invasive Breast Carcinomas. Breast 2009, 18, 294–298. [Google Scholar] [CrossRef]
- Zgajnar, J.; Hocevar, M.; Frkovic-Grazio, S.; Hertl, K.; Schweiger, E.; Besic, N. Radioguided Occult Lesion Localization (ROLL) of the Nonpalpable Breast Lesions. Neoplasma 2004, 51, 385–389. [Google Scholar]
- Hellingman, D.; Donswijk, M.L.; Winter-Warnars, G.A.O.; de Koekkoek-Doll, P.; Pinas, M.; Budde-van Namen, Y.; Westerga, J.; Vrancken Peeters, M.-J.T.F.D.; Kimmings, N.; Stokkel, M.P.M. Feasibility of Radioguided Occult Lesion Localization of Clip-Marked Lymph Nodes for Tailored Axillary Treatment in Breast Cancer Patients Treated with Neoadjuvant Systemic Therapy. EJNMMI Res. 2019, 9, 94. [Google Scholar] [CrossRef] [PubMed]
- Adamczyk, B.; Seraszek-Jaros, A.; Listwan, K.; Wasiewicz, J. Is SNOLL a Good Localization Technique in Early Breast Cancer Treatment? A Single Center’s Experience. Rep. Pract. Oncol. Radiother. 2020, 25, 594–597. [Google Scholar] [CrossRef]
- Malter, W.; Eichler, C.; Hanstein, B.; Mallmann, P.; Holtschmidt, J. First Reported Use of Radiofrequency Identification (RFID) Technique for Targeted Excision of Suspicious Axillary Lymph Nodes in Early Stage Breast Cancer—Evaluation of Feasibility and Review of Current Recommendations. Vivo Athens Greece 2020, 34, 1207–1213. [Google Scholar] [CrossRef]
- den Dekker, B.M.; Christenhusz, A.; van Dalen, T.; Jongen, L.M.; van der Schaaf, M.C.; Dassen, A.E.; Pijnappel, R.M. A Multicenter Prospective Cohort Study to Evaluate Feasibility of Radio-Frequency Identification Surgical Guidance for Nonpalpable Breast Lesions: Design and Rationale of the RFID Localizer 1 Trial. BMC Cancer 2022, 22, 305. [Google Scholar] [CrossRef] [PubMed]
- Wazir, U.; Tayeh, S.; Perry, N.; Michell, M.; Malhotra, A.; Mokbel, K. Wireless Breast Localization Using Radio-Frequency Identification Tags: The First Reported European Experience in Breast Cancer. Vivo Athens Greece 2020, 34, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Lowes, S.; Bell, A.; Milligan, R.; Amonkar, S.; Leaver, A. Use of Hologic LOCalizer Radiofrequency Identification (RFID) Tags to Localise Impalpable Breast Lesions and Axillary Nodes: Experience of the First 150 Cases in a UK Breast Unit. Clin. Radiol. 2020, 75, 942–949. [Google Scholar] [CrossRef] [PubMed]
- Heindl, F.; Schulz-Wendtland, R.; Jud, S.; Erber, R.; Hack, C.C.; Preuss, C.; Behrens, A.; Pöschke, P.; Emons, J. Evaluation of a Wireless Localization System for Nonpalpable Breast Lesions—Feasibility and Cost-Effectiveness in Everyday Clinical Routine. Vivo Athens Greece 2022, 36, 2342–2349. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Prospective Trial | Overall FNR (%) | FNR Stratified by Number of SLNs (%) | FNR Stratified by SLN-Detection Technique (%) | |||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | Single Agent | Dual Agent | ||
| SENTINA | 14.2 | 24.3 | 18.5 | 7.3 | 16 | 8.6 |
| ACOSOG Z1071 | 12.6 | 31.5 | 21 | 9.1 | 20.3 | 10.8 |
| SN FNAC | 8.4 | 18.2 | 4.9 * | NR | 16.0 | 5.2 |
| GANEA 2 | 11.9 a | 19.4 | 7.8 * | NR | NR | 11.9 |
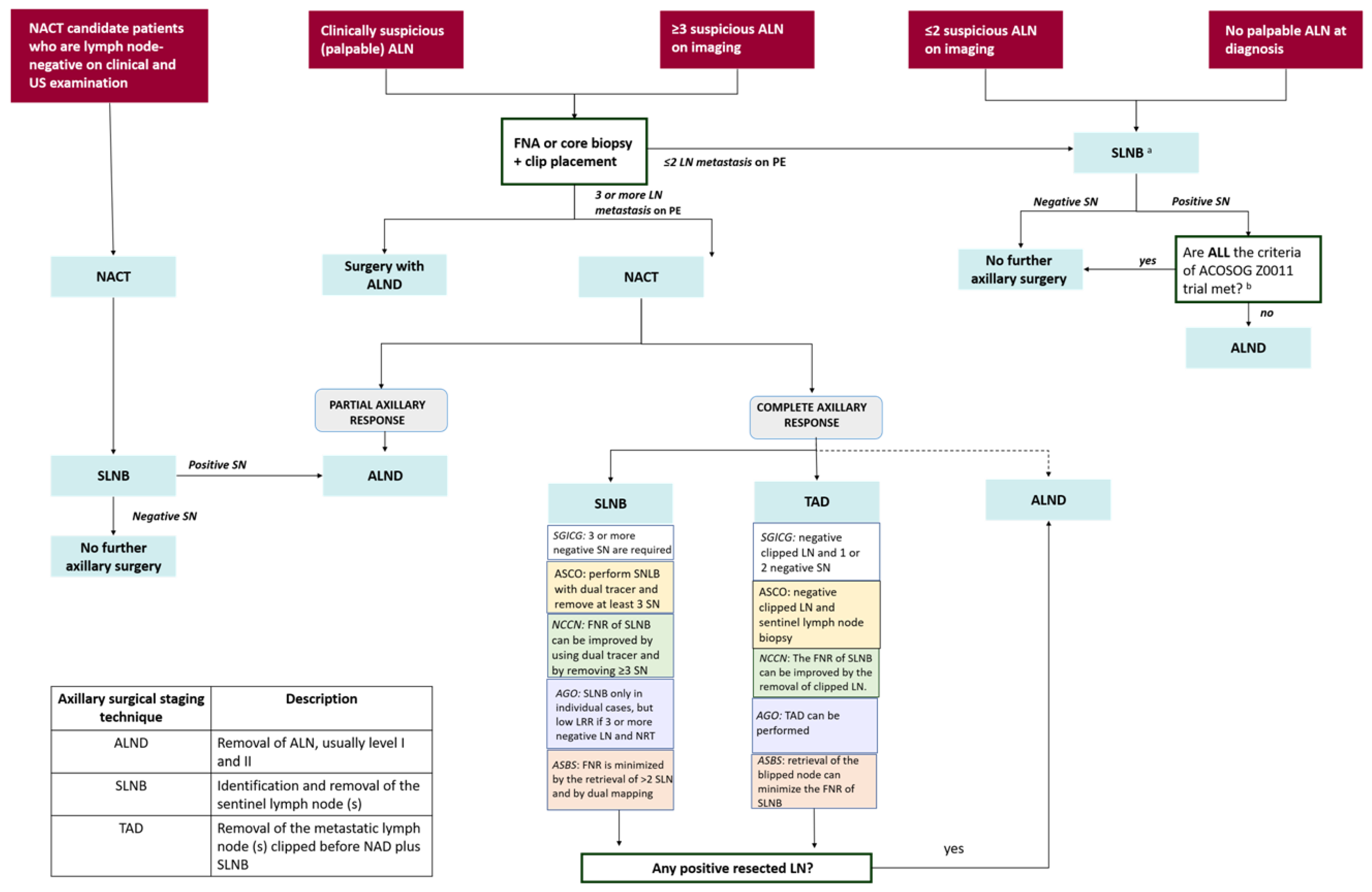
| Guidelines | Staging Recommendations in Cases of Conversion from Positive LN at Diagnosis to Negative LN after NACT | Level of Evidence/ Grade of Evidence |
|---|---|---|
| St. Gallen International Consensus Guidelines (SGICG) [34] | TAD may avoid ALND if the TAD after NACT removes the marked node and one or two additional sentinel nodes, and all are negative. SLNB after NACT could be adequate only for patients with at least 3 or more negative SLNs. | Not provided |
| American Society of Clinical Oncology (ASCO) [35] | SLNB is recommended to restage the axilla. Restaging can be achieved by placing a biopsy clip into the biopsied positive node at diagnosis and localizing it at surgery along with sentinel node biopsy or, in institutions where the use of biopsy clips for nodes is not available, by performing sentinel node biopsy with a dual tracer and excising at least three sentinel nodes. | Evidence quality: low; Strength of recommendation: weak |
| National Comprehensive Cancer Network (NCCN) [13] | Panel recommends pathologic confirmation of malignancy using ultrasound-guided fine-needle aspiration or core biopsy of suspicious nodes with clip placement. These patients may undergo SLNB with the removal of the clipped lymph node. A relatively high false-negative rate (FNR) (>10%) can be improved by marking biopsied lymph nodes to document their removal, using a dual tracer, and by removing 3 sentinel nodes (targeted ALND). When sentinel nodes are not successfully identified, the panel recommends level I and II axillary dissections be performed for axillary staging. | 2B |
| Breast Committee of the German Gynaecological Oncology Working Group (AGO) [36] | Suspicious lymph nodes should be evaluated before NACT by core needle biopsy and marker placement. SLNB only may be performed only in individual cases (AGO+/−); however, if 3 or more negative SLNs alone were removed and nodal radiotherapy was performed, the local recurrence rate is very low. ALND can be performed (AGO+) but may be harmful. TAD can be performed (AGO+). However, in case of extensive axillary tumor load (≥4 suspicious nodes) at presentation it should be used with caution (AGO+/−). | 2B |
| American Society of Breast Surgeons (ASBS) [37] | SLNB is suitable. The false-negative rate of SLNB is minimized by the retrieval of >2 SLN, by dual mapping, and by retrieval of the biopsied/clipped node. ALND is indicated for patients who are cN0 but SLN+. | Not provided |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Paola, V.; Mazzotta, G.; Conti, M.; Palma, S.; Orsini, F.; Mola, L.; Ferrara, F.; Longo, V.; Bufi, E.; D’Angelo, A.; et al. Image-Guided Localization Techniques for Metastatic Axillary Lymph Nodes in Breast Cancer; What Radiologists Should Know. Cancers 2023, 15, 2130. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15072130
Di Paola V, Mazzotta G, Conti M, Palma S, Orsini F, Mola L, Ferrara F, Longo V, Bufi E, D’Angelo A, et al. Image-Guided Localization Techniques for Metastatic Axillary Lymph Nodes in Breast Cancer; What Radiologists Should Know. Cancers. 2023; 15(7):2130. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15072130
Chicago/Turabian StyleDi Paola, Valerio, Giorgio Mazzotta, Marco Conti, Simone Palma, Federico Orsini, Laura Mola, Francesca Ferrara, Valentina Longo, Enida Bufi, Anna D’Angelo, and et al. 2023. "Image-Guided Localization Techniques for Metastatic Axillary Lymph Nodes in Breast Cancer; What Radiologists Should Know" Cancers 15, no. 7: 2130. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15072130