
Evaluation of a “Picture Assisted Illustration Reinforcement” (PAIR) System for Oral Hygiene in Children with Autism: A Double-Blind Randomized Controlled Trial

 ,
, 
 ,
,
Abstract
:1. Introduction
1.1. Null Hypothesis
1.2. Alternative Hypothesis
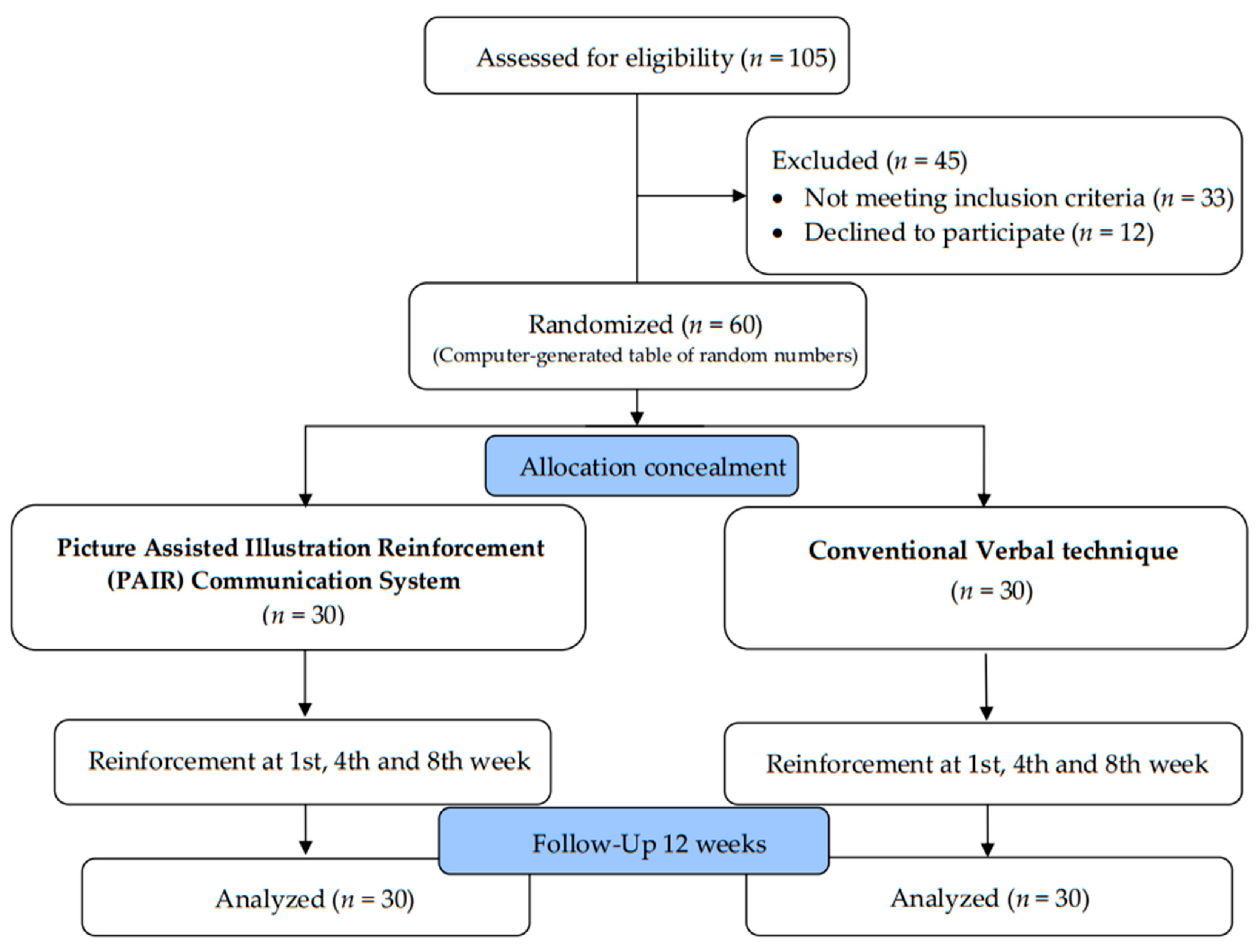
2. Materials and Methods
2.1. Study Design and Study Setting
2.2. Ethical Considerations
2.3. Pilot Study
2.4. Sample Size Estimation
2.5. Inclusion and Exclusion Criteria
2.6. Phases of Study Conduct
2.6.1. Preparatory Phase
2.6.2. Cognitive and Pre-Evaluation Phase
2.6.3. Intervention Phase
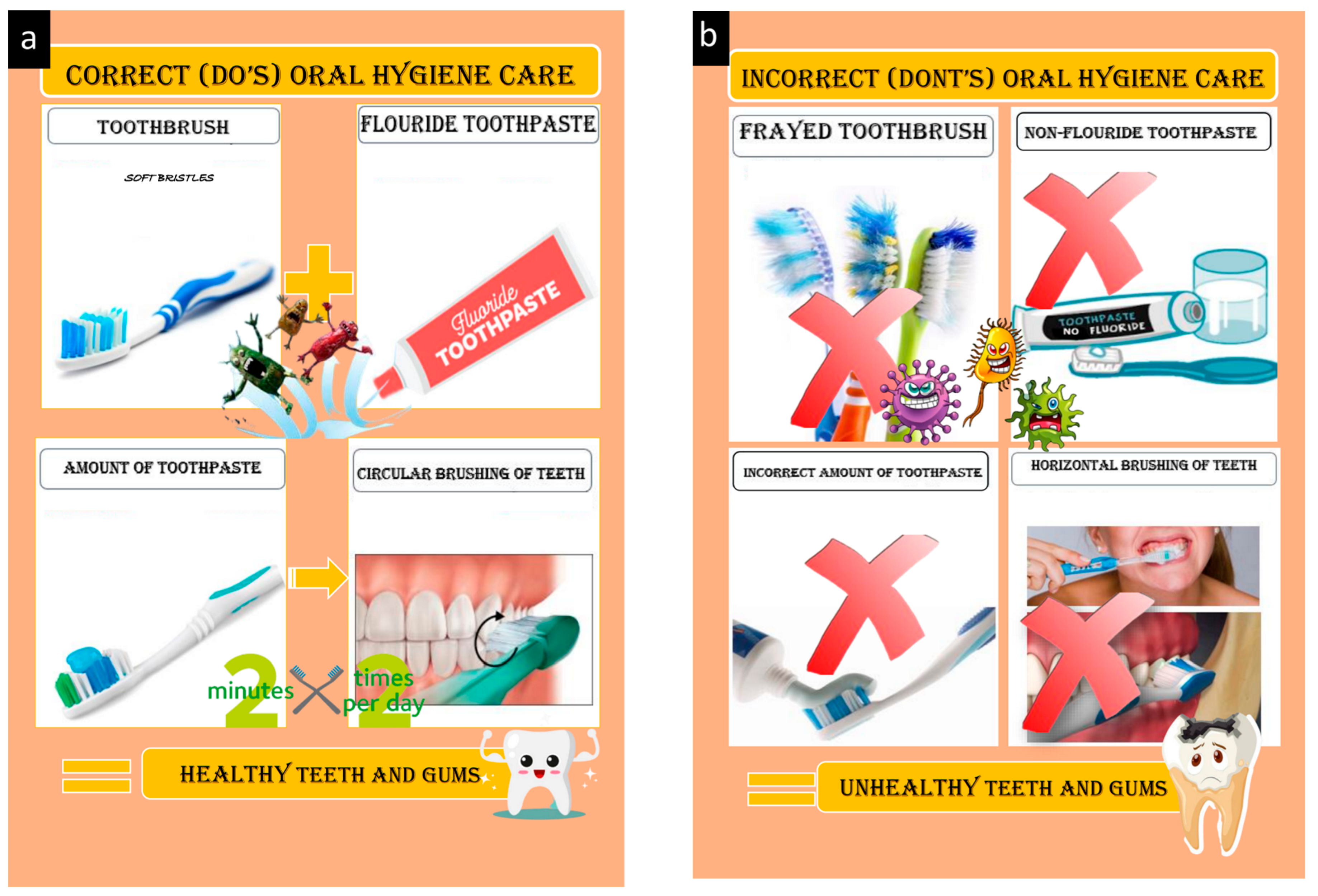
PAIR Technique
Conventional Technique
2.6.4. Post-Intervention at 12th Week
2.7. Statistical Analysis
3. Results
3.1. Cognition and Sociodemographic Status of the Children
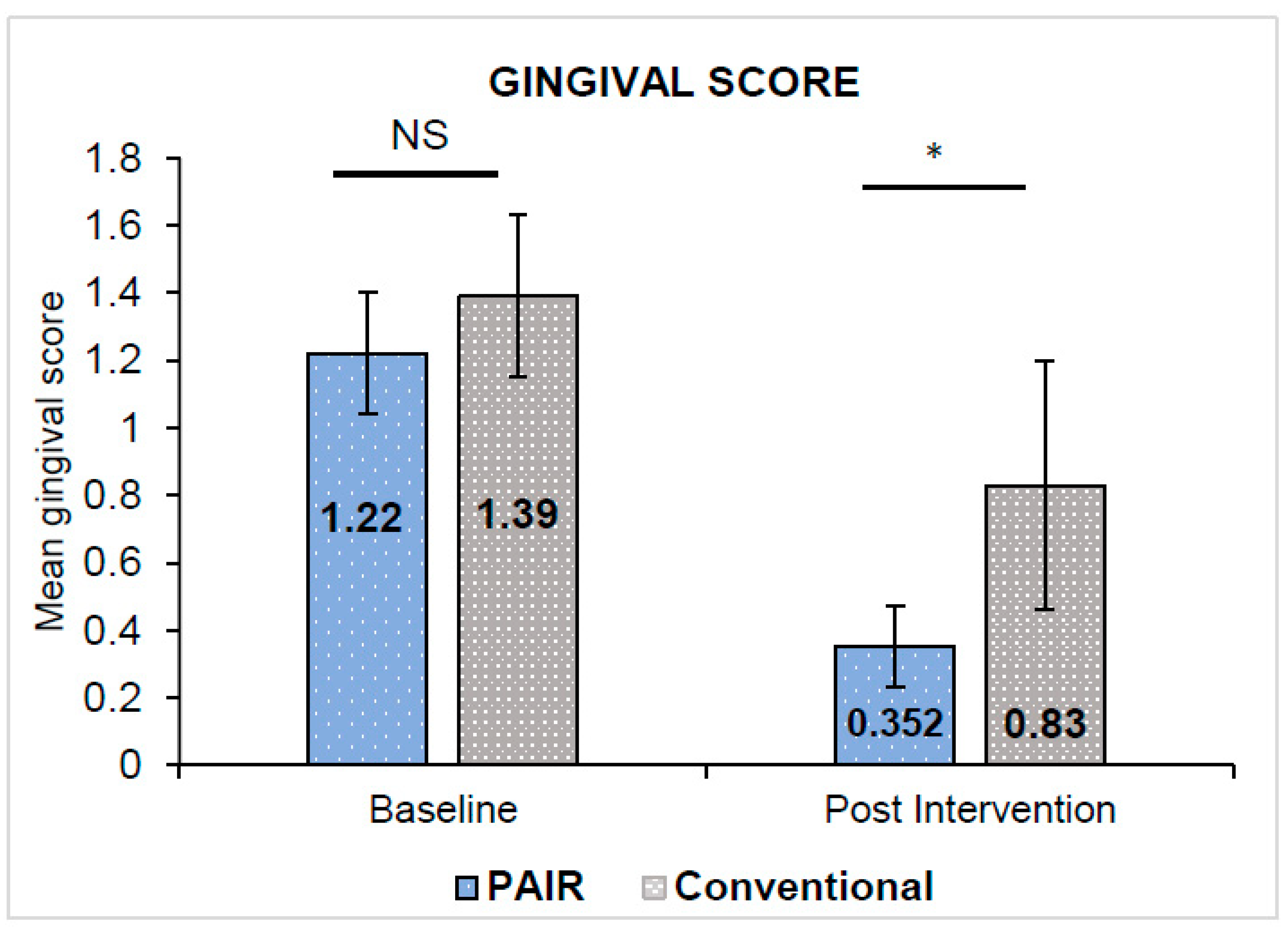
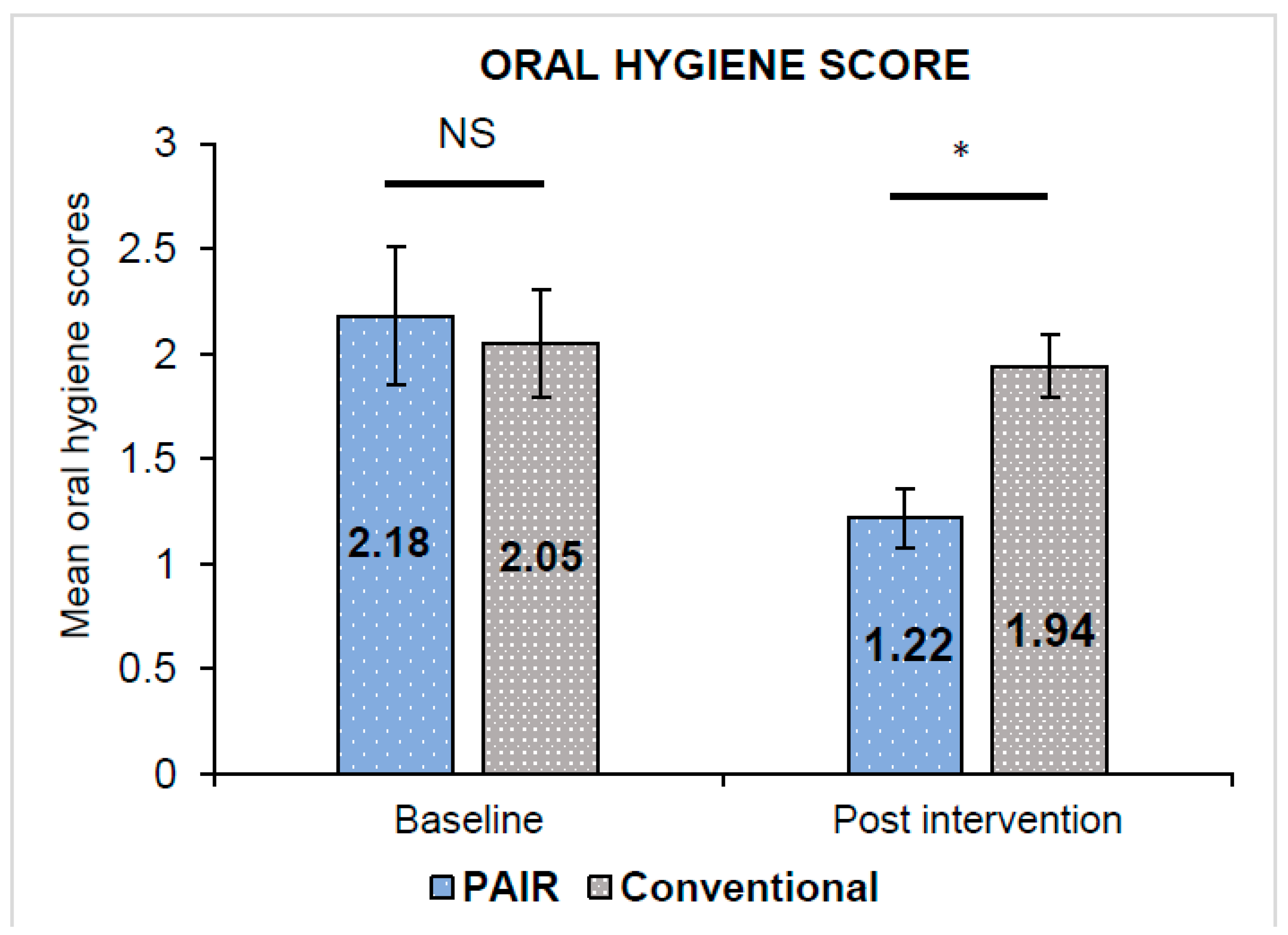
3.2. Oral Health Conditions among the Children
3.3. Caregiver Perception of Oral Hygiene Practices among the Children
4. Discussion
4.1. Strength and Limitations
4.2. Clinical Significance
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chandrashekhar, S.; Bommangoudar, J.S. Management of autistic patients in dental office: A clinical update. Int. J. Clin. Pediatr. Dent. 2018, 11, 219. [Google Scholar]
- DSM-5 American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Frye, R.E. Social skills deficits in autism spectrum disorder: Potential biological origins and progress in developing therapeutic agents. CNS Drugs 2018, 32, 713–734. [Google Scholar] [CrossRef]
- US Department of Health and Human Services. Autism Spectrum Disorder: Communication Problems in Children; National Institute on Deafness and Other Communication Disorders [NIDCD]: Bethesda, MD, USA, 2017.
- Myers, S.M.; Johnson, C.P. Management of children with autism spectrum disorders. Pediatrics 2007, 120, 1162–1182. [Google Scholar] [CrossRef] [PubMed]
- Karimi, P.; Kamali, E.; Mousavi, S.M.; Karahmadi, M. Environmental factors influencing the risk of autism. J. Res. Med. Sci. 2017, 22, 27. [Google Scholar]
- Sarnat, H.; Samuel, E.; Ashkenazi-Alfasi, N.; Peretz, B. Oral health characteristics of preschool children with autistic syndrome disorder. J. Clin. Pediatr. Dent. 2016, 40, 21–25. [Google Scholar] [CrossRef]
- Jaber, M.A. Dental caries experience, oral health status and treatment needs of dental patients with autism. J. Appl. Oral Sci. 2011, 19, 212–217. [Google Scholar] [CrossRef]
- Ide-Okochi, A.; Funayama, H.; Asada, Y. Pediatric dentists’ perspectives of children with special health care needs in Japan: Developmental disabilities, phobia, maltreatment, and multidisciplinary collaboration. BMC Pediatr. 2021, 21, 240. [Google Scholar] [CrossRef]
- El Khatib, A.A.; El Tekeya, M.M.; El Tantawi, M.A.; Omar, T. Oral health status and behaviours of children with Autism Spectrum Disorder: A case–control study. Int. J. Paediatr. Dent. 2014, 24, 314–323. [Google Scholar] [CrossRef] [PubMed]
- Hodges, H.; Fealko, C.; Soares, N. Autism spectrum disorder: Definition, epidemiology, causes, and clinical evaluation. Transl. Pediatr. 2020, 9, S55. [Google Scholar] [CrossRef]
- Rodgers, M.; Simmonds, M.; Marshall, D.; Hodgson, R.; Stewart, L.A.; Rai, D.; Wright, K.; Ben-Itzchak, E.; Eikeseth, S.; Eldevik, S.; et al. Intensive behavioural interventions based on applied behaviour analysis for young children with autism: An international collaborative individual participant data meta-analysis. Autism 2021, 25, 1137–1153. [Google Scholar] [CrossRef]
- Magiati, I.; Howlin, P. A pilot evaluation study of the Picture Exchange Communication System (PECS) for children with autistic spectrum disorders. Autism 2003, 7, 297–320. [Google Scholar] [CrossRef]
- Al-Batayneh, O.B.; Nazer, T.S.; Khader, Y.S.; Owais, A.I. Effectiveness of a tooth-brushing programme using the picture exchange communication system (PECS) on gingival health of children with autism spectrum disorders. Eur. Arch. Paediatr. Dent. 2020, 21, 277–283. [Google Scholar] [CrossRef]
- Bondy, A.S.; Frost, L.A. The picture exchange communication system. Focus Autistic Behav. 1994, 9, 1–9. [Google Scholar] [CrossRef]
- Howlin, P.; Gordon, R.K.; Pasco, G.; Wade, A.; Charman, T. The effectiveness of Picture Exchange Communication System (PECS) training for teachers of children with autism: A pragmatic, group randomised controlled trial. J. Child Psychol. Psychiatry 2007, 48, 473–481. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines; World Health Organization: Geneva, Switzerland, 1992. [Google Scholar]
- Regier, D.A.; Kuhl, E.A.; Kupfer, D.J. The DSM-5: Classification and criteria changes. World Psychiatry 2013, 12, 92–98. [Google Scholar] [CrossRef]
- World Health Organization. Oral Health Surveys: Basic Methods; World Health Organization: Geneva, Switzerland, 2013. [Google Scholar]
- Greene, J.C.; Vermillion, J.R. The simplified oral hygiene index. J. Am. Dent. Assoc. 1964, 68, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Loe, H. The gingival index, the plaque index and the retention index systems. J. Periodontol. 1967, 38, 610–616. [Google Scholar] [CrossRef]
- Baron-Cohen, S.; Wheelwright, S.; Skinner, R.; Martin, J.; Clubley, E. The autism-spectrum quotient (AQ): Evidence from asperger syndrome/high-functioning autism, malesand females, scientists and mathematicians. J. Autism Dev. Disord. 2001, 31, 5–17. [Google Scholar] [CrossRef]
- Al Rashed, W.A.; Shihah, A.S.; Alhomoud, A.S.; Alharbi, M.M.; Shadid, A.M.; Alghamdi, M.A.; Alfaris, A.; Alrashed, A.W.; Osman, E.A.; Khandekar, R. Knowledge, attitude, and practice toward glaucoma and its management among adult Saudi patients. Saudi J. Ophthalmol. 2020, 34, 261. [Google Scholar]
- Koritsas, S.; Iacono, T. Secondary conditions in people with developmental disability. Am. J. Intellect. Dev. Disabil. 2011, 116, 36–47. [Google Scholar] [CrossRef]
- Como, D.H.; Stein Duker, L.I.; Polido, J.C.; Cermak, S.A. Oral health and Autism Spectrum Disorders: A unique collaboration between dentistry and occupational therapy. Int. J. Environ. Res. Public Health. 2021, 18, 135. [Google Scholar] [CrossRef] [PubMed]
- Alumran, A.; Almulhim, L.; Almolhim, B.; Bakodah, S.; Aldossary, H.; Alakrawi, Z. Preparedness and willingness of dental care providers to treat patients with special needs. Clin. Cosmet. Investig. Dent. 2018, 10, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Formicola, A.J.; Bailit, H.L.; Weintraub, J.A.; Fried, J.L.; Polverini, P.J. Advancing Dental Education in the 21st Century: Phase 2 Report on Strategic Analysis and Recommendations. J. Dent. Educ. 2018, 82, eS1–eS32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, L.I.; Polido, J.C.; Najera, S.O.; Cermak, S.A. Oral care experiences and challenges in children with autism spectrum disorders. Pediatr Dent. 2012, 34, 387–391. [Google Scholar] [PubMed]
- Shapira, J.; Mann, J.; Tamari, I.; Mester, R.; Knobler, H.; Yoeli, Y.; Newbrun, E. Oral health status and dental needs of an autistic population of children and young adults. Spec Care Dent. 1989, 9, 38–41. [Google Scholar] [CrossRef]
- Johnson, N.L.; Rodrigues, D. Children with autism spectrum disorder at a pediatric hospital: A systematic review of the literature. Pediatr. Nurs. 2013, 39, 131–141. [Google Scholar]
- Accreditation Standards for Dental Education Programs; American Dental Association: Chicago, IL, USA, 2004; Available online: https://coda.ada.org/en/accreditation (accessed on 10 November 2022).
- Pini, D.M.; Fröhlich, P.C.; Rigo, L. Oral health evaluation in special needs individuals. Einstein 2016, 14, 501–507. [Google Scholar] [CrossRef]
- Mehta, A.; Gupta, R.; Mansoob, S.; Mansoori, S. Assessment of oral health status of children with special needs in Delhi, India. Rev. Sul-Bras. De Odontol. 2015, 12, 239–246. [Google Scholar]
- Charman, T.; Pickles, A.; Simonoff, E.; Chandler, S.; Loucas, T.; Baird, G. IQ in children with autism spectrum disorders: Data from the Special Needs and Autism Project (SNAP). Psychol. Med. 2011, 41, 619–627. [Google Scholar] [CrossRef]
- Edirisooriya, M.; Dykiert, D.; Auyeung, B. IQ and Internalising Symptoms in Adolescents with ASD. J. Autism Dev. Disord. 2021, 51, 3887–3907. [Google Scholar] [CrossRef]
- Afif, I.Y.; Manik, A.R.; Munthe, K.; Maula, M.I.; Ammarullah, M.I.; Jamari, J.; Winarni, T.I. Physiological Effect of Deep Pressure in Reducing Anxiety of Children with ASD during Traveling: A Public Transportation Setting. Bioengineering 2022, 9, 157. [Google Scholar] [CrossRef] [PubMed]
- Lefer, G.; Rouches, A.; Bourdon, P.; Lopez Cazaux, S. Training children with autism spectrum disorder to undergo oral assessment using a digital iPad® application. Eur. Arch. Paediatr. Dent. 2019, 20, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Pilebro, C.; Bäckman, B. Teaching oral hygiene to children with autism. Int. J. Paediatr. Dent. 2005, 15, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Morales-Chávez, M.C. Oral health assessment of a group of children with autism disorder. J. Clin. Pediatr. Dent. 2017, 41, 147–149. [Google Scholar] [CrossRef] [PubMed]
- Marra, P.M.; Parascandolo, S.; Fiorillo, L.; Cicciù, M.; Cervino, G.; D’Amico, C.; De Stefano, R.; Salerno, P.; Esposito, U.; Itro, A. Dental Trauma in Children with Autistic Disorder: A Retrospective Study. Biomed. Res. Int. 2021, 8, 3125251. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.S.; Deshpande, A.P.; Ankola, A.V.; Sankeshwari, R.M.; Hampiholi, V.; Hebbal, M.; Jalihal, S.; Pai Khot, A.J.; Valakkunja, D.; Kotha, S.L. Impact of the Visual Performance Reinforcement Technique on Oral Hygiene Knowledge and Practices, Gingival Health, and Plaque Control in Hearing-and Speech-Impaired Adolescents: A Randomized Controlled Trial. Children 2022, 9, 1905. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cognition | Groups | Gender | ||||
|---|---|---|---|---|---|---|
| PAIR n (%) | Conventional n (%) | p-Value | Male n (%) | Female n (%) | p-Value | |
| ASQ (Mean ± SD) | 128.47 ± 16.52 | 127.58 ± 18.14 | 0.084 α | 126.22 ± 17.37 | 129.37 ± 20.28 | 0.062 α |
| VSMS (Mean ± SD) | 58.26 ± 12.23 | 62.37 ± 10.55 | 0.072 α | 55.67 ± 10.79 | 60.00 ± 3.46 | <0.001 α,* |
| IQ | 0.059 β | <0.001 β,** | ||||
| Intellectually superior | 4 (13.33%) | 5 (16.67%) | 1 (2.63%) | 2 (9.09%) | ||
| Definitely above average | 4 (13.33%) | 3 (10%) | 2 (5.26%) | 5 (22.7%) | ||
| Intellectually average | 12 (40%) | 16 (53.33%) | 20 (52.63%) | 7 (31.82%) | ||
| Definitely below average | 9 (30%) | 4 (13.33%) | 14 (36.84%) | 4 (18.18%) | ||
| Intellectually impaired | 1 (3.33%) | 2 (6.67%) | 1 (2.63%) | 4 (18.18%) | ||
| Frankl Behavioural scale | 0.066 β | 0.034 β* | ||||
| Definitely positive | 7 (23.33%) | 5 (16.67%) | 7 (18.42%) | 2 (9.09%) | ||
| Positive | 18 (60%) | 17 (56.67%) | 26 (68.4%) | 14 (63.64%) | ||
| Negative | 5 (16.67%) | 8 (26.67%) | 5 (13.16%) | 6 (27.27%) | ||
| Oral Health Conditions | PAIR Group n (%) = 30 | Conventional Group n (%) = 30 | Total n (%) = 60 | p-Value |
|---|---|---|---|---|
| Caries experience—DMFT (Mean ± SD) | 2.40 ± 0.12 | 2.70 ± 0.23 | 5.10 ± 0.350 | 0.247 ȶ |
| Oral hygiene status | 0.078 ɤ | |||
| Good | 5 (16.67%) | 8 (26.67%) | 13 (21.66%) | |
| Fair | 9 (30%) | 7 (23.33%) | 16 (26.67%) | |
| Poor | 16 (53.33%) | 15 (50%) | 31 (51.67%) | |
| Gingivitis | 0.067 ɤ | |||
| None or Mild | 14 (46.67%) | 12 (40%) | 26 (43.33%) | |
| Moderate | 9 (30%) | 10 (33.33%) | 19 (31.67%) | |
| Severe | 7 (23.33%) | 8 (26.67%) | 15 (25%) | |
| Dental trauma | 0.043 ɤ,* | |||
| No trauma | 18 (60%) | 16 (53.33%) | 34 (56.66%) | |
| Enamel fracture | 8 (26.67%) | 11 (36.67%) | 19 (31.67%) | |
| Treated injury | 4 (13.33%) | 3 (10%) | 7 (11.67%) | |
| Oral mucosal lesions | 0.025 ɤ, | |||
| No abnormal condition | 25 (83.34%) | 21 (70%) | 46 (76.67%) | |
| Ulceration | 4 (13.33%) | 6 (20%) | 10 (16.66%) | |
| Soft tissue lesion | 1 (3.33%) | 3 (10%) | 4 (6.67%) | |
| Response Frequencies n (%) | ||||||||
|---|---|---|---|---|---|---|---|---|
| Sl. No | Questions | PAIR Technique (n = 30) | Conventional Technique (n = 30) | |||||
| Pre-Health Education | Post-Health Education | p-Value | Pre-Health Education | Post-Health Education | p-Value | |||
| 1. | How does the child clean his/her teeth? | Brush | 18 (60%) | 26 (86.7%) | <0.001 ¥,** | 16 (53.3%) | 21 (70%) | <0.001 ¥,** |
| Finger | 12 (40%) | 4 (13.3%) | 14 (46.7%) | 9 (30%) | ||||
| 2. | In which direction does the child brush his/her teeth? | Vertical | 7 (23.3%) | 0 | 0.004 ¶,** | 5 (16.7%) | 3 (10%) | 0.057 ¶ |
| Horizontal | 13 (43.4%) | 7 (23.3%) | 14 (46.7%) | 12 (40%) | ||||
| Circular | 4 (13.3%) | 23 (76.7%) | 3 (10%) | 8 (26.7%) | ||||
| Any other | 6 (20%) | 0 | 8 (26.6%) | 7 (23.3%) | ||||
| 3. | How many times does the child brush his/her teeth in a day? | Once | 21 (70%) | 6 (20%) | 0.001 ¶,** | 21 (70%) | 17 (56.7%) | <0.001 ¶,** |
| Twice | 5 (16.7%) | 16 (53.3%) | 4 (13.3%) | 9 (30%) | ||||
| After every meal | 1 (3.3%) | 8 (26.7%) | 1 (3.3%) | 1 (3.3%) | ||||
| Don’t clean everyday | 3 (10%) | 0 | 4 (13.3%) | 3 (10%) | ||||
| 4. | When does the child clean his/her teeth? | Before meal | 11 (36.7%) | 9 (30%) | 0.082 ¥ | 16 (53.3%) | 4 (13.3%) | 0.063 ¥ |
| After meal | 19 (63.3%) | 21 (70%) | 14 (46.7%) | 26 (86.7%) | ||||
| 5. | What does the child use to clean his/her teeth? | Toothpaste | 24 (80%) | 29 (96.7%) | 0.746 ¥ | 26 (86.7%) | 28 (93.3%) | 0.951 ¥ |
| Toothpowder | 6 (20%) | 1 (3.3%) | 4 (13.3%) | 2 (6.7%) | ||||
| 6. | How often does the child change their toothbrush? | 1–3 months | 2 (6.7%) | 22 (73.3%) | 0.003 ¶,** | 2 (6.7%) | 7 (23.4%) | <0.001 ¶,** |
| 4–6 months | 9 (30%) | 5 (16.7%) | 10 (33.3%) | 10 (33.3%) | ||||
| 6 months | 6 (20%) | 3 (10%) | 4 (13.3%) | 4 (13.3%) | ||||
| Not applicable | 13 (43.3%) | 0 | 14 (46.7%) | 9 (30%) | ||||
| 7. | How often does the child rinse his/her mouth with water after eating? | Always | 4 (13.3%) | 11 (36.7%) | 0.369 ¶ | 6 (20%) | 9 (30%) | 0.448 ¶ |
| Sometimes | 9 (30%) | 17 (56.6%) | 17 (56.7%) | 18 (60%) | ||||
| Never | 17 (56.7%) | 2 (6.7%) | 7 (23.3%) | 3 (10%) | ||||
| 8. | Does the child use any other oral hygiene aids? | Yes | 2 (6.7%) | 9 (30%) | 0.527 ¥ | 2 (6.7%) | 8 (26.7%) | 0.762 ¥ |
| No | 28 (93.3%) | 21 (70%) | 28 (93.3%) | 22 (73.3%) | ||||
| Practice | PAIR Technique (n = 30) | Conventional Verbal Technique (n = 30) | Statistics | |||
|---|---|---|---|---|---|---|
| Mean ± SD | 95% CI | Mean ± SD | 95% CI | t-Value | p-Value || | |
| Before intervention | 2.53 ± 1.25 | 2.07–3.00 | 2.47 ± 1.38 | 1.95–2.98 | −0.023 | 0.846 |
| After intervention | 5.50 ± 1.12 | 5.05–5.95 | 3.57 ± 1.10 | 3.15–3.98 | 5.842 | <0.001 ** |
| t-value | −13.049 | −4.387 | ||||
| 95% CI | −3.43 to −2.50 | −1.61 to −0.59 | ||||
| p-Value § | <0.001 ** | <0.001 ** | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pai Khot, A.J.; Choudhury, A.R.; Ankola, A.V.; Sankeshwari, R.M.; Hampiholi, V.; Hebbal, M.; Jalihal, S.; Kumar, R.S.; Kabra, L.; Kotha, S.L. Evaluation of a “Picture Assisted Illustration Reinforcement” (PAIR) System for Oral Hygiene in Children with Autism: A Double-Blind Randomized Controlled Trial. Children 2023, 10, 369. https://0-doi-org.brum.beds.ac.uk/10.3390/children10020369
Pai Khot AJ, Choudhury AR, Ankola AV, Sankeshwari RM, Hampiholi V, Hebbal M, Jalihal S, Kumar RS, Kabra L, Kotha SL. Evaluation of a “Picture Assisted Illustration Reinforcement” (PAIR) System for Oral Hygiene in Children with Autism: A Double-Blind Randomized Controlled Trial. Children. 2023; 10(2):369. https://0-doi-org.brum.beds.ac.uk/10.3390/children10020369
Chicago/Turabian StylePai Khot, Atrey J., Abhra Roy Choudhury, Anil V. Ankola, Roopali M. Sankeshwari, Vinuta Hampiholi, Mamata Hebbal, Sagar Jalihal, Ram Surath Kumar, Laxmi Kabra, and Sree Lalita Kotha. 2023. "Evaluation of a “Picture Assisted Illustration Reinforcement” (PAIR) System for Oral Hygiene in Children with Autism: A Double-Blind Randomized Controlled Trial" Children 10, no. 2: 369. https://0-doi-org.brum.beds.ac.uk/10.3390/children10020369