
Independent Tissue-Based Biomarkers in Endometrioid Endometrial Cancer: Tumor Budding in Microsatellite Instability and WHO Grading in Copy-Number-Low Patients
 , , , , , ,
, , , , , ,
Abstract
:Simple Summary
Abstract
1. Background
2. Methods
2.1. Study Cohort
2.2. Validation Cohorts
2.3. Histomorphologic Parameters Analyzed
2.4. Cutoff Determination
2.5. ITBCC Grading Scheme
2.6. Statistical Methods
2.7. Ethics
3. Results
3.1. Metrics of Histomorphologic Parameters
3.2. Mutual Correlations of Histomorphologic Parameters
3.3. Clinicopathologic Correlations of Histomorphologic Parameters
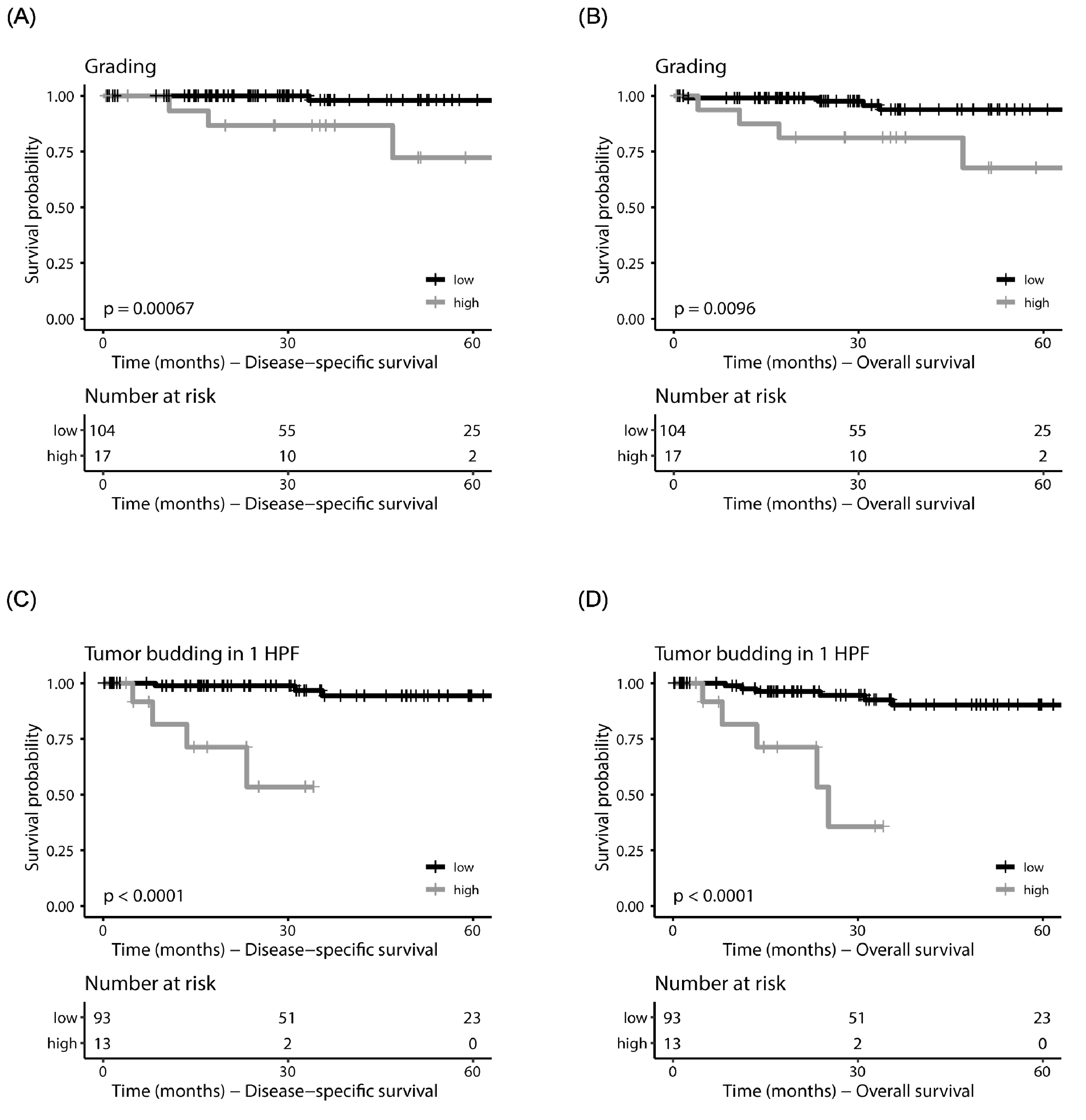
3.4. Prognostic Significance of Histomorphologic Parameters in Univariate Survival Analysis
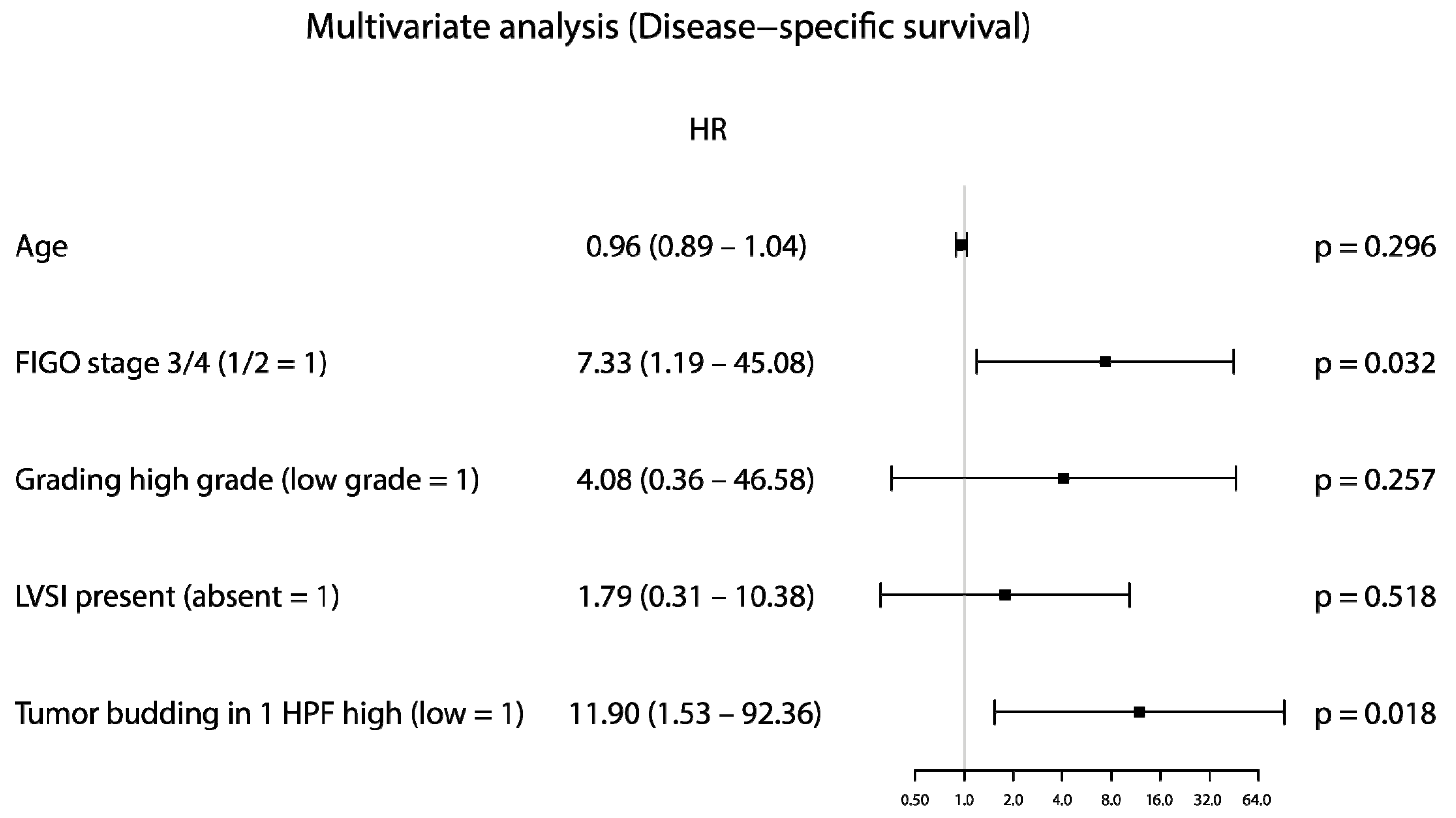
3.5. Prognostic Significance of Histomorphologic Parameters in Cox Proportional Hazard Analyses
3.6. Validation of the Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CNV | Copy number variation |
| CPTAC | Clinical Proteomic Tumor Analysis Consortium |
| DSS | Disease-specific survival |
| FIGO | Fédération Internationale de Gynécologie et d’Obstétrique |
| GDC | Genomic Data Commons |
| H&E | Hematoxylin and eosin |
| HPF | High-power field |
| LVSI | Lymphovascular space invasion |
| MELF | Microcystic, elongated, fragmented |
| MSI | Microsatellite instability |
| OS | Overall survival |
| PFS | Progression-free survival |
| POLE | Polymerase ε |
| TB | Tumor budding |
| TCGA | The Cancer Genome Atlas |
| TIL | Tumor infiltrating lymphocytes |
| TSR | Tumor–stroma ratio/stromal desmoplasia |
| UCEC | Uterine Corpus Endometrial Carcinoma |
| WHO | World Health Organization |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carter, J.; Pather, S. An Overview of Uterine Cancer and Its Management. Expert Rev. Anticancer Ther. 2006, 6, 33–42. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research Network; Kandoth, C.; Schultz, N.; Cherniack, A.D.; Akbani, R.; Liu, Y.; Shen, H.; Robertson, A.G.; Pashtan, I.; Shen, R.; et al. Integrated Genomic Characterization of Endometrial Carcinoma. Nature 2013, 497, 67–73. [Google Scholar]
- Talhouk, A.; McConechy, M.K.; Leung, S.; Li-Chang, H.H.; Kwon, J.S.; Melnyk, N.; Yang, W.; Senz, J.; Boyd, N.; Karnezis, A.N.; et al. A Clinically Applicable Molecular-Based Classification for Endometrial Cancers. Br. J. Cancer 2015, 113, 299–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexa, M.; Hasenburg, A.; Battista, M.J. The TCGA Molecular Classification of Endometrial Cancer and Its Possible Impact on Adjuvant Treatment Decisions. Cancers 2021, 13, 1478. [Google Scholar] [CrossRef] [PubMed]
- Pasanen, A.; Loukovaara, M.; Ahvenainen, T.; Vahteristo, P.; Bützow, R. Differential Impact of Clinicopathological Risk Factors within the 2 Largest ProMisE Molecular Subgroups of Endometrial Carcinoma. PLoS ONE 2021, 16, e0253472. [Google Scholar] [CrossRef]
- Wang, M.; Hui, P. A Timely Update of Immunohistochemistry and Molecular Classification in the Diagnosis and Risk Assessment of Endometrial Carcinomas. Arch. Pathol. Lab. Med. 2021, 145, 1367–1378. [Google Scholar] [CrossRef]
- Li, R.; Shinde, A.; Han, E.; Lee, S.; Beriwal, S.; Harkenrider, M.; Kamrava, M.; Chen, Y.-J.; Glaser, S. A Proposal for a New Classification of “Unfavorable Risk Criteria” in Patients with Stage I Endometrial Cancer. Int. J. Gynecol. Cancer 2019, 29, 1086–1093. [Google Scholar] [CrossRef] [Green Version]
- Nasioudis, D.; Oh, J.; Ko, E.M.; Haggerty, A.F.; Cory, L.; Ii, R.L.G.; Kim, S.H.; Morgan, M.A.; Latif, N.A. Adjuvant Chemotherapy for Stage I High-Intermediate Risk Endometrial Carcinoma with Lymph-Vascular Invasion. Int. J. Gynecol. Cancer 2022, 32, 1129–1134. [Google Scholar] [CrossRef]
- Randall, M.E.; Filiaci, V.; McMeekin, D.S.; von Gruenigen, V.; Huang, H.; Yashar, C.M.; Mannel, R.S.; Kim, J.-W.; Salani, R.; DiSilvestro, P.A.; et al. Phase III Trial: Adjuvant Pelvic Radiation Therapy Versus Vaginal Brachytherapy Plus Paclitaxel/Carboplatin in High-Intermediate and High-Risk Early Stage Endometrial Cancer. J. Clin. Oncol. 2019, 37, 1810–1818. [Google Scholar] [CrossRef]
- Concin, N.; Matias-Guiu, X.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.; Bosse, T.; Chargari, C.; Fagotti, A.; et al. ESGO/ESTRO/ESP Guidelines for the Management of Patients with Endometrial Carcinoma. Int. J. Gynecol. Cancer 2021, 31, 12–39. [Google Scholar] [CrossRef] [PubMed]
- Cosgrove, C.M.; Barrington, D.; Backes, F.J. Impact of Molecular Classification on Treatment Paradigms in Uterine Cancers. Curr. Oncol. Rep. 2021, 23, 75. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; Chen, H.; Liu, Y.; Niu, L.; Jin, L.; Li, D.; Song, L.; Shang, L.; Lin, X.; Wang, F.; et al. Is Lymph Node Dissection Mandatory among Early Stage Endometrial Cancer Patients? A Retrospective Study. BMC Women′s Health 2020, 20, 258. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Liang, C.; Chen, M.; Su, W. Association between Tumor–Stroma Ratio and Prognosis in Solid Tumor Patients: A Systematic Review and Meta-Analysis. Oncotarget 2016, 7, 68954–68965. [Google Scholar] [CrossRef] [Green Version]
- Ahn, B.; Chae, Y.-S.; Kim, C.H.; Lee, Y.; Lee, J.H.; Kim, J.Y. Tumor Microenvironmental Factors Have Prognostic Significances in Advanced Gastric Cancer. APMIS 2018, 126, 814–821. [Google Scholar] [CrossRef]
- van Wyk, H.C.; Roseweir, A.; Alexander, P.; Park, J.H.; Horgan, P.G.; McMillan, D.C.; Edwards, J. The Relationship Between Tumor Budding, Tumor Microenvironment, and Survival in Patients with Primary Operable Colorectal Cancer. Ann. Surg. Oncol. 2019, 26, 4397–4404. [Google Scholar] [CrossRef] [PubMed]
- Lugli, A.; Zlobec, I.; Berger, M.D.; Kirsch, R.; Nagtegaal, I.D. Tumour Budding in Solid Cancers. Nat. Rev. Clin. Oncol. 2021, 18, 101–115. [Google Scholar] [CrossRef]
- Ailia, M.J.; Thakur, N.; Chong, Y.; Yim, K. Tumor Budding in Gynecologic Cancer as a Marker for Poor Survival: A Systematic Review and Meta-Analysis of the Perspectives of Epithelial-Mesenchymal Transition. Cancers 2022, 14, 1431. [Google Scholar] [CrossRef]
- Rau, T.T.; Bettschen, E.; Büchi, C.; Christe, L.; Rohner, A.; Müller, M.D.; Carlson, J.W.; Imboden, S.; Zlobec, I. Prognostic Impact of Tumor Budding in Endometrial Carcinoma within Distinct Molecular Subgroups. Mod. Pathol. 2021, 34, 222–232. [Google Scholar] [CrossRef]
- Qi, X.; Zhu, L.; Zhang, B. Clinicopathologic Association and Prognostic Impact of Microcystic, Elongated and Fragmented Pattern Invasion, Combined with Tumor Budding in Endometrioid Endometrial Cancer. J. Obstet. Gynaecol. Res. 2022, 48, 2431–2441. [Google Scholar] [CrossRef]
- Okcu, O.; Şen, B.; Aşkan, G.; Öztürk, Ç.; Öztürk, S.D.; Bedir, R. Tumor Budding Is an Independent Prognostic Factor to Predict Overall Survival in Endometrial Endometrioid Carcinoma: A Retrospective Study. Int. J. Surg. Pathol. 2023, 31, 26–37. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Shen, Z.; Deng, Z.; Mei, L. Impact of Tumor–Stroma Ratio on the Prognosis of Colorectal Cancer: A Systematic Review. Front. Oncol. 2021, 11, 738080. [Google Scholar] [CrossRef] [PubMed]
- Dolens, E.d.S.; Dourado, M.R.; Almangush, A.; Salo, T.A.; Gurgel Rocha, C.A.; da Silva, S.D.; Brennan, P.A.; Coletta, R.D. The Impact of Histopathological Features on the Prognosis of Oral Squamous Cell Carcinoma: A Comprehensive Review and Meta-Analysis. Front. Oncol. 2021, 11, 784924. [Google Scholar] [CrossRef] [PubMed]
- Maibach, F.; Sadozai, H.; Seyed Jafari, S.M.; Hunger, R.E.; Schenk, M. Tumor-Infiltrating Lymphocytes and Their Prognostic Value in Cutaneous Melanoma. Front. Immunol. 2020, 11, 2105. [Google Scholar] [CrossRef] [PubMed]
- Panayiotou, H.; Orsi, N.M.; Thygesen, H.H.; Wright, A.I.; Winder, M.; Hutson, R.; Cummings, M. The Prognostic Significance of Tumour-Stroma Ratio in Endometrial Carcinoma. BMC Cancer 2015, 15, 955. [Google Scholar] [CrossRef] [Green Version]
- Santoro, A.; Angelico, G.; Travaglino, A.; Inzani, F.; Arciuolo, D.; Valente, M.; D’Alessandris, N.; Scaglione, G.; Fiorentino, V.; Raffone, A.; et al. New Pathological and Clinical Insights in Endometrial Cancer in View of the Updated ESGO/ESTRO/ESP Guidelines. Cancers 2021, 13, 2623. [Google Scholar] [CrossRef]
- Grossman, R.L.; Heath, A.P.; Ferretti, V.; Varmus, H.E.; Lowy, D.R.; Kibbe, W.A.; Staudt, L.M. Toward a Shared Vision for Cancer Genomic Data. N. Engl. J. Med. 2016, 375, 1109–1112. [Google Scholar] [CrossRef]
- Willvonseder, B.; Stögbauer, F.; Steiger, K.; Jesinghaus, M.; Kuhn, P.-H.; Brambs, C.; Engel, J.; Bronger, H.; Schmidt, G.P.; Haller, B.; et al. The Immunologic Tumor Microenvironment in Endometrioid Endometrial Cancer in the Morphomolecular Context: Mutual Correlations and Prognostic Impact Depending on Molecular Alterations. Cancer Immunol. Immunother. 2021, 70, 1679–1689. [Google Scholar] [CrossRef] [PubMed]
- Dou, Y.; Kawaler, E.A.; Cui Zhou, D.; Gritsenko, M.A.; Huang, C.; Blumenberg, L.; Karpova, A.; Petyuk, V.A.; Savage, S.R.; Satpathy, S.; et al. Proteogenomic Characterization of Endometrial Carcinoma. Cell 2020, 180, 729–748.e26. [Google Scholar] [CrossRef]
- Colaprico, A.; Silva, T.C.; Olsen, C.; Garofano, L.; Cava, C.; Garolini, D.; Sabedot, T.S.; Malta, T.M.; Pagnotta, S.M.; Castiglioni, I.; et al. TCGAbiolinks: An R/Bioconductor Package for Integrative Analysis of TCGA Data. Nucleic Acids Res. 2016, 44, e71. [Google Scholar] [CrossRef]
- Silva, T.C.; Colaprico, A.; Olsen, C.; D’Angelo, F.; Bontempi, G.; Ceccarelli, M.; Noushmehr, H. Analyze Cancer Genomics and Epigenomics Data Using Bioconductor Packages. F1000Research 2016, 5, 1542. [Google Scholar] [CrossRef]
- Mounir, M.; Lucchetta, M.; Silva, T.C.; Olsen, C.; Bontempi, G.; Chen, X.; Noushmehr, H.; Colaprico, A.; Papaleo, E. New Functionalities in the TCGAbiolinks Package for the Study and Integration of Cancer Data from GDC and GTEx. PLoS Comput. Biol. 2019, 15, e1006701. [Google Scholar] [CrossRef] [Green Version]
- Clark, K.; Vendt, B.; Smith, K.; Freymann, J.; Kirby, J.; Koppel, P.; Moore, S.; Phillips, S.; Maffitt, D.; Pringle, M.; et al. The Cancer Imaging Archive (TCIA): Maintaining and Operating a Public Information Repository. J. Digit. Imaging 2013, 26, 1045–1057. [Google Scholar] [CrossRef] [Green Version]
- WHO Classification of Tumours Editorial Board. Female Genital Tumours; International Agency for Research on Cancer: Lyon, France, 2020; ISBN 9789283245049. [Google Scholar]
- Kemi, N.; Eskuri, M.; Herva, A.; Leppänen, J.; Huhta, H.; Helminen, O.; Saarnio, J.; Karttunen, T.J.; Kauppila, J.H. Tumour-Stroma Ratio and Prognosis in Gastric Adenocarcinoma. Br. J. Cancer 2018, 119, 435–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hendry, S.; Salgado, R.; Gevaert, T.; Russell, P.A.; John, T.; Thapa, B.; Christie, M.; van de Vijver, K.; Estrada, M.V.; Gonzalez-Ericsson, P.I.; et al. Assessing Tumor-Infiltrating Lymphocytes in Solid Tumors: A Practical Review for Pathologists and Proposal for a Standardized Method From the International Immunooncology Biomarkers Working Group: Part 1: Assessing the Host Immune Response, TILs in Invasive Breast Carcinoma and Ductal Carcinoma In Situ, Metastatic Tumor Deposits and Areas for Further Research. Adv. Anat. Pathol. 2017, 24, 235–251. [Google Scholar] [PubMed] [Green Version]
- Murray, S.K.; Young, R.H.; Scully, R.E. Unusual Epithelial and Stromal Changes in Myoinvasive Endometrioid Adenocarcinoma: A Study of Their Frequency, Associated Diagnostic Problems, and Prognostic Significance. Int. J. Gynecol. Pathol. 2003, 22, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Väyrynen, J.P.; Tuomisto, A.; Klintrup, K.; Mäkelä, J.; Karttunen, T.J.; Mäkinen, M.J. Detailed Analysis of Inflammatory Cell Infiltration in Colorectal Cancer. Br. J. Cancer 2013, 109, 1839–1847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bankhead, P.; Loughrey, M.B.; Fernández, J.A.; Dombrowski, Y.; McArt, D.G.; Dunne, P.D.; McQuaid, S.; Gray, R.T.; Murray, L.J.; Coleman, H.G.; et al. QuPath: Open Source Software for Digital Pathology Image Analysis. Sci. Rep. 2017, 7, 16878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Budczies, J.; Klauschen, F.; Sinn, B.V.; Győrffy, B.; Schmitt, W.D.; Darb-Esfahani, S.; Denkert, C. Cutoff Finder: A Comprehensive and Straightforward Web Application Enabling Rapid Biomarker Cutoff Optimization. PLoS ONE 2012, 7, e51862. [Google Scholar] [CrossRef] [Green Version]
- Lugli, A.; Kirsch, R.; Ajioka, Y.; Bosman, F.; Cathomas, G.; Dawson, H.; El Zimaity, H.; Fléjou, J.F.; Hansen, T.P.; Hartmann, A.; et al. Recommendations for Reporting Tumor Budding in Colorectal Cancer Based on the International Tumor Budding Consensus Conference (ITBCC) 2016. Mod. Pathol. 2017, 30, 1299–1311. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Raffone, A.; Travaglino, A.; Mascolo, M.; Carbone, L.; Guida, M.; Insabato, L.; Zullo, F. TCGA Molecular Groups of Endometrial Cancer: Pooled Data about Prognosis. Gynecol. Oncol. 2019, 155, 374–383. [Google Scholar] [CrossRef] [PubMed]
- Grigore, A.D.; Jolly, M.K.; Jia, D.; Farach-Carson, M.C.; Levine, H. Tumor Budding: The Name Is EMT. Partial EMT. J. Clin. Med. Res. 2016, 5, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pölcher, M.; Rottmann, M.; Brugger, S.; Mahner, S.; Dannecker, C.; Kiechle, M.; Brambs, C.; Grab, D.; Anthuber, C.; von Koch, F.; et al. Lymph Node Dissection in Endometrial Cancer and Clinical Outcome: A Population-Based Study in 5546 Patients. Gynecol. Oncol. 2019, 154, 65–71. [Google Scholar] [CrossRef]
- Oaknin, A.; Bosse, T.J.; Creutzberg, C.L.; Giornelli, G.; Harter, P.; Joly, F.; Lorusso, D.; Marth, C.; Makker, V.; Mirza, M.R.; et al. Endometrial Cancer: ESMO Clinical Practice Guideline for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2022, 33, 860–877. [Google Scholar] [CrossRef]
- Kong, T.W.; Chang, S.J.; Paek, J.; Lee, Y.; Chun, M.; Ryu, H.S. Risk Group Criteria for Tailoring Adjuvant Treatment in Patients with Endometrial Cancer: A Validation Study of the Gynecologic Oncology Group Criteria. J. Gynecol. Oncol. 2015, 26, 32–39. [Google Scholar] [CrossRef] [Green Version]
- Stögbauer, F.; Lautizi, M.; Kriegsmann, M.; Winter, H.; Muley, T.; Kriegsmann, K.; Jesinghaus, M.; Baumbach, J.; Schüffler, P.; Weichert, W.; et al. Tumour Cell Budding and Spread through Air Spaces in Squamous Cell Carcinoma of the Lung—Determination and Validation of Optimal Prognostic Cut-Offs. Lung Cancer 2022, 169, 1–12. [Google Scholar] [CrossRef]
- Karlberg, M.; Stenstedt, K.; Hallström, M.; Ragnhammar, P.; Lenander, C.; Edler, D. Tumor Budding Mismatch Repair Status in Colorectal Cancer—An Exploratory Analysis. Anticancer Res. 2018, 38, 4713–4721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zlobec, I.; Lugli, A. Tumour Budding in Colorectal Cancer: Molecular Rationale for Clinical Translation. Nat. Rev. Cancer 2018, 18, 203–204. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M.; Kaizaki, Y.; Kogami, A.; Hara, T.; Sakai, Y.; Tsuchida, T. Prognostic Significance of Tumor Budding, Poorly Differentiated Cluster, and Desmoplastic Reaction in Endometrioid Endometrial Carcinomas. J. Obstet. Gynaecol. Res. 2021, 47, 3958–3967. [Google Scholar] [CrossRef]
- Adamczyk-Gruszka, O.; Horecka-Lewitowicz, A.; Gruszka, J.; Wawszczak-Kasza, M.; Strzelecka, A.; Lewitowicz, P. FGFR-2 and Epithelial-Mesenchymal Transition in Endometrial Cancer. J. Clin. Med. Res. 2022, 11, 5416. [Google Scholar] [CrossRef]
- Park, J.Y.; Hong, D.G.; Chong, G.O.; Park, J.Y. Tumor Budding Is a Valuable Diagnostic Parameter in Prediction of Disease Progression of Endometrial Endometrioid Carcinoma. Pathol. Oncol. Res. 2019, 25, 723–730. [Google Scholar] [CrossRef] [PubMed]
- Almangush, A.; Youssef, O.; Pirinen, M.; Sundström, J.; Leivo, I.; Mäkitie, A.A. Does Evaluation of Tumour Budding in Diagnostic Biopsies Have a Clinical Relevance? A Systematic Review. Histopathology 2019, 74, 536–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| TCGA | Munich | CPTAC | ||||
|---|---|---|---|---|---|---|
| Number of Patients with Available Data | % | Number of Patients with Available Data | % | Number of Patients with Available Data | % | |
| Age (median, interquartile range) | 61.0, 13.0 | 69.7, 11.8 | 64.2, 5.7 | |||
| N/A | 2 | 0 | 0 | |||
| FIGO stage | ||||||
| I | 172 | 75.4 | 28 | 59.6 | 21 | 84.0 |
| II | 19 | 8.3 | 9 | 19.1 | 2 | 8.0 |
| III | 34 | 14.9 | 6 | 12.8 | 2 | 8.0 |
| IV | 3 | 1.3 | 4 | 8.5 | 0 | 0 |
| Grading | ||||||
| G1 | 61 | 26.8 | 9 | 19.1 | 8 | 32.0 |
| G2 | 106 | 46.5 | 14 | 29.8 | 13 | 52.0 |
| G3 | 61 | 26.8 | 24 | 51.1 | 4 | 16.0 |
| pT | ||||||
| 1 | 120 | 75.9 | 29 | 61.7 | 20 | 83.3 |
| 2 | 23 | 14.6 | 11 | 23.4 | 2 | 8.3 |
| 3 | 15 | 9.5 | 7 | 14.9 | 2 | 8.3 |
| 4 | 0 | 0 | 0 | 0 | 0 | 0 |
| N/A | 70 | 0 | 0 | 1 | ||
| pN | ||||||
| N0 | 187 | 85.0 | 43 | 91.5 | 16 | 66.7 |
| N1/N2 | 21 | 9.5 | 4 | 8.5 | 0 | 0 |
| NX | 12 | 5.5 | 0 | 0 | 8 | 33.3 |
| N/A | 8 | 0 | 0 | 1 | ||
| Lymphovascular space invasion | ||||||
| absent | 187 | 82.0 | 33 | 75.0 | 17 | 94.4 |
| present | 41 | 18.0 | 11 | 25.0 | 1 | 5.6 |
| N/A | 0 | 3 | 7 | |||
| Perineural invasion | ||||||
| absent | 226 | 99.1 | 42 | 95.5 | 18 | 100 |
| present | 2 | 0.9 | 2 | 4.5 | 0 | |
| N/A | 0 | 0 | 7 | |||
| Residual tumor | ||||||
| R0 | 163 | 88.1 | 41 | 89.1 | 14 | 60.9 |
| R1/R2 | 10 | 5.0 | 3 | 6.5 | 2 | 8.6 |
| RX | 12 | 6.5 | 2 | 4.3 | 7 | 30.4 |
| N/A | 43 | 1 | 2 | |||
| Subtype | ||||||
| MSI | 107 | 46.9 | 44 | 100 | 25 | 100 |
| CN-LOW | 121 | 53.1 | - | - | - | - |
| Grading | TB in 1 HPF | TB in 10 HPF | Minimal Cell Nest Size | TSR | TIL | MELF | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Low | High | p | Low | High | p | Low | High | p | Small | Big | p | Low | High | p | Low | High | p | Absent | Present | p | |
| Age (median; IQR) | 60 (12.5) | 62 (17) | 0.632 | 61 (12.5) | 60 (14.5) | 0.446 | 60.5 (13) | 64.5 (19.5) | 0.899 | 59.5 (14.5) | 61 (12.25) | 0.308 | 61.5 (17.25) | 61 (13) | 0.844 | 61 (13) | 60.5 (10.75) | 0.974 | 61 (15) | 61 (7.5) | 0.919 |
| N/A | 2 | 2 | |||||||||||||||||||
| pT | |||||||||||||||||||||
| 1 | 90 (80.4) | 30 (65.2) | 0.108 | 110 (76.4) | 10 (71.4) | 0.259 | 114 (78.1) | 6 (50.0) | 0.045 | 17 (70.8) | 103 (76.9) | 0.401 | 5 (50.0) | 115 (77.7) | 0.012 | 115 (76.2) | 5 (71.4) | 0.194 | 103 (76.9) | 30 (69.8) | 0.227 |
| 2 | 14 (12.5) | 9 (19.6) | 22 (15.3) | 1 (7.1) | 20 (13.7) | 3 (25.0) | 3 (12.5) | 20 (14.9) | 1 (10.0) | 22 (14.9) | 23 (15.2) | 0 (0.0) | 20 (14.9) | 5 (11.6) | |||||||
| 3 | 8 (7.1) | 7 (15.2) | 12 (8.3) | 3 (21.4) | 12 (8.2) | 3 (25.0) | 4 (16.7) | 11 (8.2) | 4 (40.0) | 11 (7.4) | 13 (8.6) | 2 (28.6) | 11 (8.2) | 8 (18.6) | |||||||
| N/A | 70 | 70 | |||||||||||||||||||
| pN | |||||||||||||||||||||
| 0 | 142 (88.8) | 45 (75.0) | 0.001 | 176 (87.6) | 11 (57.9) | <0.001 | 177 (87.2) | 10 (58.8) | 0.007 | 23 (67.6) | 164 (88.2) | 0.003 | 12 (75.0) | 175 (85.8) | 0.249 | 179 (85.2) | 8 (80.0) | 0.324 | 164 (86.3) | 41 (77.4) | 0.007 |
| + | 8 (5.0) | 13 (21.7) | 14 (7.0) | 7 (36.8) | 16 (7.9) | 5 (29.4) | 9 (26.5) | 12 (6.5) | 3 (18.8) | 18 (8.8) | 19 (9.0) | 2 (20.0) | 14 (7.4) | 11 (20.8) | |||||||
| X | 10 (6.2) | 2 (3.3) | 11 (5.5) | 1 (5.3) | 10 (4.9) | 2 (11.8) | 2 (5.9) | 10 (5.4) | 1 (6.2) | 11 (5.4) | 12 (5.7) | 0 (0.0) | 12 (6.3) | 1 (1.9) | |||||||
| N/A | 8 | 8 | |||||||||||||||||||
| FIGO stage | |||||||||||||||||||||
| 1/2 | 146 (87.4) | 45 (73.8) | 0.024 | 178 (85.6) | 13 (65.0) | 0.026 | 178 (84.8) | 13 (72.2) | 0.182 | 27 (75.0) | 164 (85.4) | 0.139 | 10 (62.5) | 181 (85.4) | 0.028 | 185 (84.9) | 6 (60.0) | 0.060 | 169 (85.8) | 39 (72.2) | 0.028 |
| 3/4 | 21 (12.6) | 16 (26.2) | 30 (14.4) | 7 (35.0) | 32 (15.2) | 5 (27.8) | 9 (25.0) | 28 (14.6) | 6 (37.5) | 31 (14.6) | 33 (15.1) | 4 (40.0) | 28 (14.2) | 15 (27.8) | |||||||
| Grading | |||||||||||||||||||||
| Low-grade | - | - | - | 165 (79.3) | 2 (10.0) | <0.001 | 164 (78.1) | 3 (16.7) | <0.001 | 9 (25.0) | 158 (82.3) | <0.001 | 11 (68.8) | 156 (73.6) | 0.770 | 162 (74.3) | 5 (50.0) | 0.137 | 144 (73.1) | 37 (68.5) | >0.999 |
| High-grade | - | - | 43 (20.7) | 18 (90.0) | 46 (21.9) | 15 (83.3) | 27 (75.0) | 34 (17.7) | 5 (31.2) | 56 (26.4) | 56 (25.7) | 5 (50.0) | 53 (26.9) | 17 (31.5) | |||||||
| Lymphovascular space invasion | |||||||||||||||||||||
| Absent | 146 (87.4) | 41 (67.2) | <0.001 | 174 (83.7) | 13 (65.0) | 0.061 | 177 (84.3) | 10 (55.6) | 0.006 | 25 (69.4) | 162 (84.4) | 0.055 | 11 (68.8) | 176 (83.0) | 0.175 | 178 (81.7) | 9 (90.0) | 0.695 | 164 (83.2) | 44 (81.5) | 0.322 |
| Present | 21 (12.6) | 20 (32.8) | 34 (16.3) | 7 (35.0) | 33 (15.7) | 8 (44.4) | 11 (30.6) | 30 (15.6) | 5 (31.2) | 36 (17.0) | 40 (18.3) | 1 (10.0) | 33 (16.8) | 10 (18.5) | |||||||
| Perineural invasion | |||||||||||||||||||||
| Absent | 167 (100) | 59 (96.7) | 0.071 | 207 (99.5) | 19 (95.0) | 0.168 | 209 (99.5) | 17 (94.4) | 0.152 | 35 (97.2) | 191 (99.5) | 0.291 | 15 (93.8) | 211 (99.5) | 0.136 | 216 (99.1) | 10 (100.0) | > 0.999 | 195 (99.0) | 54 (100.0) | >0.999 |
| Present | 0 (0.0) | 2 (3.3) | 1 (0.5) | 1 (5.0) | 1 (0.5) | 1 (5.6) | 1 (2.8) | 1 (0.5) | 1 (6.2) | 1 (0.5) | 2 (0.9) | 0 (0.0) | 2 (1.0) | 0 (0.0) | |||||||
| Residual tumor | |||||||||||||||||||||
| R0 | 125 (91.9) | 38 (77.6) | <0.001 | 152 (90.5) | 11 (64.7) | <0.001 | 154 (90.6) | 9 (60.0) | 0.002 | 21 (72.4) | 142 (91.0) | 0.002 | 13 (92.9) | 150 (87.7) | 0.511 | 156 (89.1) | 7 (70.0) | 0.101 | 144 (90.0) | 38 (84.4) | 0.048 |
| R1/R2 | 2 (1.5) | 8 (16.3) | 5 (3.0) | 5 (29.4) | 6 (3.5) | 4 (26.7) | 6 (20.7) | 4 (2.6) | 1 (7.1) | 9 (5.3) | 9 (5.1) | 1 (10.0) | 6 (3.8) | 5 (11.1) | |||||||
| RX | 9 (6.6) | 3 (6.1) | 11 (6.5) | 1 (5.9) | 10 (5.9) | 2 (13.3) | 2 (6.9) | 10 (6.4) | 0 (0.0) | 12 (7.0) | 10 (5.7) | 2 (20.0) | 10 (6.2) | 2 (4.4) | |||||||
| N/A | 43 | 43 | |||||||||||||||||||
| Subtype | |||||||||||||||||||||
| MSI | 63 (37.7) | 44 (72.1) | <0.001 | 93 (44.7) | 14 (70.0) | 0.036 | 93 (44.3) | 14 (77.8) | 0.007 | 25 (69.4) | 82 (42.7) | 0.004 | 7 (43.8) | 100 (47.2) | >0.999 | 99 (45.4) | 8 (80.0) | 0.049 | 92 (46.7) | 28 (51.9) | 0.846 |
| CN-LOW | 104 (62.3) | 17 (27.9) | 115 (55.3) | 6 (30.0) | 117 (55.7) | 4 (22.2) | 11 (30.6) | 110 (57.3) | 9 (56.2) | 112 (52.8) | 119 (54.6) | 2 (20.0) | 105 (53.3) | 26 (48.1) | |||||||
| Depth of myometrial invasion | |||||||||||||||||||||
| Inner half | 113 (75.3) | 19 (40.4) | <0.001 | 123 (68.0) | 9 (56.2) | 0.407 | 127 (69.0) | 5 (38.5) | 0.033 | 14 (46.7) | 118 (70.7) | 0.019 | 8 (57.1) | 124 (67.8) | 0.556 | 128 (67.4) | 4 (57.1) | 0.686 | 120 (69.4) | 23 (51.1) | 0.056 |
| Outer half | 37 (24.7) | 28 (59.6) | 58 (32.0) | 7 (43.8) | 57 (31.0) | 8 (61.5) | 16 (53.3) | 49 (29.3) | 6 (42.9) | 59 (32.2) | 62 (32.6) | 3 (42.9) | 53 (30.6) | 22 (48.9) | |||||||
| N/A | 31 | ||||||||||||||||||||
| Grading (Low vs. High) | TB in 1 HPF (Low vs. High) | TB in 10 HPF (Low vs. High) | MCNS (Low vs. High) | TSR (Low vs. High) | TIL (Low vs. High) | MELF (Absent vs. Present) | Lymphovascular Space Invasion (Absent vs. Present) | ITBCC Grading Scheme (Bd1 vs. Bd2 vs. Bd3) | ||
|---|---|---|---|---|---|---|---|---|---|---|
| TCGA | DSS | <0.001 | <0.001 | <0.001 | <0.001 | 0.022 | 0.276 | 0.028 | <0.001 | <0.001 |
| OS | <0.001 | <0.001 | <0.001 | <0.001 | 0.014 | 0.077 | 0.549 | 0.078 | <0.001 | |
| PFS | 0.011 | <0.001 | 0.001 | 0.066 | 0.879 | 0.813 | 0.987 | 0.034 | 0.026 | |
| MSI | DSS | 0.007 | <0.001 | <0.001 | 0.002 | 0.004 | 0.503 | 0.014 | 0.008 | 0.001 |
| OS | 0.067 | <0.001 | <0.001 | <0.001 | 0.034 | 0.403 | 0.217 | 0.115 | <0.001 | |
| PFS | 0.045 | <0.001 | 0.007 | 0.066 | 0.334 | 0.230 | 0.258 | 0.339 | 0.064 | |
| CN-low | DSS | <0.001 | 0.061 | 0.043 | 0.212 | 0.735 | <0.001 | 0.666 | 0.041 | 0.168 |
| OS | 0.010 | 0.377 | 0.326 | 0.723 | 0.215 | <0.001 | 0.644 | 0.523 | 0.682 | |
| PFS | 0.240 | 0.177 | 0.115 | 0.692 | 0.366 | 0.034 | 0.281 | 0.049 | 0.483 | |
| TB in 1 HPF | TB in 10 HPF | Minimal Cell Nest Size | |||||||
|---|---|---|---|---|---|---|---|---|---|
| HR | p | HR | p | HR | p | ||||
| TCGA | Age | 0.95 (0.90–1.01) | 0.091 | Age | 0.95 (0.89–1.01) | 0.085 | Age | 0.94 (0.88–1.00) | 0.061 |
| FIGO stage 3/4 (1/2 = 1) | 2.72 (0.70–10.52) | 0.148 | FIGO stage 3/4 (1/2 = 1) | 3.14 (0.83–11.91) | 0.093 | FIGO stage 3/4 (1/2 = 1) | 3.76 (1.06–13.36) | 0.040 | |
| Grading high-grade (low-grade = 1) | 7.60 (1.47–39.22) | 0.015 | Grading high-grade (low-grade = 1) | 9.03 (1.81–45.17) | 0.007 | Grading high-grade (low-grade = 1) | 9.89 (1.85–52.91) | 0.007 | |
| LVSI present (absent = 1) | 5.83 (1.57–21.66) | 0.008 | LVSI present (absent = 1) | 5.22 (1.43–19.00) | 0.012 | LVSI present (absent = 1) | 5.38 (1.48–19.58) | 0.011 | |
| TB in 1 HPF high (low = 1) | 3.41 (0.76–15.36) | 0.111 | TB in 10 HPF high (low = 1) | 2.21 (0.48–10.31) | 0.311 | Minimal cell nest size (absent = 1) | 1.31 (0.29–5.90) | 0.726 | |
| MSI | Age | 0.96 (0.89–1.04) | 0.296 | Age | 0.97 (0.89–1.05) | 0.414 | Age | 0.98 (0.90–1.06) | 0.576 |
| FIGO stage 3/4 (1/2 = 1) | 7.33 (1.19–45.08) | 0.032 | FIGO stage 3/4 (1/2 = 1) | 6.75 (1.16–39.14) | 0.033 | FIGO stage 3/4 (1/2 = 1) | 7.60 (1.40–41.25) | 0.019 | |
| Grading high-grade (low-grade = 1) | 4.08 (0.36–46.58) | 0.257 | Grading high grade (low-grade = 1) | 5.66 (0.57–55.89) | 0.138 | Grading high-grade (low-grade = 1) | 4.46 (0.40–49.44) | 0.223 | |
| LVSI present (absent = 1) | 1.79 (0.31–10.38) | 0.518 | LVSI present (absent = 1) | 1.62 (0.27–9.80) | 0.598 | LVSI present (absent = 1) | 2.68 (0.56–12.87) | 0.219 | |
| TB in 1 HPF high (low = 1) | 11.90 (1.53–92.36) | 0.018 | TB in 10 HPF high (low = 1) | 6.48 (0.89–46.94) | 0.064 | Minimal cell nest size (absent = 1) | 3.72 (0.58–24.04) | 0.167 | |
| CN-low | Age | 0.81 (0.67–0.99) | 0.039 | Age | 0.81 (0.67–0.99) | 0.039 | Age | 0.82 (0.67–0.99) | 0.036 |
| FIGO stage 3/4 (1/2 = 1) | 0.31 (0.00–73.02) | 0.676 | FIGO stage 3/4 (1/2 = 1) | 0.31 (0.00–68.35) | 0.669 | FIGO stage 3/4 (1/2 = 1) | 0.91 (0.00–1437.06) | 0.979 | |
| Grading high-grade (low-grade = 1) | 37.78 (1.88–757.32) | 0.018 | Grading high-grade (low-grade = 1) | 37.73 (1.87–760.53) | 0.018 | Grading high-grade (low-grade = 1) | 41.91 (2.29–767.91) | 0.012 | |
| LVSI present (absent = 1) | 24.61 (1.19–509.08) | 0.038 | LVSI present (absent = 1) | 24.67 (1.20–508.78) | 0.038 | LVSI present (absent = 1) | 20.76 (0.91–471.82) | 0.057 | |
| TB in 1 HPF high (low = 1) | 0.72 (0.00–181.61) | 0.907 | TB in 10 HPF high (low = 1) | 0.74 (0.00–179.96) | 0.913 | Minimal cell nest size (absent = 1) | 0.21 (0.00–579.03) | 0.703 | |
| TSR | MELF | ITBCC scheme | |||||||
| HR | p | HR | p | HR | p | ||||
| TCGA | Age | 0.93 (0.87–0.99) | 0.017 | Age | 0.97 (0.90–1.04) | 0.341 | Age | 0.95 (0.89–1.01) | 0.089 |
| FIGO stage 3/4 (1/2 = 1) | 2.95 (0.77–11.30) | 0.115 | FIGO stage 3/4 (1/2 = 1) | 2.64 (0.66–10.53) | 0.169 | FIGO stage 3/4 (1/2 = 1) | 3.08 (0.79–11.95) | 0.105 | |
| Grading high-grade (low-grade = 1) | 11.61 (2.43–55.53) | 0.002 | Grading high-grade (low-grade = 1) | 9.29 (1.90–45.42) | 0.006 | Grading high-grade (low-grade = 1) | 8.31 (1.57–44.09) | 0.013 | |
| LVSI present (absent = 1) | 4.25 (1.11–16.21) | 0.034 | LVSI present (absent = 1) | 4.94 (1.22–19.98) | 0.025 | LVSI present (absent = 1) | 6.22 (1.61–24.00) | 0.008 | |
| TSR (high = 1) | 4.04 (0.59–27.82) | 0.156 | MELF (absent = 1) | 2.81 (0.68–11.54) | 0.152 | ITBCC scheme (Bd1/Bd2 = 1) | 2.21 (0.42–11.61) | 0.349 | |
| MSI | Age | 0.94 (0.86–1.02) | 0.133 | Age | 1.03 (0.94–1.14) | 0.521 | Age | 0.98 (0.90–1.06) | 0.575 |
| FIGO stage 3/4 (1/2 = 1) | 5.19 (0.87–30.94) | 0.070 | FIGO stage 3/4 (1/2 = 1) | 8.29 (0.97–70.51) | 0.053 | FIGO stage 3/4 (1/2 = 1) | 6.05 (1.08–33.98) | 0.041 | |
| Grading high-grade (low-grade = 1) | 9.29 (1.06–81.38) | 0.044 | Grading high-grade (low-grade = 1) | 6.09 (0.45–82.29) | 0.174 | Grading high-grade (low-grade = 1) | 3.97 (0.36–44.35) | 0.263 | |
| LVSI present (absent = 1) | 1.79 (0.30–10.67) | 0.524 | LVSI present (absent = 1) | 5.21 (0.57–47.97) | 0.145 | LVSI present (absent = 1) | 3.27 (0.64–16.74) | 0.155 | |
| TSR (high = 1) | 5.38 (0.51–56.31) | 0.160 | MELF (absent = 1) | 14.14 (1.52–131.48) | 0.020 | ITBCC scheme (Bd1/Bd2 = 1) | 5.00 (0.72–34.68) | 0.103 | |
| CN-low | Age | 0.81 (0.67–0.99) | 0.038 | Age | 0.82 (0.68–0.99) | 0.039 | Age | 0.81 (0.67–0.99) | 0.035 |
| FIGO stage 3/4 (1/2 = 1) | 0.24 (0.01–10.75) | 0.463 | FIGO stage 3/4 (1/2 = 1) | 0.27 (0.00–201.15) | 0.701 | FIGO stage 3/4 (1/2 = 1) | 0.76 (0.00–2271.29) | 0.947 | |
| Grading high-grade (low-grade = 1) | 35.18 (1.95–636.22) | 0.016 | Grading high-grade (low-grade = 1) | 30.37 (1.68–548.13) | 0.021 | Grading high-grade (low-grade = 1) | 40.88 (2.15–778.76) | 0.014 | |
| LVSI present (absent = 1) | 24.55 (1.22–492.96) | 0.036 | LVSI present (absent = 1) | 24.82 (1.24–496.83) | 0.036 | LVSI present (absent = 1) | 22.47 (1.04–484.32) | 0.047 | |
| TSR (high = 1) | 0.00 (0.00–Inf) | 0.999 | MELF (absent = 1) | 0.94 (0.00–417.53) | 0.984 | ITBCC scheme (Bd1/Bd2 = 1) | 0.27 (0.00–1388.68) | 0.762 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stögbauer, F.; Geß, B.; Brambs, C.; Lautizi, M.; Kacprowski, T.; Ourailidis, I.; Bronger, H.; Kiechle, M.; Noske, A.; Keller, G.; et al. Independent Tissue-Based Biomarkers in Endometrioid Endometrial Cancer: Tumor Budding in Microsatellite Instability and WHO Grading in Copy-Number-Low Patients. Cancers 2023, 15, 3832. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15153832
Stögbauer F, Geß B, Brambs C, Lautizi M, Kacprowski T, Ourailidis I, Bronger H, Kiechle M, Noske A, Keller G, et al. Independent Tissue-Based Biomarkers in Endometrioid Endometrial Cancer: Tumor Budding in Microsatellite Instability and WHO Grading in Copy-Number-Low Patients. Cancers. 2023; 15(15):3832. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15153832
Chicago/Turabian StyleStögbauer, Fabian, Barbara Geß, Christine Brambs, Manuela Lautizi, Tim Kacprowski, Iordanis Ourailidis, Holger Bronger, Marion Kiechle, Aurelia Noske, Gisela Keller, and et al. 2023. "Independent Tissue-Based Biomarkers in Endometrioid Endometrial Cancer: Tumor Budding in Microsatellite Instability and WHO Grading in Copy-Number-Low Patients" Cancers 15, no. 15: 3832. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers15153832