

Hospital Factors Associated with the Survival of Infants Born at Periviable Gestation: The USA National Database
 , ,
, ,
Abstract
:1. Background
2. Methods
2.1. Data Sources and Management
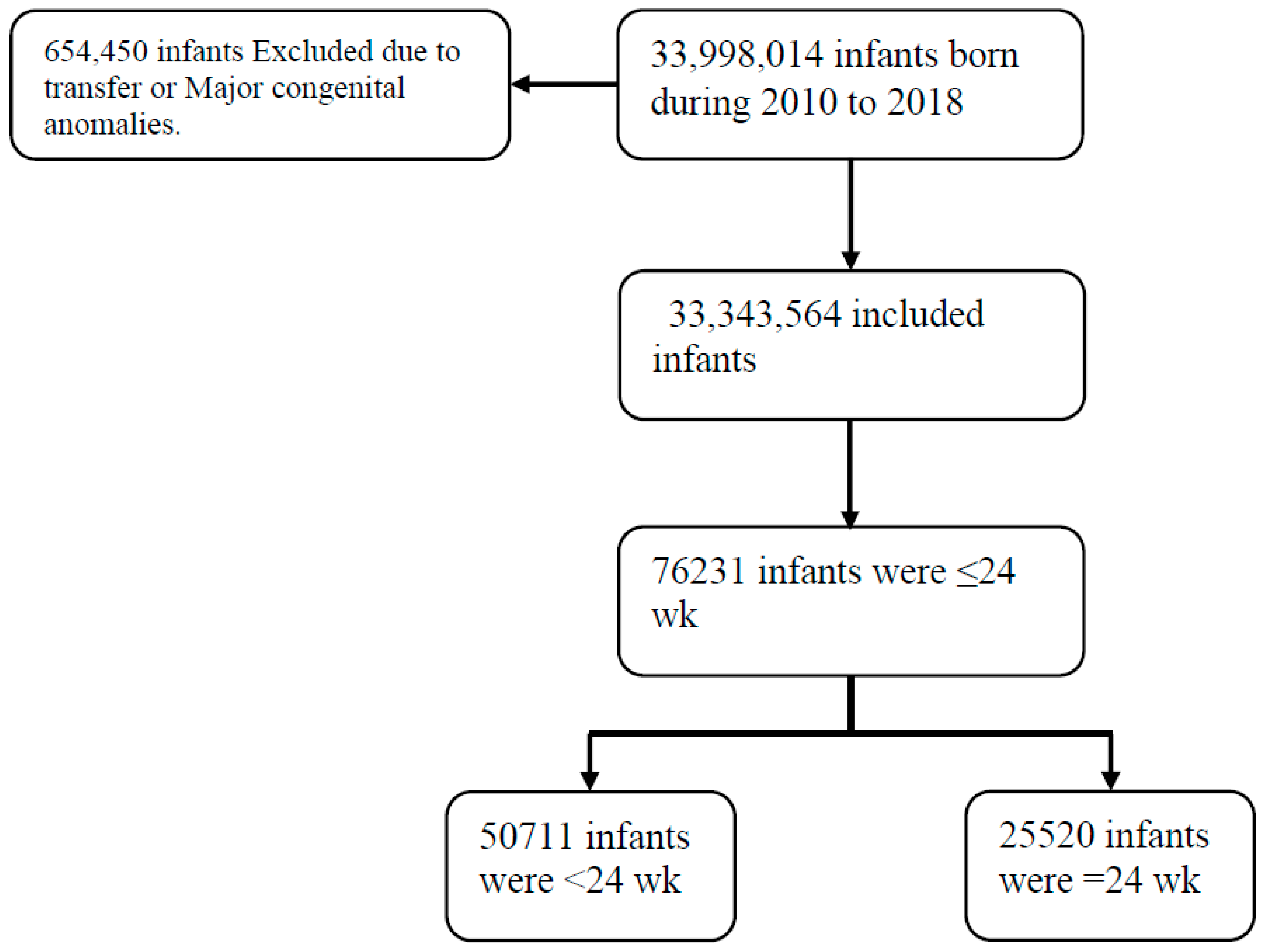
2.2. Study Design and Population
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Heart Association. 2005 American Heart Association (AHA) guidelines for cardiopulmonary resuscitation (CPR) and emergency cardiovascular care (ECC) of pediatric and neonatal patients: Pediatric basic life support. Pediatrics 2006, 117, e989–e1004. [Google Scholar] [CrossRef] [PubMed]
- Ecker, J.L.; Kaimal, A.; Mercer, B.M.; Blackwell, S.C.; DeRegnier, R.A.O.; Farrell, R.M.; Grobman, W.A.; Resnik, J.L.; Sciscione, A.C.; American College of Obstetricians and Gynecologists. #3: Periviable birth. Am. J. Obstet. Gynecol. 2015, 213, 604–614. [Google Scholar] [PubMed]
- Kelly, K.; Meaney, S.; Leitao, S.; O’Donoghue, K. A review of stillbirth definitions: A rationale for change. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 256, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Mehler, K.; Oberthuer, A.; Keller, T.; Becker, I.; Valter, M.; Roth, B.; Kribs, A. Survival Among Infants Born at 22 or 23 Weeks’ Gestation Following Active Prenatal and Postnatal Care. JAMA Pediatr. 2016, 170, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Stoll, B.J.; Hansen, N.I.; Bell, E.F.; Walsh, M.C.; Carlo, W.A.; Shankaran, S.; Laptook, A.R.; Sánchez, P.J.; Van Meurs, K.P.; Wyckoff, M.; et al. Trends in Care Practices, Morbidity, and Mortality of Extremely Preterm Neonates, 1993–2012. JAMA 2015, 314, 1039–1051. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.M.; Rysavy, M.A.; Bell, E.F.; Tyson, J.E. Survival of Infants Born at Periviable Gestational Ages. Clin. Perinatol. 2017, 44, 287–303. [Google Scholar] [CrossRef] [PubMed]
- Martin, J.A.; Hamilton, B.E.; Osterman, M.J.K.; Driscoll, A.K.; Mathews, T.J. Births: Final Data for 2015. Natl. Vital. Stat. Rep. 2017, 66, 1. [Google Scholar] [PubMed]
- Martin, J.A.; Hamilton, B.E.; Osterman, M.J.; Curtin, S.C.; Matthews, T.J. Births: Final data for 2013. Natl. Vital. Stat. Rep. 2015, 64, 1–65. [Google Scholar] [PubMed]
- Checchia, P.A.; McCollegan, J.; Daher, N.; Kolovos, N.; Levy, F.; Markovitz, B. The effect of surgical case volume on outcome after the Norwood procedure. J. Thorac. Cardiovasc. Surg. 2005, 129, 754–759. [Google Scholar] [CrossRef] [PubMed]
- Barrett, M.; Coffey, R.; Levit, K. Population Denominator Data Sources and Data for Use with the HCUP Databases (Updated with 2020 Population Data). HCUP Methods Series Report # 2021-04 ONLINE. U.S. Agency for Healthcare Research and Quality. 15 December 2021. Available online: www.hcup-us.ahrq.gov/reports/methods/methods.jsp (accessed on 26 December 2021).
- Phibbs, C.S.; Baker, L.C.; Caughey, A.B.; Danielsen, B.; Schmitt, S.K.; Phibbs, R.H. Level and volume of neonatal intensive care and mortality in very-low-birth-weight infants. N. Engl. J. Med. 2007, 356, 2165–2175. [Google Scholar] [CrossRef] [PubMed]
- Binder, S.; Hill, K.; Meinzen-Derr, J.; Greenberg, J.M.; Narendran, V. Increasing VLBW deliveries at subspecialty perinatal centers via perinatal outreach. Pediatrics 2011, 127, 487–493. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, F.; Robinson, B.K.; Tucker Edmonds, B. Do maternal characteristics influence maternal-fetal medicine physicians’ willingness to intervene when managing periviable deliveries? J. Perinatol. 2016, 36, 522–528. [Google Scholar] [CrossRef] [PubMed]
- Arbour, K.; Lindsay, E.; Laventhal, N.; Myers, P.; Andrews, B.; Klar, A.; Dunbar, A.E., III. Shifting Provider Attitudes and Institutional Resources Surrounding Resuscitation at the Limit of Gestational Viability. Am. J. Perinatol. 2022, 39, 869–877. [Google Scholar]
- Bartels, D.B.; Wypij, D.; Wenzlaff, P.; Dammann, O.; Poets, C.F. Hospital volume and neonatal mortality among very low birth weight infants. Pediatrics 2006, 117, 2206–2214. [Google Scholar] [CrossRef] [PubMed]
- Mercer, B.M. Periviable Birth and the Shifting Limit of Viability. Clin. Perinatol. 2017, 44, 283–286. [Google Scholar] [CrossRef] [PubMed]
- Ishii, N.; Kono, Y.; Yonemoto, N.; Kusuda, S.; Fujimura, M.; Neonatal Research Network, Japan. Outcomes of infants born at 22 and 23 weeks’ gestation. Pediatrics 2013, 132, 62–71. [Google Scholar] [CrossRef] [PubMed]
- Venkatesh, K.K.; Lynch, C.D.; Costantine, M.M.; Backes, C.H.; Slaughter, J.L.; Frey, H.A.; Huang, X.; Landon, M.B.; Klebanoff, M.A.; Khan, S.S.; et al. Trends in Active Treatment of Live-born Neonates Between 22 Weeks 0 Days and 25 Weeks 6 Days by Gestational Age and Maternal Race and Ethnicity in the US, 2014 to 2020. JAMA 2022, 328, 652–662. [Google Scholar] [CrossRef] [PubMed]
- Younge, N.; Goldstein, R.F.; Bann, C.M.; Hintz, S.R.; Patel, R.M.; Smith, P.B.; Bell, E.F.; Rysavy, M.A.; Duncan, A.F.; Vohr, B.R.; et al. Survival and neurodevelopmental outcomes among periviable infants. N. Engl. J. Med. 2017, 376, 617–628. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| <24-Week GA | Completed 24-Week GA | ||||||
|---|---|---|---|---|---|---|---|
| Total | Alive (%) | p-Value | Total | Alive (%) | p-Value | ||
| Location/teaching status of hospital | Rural | 2258 | 75 (3.3) | 345 | 138 (40) | ||
| Urban non-teaching | 9352 | 824 (8.8) | 2962 | 1654 (55.8) | |||
| Urban teaching | 38,762 | 7171 (18.5) | 22,094 | 13,820 (62.6) | |||
| <0.001 | <0.001 | ||||||
| Region of the hospital | Northeast | 8740 | 1090 (12.5) | 3584 | 1990 (55.5) | ||
| Midwest | 11,677 | 1928 (16.5) | 5409 | 3362 (62.2) | |||
| South | 19,642 | 3576 (18.2) | 11,214 | 6928 (61.8) | |||
| West | 10,653 | 1515 (14.2) | 5313 | 3387 (63.7) | |||
| <0.001 | <0.001 | ||||||
| Control/ownership of hospital | Government, nonfederal | 6394 | 1204 (18.8) | 3623 | 2212 (61.1) | ||
| Private, not-for-profit | 38,506 | 5989 (15.6) | 19,326 | 11,989 (62) | |||
| Private, investment ownership | 5472 | 876 (16) | 2452 | 1411 (57.5) | |||
| <0.001 | <0.001 | ||||||
| Deliveries/Year | Survival % during Hospital Stay (Excluding Who Babies Died on Day 0) | ||
|---|---|---|---|
| <24 Weeks | <500 gm | <24 Weeks and <500 g | |
| <2000 deliveries/year | 22.0% | 19.1% | 13.7% |
| 2000–4000 deliveries/year | 23.5% | 25.8% | 17.5% |
| 4000–6000 deliveries/year | 24.7% | 28% | 17.6% |
| 6000–8000 deliveries/year | 26.6% | 30.2% | 18.1% |
| >8000 deliveries/year | 26.9% | 30% | 22.4% |
| p-value | <0.001 | <0.03 | <0.001 |
| Died on Day 0 | Died on Day 1 | Died on Day 2 | |
|---|---|---|---|
| 2010 | 66.1% | 11.5% | 1.9% |
| 2011 | 67.0% | 10.6% | 1.8% |
| 2012 | 60.3% | 13.5% | 1.7% |
| 2013 | 64.1% | 13.1% | 1.6% |
| 2014 | 59.3% | 13.1% | 2.6% |
| 2015 | 56.5% | 12.6% | 2.3% |
| 2016 | 53.7% | 13.0% | 2.5% |
| 2017 | 53.7% | 13.3% | 2.9% |
| 2018 | 51.4% | 15.0% | 3.4% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qattea, I.; Quatei, A.; Farghaly, M.A.A.; Abdalla, A.; Mohamed, M.A.; Aly, H. Hospital Factors Associated with the Survival of Infants Born at Periviable Gestation: The USA National Database. Children 2024, 11, 133. https://0-doi-org.brum.beds.ac.uk/10.3390/children11010133
Qattea I, Quatei A, Farghaly MAA, Abdalla A, Mohamed MA, Aly H. Hospital Factors Associated with the Survival of Infants Born at Periviable Gestation: The USA National Database. Children. 2024; 11(1):133. https://0-doi-org.brum.beds.ac.uk/10.3390/children11010133
Chicago/Turabian StyleQattea, Ibrahim, Amani Quatei, Mohsen A. A. Farghaly, Alshimaa Abdalla, Mohamed A. Mohamed, and Hany Aly. 2024. "Hospital Factors Associated with the Survival of Infants Born at Periviable Gestation: The USA National Database" Children 11, no. 1: 133. https://0-doi-org.brum.beds.ac.uk/10.3390/children11010133