
Secondary Pulmonary Vein Stenosis Due to Total Anomalous Pulmonary Venous Connection Repair in Children: Extravascular MDCT Findings

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Institutional Review Board Approval
2.2. Study Cohort
2.3. Patient’s Clinical Information
2.4. Pulmonary Vein Stenosis Diagnostic Criteria
2.5. Thoracic MDCT Angiography Technique
2.5.1. MDCT Scanner Types
2.5.2. Thoracic MDCT Parameters
2.6. Thoracic MDCT Angiography Image Reconstruction and Review
2.6.1. Thoracic MDCT Angiography Image Reconstruction
2.6.2. Thoracic MDCT Angiography Image Review Preparation
2.6.3. Thoracic MDCT Angiography Image Review
2.7. Thoracic MDCT Angiography Image Assessment
2.7.1. Lung and Airway Evaluation
2.7.2. Pleural Evaluation
2.7.3. Mediastinal Evaluation
2.7.4. Main Pulmonary Artery to Ascending Aorta Ratio Evaluation
2.8. Statistical Analysis
3. Results
3.1. Study Cohort Characteristics
3.2. Thoracic MDCT Angiography Findings
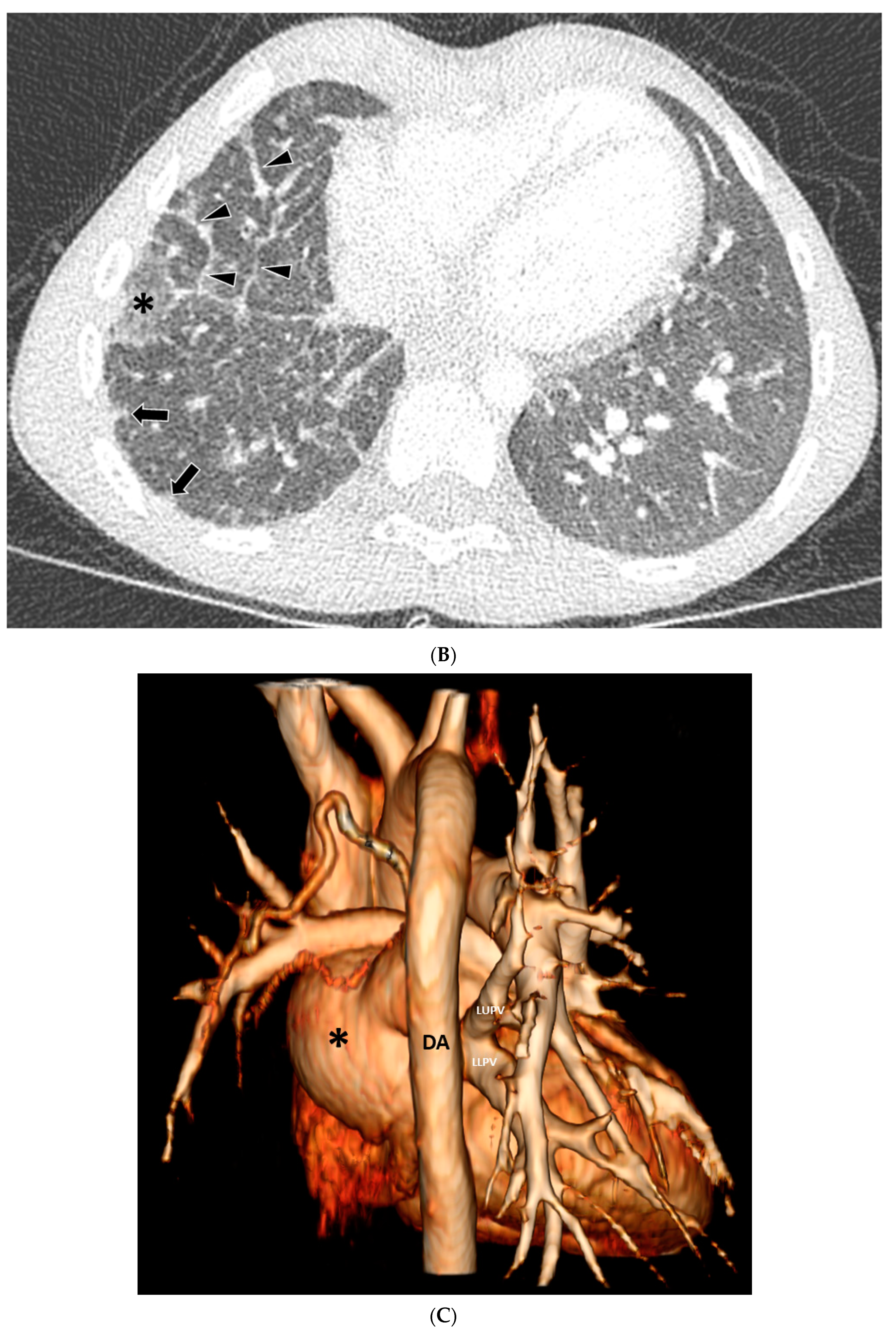
3.2.1. Lung and Airway Abnormalities
3.2.2. Pleural Abnormalities
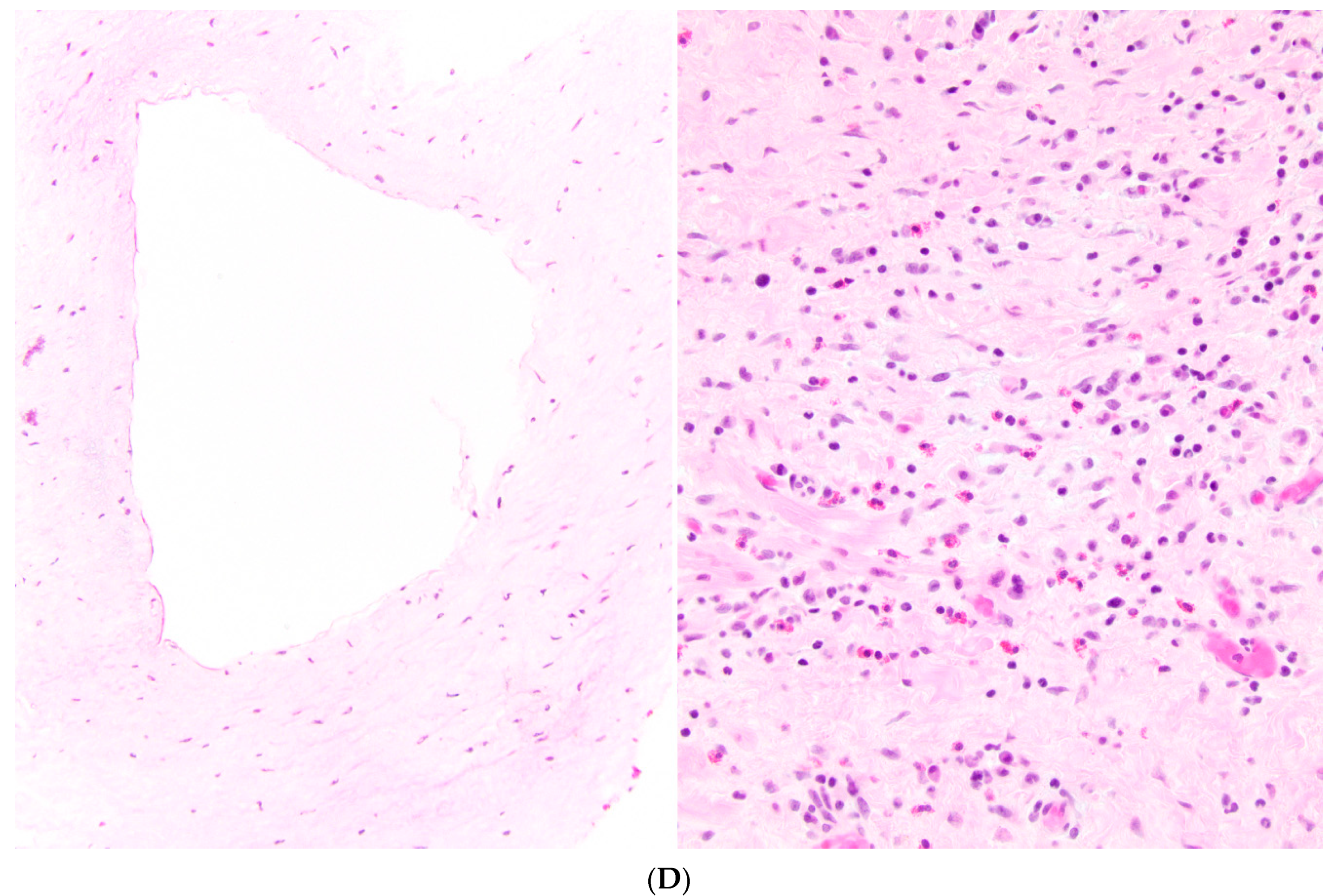
3.2.3. Mediastinal Abnormalities
3.2.4. Main Pulmonary Artery to Ascending Aorta Ratio
3.3. Interobserver Agreement
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Frank, D.B.; Levy, P.T.; Stiver, C.A.; Boe, B.A.; Baird, C.W.; Callahan, R.M. Primary pulmonary vein stenosis during infancy: State of the art review. J. Perinatol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Schramm, J.; Sivalingam, S.; Moreno, G.E.; Thanh, D.Q.L.; Gauvrea, K.; Doherty-Schmeck, K.; Jenkins, K.J. Pulmonary vein stenosis: A rare disease with a global reach. Children 2021, 8, 198. [Google Scholar] [CrossRef] [PubMed]
- Seale, A.N.; Uemura, H.; Webber, S.A.; Partridge, J.; Roughton, M.; Ho, S.Y. Total anomalous pulmonary venous connection: Outcome of postoperative pulmonary venous obstruction. J. Thorac. Cardiovasc. Surg. 2013, 145, 1255–1262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hancock Friesen, C.L.; Zurakowski, D.; Thiagarajan, R.R.; Forbess, J.M.; Pedro, J.; Mayer, J.E.; Jonas, R.A. Total anomalous pulmonary venous connection: An analysis of current management strategies in a single institution. Ann. Thorac. Surg. 2005, 79, 596–606. [Google Scholar] [CrossRef] [PubMed]
- Hyde, J.A.; Stumper, O.; Barth, M.J.; Wright, J.G.C.; Silove, E.D.; De Giovanni, J.V.; Sethia, B. Total anomalous pulmonary venous connection: Outcome of surgical correction and management of recurrent venous obstruction. Eur. J. Cardiothorac. Surg. 1999, 15, 735–740. [Google Scholar] [CrossRef] [Green Version]
- White, B.R.; Ho, D.Y.; Faerber, J.A.; Katcoff, H.; Glatz, A.C.; Mascio, C.E.; Stephens, P., Jr.; Cohen, M.S. Repair of total anomalous pulmonary venous connection: Risk factors for postoperative obstruction. Ann. Thorac. Surg. 2019, 108, 122–129. [Google Scholar] [CrossRef] [PubMed]
- DiLorenzo, M.P.; Santo, A.; Rome, J.J.; Zhang, H.; Vaerber, J.A.; Mercer-Rosa, L.; Hopper, R.K. Pulmonary vein stenosis: Outcomes in children with congenital heart disease and prematurity. Semin. Thorac. Cardovasc. Surg. 2019, 31, 266–273. [Google Scholar] [CrossRef]
- Suntharos, P.; Prieto, L.R. Treatment of congenital and acquired pulmonary vein stenosis. Curr. Cardiol. Rep. 2020, 22, 153. [Google Scholar] [CrossRef] [PubMed]
- Vanderlaan, R.D.; Rome, J.; Hirsch, R.; Ivy, D.; Caldarone, C.A. Pulmonary vein stenosis: Treatment and challenges. J. Thorac. Cardiovasc. Surg. 2012, 161, 2169–2176. [Google Scholar] [CrossRef] [PubMed]
- Hump, T.; Fineman, J.; Qureshi, A.M. The many faces and outcomes of pulmonary vein stenosis in early childhood. Pediatr. Pulmonol. 2021, 56, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Hart, A.; Lee, E.Y. Chapter 10: Pediatric Chest Disorders: Practical Imaging Approach to Diagnosis. In Diseases of the Chest, Breast, Heart and Vessels 2019–2022: Diagnostic and Interventional Imaging; Springer Publishing: New York, NY, USA, 2019. [Google Scholar]
- Lee, E.Y.; Jenkins, K.J.; Muneeb, M.; Marshall, A.C.; Tracy, D.A.; Zurakowski, D.; Boiselle, P.M. Proximal pulmonary vein stenosis detection in pediatric patients: Value of multiplanar and 3-D VR imaging evaluation. Pediatr. Radiol. 2013, 43, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Barrera, C.A.; Saul, D.; Rapp, J.B.; Smith, C.L.; White, A.M.; Biko, D.M.; Otero, H.J. Diagnostic performance of CT angiography to detect pulmonary vein stenosis in children. Int. J. Cardiovasc. Imaging 2020, 36, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.Y.; Jenkins, K.J.; Vargas, S.O.; Callahan, R.; Park, H.J.; Gauthier, Z.; Winant, A.J. Thoracic multidetector computed tomography angiography of primary pulmonary vein stenosis in children: Evaluation of characteristic extravascular findings. J. Thorac. Imaging 2021. [Google Scholar] [CrossRef] [PubMed]
- Balasubramanian, S.; Rehman, M.; Gauvreau, K.; Jenkins, K.J. Bilateral disease and early age at presentation are associated with shorter survival in patients with congenital heart disease and intraluminal pulmonary vein stenosis. Congenit Heart Dis. 2012, 7, 378–386. [Google Scholar] [CrossRef] [PubMed]
- Hansell, D.M.; Bankier, A.A.; MacMahon, H.; McLoud, T.C.; Müller, N.L.; Remy, J. Fleischner Society: Glossary of terms for thoracic imaging. Radiology 2008, 3, 697–722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, E.Y.; Khatwa, U.; McAdam, A.J.; Bastos, M.d.; Mahmood, S.A.; Ervoes, J.P.; Boiselle, P.M. Streptococcus milleri group pleuropulmonary infection in children: Computed tomography findings and clinical features. J. Comput. Assist. Tomogr. 2010, 43, 927–932. [Google Scholar] [CrossRef] [PubMed]
- SAS Institute Inc. SAS/STAT 141 User Guide; SAS Institute Inc.: Gary, India, 2015. [Google Scholar]
- Ngo, A.V.; Winant, A.J.; Lee, E.Y.; Phillips, G.S. Strategies for reducing radiation dose in CT for pediatric patients: How we do it. Semin. Roentgenol. 2018, 53, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Sodhi, K.S.; Krishna, S.; Saxena, A.K.; Sinha, A.; Khandelwal, N.; Lee, E.Y. Clinical application of ‘justification’ and ‘optimization’ principle of ALARA in pediatric CT imaging: “how many children can be protected from unnecessary radiation?”. Eur. J. Radiol. 2015, 84, 1752–1757. [Google Scholar] [CrossRef] [PubMed]
- MacDougall, R.D.; Strauss, K.J.; Lee, E.Y. Managing radiation dose from thoracic multidetector computed tomography in pediatric patients: Background, current issues, and recommendations. Radiol. Clin. N. Am. 2013, 51, 743–760. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Types of Extravascular Thoracic MDCT Angiography Findings | Number (Percentage) of Abnormalities (n = 20) |
|---|---|
| Lung Findings | |
| GGO | 19/20 (95%) |
| Septal Thickening | 7/20 (35%) |
| Nodule | 0/0 (0%) |
| Mass | 0/0 (0%) |
| Cyst | 0/0 (0%) |
| Fibrosis | 0/0 (0%) |
| Bronchiectasis | 0/0 (0%) |
| Pleural Findings | |
| Pleural Thickening | 17/20 (85%) |
| Pleural Effusion | 0/0 (0%) |
| Pneumothorax | 0/0 (0%) |
| Mediastinal Findings | |
| Mediastinal Mass | 17/20 (85%) |
| Mediastinal Lymphadenopathy | 0/0 (0%) |
| Main Pulmonary Artery Size (mm) | Aorta Size (mm) | P/A Ratio |
|---|---|---|
| 10.56 | 9.55 | 1.1 |
| 19.09 | 13.42 | 1.42 |
| 18.44 | 13.72 | 1.34 |
| 14.25 | 12.53 | 1.14 |
| 10.30 | 8.47 | 1.22 |
| 11.51 | 9.25 | 1.24 |
| 16.00 | 10.97 | 1.46 |
| 15.96 | 10.4 | 1.53 |
| 14.35 | 10.62 | 1.35 |
| 13.81 | 7.84 | 1.76 |
| 10.03 | 5.42 | 1.85 |
| 19.99 | 11.62 | 1.72 |
| 21.22 | 16.20 | 1.31 |
| 10.91 | 4.97 | 2.19 |
| 9.70 | 4.48 | 2.17 |
| 16.13 | 12.42 | 1.30 |
| 10.98 | 9.51 | 1.15 |
| 10.03 | 8.14 | 1.23 |
| 17.43 | 12.69 | 1.37 |
| 16.11 | 14.18 | 1.14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, E.Y.; Vargas, S.O.; Jenkins, K.J.; Callahan, R.; Park, H.J.; Gauthier, Z.; Winant, A.J. Secondary Pulmonary Vein Stenosis Due to Total Anomalous Pulmonary Venous Connection Repair in Children: Extravascular MDCT Findings. Children 2021, 8, 726. https://0-doi-org.brum.beds.ac.uk/10.3390/children8090726
Lee EY, Vargas SO, Jenkins KJ, Callahan R, Park HJ, Gauthier Z, Winant AJ. Secondary Pulmonary Vein Stenosis Due to Total Anomalous Pulmonary Venous Connection Repair in Children: Extravascular MDCT Findings. Children. 2021; 8(9):726. https://0-doi-org.brum.beds.ac.uk/10.3390/children8090726
Chicago/Turabian StyleLee, Edward Y., Sara O. Vargas, Kathy J. Jenkins, Ryan Callahan, Halley J. Park, Zachary Gauthier, and Abbey J. Winant. 2021. "Secondary Pulmonary Vein Stenosis Due to Total Anomalous Pulmonary Venous Connection Repair in Children: Extravascular MDCT Findings" Children 8, no. 9: 726. https://0-doi-org.brum.beds.ac.uk/10.3390/children8090726