
Automatic Deep-Learning Segmentation of Epicardial Adipose Tissue from Low-Dose Chest CT and Prognosis Impact on COVID-19

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Population and Data
2.2.1. Population
2.2.2. Radiological Data
2.3. EAT Segmentation Model
2.3.1. Manual Segmentation
2.3.2. Manual Segmentation and Slice Detection Model
2.3.3. Performance Evaluation and Reproducibility
2.4. Prognosis Value and Association with COVID-19 Lesions
2.5. Statistical Analysis
3. Results
3.1. Population Characteristics
3.2. EAT Algorithm Performance and Reproducibility
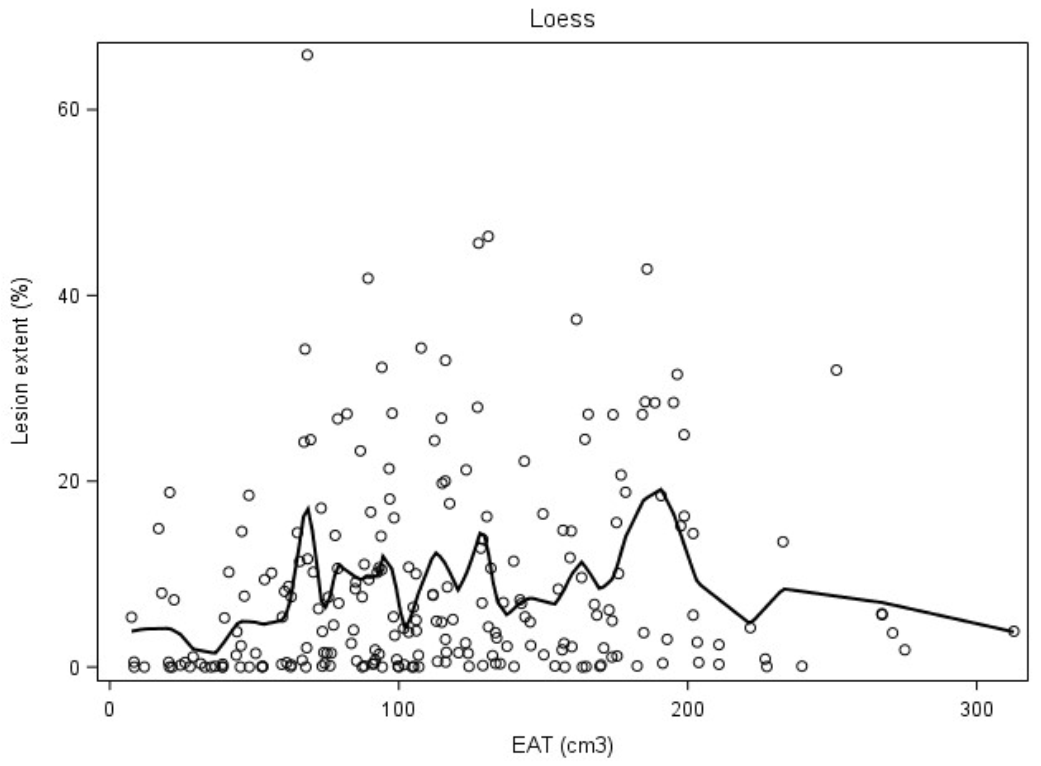
3.3. EAT and COVID-19 Association
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. LDCT Technical Parameters
Appendix B
Appendix B.1. High-Resolution Network
Appendix B.2. Object Context Representation
Appendix C



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| EAT (cm3) | Ext_EAT (%) | |||||||
|---|---|---|---|---|---|---|---|---|
| Criteria | Mean (±SD) | Minimum | Maximum | p-Value * | Mean (±SD) | Minimum | Maximum | p-Value * |
| Need for Oxygen Therapy | ||||||||
| Yes | 125.3 (±53.9) | 8.2 | 275.1 | 16.7 (±6.7) | 3.3 | 34.5 | ||
| No | 101.6 (±61.9) | 7.5 | 312.8 | p = 0.0023 | 14.6 (±6.2) | 2.2 | 31.0 | p = 0.013 |
| Hospitalization >10 days | ||||||||
| Yes | 116.2 (±52.3) | 18.0 | 221.6 | 15.2 (±6.8) | 3.5 | 34.0 | ||
| No | 112.1 (±60.9) | 7.5 | 312.8 | p = 0.6771 | 15.7 (±6.4) | 2.2 | 34.0 | p = 0.700 |
| ICU admission | ||||||||
| Yes | 143.4 (±61.0) | 16.8 | 275.1 | 19.0 (±7.2) | 6.1 | 34.5 | ||
| No | 108.3 (±57.8) | 7.5 | 312.8 | p = 0.0023 | 15.1 (±6.2) | 2.2 | 31.2 | p = 0.002 |
| Death | ||||||||
| Yes | 126.4 (±62.0) | 28.8 | 275.1 | 16.2 (±7.6) | 3.6 | 34.5 | ||
| No | 111.6 (±59.0) | 7.5 | 312.8 | p = 0.2871 | 15.5 (±6.4) | 2.2 | 33.9 | p = 0.677 |
| AUC | p * | |
|---|---|---|
| Model No DL | 0.7332 | Reference model |
| Model EAT | 0.7309 | 0.6452 |
| Model Ext_EAT | 0.7437 | 0.3169 |
| Model Lesion_Ext | 0.7995 | 0.0047 |
| Model EAT + Lesion_Ext | 0.7991 | 0.0047 |
| Model Ext_EAT + Lesion_Ext | 0.8047 | 0.0029 |
References
- Bertaso, A.G.; Bertol, D.; Duncan, B.B.; Foppa, M. Epicardial Fat: Definition, Measurements and Systematic Review of Main Outcomes. Arq. Bras. Cardiol. 2013, 101, e18–e28. [Google Scholar] [CrossRef] [PubMed]
- Gaborit, B.; Sengenes, C.; Ancel, P.; Jacquier, A.; Dutour, A. Role of Epicardial Adipose Tissue in Health and Disease: A Matter of Fat? Compr. Physiol. 2017, 7, 317-p. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.; Zhang, A.; Hamilton, D.J.; Deng, T. Epicardial Fat in the Maintenance of Cardiovascular Health. Methodist DeBakey Cardiovasc. J. 2017, 13, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahabadi, A.A.; Berg, M.H.; Lehmann, N.; Kälsch, H.; Bauer, M.; Kara, K.; Dragano, N.; Moebus, S.; Jöckel, K.H.; Erbel, R.; et al. Association of Epicardial Fat With Cardiovascular Risk Factors and Incident Myocardial Infarction in the General Population. J. Am. Coll. Cardiol. 2013, 61, 1388–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorter, P.M.; de Vos, A.M.; van der Graaf, Y.; Stella, P.R.; Doevendans, P.A.; Meijs, M.F.; Prokop, M.; Visseren, F.L. Relation of Epicardial and Pericoronary Fat to Coronary Atherosclerosis and Coronary Artery Calcium in Patients Undergoing Coronary Angiography. Am. J. Cardiol. 2008, 102, 380–385. [Google Scholar] [CrossRef] [PubMed]
- BMartínez-González, M.A.; García-López, M.; Bes-Rastrollo, M.; Toledo, E.; Martínez-Lapiscina, E.H.; Delgado-Rodriguez, M.; Vazquez, Z.; Benito, S.; Beunza, J.J. Pericardial fat is associated with carotid stiffness in the Multi-Ethnic Study of Atherosclerosis. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 332–338. [Google Scholar] [CrossRef] [Green Version]
- Raal, F.J.; Santos, R.D. Association of pericardial fat and coronary high-risk lesions as determined by cardiac CT. Atherosclerosis 2012, 222, 129–134. [Google Scholar] [CrossRef] [Green Version]
- Yerramasu, A.; Dey, D.; Venuraju, S.; Anand, D.V.; Atwal, S.; Corder, R.; Berman, D.S.; Lahiri, A. Increased volume of epicardial fat is an independent risk factor for accelerated progression of sub-clinical coronary atherosclerosis. Atherosclerosis 2011, 220, 223–230. [Google Scholar] [CrossRef]
- Malavazos, A.E.; Goldberger, J.J.; Iacobellis, G. Does epicardial fat contribute to COVID-19 myocardial inflammation? Eur. Hear. J. 2020, 41, 2333. [Google Scholar] [CrossRef]
- Pedersen, S.F.; Ho, Y.-C. SARS-CoV-2: A storm is raging. J. Clin. Investig. 2020, 130, 2202–2205. [Google Scholar] [CrossRef]
- Lasbleiz, A.; Gaborit, B.; Soghomonian, A.; Bartoli, A.; Ancel, P.; Jacquier, A.; Dutour, A. COVID-19 and Obesity: Role of Ectopic Visceral and Epicardial Adipose Tissues in Myocardial Injury. Front. Endocrinol. 2021, 12, 726967. [Google Scholar] [CrossRef] [PubMed]
- Özer, S.; Bulut, E.; Özyıldız, A.G.; Peker, M.; Turan, O.E. Myocardial injury in COVID-19 patients is associated with the thickness of epicardial adipose tissue. Kardiologiia 2021, 61, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Turker Duyuler, P.; Duyuler, S.; Demirtaş, B.; Çayhan, V. Epicardial and pericoronary adipose tissue in severe COVID-19 infection. Acta Cardiol. 2021, 76, 1–8. [Google Scholar] [CrossRef]
- Grodecki, K.; Lin, A.; Razipour, A.; Cadet, S.; McElhinney, P.A.; Chan, C.; Pressman, B.D.; Julien, P. Epicardial adipose tissue is associated with extent of pneumonia and adverse outcomes in patients with COVID-19. Metabolism 2020, 115, 154436. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Gan, H.; Jin, H.; Fang, Y.; Yang, Y.; Zhang, J.; Hu, X.; Chu, L. Epicardial adipose tissue, inflammatory biomarkers and COVID-19: Is there a possible relationship? Int. Immunopharmacol. 2020, 90, 107174. [Google Scholar] [CrossRef]
- Eslami, V.; Abrishami, A.; Zarei, E.; Khalili, N.; Baharvand, Z.; Sanei-Taheri, M. The Association of CT-measured Cardiac Indices with Lung Involvement and Clinical Outcome in Patients with COVID-19. Acad. Radiol. 2020, 28, 8–17. [Google Scholar] [CrossRef]
- Conte, C.; Esposito, A.; De Lorenzo, R.; Di Filippo, L.; Palmisano, A.; Vignale, D.; Leone, R.; Nicoletti, V.; Ruggeri, A.; Gallone, G.; et al. Epicardial adipose tissue characteristics, obesity and clinical outcomes in COVID-19: A post-hoc analysis of a prospective cohort study. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 2156–2164. [Google Scholar] [CrossRef]
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; van der Laak, J.A.W.M.; van Ginneken, B.; Sánchez, C.I. A survey on deep learning in medical image analysis. Med. Image Anal. 2017, 42, 60–88. [Google Scholar] [CrossRef] [Green Version]
- Coppini, G. Quantification of Epicardial Fat by Cardiac CT Imaging. Open Med. Inform. J. 2010, 4, 126–135. [Google Scholar] [CrossRef]
- Dey, D.; Wong, N.D.; Tamarappoo, B.; Nakazato, R.; Gransar, H.; Cheng, V.Y.; Ramesh, A.; Kakadiaris, I.; Germano, G.; Slomka, P.J.; et al. Computer-aided non-contrast CT-based quantification of pericardial and thoracic fat and their associations with coronary calcium and metabolic syndrome. Atherosclerosis 2010, 209, 136–141. [Google Scholar] [CrossRef] [Green Version]
- Volff, M.; Tonon, D.; Bommel, Y.; Peres, N.; Lagier, D.; Agard, G.; Jacquier, A.; Bartoli, A.; Carvelli, J.; Max, H.; et al. Factors Associated with 90-Day Mortality in Invasively Ventilated Patients with COVID-19 in Marseille, France. J. Clin. Med. 2021, 10, 5650. [Google Scholar] [CrossRef] [PubMed]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.-C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoang-Thi, T.-N.; Vakalopoulou, M.; Christodoulidis, S.; Paragios, N.; Revel, M.-P.; Chassagnon, G. Deep learning for lung disease segmentation on CT: Which reconstruction kernel should be used? Diagn. Interv. Imaging 2021, 102, 691–695. [Google Scholar] [CrossRef]
- Kim, W.H.; Kim, C.G.; Kim, D.-W. Optimal CT Number Range for Adipose Tissue When Determining Lean Body Mass in Whole-Body F-18 FDG PET/CT Studies. Nucl. Med. Mol. Imaging 2012, 46, 294–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Commandeur, F.; Goeller, M.; Betancur, J.; Cadet, S.; Doris, M.; Chen, X.; Berman, D.S.; Slomka, P.J.; Tamarappoo, B.K.; Dey, D. Deep Learning for Quantification of Epicardial and Thoracic Adipose Tissue From Non-Contrast CT. IEEE Trans. Med. Imaging 2018, 37, 1835–1846. [Google Scholar] [CrossRef] [PubMed]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 1–26 June 2016; pp. 770–778. [Google Scholar]
- Zhang, Z.; Wu, C.; Coleman, S.; Kerr, D. DENSE-INception U-net for medical image segmentation. Methods Programs Biomed. 2020, 192, 105395. [Google Scholar] [CrossRef]
- Slipczuk, L.; Castagna, F.; Schonberger, A.; Novogrodsky, E.; Sekerak, R.; Dey, D.; Jorde, U.P.; Levsky, J.M.; Garcia, M.J. Coronary artery calcification and epicardial adipose tissue as independent predictors of mortality in COVID-19. Int. J. Cardiovasc. Imaging 2021, 37, 3093–3100. [Google Scholar] [CrossRef]
- Nerlekar, N.; Brown, A.J.; Muthalaly, R.G.; Talman, A.; Hettige, T.; Cameron, J.D.; Wong, D.T.L. Association of Epicardial Adipose Tissue and High-Risk Plaque Characteristics: A Systematic Review and Meta-Analysis. J. Am. Hear. Assoc. 2017, 6, e006379. [Google Scholar] [CrossRef]
- Ding, X.; Terzopoulos, D.; Diaz-Zamudio, M.; Berman, D.S.; Slomka, P.J.; Dey, D. Automated pericardium delineation and epicardial fat volume quantification from noncontrast CT: Automated epicardial fat volume quantification from noncontrast CT. Med. Phys. 2015, 42, 5015–5026. [Google Scholar] [CrossRef]
- Militello, C.; Rundo, L.; Toia, P.; Conti, V.; Russo, G.; Filorizzo, C.; Maffei, E.; Cademartiri, F.; La Grutta, L.; Midiri, M.; et al. A semi-automatic approach for epicardial adipose tissue segmentation and quantification on cardiac CT scans. Comput. Biol. Med. 2019, 114, 103424. [Google Scholar] [CrossRef]
- Commandeur, F.; Goeller, M.; Razipour, A.; Cadet, S.; Hell, M.M.; Kwiecinski, J.; Chen, X.; Chang, H.-J.; Marwan, M.; Achenbach, S.; et al. Fully Automated CT Quantification of Epicardial Adipose Tissue by Deep Learning: A Multicenter Study. Radiol. Artif. Intell. 2019, 1, e190045. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Caruso, D.; Tuccinardi, D.; Risi, R.; Zerunian, M.; Polici, M.; Pucciarelli, F.; Tarallo, M.; Strigari, L.; Manfrini, S.; et al. Visceral fat shows the strongest association with the need of intensive care in patients with COVID-19. Metabolism 2020, 111, 154319. [Google Scholar] [CrossRef] [PubMed]
- Phan, F.; Boussouar, S.; Lucidarme, O.; Zarai, M.; Salem, J.-E.; Kachenoura, N.; Bouazizi, K.; Charpentier, E.; Niati, Y.; Bekkaoui, H.; et al. Cardiac adipose tissue volume and IL-6 level at admission are complementary predictors of severity and short-term mortality in COVID-19 diabetic patients. Cardiovasc. Diabetol. 2021, 20, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Sevilla, T.; Aparisi-Sanz, Á.; Aristizábal-Duque, C.; Gómez-Salvador, I.; Baladrón, C.; San Román, A. Epicardial adipose tissue attenuation in admitted patients with COVID-19. Rev. Esp. Cardiol. 2022, 75, 98–100. [Google Scholar] [CrossRef]
- Patel, V.B.; Mori, J.; McLean, B.A.; Basu, R.; Das, S.K.; Ramprasath, T.; Parajuli, N.; Penninger, J.M.; Grant, M.B.; Lopaschuk, G.D.; et al. ACE2 Deficiency Worsens Epicardial Adipose Tissue Inflammation and Cardiac Dysfunction in Response to Diet-Induced Obesity. Diabetes 2015, 65, 85–95. [Google Scholar] [CrossRef] [Green Version]
- Flinn, B.; Royce, N.; Gress, T.; Chowdhury, N.; Santanam, N. Dual role for angiotensin-converting enzyme 2 in Severe Acute Respiratory Syndrome Coronavirus 2 infection and cardiac fat. Obes. Rev. 2021, 22, e13225. [Google Scholar] [CrossRef]
- Shaihov-Teper, O.; Ram, E.; Ballan, N.; Brzezinski, R.Y.; Naftali-Shani, N.; Masoud, R.; Ziv, T.; Lewis, N.; Schary, Y.; Levin-Kotler, L.-P.; et al. Extracellular Vesicles From Epicardial Fat Facilitate Atrial Fibrillation. Circulation 2021, 143, 2475–2493. [Google Scholar] [CrossRef]
- Sun, K.; Xiao, B.; Liu, D.; Wang, J. Deep High-Resolution Representation Learning for Human Pose Estimation. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR), Long Beach, CA, USA, 16–20 June 2019; pp. 5686–5696. [Google Scholar]



| EAT Segmentation Model Dataset | EAT/COVID-19 Prognosis Dataset | ||
|---|---|---|---|
| Training Dataset (n = 95) | Testing Dataset (n = 20) | (n = 238) | |
| Gender | |||
| Male, n (%) | 49 (51.58) | 7 (35.00) | 143 (60.01) |
| Age | |||
| 18–44 years, n (%) | 16 (16.80) | 4 (20.00) | 32 (13.45) |
| 45–64 years, n (%) | 47 (49.47) | 9 (45.00) | 104 (43.70) |
| >64 years, n (%) | 32 (33.68) | 7 (35.00) | 102 (42.86) |
| Body mass index (kg/m2), mean (±SD), | 25.7 (±4.37) | 24.3 (±4.28) | 24.1 (±3.87) |
| Comorbidities | |||
| Diabetes, n (%) | 75 (78.94) | 14 (70.00) | 152 (63.4) |
| Hypertension, n (%) | 46 (98.42) | 11 (55.00) | 97 (40.7) |
| Underweight, n (%) | 0 (0.00) | 0 (0.00) | 3 (1.26) |
| Overweight, n (%) | 24 (25.26) | 7 (35.00) | 88 (36.9) |
| Obesity, n (%) | 18 (18.94) | 3 (15.00) | 47 (19.75) |
| Dyslipidemia, n (%) | 28 (29.47) | 6 (30.00) | 62 (26.05) |
| Coronary artery disease, n (%) | 11 (11.58) | 1 (5.00) | 44 (18.49) |
| Number of comorbidities | |||
| None, n (%) | 10 (10.52) | 2 (10.00) | 60 (25.21) |
| One, n (%) | 27 (28.42) | 5 (25.00) | 80 (33.61) |
| Two or more, n (%) | 58 (61.05) | 13 (65.00) | 98 (41.17) |
| Epicardial adipose tissue measures | |||
| Peri (cm3), mean (±SD) | 680.40 (±198.40) | 617.93 (±104.47) | 709.71 (±145.12) |
| Peri/BSA, (cm3/m2), mean | 359.78 | 328.16 | 365.41 |
| EAT (cm3), mean (±SD) | 119.17 (±71.36) | 115.47 (±49.12) | 112.83 (±59.30) |
| EAT/BSA (cm3/m2), mean | 63.05 | 61.32 | 58.83 |
| Ext_EAT (%), mean (±SD) | 17.51 (±21.64) | 18.68 (±22.14) | 15.60 (±6.50) |
| Delay symptoms—LDCT | |||
| Delay <7 days/asymptomatic, n (%) | x | x | 148 (62.18) |
| Delay ≥7 days, n (%) | x | x | 90 (37.82) |
| COVID-19 pulmonary lesions | |||
| Lesion _Ext (%), mean (± SD) | x | x | 8.88 (±10.83) |
| Clinical outcomes | |||
| Oxygen therapy, n (%) | x | x | 113 (47.48) |
| Hospitalization >10 days, n (%) | x | x | 46 (19.33) |
| ICU, n (%) | x | x | 30 (12.61) |
| Death, n (%) | x | x | 22 (9.24) |
| Hospitalization >10 days/ICU/death/oxygen therapy, n (%) | x | x | 128 (53.78) |
| O1a vs. Auto (n = 20) | O1a vs. O1b (n = 20) | O1a vs. O2 (n = 20) | |
|---|---|---|---|
| Technical Metrics | |||
| Peri | |||
| Mean Dice | 0.93 (±0.03) | 0.92 (±0.02) | 0.93 (±0.02) |
| Median Dice | 0.93 | 0.92 | 0.93 |
| EAT | |||
| Mean Dice | 0.85 (±0.05) | 0.85 (±0.04) | 0.86 (±0.03) |
| Median Dice | 0.87 | 0.85 | 0.86 |
| Clinical Metric: Volume | |||
| Peri | |||
| MAE (cm3) (mean ± SD) | 35.4 (±23.4) | 37.2 (±23.2) | 40.3 (±22.3) |
| Bias (cm3) (mean ± SD); p | −6.8 (±42.7); p = 0.6 | −22.4 (±38.3); p = 0.02 | −21.8 (±41.3); p = 0.04 |
| Corr. | 0.945 | 0.945 | 0.936 |
| EAT | |||
| MAE (cm3) (mean ± SD) | 11.7 (±8.1) | 12.0 (±9.1) | 14.9 (±11.2) |
| Bias (cm3) (mean ± SD); p | −4.0 (±13.9); p = 0.18 | −6.0 (±14.0); p = 0.06 | −12.8 (±13.6); p < 0.01 |
| Corr. | 0.963 | 0.962 | 0.970 |
| DL_Measures | Mean (±SD) | Minimum | Median | Max | Pearson Correlation Coefficient (p-Value) |
|---|---|---|---|---|---|
| EAT (cm3) | 112.8 ± 59.3 | 7.5 | 105.5 | 312.8 | |
| Lesion _Ext (%) | 8.9 ± 10.8 | 0.0 | 5.0 | 65.9 | 0.139 (0.037) |
| Ext_EAT (%) | 15.6 ± 6.5 | 2.2 | 15.0 | 34.6 | |
| Lesion _Ext (%) | 8.9 ± 10.8 | 0.0 | 5.0 | 65.9 | 0.043 (0.522) |
| Model No DL | Model Ext_EAT | Model Lesion_Ext | Model Ext_EAT + Lesion_Ext | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | OR | 95% CI | |||||
| Gender (Male vs. Female) | 2.92 | 1.65 | 5.15 | 2.96 | 1.66 | 5.29 | 2.35 | 1.27 | 4.38 | 2.33 | 1.23 | 4.40 |
| Age | 1.04 | 1.02 | 1.06 | 1.04 | 1.02 | 1.06 | 1.03 | 1.01 | 1.05 | 1.03 | 1.01 | 1.05 |
| Number of comorbidities (1 vs. 0) | 1.51 | 0.75 | 3.04 | 1.73 | 0.84 | 3.59 | 1.39 | 0.64 | 3.03 | 1.62 | 0.72 | 3.64 |
| Number of comorbidities (2 vs. 0) | 1.22 | 0.62 | 2.42 | 1.18 | 0.58 | 2.41 | 1.26 | 0.60 | 2.61 | 1.28 | 0.60 | 2.77 |
| Ext_EAT (%) | 1.04 | 1.00 | 1.09 | 1.05 | 0.99 | 1.10 | ||||||
| Lesion_Ext | 1.10 | 1.05 | 1.15 | 1.10 | 1.05 | 1.15 | ||||||
| Area Under Curve (AUC) | 0.733 | 0.744 (p * = 0.3169) | 0.800 (p * = 0.0047) | 0.805 (p * = 0.0029). | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bartoli, A.; Fournel, J.; Ait-Yahia, L.; Cadour, F.; Tradi, F.; Ghattas, B.; Cortaredona, S.; Million, M.; Lasbleiz, A.; Dutour, A.; et al. Automatic Deep-Learning Segmentation of Epicardial Adipose Tissue from Low-Dose Chest CT and Prognosis Impact on COVID-19. Cells 2022, 11, 1034. https://0-doi-org.brum.beds.ac.uk/10.3390/cells11061034
Bartoli A, Fournel J, Ait-Yahia L, Cadour F, Tradi F, Ghattas B, Cortaredona S, Million M, Lasbleiz A, Dutour A, et al. Automatic Deep-Learning Segmentation of Epicardial Adipose Tissue from Low-Dose Chest CT and Prognosis Impact on COVID-19. Cells. 2022; 11(6):1034. https://0-doi-org.brum.beds.ac.uk/10.3390/cells11061034
Chicago/Turabian StyleBartoli, Axel, Joris Fournel, Léa Ait-Yahia, Farah Cadour, Farouk Tradi, Badih Ghattas, Sébastien Cortaredona, Matthieu Million, Adèle Lasbleiz, Anne Dutour, and et al. 2022. "Automatic Deep-Learning Segmentation of Epicardial Adipose Tissue from Low-Dose Chest CT and Prognosis Impact on COVID-19" Cells 11, no. 6: 1034. https://0-doi-org.brum.beds.ac.uk/10.3390/cells11061034