
Immunotherapy in Nonendemic Nasopharyngeal Carcinoma: Real-World Data from Two Nonendemic Regions

 , ,
, ,  , , , , , , , ,
, , , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Treatment, Response and Toxicity
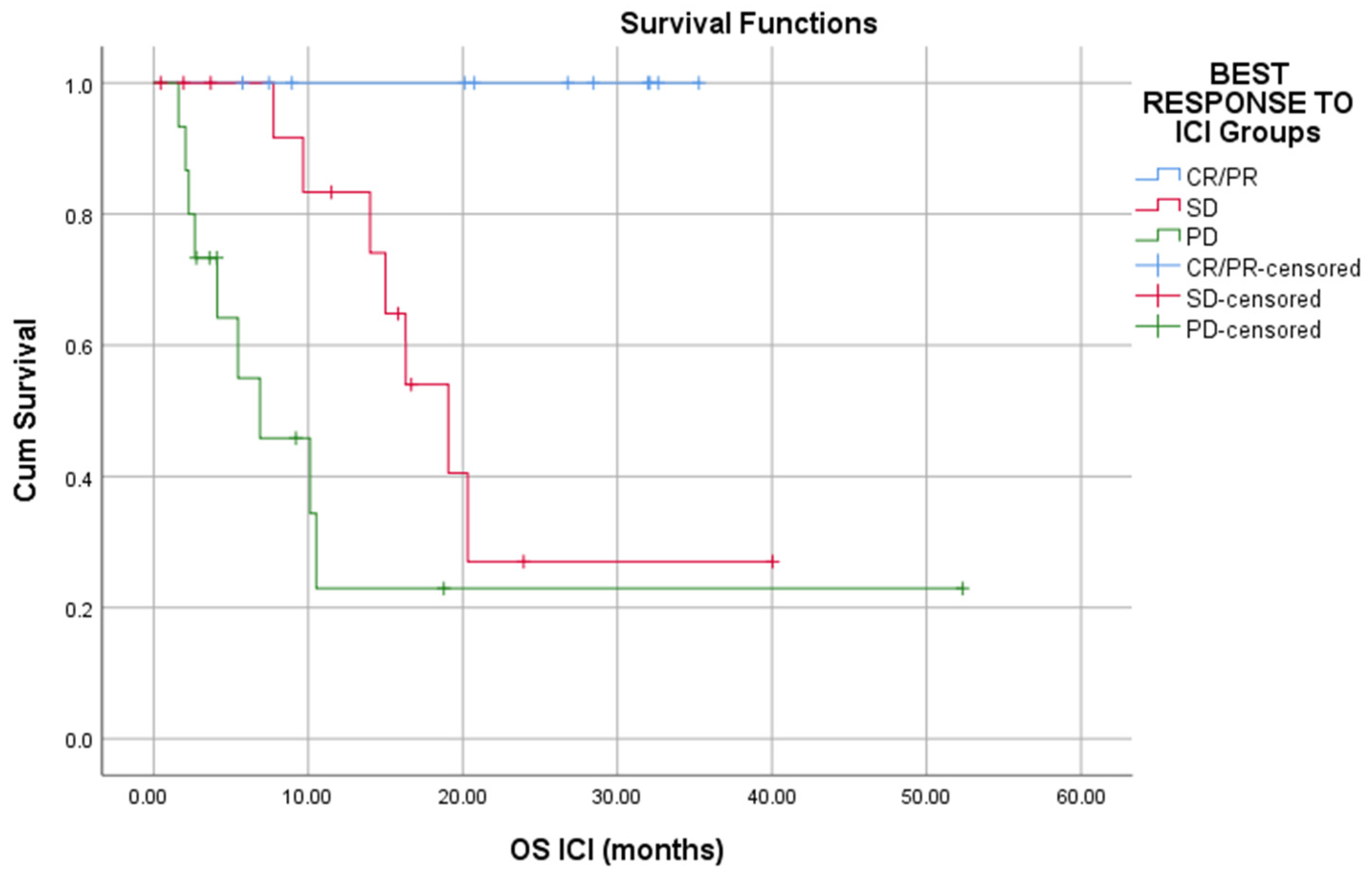
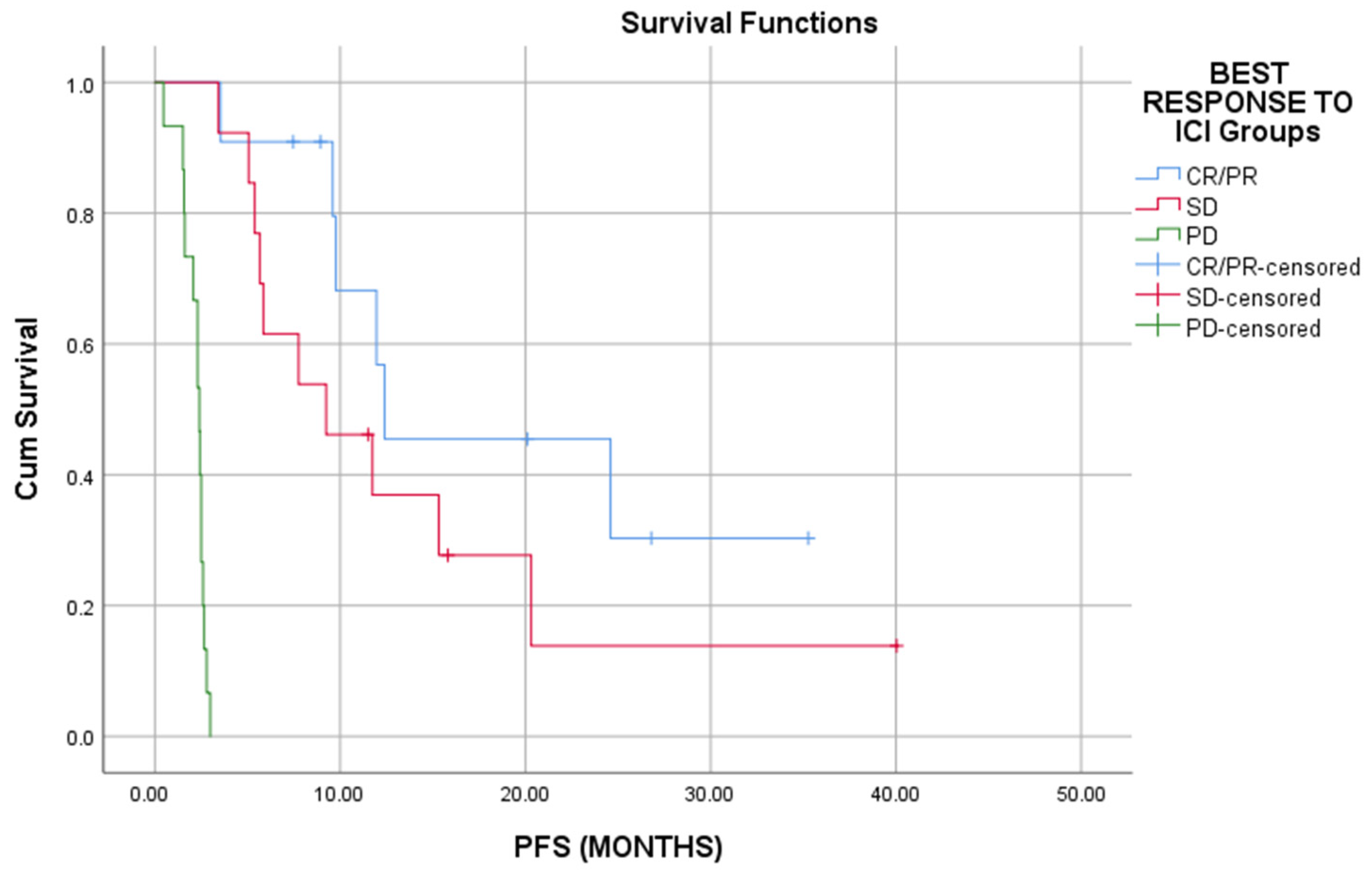
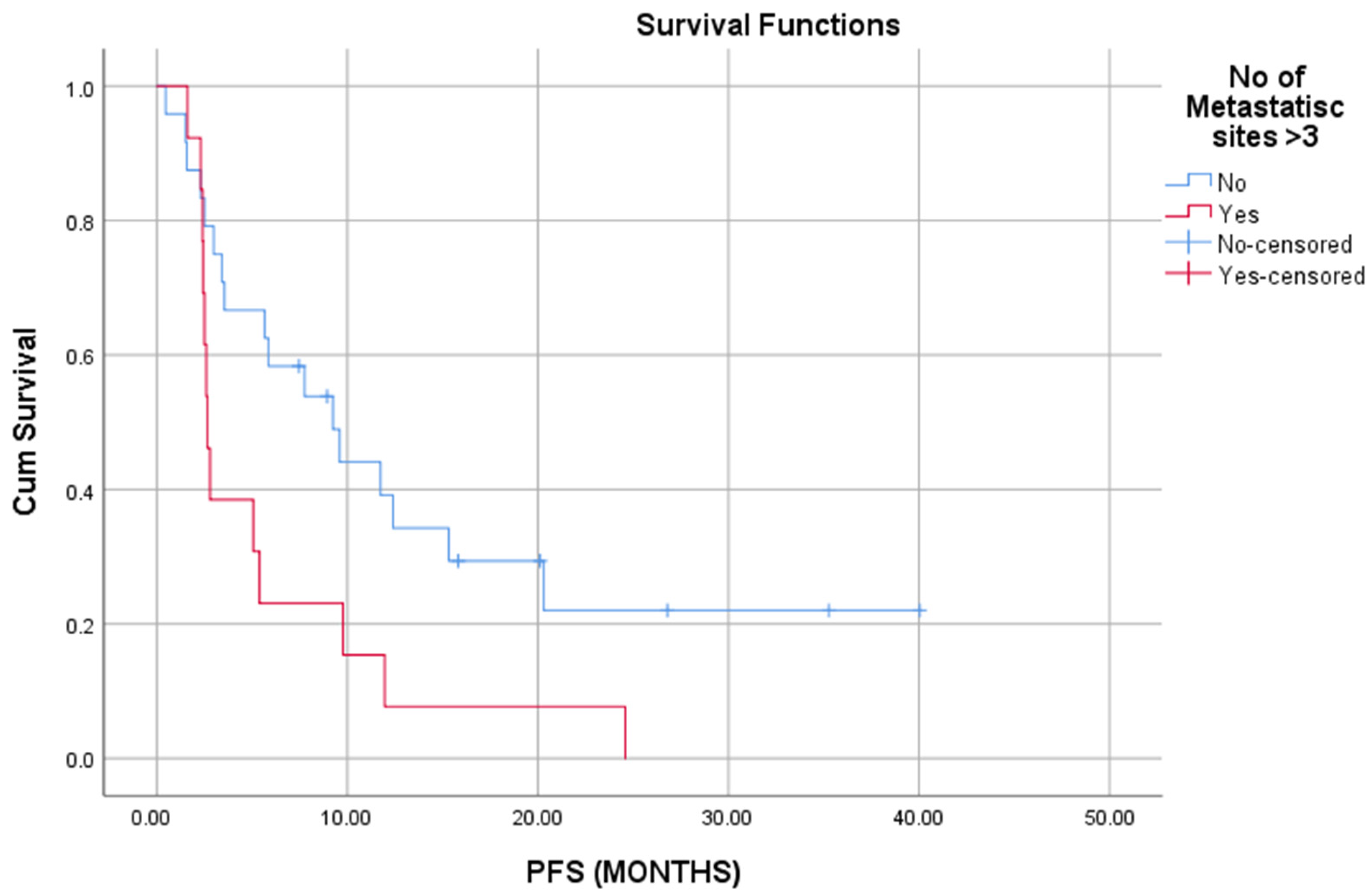
3.3. Association with Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chang, E.T.; Adami, H.-O. The Enigmatic Epidemiology of Nasopharyngeal Carcinoma. Cancer Epidemiol. Biomark. Prev. 2006, 15, 1765–1777. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.P.; Chan, A.T.C.; Le, Q.T.; Blanchard, P.; Sun, Y.; Ma, J. Nasopharyngeal carcinoma. Lancet 2019, 394, 64–80. [Google Scholar] [CrossRef]
- Hildesheim, A.; Wang, C.-P. Genetic predisposition factors and nasopharyngeal carcinoma risk: A review of epidemiological association studies, 2000–2011: Rosetta Stone for NPC: Genetics, viral infection, and other environmental factors. Semin. Cancer Biol. 2012, 22, 107–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, T.; Tang, J.; Gu, M.; Liu, L.; Wei, W.; Yang, H. Recurrent Nasopharyngeal Carcinoma: A Clinical Dilemma and Challenge. Curr. Oncol. 2013, 20, 406–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peng, G.; Wang, T.; Yang, K.-Y.; Zhang, S.; Zhang, T.; Li, Q.; Han, J.; Wu, G. A prospective, randomized study comparing outcomes and toxicities of intensity-modulated radiotherapy vs. conventional two-dimensional radiotherapy for the treatment of nasopharyngeal carcinoma. Radiother. Oncol. 2012, 104, 286–293. [Google Scholar] [CrossRef]
- Lee, A.W.; Ma, B.; Ng, W.T.; Chan, A.T. Management of Nasopharyngeal Carcinoma: Current Practice and Future Perspective. J. Clin. Oncol. 2015, 33, 3356–3364. [Google Scholar] [CrossRef]
- You, R.; Liu, Y.P.; Huang, P.Y.; Zou, X.; Sun, R.; He, Y.X.; Wu, Y.S.; Shen, G.P.; Zhang, H.D.; Duan, C.Y.; et al. Efficacy and Safety of Locoregional Radiotherapy With Chemotherapy vs Chemotherapy Alone in De Novo Metastatic Nasopharyngeal Carcinoma: A Multicenter Phase 3 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 1345–1352. [Google Scholar] [CrossRef]
- Mai, H.-Q.; Chen, Q.-Y.; Chen, D.; Hu, C.; Yang, K.; Wen, J.; Li, J.; Shi, Y.-R.; Jin, F.; Xu, R.; et al. Toripalimab or placebo plus chemotherapy as first-line treatment in advanced nasopharyngeal carcinoma: A multicenter randomized phase 3 trial. Nat. Med. 2021, 27, 1536–1543. [Google Scholar] [CrossRef]
- Yang, Y.; Qu, S.; Li, J.; Hu, C.; Xu, M.; Li, W.; Zhou, T.; Shen, L.; Wu, H.; Lang, J.; et al. Camrelizumab versus placebo in combination with gemcitabine and cisplatin as first-line treatment for recurrent or metastatic nasopharyngeal carcinoma (CAPTAIN-1st): A multicentre, randomised, double-blind, phase 3 trial. Lancet Oncol. 2021, 22, 1162–1174. [Google Scholar] [CrossRef]
- Hsu, C.; Lee, S.-H.; Ejadi, S.; Even, C.; Cohen, R.B.; Le Tourneau, C.; Mehnert, J.M.; Algazi, A.; Van Brummelen, E.M.; Saraf, S.; et al. Safety and Antitumor Activity of Pembrolizumab in Patients With Programmed Death-Ligand 1–Positive Nasopharyngeal Carcinoma: Results of the KEYNOTE-028 Study. J. Clin. Oncol. 2017, 35, 4050–4056. [Google Scholar] [CrossRef]
- Ma, B.B.Y.; Lim, W.-T.; Goh, B.-C.; Hui, E.P.; Lo, K.-W.; Pettinger, A.; Foster, N.R.; Riess, J.W.; Agulnik, M.; Chang, A.Y.C.; et al. Antitumor Activity of Nivolumab in Recurrent and Metastatic Nasopharyngeal Carcinoma: An International, Multicenter Study of the Mayo Clinic Phase 2 Consortium (NCI-9742). J. Clin. Oncol. 2018, 36, 1412–1418. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.; Lee, V.; Hong, R.-L.; Ahn, M.-J.; Chong, W.; Kim, S.-B.; Fuang, H.G.; Caguioa, P.; Ngamphaiboon, N.; Ho, C.; et al. 858O Results of KEYNOTE-122: A phase III study of pembrolizumab (pembro) monotherapy vs chemotherapy (chemo) for platinum-pretreated, recurrent or metastatic (R/M) nasopharyngeal carcinoma (NPC). Ann. Oncol. 2021, 32, S786. [Google Scholar] [CrossRef]
- Huang, S.H.; O’Sullivan, B. Overview of the 8th Edition TNM Classification for Head and Neck Cancer. Curr. Treat. Options Oncol. 2017, 18, 40. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Michot, J.; Bigenwald, C.; Champiat, S.; Collins, M.; Carbonnel, F.; Postel-Vinay, S.; Berdelou, A.; Varga, A.; Bahleda, R.; Hollebecque, A.; et al. Immune-related adverse events with immune checkpoint blockade: A comprehensive review. Eur. J. Cancer 2016, 54, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Stelow, E.B.; Wenig, B.M. Update From The 4th Edition of the World Health Organization Classification of Head and Neck Tumours: Nasopharynx. Head Neck Pathol. 2017, 11, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Limkin, E.J.; Blanchard, P. Does East meet West? Towards a unified vision of the management of Nasopharyngeal carcinoma. Br. J. Radiol. 2019, 92, 20190068. [Google Scholar] [CrossRef]
- Marks, J.E.; Phillips, J.L.; Menck, H.R. The national cancer data base report on the relationship of race and national origin to the histology of nasopharyngeal carcinoma. Cancer 1998, 83, 582–588. [Google Scholar] [CrossRef]
- Asher, N.; Ben-Betzalel, G.; Lev-Ari, S.; Shapira-Frommer, R.; Steinberg-Silman, Y.; Gochman, N.; Schachter, J.; Meirson, T.; Markel, G. Real World Outcomes of Ipilimumab and Nivolumab in Patients with Metastatic Melanoma. Cancers 2020, 12, 2329. [Google Scholar] [CrossRef]
- Tarhini, A.; Kudchadkar, R.R. Predictive and on-treatment monitoring biomarkers in advanced melanoma: Moving toward personalized medicine. Cancer Treat. Rev. 2018, 71, 8–18. [Google Scholar] [CrossRef] [Green Version]
- Alfieri, S.; Iacovelli, N.A.; Marceglia, S.; Lasorsa, I.; Resteghini, C.; Taverna, F.; Mazzocchi, A.; Orlandi, E.; Guzzo, M.; Bianchi, R.; et al. Circulating pre-treatment Epstein-Barr virus DNA as prognostic factor in locally-advanced nasopharyngeal cancer in a non-endemic area. Oncotarget 2017, 8, 47780–47789. [Google Scholar] [CrossRef] [Green Version]
- Kao, H.F.; Hsu, C.; Huang, H.C.; Cheng, J.; Hong, R.L. Correlation between plasma EBV DNA and clinical response to pembrolizumab in patients with advanced or metastatic nasopharyngeal carcinoma. Ann. Oncol. 2015, 26, viii5–viii7. [Google Scholar] [CrossRef] [Green Version]
- Lim, D.W.-T.; Wang, H.-M.; Li, S.-H.; Ngan, R.; Dechaphunkul, A.; Zhang, L.; Yen, C.J.; Chan, P.C.; Chakrabandhu, S.; Ma, B.; et al. Abstract CT150: Phase II study of spartalizumab (PDR001) vs chemotherapy (CT) in patients with recurrent/metastatic nasopharyngeal cancer (NPC). Cancer Res. 2019, 79, CT150. [Google Scholar]
- Zhang, L.; Yang, Y.; Chen, X.; Li, J.; Pan, J.; He, X.; Lin, L.; Shi, Y.; Feng, W.; Xiong, J.; et al. 912MO A single-arm, open-label, multicenter phase II study of camrelizumab in patients with recurrent or metastatic (R/M) nasopharyngeal carcinoma (NPC) who had progressed on ≥2 lines of chemotherapy: CAPTAIN study. Ann. Oncol. 2020, 31, S659. [Google Scholar] [CrossRef]
- Wang, F.-H.; Wei, X.-L.; Feng, J.; Li, Q.; Xu, N.; Hu, X.-C.; Liao, W.; Jiang, Y.; Lin, X.-Y.; Zhang, Q.-Y.; et al. Efficacy, Safety, and Correlative Biomarkers of Toripalimab in Previously Treated Recurrent or Metastatic Nasopharyngeal Carcinoma: A Phase II Clinical Trial (POLARIS-02). J. Clin. Oncol. 2021, 39, 704–712. [Google Scholar] [CrossRef] [PubMed]
- Sakuramoto, S.; Sasako, M.; Yamaguchi, T.; Kinoshita, T.; Fujii, M.; Nashimoto, A.; Furukawa, H.; Nakajima, T.; Ohashi, Y.; Imamura, H.; et al. Adjuvant Chemotherapy for Gastric Cancer with S-1, an Oral Fluoropyrimidine. N. Engl. J. Med. 2007, 357, 1810–1820. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | N | % | |
|---|---|---|---|
| Age | <65 years | 35 | 76.1 |
| ≥65 years | 11 | 23.9 | |
| Sex | Male | 36 | 78.3 |
| Female | 10 | 21.7 | |
| History of tobacco use | Active smoker | 14 | 30.4 |
| Former smoker | 11 | 23.9 | |
| Nonsmoker | 21 | 45.7 | |
| History of alcohol consumption | No | 41 | 89.1 |
| Moderate/Heavy | 5 | 10.9 | |
| Charlson comorbidity index | ≤2 | 16 | 34.8 |
| >2 | 22 | 47.8 | |
| N/A | 8 | 17.4 | |
| Site of metastasis | Lung | 10 | 21.7 |
| Bone | 16 | 34.8 | |
| Liver | 11 | 23.9 | |
| Other | 6 | 13 | |
| None | 17 | 36.9 | |
| Stage TNM | II–III | 18 | 39.1 |
| IV | 24 | 52.2 | |
| N/A | 4 | 8.7 | |
| Histology (WHO classification) | Nonkeratinizing squamous cell carcinoma | 40 | 86.9 |
| Keratinizing squamous cell carcinoma | 3 | 6.5 | |
| Basaloid | 1 | 2.2 | |
| Pretreatment plasma EBV DNA | N/A | 2 | 4.4 |
| Positive | 18 | 39.1 | |
| Negative | 13 | 28.3 | |
| Unavailable | 15 | 32.6 |
| Covariates | Univariate Anaylsis | Mutlivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|---|
| HR | 95.0% CI | p-Value | HR | 95.0% CI | p-Value | |||
| Age (years) | 1.011 | 0.969 | 1.056 | 0.612 | 1.002 | 0.910 | 1.103 | 0.970 |
| Comorbidities | 1.019 | 0.859 | 1.208 | 0.829 | 0.549 | 0.269 | 1.120 | 0.099 |
| EBV DNA at first diagnosis | 1.000 | 1.000 | 1.000 | 0.082 | 1.000 | 1.000 | 1.000 | 0.361 |
| Pre-ICI EBV DNA | 1.000 | 1.000 | 1.000 | 0.583 | 1.000 | 1.000 | 1.000 | 0.687 |
| Line of therapy | 1.026 | 0.735 | 1.431 | 0.881 | 1.569 | 0.680 | 3.618 | 0.291 |
| No. of metastatic sites | 1.002 | 0.894 | 1.124 | 0.966 | 0.919 | 0.582 | 1.451 | 0.716 |
| Study/ICI | N of Pts (Total (Assigned to ICI)) | Setting | Phase | Median PFS (Months) | Median OS (Months) | ORR % | Ref |
|---|---|---|---|---|---|---|---|
| NCI-9742/Nivolumab | 45 | Pretreated | II | 2.8 | 17.1 | 20.5 | [11] |
| Keynote-028/Pembrolizumab | 27 | Pretreated | Ib | 6.5 | 16.1 | 25.9 | [10] |
| Keynote-122/Pembrolizumab vs. chemotherapy | 233 (117) | Platinum-refractory | III | 4.1 vs. 5.5 | 17.2 vs. 18 | 21.4 vs. 23.3 | [12] |
| PDR001/Spartalizumab vs. chemotherapy | 122 (76) | Platinum-refractory | II | 1.9 vs. 6.6 | NR in either group | 18.4 vs. 32.4 | [23] |
| Captain-1st/Camrelizumab + chemotherapy vs. placebo + chemotherapy | 263 (134) | 1st line | III | 9.7 vs. 6.9 | NR vs. 22.6 | 87.3 vs. 80.6 | [9] |
| Jupiter-02/Toparilimab + chemotherapy vs. placebo + chemotherapy | 289 (146) | 1st line | III | 11.7 vs. 8 | NR in either arm | 77.4 vs. 66.4 | [8] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Economopoulou, P.; Pantazopoulos, A.; Spathis, A.; Kotsantis, I.; Kyriazoglou, A.; Kavourakis, G.; Zakopoulou, R.; Chatzidakis, I.; Anastasiou, M.; Prevezanou, M.; et al. Immunotherapy in Nonendemic Nasopharyngeal Carcinoma: Real-World Data from Two Nonendemic Regions. Cells 2022, 11, 32. https://0-doi-org.brum.beds.ac.uk/10.3390/cells11010032
Economopoulou P, Pantazopoulos A, Spathis A, Kotsantis I, Kyriazoglou A, Kavourakis G, Zakopoulou R, Chatzidakis I, Anastasiou M, Prevezanou M, et al. Immunotherapy in Nonendemic Nasopharyngeal Carcinoma: Real-World Data from Two Nonendemic Regions. Cells. 2022; 11(1):32. https://0-doi-org.brum.beds.ac.uk/10.3390/cells11010032
Chicago/Turabian StyleEconomopoulou, Panagiota, Anastasios Pantazopoulos, Aris Spathis, Ioannis Kotsantis, Anastasios Kyriazoglou, George Kavourakis, Roubini Zakopoulou, Ioannis Chatzidakis, Maria Anastasiou, Maria Prevezanou, and et al. 2022. "Immunotherapy in Nonendemic Nasopharyngeal Carcinoma: Real-World Data from Two Nonendemic Regions" Cells 11, no. 1: 32. https://0-doi-org.brum.beds.ac.uk/10.3390/cells11010032