
Neurofilament Light Chain (NfL) in Blood—A Biomarker Predicting Unfavourable Outcome in the Acute Phase and Improvement in the Late Phase after Stroke



{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. High Blood NfL Levels in the Acute Phase after Stroke Predict Unfavourable Outcome
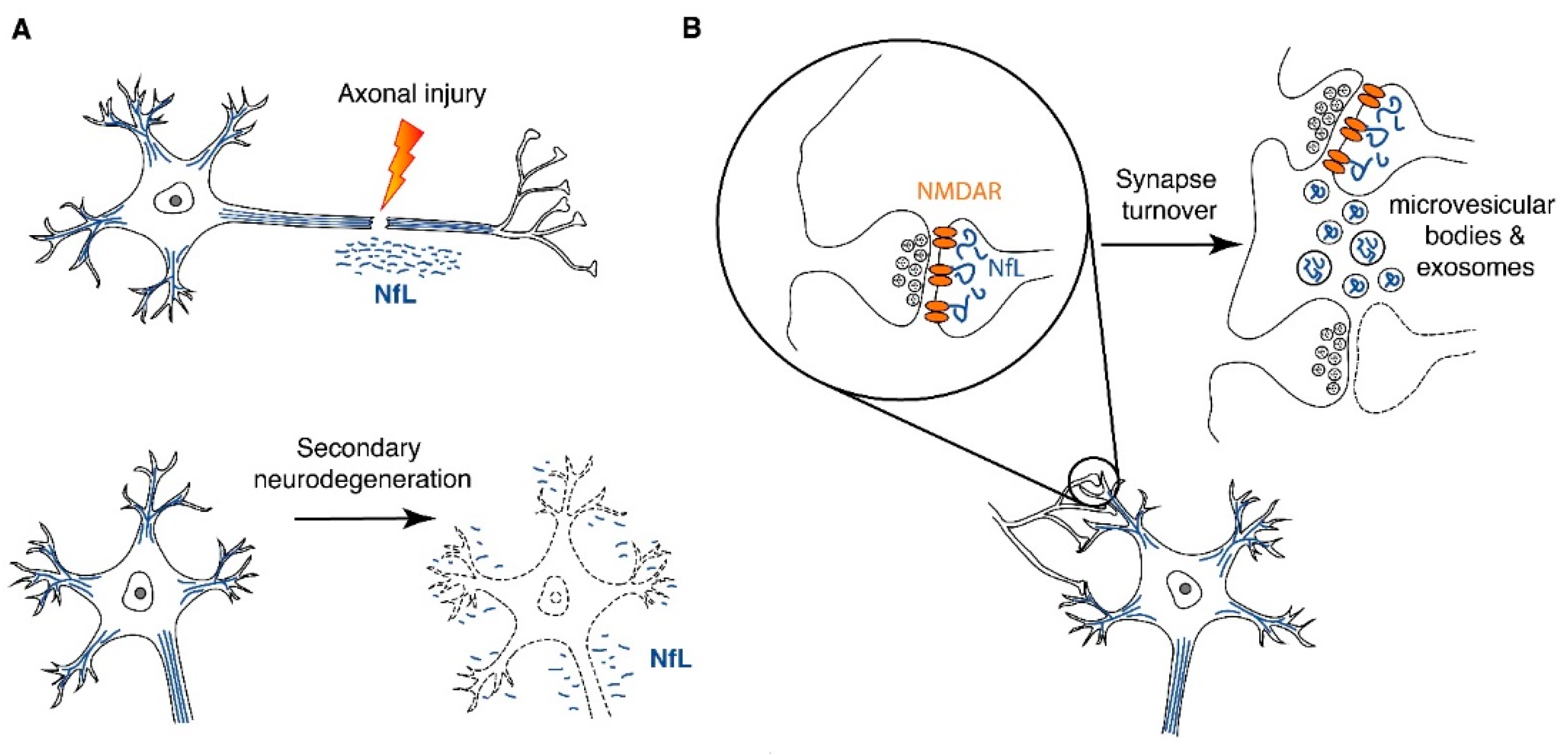
3. Blood NfL as a Biomarker of Post-Stroke Secondary Neurodegeneration
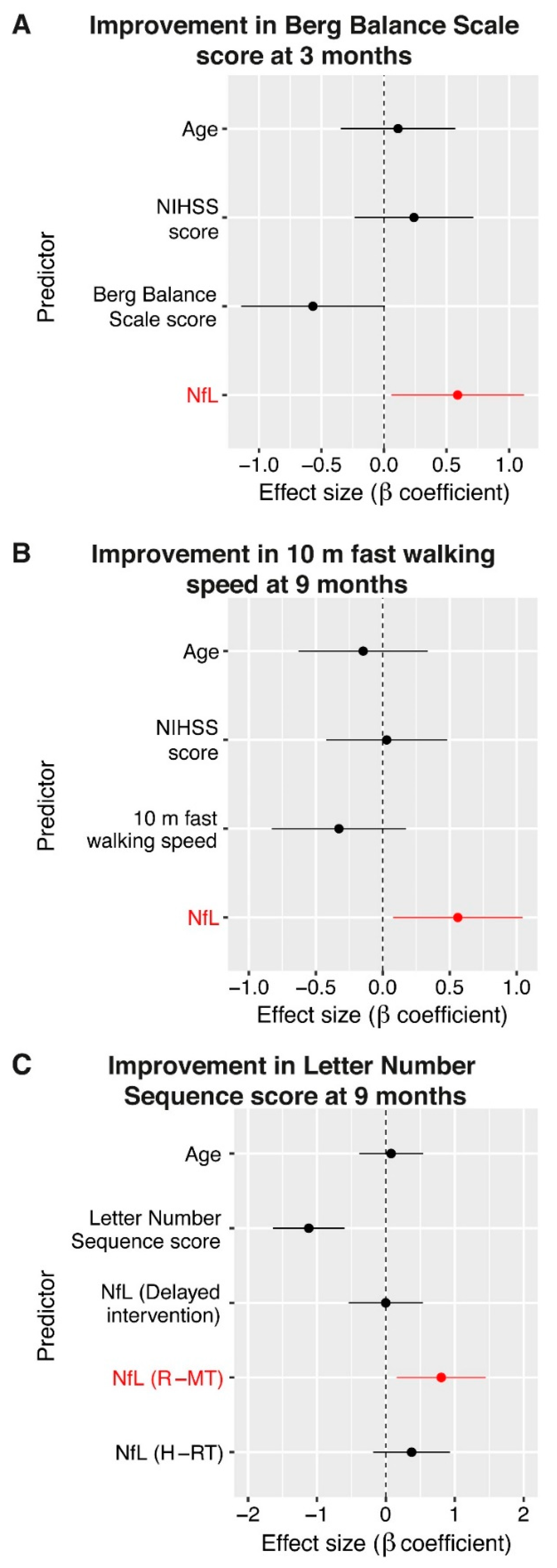
4. Blood NfL as a Predictor of Functional Improvement in the Late Phase after Stroke
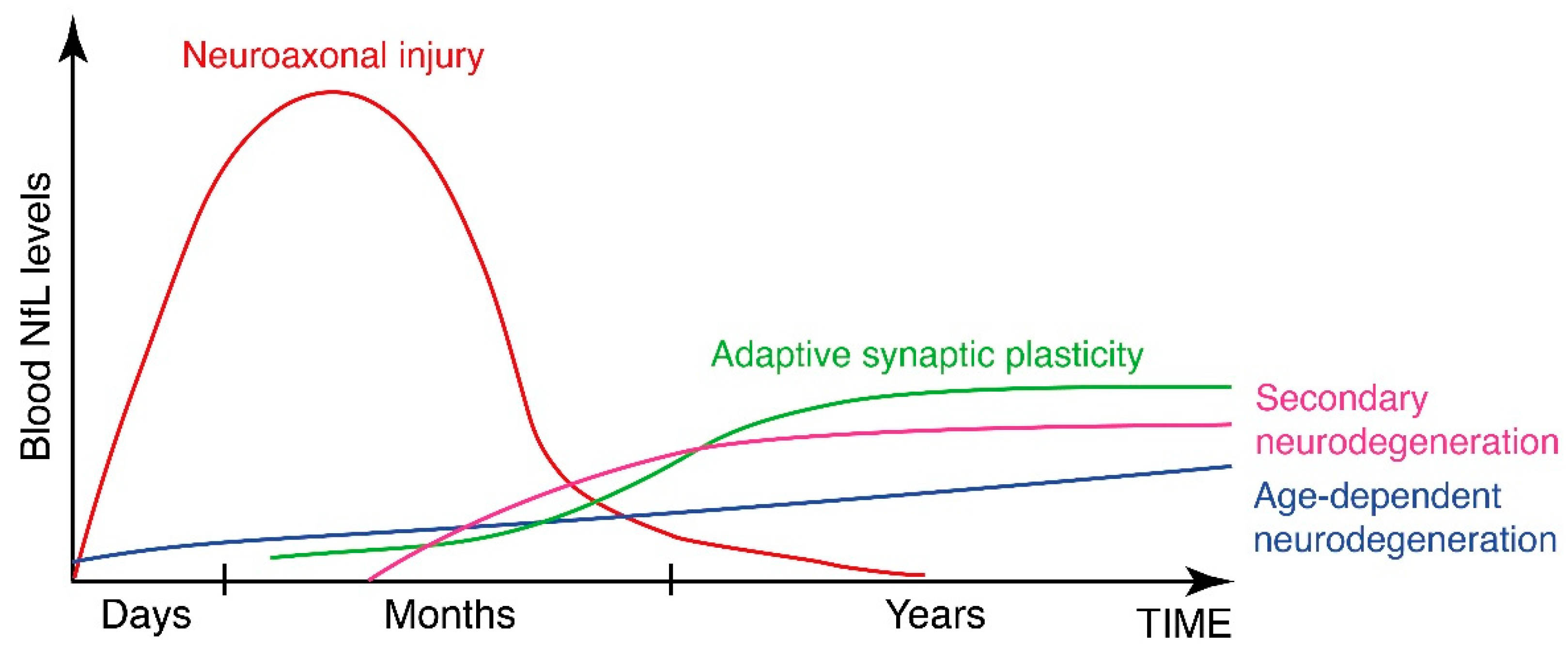
5. The Non-Axonal Functions of NfL and the Aspect of Time after Stroke
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feigin, V.L.; Lawes, C.M.; Bennett, D.A.; Barker-Collo, S.L.; Parag, V. Worldwide stroke incidence and early case fatality reported in 56 population-based studies: A systematic review. Lancet Neurol. 2009, 8, 355–369. [Google Scholar] [CrossRef]
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Pekna, M.; Pekny, M.; Nilsson, M. Modulation of neural plasticity as a basis for stroke rehabilitation. Stroke 2012, 43, 2819–2828. [Google Scholar] [CrossRef] [Green Version]
- Wieloch, T.; Nikolich, K. Mechanisms of neural plasticity following brain injury. Curr. Opin. Neurobiol. 2006, 16, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Lundkvist, A.; Andersson, D.; Wilhelmsson, U.; Nagai, N.; Pardo, A.C.; Nodin, C.; Stahlberg, A.; Aprico, K.; Larsson, K.; et al. Protective role of reactive astrocytes in brain ischemia. J. Cereb. Blood Flow Metab. 2008, 28, 468–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pekny, M.; Nilsson, M. Astrocyte activation and reactive gliosis. Glia 2005, 50, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Pekny, M.; Pekna, M. Reactive gliosis in the pathogenesis of CNS diseases. Biochim. Biophys. Acta 2016, 1862, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Hankey, G.J.; Spiesser, J.; Hakimi, Z.; Bego, G.; Carita, P.; Gabriel, S. Rate, degree, and predictors of recovery from disability following ischemic stroke. Neurology 2007, 68, 1583–1587. [Google Scholar] [CrossRef]
- Hankey, G.J.; Spiesser, J.; Hakimi, Z.; Carita, P.; Gabriel, S. Time frame and predictors of recovery from disability following recurrent ischemic stroke. Neurology 2007, 68, 202–205. [Google Scholar] [CrossRef]
- Ferrarello, F.; Baccini, M.; Rinaldi, L.A.; Cavallini, M.C.; Mossello, E.; Masotti, G.; Marchionni, N.; Di Bari, M. Efficacy of physiotherapy interventions late after stroke: A meta-analysis. J. Neurol. Neurosurg. Psychiatry 2011, 82, 136–143. [Google Scholar] [CrossRef] [Green Version]
- Bunketorp Käll, L.; Lundgren-Nilsson, Å.; Samuelsson, H.; Pekny, T.; Blomqvist, K.; Pekna, M.; Pekny, M.; Blomstrand, C.; Nilsson, M. Long-term improvements after multimodal rehabilitation in late phase after stroke: A randomized controlled trial. Stroke 2017, 48, 1916–1924. [Google Scholar] [CrossRef]
- Bivard, A.; Lillicrap, T.; Marechal, B.; Garcia-Esperon, C.; Holliday, E.; Krishnamurthy, V.; Levi, C.R.; Parsons, M. Transient Ischemic Attack Results in Delayed Brain Atrophy and Cognitive Decline. Stroke 2018, 49, 384–390. [Google Scholar] [CrossRef]
- Gauthier, L.V.; Taub, E.; Mark, V.W.; Barghi, A.; Uswatte, G. Atrophy of spared gray matter tissue predicts poorer motor recovery and rehabilitation response in chronic stroke. Stroke 2012, 43, 453–457. [Google Scholar] [CrossRef] [Green Version]
- Kuchcinski, G.; Munsch, F.; Lopes, R.; Bigourdan, A.; Su, J.; Sagnier, S.; Renou, P.; Pruvo, J.P.; Rutt, B.K.; Dousset, V.; et al. Thalamic alterations remote to infarct appear as focal iron accumulation and impact clinical outcome. Brain 2017, 140, 1932–1946. [Google Scholar] [CrossRef]
- Duering, M.; Righart, R.; Wollenweber, F.A.; Zietemann, V.; Gesierich, B.; Dichgans, M. Acute infarcts cause focal thinning in remote cortex via degeneration of connecting fiber tracts. Neurology 2015, 84, 1685–1692. [Google Scholar] [CrossRef] [Green Version]
- Gentil, B.J.; Tibshirani, M.; Durham, H.D. Neurofilament dynamics and involvement in neurological disorders. Cell Tissue Res. 2015, 360, 609–620. [Google Scholar] [CrossRef]
- Zhu, Q.; Couillard-Després, S.; Julien, J.P. Delayed maturation of regenerating myelinated axons in mice lacking neurofilaments. Exp. Neurol. 1997, 148, 299–316. [Google Scholar] [CrossRef] [PubMed]
- Yuan, A.; Rao, M.V.; Veeranna; Nixon, R.A. Neurofilaments and Neurofilament Proteins in Health and Disease. Cold Spring Harbor Perspect. Biol. 2017, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Disanto, G.; Barro, C.; Benkert, P.; Naegelin, Y.; Schadelin, S.; Giardiello, A.; Zecca, C.; Blennow, K.; Zetterberg, H.; Leppert, D.; et al. Serum Neurofilament light: A biomarker of neuronal damage in multiple sclerosis. Ann. Neurol. 2017, 81, 857–870. [Google Scholar] [CrossRef] [PubMed]
- Kuhle, J.; Nourbakhsh, B.; Grant, D.; Morant, S.; Barro, C.; Yaldizli, O.; Pelletier, D.; Giovannoni, G.; Waubant, E.; Gnanapavan, S. Serum neurofilament is associated with progression of brain atrophy and disability in early MS. Neurology 2017, 88, 826–831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalil, M.; Teunissen, C.E.; Otto, M.; Piehl, F.; Sormani, M.P.; Gattringer, T.; Barro, C.; Kappos, L.; Comabella, M.; Fazekas, F.; et al. Neurofilaments as biomarkers in neurological disorders. Nat. Rev. Neurol. 2018, 14, 577–589. [Google Scholar] [CrossRef]
- Barro, C.; Chitnis, T.; Weiner, H.L. Blood neurofilament light: A critical review of its application to neurologic disease. Ann. Clin. Transl. Neurol. 2020, 7, 2508–2523. [Google Scholar] [CrossRef]
- Gattringer, T.; Pinter, D.; Enzinger, C.; Seifert-Held, T.; Kneihsl, M.; Fandler, S.; Pichler, A.; Barro, C.; Gröbke, S.; Voortman, M.; et al. Serum neurofilament light is sensitive to active cerebral small vessel disease. Neurology 2017, 89, 2108–2114. [Google Scholar] [CrossRef] [PubMed]
- Tiedt, S.; Duering, M.; Barro, C.; Kaya, A.G.; Boeck, J.; Bode, F.J.; Klein, M.; Dorn, F.; Gesierich, B.; Kellert, L.; et al. Serum neurofilament light: A biomarker of neuroaxonal injury after ischemic stroke. Neurology 2018, 91, e1338–e1347. [Google Scholar] [CrossRef]
- Pedersen, A.; Stanne, T.M.; Nilsson, S.; Klasson, S.; Rosengren, L.; Holmegaard, L.; Jood, K.; Blennow, K.; Zetterberg, H.; Jern, C. Circulating neurofilament light in ischemic stroke: Temporal profile and outcome prediction. J. Neurol. 2019, 266, 2796–2806. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uphaus, T.; Bittner, S.; Groschel, S.; Steffen, F.; Muthuraman, M.; Wasser, K.; Weber-Kruger, M.; Zipp, F.; Wachter, R.; Groschel, K. NfL (neurofilament light chain) levels as a predictive marker for long-term outcome after ischemic stroke. Stroke 2019, 50, 3077–3084. [Google Scholar] [CrossRef] [PubMed]
- Pujol-Calderón, F.; Portelius, E.; Zetterberg, H.; Blennow, K.; Rosengren, L.E.; Höglund, K. Neurofilament changes in serum and cerebrospinal fluid after acute ischemic stroke. Neurosci. Lett. 2019, 698, 58–63. [Google Scholar] [CrossRef]
- Peters, N.; van Leijsen, E.; Tuladhar, A.M.; Barro, C.; Konieczny, M.J.; Ewers, M.; Lyrer, P.; Engelter, S.T.; Kuhle, J.; Duering, M.; et al. Serum Neurofilament Light Chain Is Associated with Incident Lacunes in Progressive Cerebral Small Vessel Disease. J. Stroke 2020, 22, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Chen, J.; Wang, X.; Xin, J.; Cao, R.; Liu, Z. Serum Neurofilament Light Chain as a Predictive Biomarker for Ischemic Stroke Outcome: A Systematic Review and Meta-analysis. J. Stroke Cerebrovasc. Dis. Off. J. Natl. Stroke Assoc. 2020, 29, 104813. [Google Scholar] [CrossRef]
- Gafson, A.R.; Barthelemy, N.R.; Bomont, P.; Carare, R.O.; Durham, H.D.; Julien, J.P.; Kuhle, J.; Leppert, D.; Nixon, R.A.; Weller, R.O.; et al. Neurofilaments: Neurobiological foundations for biomarker applications. Brain 2020, 143, 1975–1998. [Google Scholar] [CrossRef]
- Stokowska, A.; Bunketorp Käll, L.; Blomstrand, C.; Simrén, J.; Nilsson, M.; Zetterberg, H.; Blennow, K.; Pekny, M.; Pekna, M. Plasma neurofilament light chain levels predict improvement in late phase after stroke. Eur. J. Neurol. 2021, 28, 2218–2228. [Google Scholar] [CrossRef] [PubMed]
- Ehlers, M.D.; Fung, E.T.; O’Brien, R.J.; Huganir, R.L. Splice variant-specific interaction of the NMDA receptor subunit NR1 with neuronal intermediate filaments. J. Neurosci. 1998, 18, 720–730. [Google Scholar] [CrossRef] [Green Version]
- Ratnam, J.; Teichberg, V.I. Neurofilament-light increases the cell surface expression of the N-methyl-D-aspartate receptor and prevents its ubiquitination. J. Neurochem. 2005, 92, 878–885. [Google Scholar] [CrossRef] [PubMed]
- Yuan, A.; Veeranna; Sershen, H.; Basavarajappa, B.S.; Smiley, J.F.; Hashim, A.; Bleiwas, C.; Berg, M.; Guifoyle, D.N.; Subbanna, S.; et al. Neurofilament light interaction with GluN1 modulates neurotransmission and schizophrenia-associated behaviors. Transl. Psychiatry 2018, 8, 167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albargothy, N.J.; Johnston, D.A.; MacGregor-Sharp, M.; Weller, R.O.; Verma, A.; Hawkes, C.A.; Carare, R.O. Convective influx/glymphatic system: Tracers injected into the CSF enter and leave the brain along separate periarterial basement membrane pathways. Acta Neuropathol. 2018, 136, 139–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasmussen, M.K.; Mestre, H.; Nedergaard, M. Fluid Transport in the Brain. Physiol. Rev. 2021. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pekny, M.; Wilhelmsson, U.; Stokowska, A.; Tatlisumak, T.; Jood, K.; Pekna, M. Neurofilament Light Chain (NfL) in Blood—A Biomarker Predicting Unfavourable Outcome in the Acute Phase and Improvement in the Late Phase after Stroke. Cells 2021, 10, 1537. https://0-doi-org.brum.beds.ac.uk/10.3390/cells10061537
Pekny M, Wilhelmsson U, Stokowska A, Tatlisumak T, Jood K, Pekna M. Neurofilament Light Chain (NfL) in Blood—A Biomarker Predicting Unfavourable Outcome in the Acute Phase and Improvement in the Late Phase after Stroke. Cells. 2021; 10(6):1537. https://0-doi-org.brum.beds.ac.uk/10.3390/cells10061537
Chicago/Turabian StylePekny, Milos, Ulrika Wilhelmsson, Anna Stokowska, Turgut Tatlisumak, Katarina Jood, and Marcela Pekna. 2021. "Neurofilament Light Chain (NfL) in Blood—A Biomarker Predicting Unfavourable Outcome in the Acute Phase and Improvement in the Late Phase after Stroke" Cells 10, no. 6: 1537. https://0-doi-org.brum.beds.ac.uk/10.3390/cells10061537