
Effect of Centralization on Surgical Outcome of Children Operated for Liver Tumors in Switzerland: A Retrospective Comparative Study

 , , ,
, , ,
Abstract
:1. Introduction
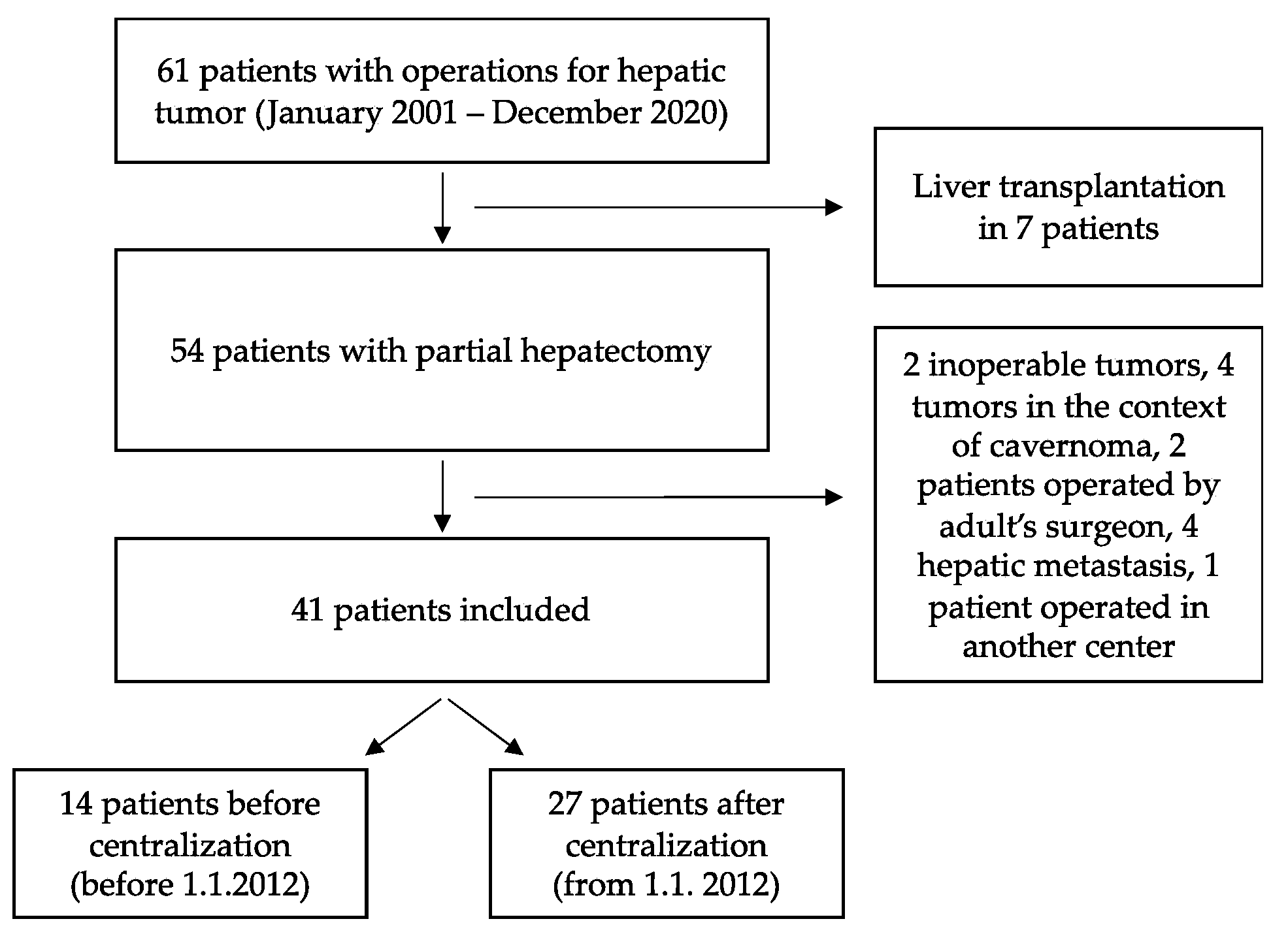
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Darbari, A.; Sabin, K.; Shapiro, C.N.; Schwarz, K.B. Epidemiology of primary hepatic malignancies in U.S. children. Hepatology 2003, 38, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Finegold, M.J.; Egler, R.A.; Goss, J.A.; Guillerman, R.P.; Karpen, S.J.; Krishnamurthy, R.; O’Mahony, C.A. Liver tumors: Pediatric population. Liver Transplant. 2008, 14, 1545–1556. [Google Scholar] [CrossRef]
- Ng, K.; Mogul, D.B. Pediatric Liver Tumors. Clin. Liver Dis. 2018, 22, 753–772. [Google Scholar] [CrossRef] [PubMed]
- Isaacs, H. Fetal and neonatal hepatic tumors. J. Pediatr. Surg. 2007, 42, 1797–1803. [Google Scholar] [CrossRef]
- Roebuck, D.J. Assessment of malignant liver tumors in children. Cancer Imaging 2009, 9, S98–S103. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, J.; Hoffmann, K.; Murtha-Lemekhova, A.; Kessler, M.; Günther, P.; Frongia, G.; Probst, P.; Mehrabi, A. Establishing a Standardized Measure of Quality in Pediatric Liver Surgery: Definition and Validation of Textbook Outcome with Associated Predictors. Front. Surg. 2021, 8, 708351. [Google Scholar] [CrossRef]
- Vonlanthen, R.; Lodge, P.; Barkun, J.S.; Farges, O.; Rogiers, X.; Soreide, K.; Kehlet, H.; Reynolds, J.V.; Käser, S.A.; Naredi, P.; et al. Toward a Consensus on Centralization in Surgery. Ann. Surg. 2018, 268, 712–724. [Google Scholar] [CrossRef] [Green Version]
- Lampela, H.; Ritvanen, A.; Kosola, S.; Koivusalo, A.; Rintala, R.; Jalanko, H.; Pakarinen, M. National centralization of biliary atresia care to an assigned multidisciplinary team provides high-quality outcomes. Scand. J. Gastroenterol. 2011, 47, 99–107. [Google Scholar] [CrossRef]
- Davenport, M.; Ong, E.; Sharif, K.; Alizai, N.; McClean, P.; Hadzic, N.; Kelly, D.A. Biliary atresia in England and Wales: Results of centralization and new benchmark. J. Pediatr. Surg. 2011, 46, 1689–1694. [Google Scholar] [CrossRef]
- Polonski, A.; Izbicki, J.R.; Uzunoglu, F.G. Centralization of Pancreatic Surgery in Europe. J. Gastrointest. Surg. 2019, 23, 2081–2092. [Google Scholar] [CrossRef]
- Wildhaber, B.E.; Majno, P.; Mayr, J.; Zachariou, Z.; Hohlfeld, J.; Schwoebel, M.; Kistler, W.; Meuli, M.; Le Coultre, C.; Mentha, G.; et al. Biliary Atresia: Swiss National Study, 1994–2004. J. Pediatr. Gastroenterol. Nutr. 2008, 46, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Meyers, R.L. Tumors of the liver in children. Surg. Oncol. 2007, 16, 195–203. [Google Scholar] [CrossRef]
- Hartley, A.L.; Birch, J.M.; Kelsey, A.M.; Jones, P.H.M.; Harris, M.; Blair, V. Epidemiological and familial aspects of hepatoblastoma. Med Pediatr. Oncol. 1990, 18, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Wijnen, M.H.; Hulscher, J.B. Centralization of pediatric surgical care in the Netherlands: Lessons learned. J. Pediatr. Surg. 2021, 57, 178–181. [Google Scholar] [CrossRef] [PubMed]
- Durkin, N.; Davenport, M. Centralization of Pediatric Surgical Procedures in the United Kingdom. Eur. J. Pediatr. Surg. 2017, 27, 416–421. [Google Scholar] [CrossRef] [PubMed]
- Wijnen, M.H. Centralization of Pediatric Surgery in The Netherlands. Eur. J. Pediatr. Surg. 2017, 27, 407–409. [Google Scholar] [CrossRef] [PubMed]
- Pintér, A.; Vajda, P. Centralization of Pediatric Surgery in Hungary. Eur. J. Pediatr. Surg. 2017, 27, 429–430. [Google Scholar] [CrossRef]
- Lundström, N.; Berggren, H.; Björkhem, G.; Jögi, P.; Sunnegårdh, J. Centralization of Pediatric Heart Surgery in Sweden. Pediatr. Cardiol. 2000, 21, 353–357. [Google Scholar] [CrossRef]
- Roy, P.; van Peer, S.E.; de Witte, M.M.; Tytgat, G.A.M.; Karim-Kos, H.E.; van Grotel, M.; van de Ven, C.P.; Mavinkurve-Groothuis, A.M.C.; Merks, J.H.M.; Kuiper, R.P.; et al. Characteristics and outcome of children with renal tumors in the Netherlands: The first five-year’s experience of national centralization. PLoS ONE 2022, 17, e0261729. [Google Scholar] [CrossRef]
- Sheetz, K.H.; Dimick, J.B.; Nathan, H. Centralization of High-Risk Cancer Surgery Within Existing Hospital Systems. J. Clin. Oncol. 2019, 37, 3234–3242. [Google Scholar] [CrossRef]
- Siemens, D.R.; Visram, K.; Wei, X.; Booth, C. Effect of centralization on complex surgical care: A population-based case study of radical cystectomy. Can. Urol. Assoc. J. 2019, 14, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Ratnayake, B.; Pendharkar, S.A.; Connor, S.; Koea, J.; Sarfati, D.; Dennett, E.; Pandanaboyana, S.; Windsor, J.A. Patient volume and clinical outcome after pancreatic cancer resection: A contemporary systematic review and meta-analysis. Surgery 2022. [Google Scholar] [CrossRef] [PubMed]
- Tol, J.A.M.G.; Van Gulik, T.M.; Busch, O.R.C.; Gouma, D.J. Centralization of Highly Complex Low-Volume Procedures in Upper Gastrointestinal Surgery. A Summary of Systematic Reviews and Meta-Analyses. Dig. Surg. 2012, 29, 374–383. [Google Scholar] [CrossRef] [PubMed]
- Van Gijn, W.; Gooiker, G.; Wouters, M.; Post, P.; Tollenaar, R.; van de Velde, C. Volume and outcome in colorectal cancer surgery. Eur. J. Surg. Oncol. 2010, 36, S55–S63. [Google Scholar] [CrossRef] [Green Version]
- Archampong, D.; Borowski, D.; Wille-Jørgensen, P.; Iversen, L.H. Workload and surgeon´s specialty for outcome after colorectal cancer surgery. Cochrane Database Syst. Rev. 2012, 2012, CD005391. [Google Scholar] [CrossRef] [PubMed]
- Bradshaw, B.G.; Liu, S.S.; Thirlby, R.C. Standardized Perioperative Care Protocols and Reduced Length of Stay After Colon Surgery. J. Am. Coll. Surg. 1998, 186, 501–506. [Google Scholar] [CrossRef]
- Clark, C.J.; Ali, S.M.; Zaydfudim, V.; Jacob, A.K.; Nagorney, D.M. Safety of an Enhanced Recovery Pathway for Patients Undergoing Open Hepatic Resection. PLoS ONE 2016, 11, e0150782. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Total Cohort (n = 41) | Before Centralisation (n = 14) | After Centralisation (n = 27) | p-Value | ||
|---|---|---|---|---|---|
| Gender, n (%) | Male | 24 (59) | 7 (50) | 17 (63) | 0.51 |
| Female | 17 (41) | 7 (50) | 10 (37) | ||
| Age at diagnosis (months), median (IQR) | 24 m (9–77 m) | 21 m (7–132 m) | 24 m (10–54 m) | 0.13 | |
| Weight at surgery, median (IQR) | 12 kg (9–20 kg) | 13 kg (9–30 kg) | 12 kg (9–17 kg) | 0.20 | |
| Birth data | n = 22 | n = 7 | n = 15 | 0.63 | |
| Term born (38–42 SA), n (%) | 15 (68) | 4 (57) | 11 (73) | ||
| Pre term (< 38 SA), n (%) | 6 (27) | 3 (43) | 3 (20) | ||
| Late term (> 42 SA), n (%) | 1 (5) | 0 (0) | 1 (7) | ||
| Birth weight, median (IQR) | 2840 g (2509–3473 g) | 2645 g (2635–2898 g) | 2840 g (2145–3473 g) | 0.99 | |
| Comorbidity * | Yes, n (%) | 9 (22) | 4 (29) | 5 (19) | 0.69 |
| No, n (%) | 32 (78) | 10 (71) | 22 (81) | ||
| Biopsy before surgery | Yes, n (%) | 38 (93) | 11 (79) | 27 (100) | 0.03 |
| No, n (%) | 3 (7) | 3 (21) | 0 (0) | ||
| Tumor characteristics | 0.71 | ||||
| Benign disease, n (%) | 10 (24) | 4 (29) | 6 (22) | ||
| Mesenchymal hamartoma | 4 | 2 | 2 | ||
| Focal nodular hyperplasia | 3 | 2 | 1 | ||
| Lipoblastoma | 1 | 0 | 1 | ||
| Hemangioma | 1 | 0 | 1 | ||
| Adenoma | 1 | 0 | 1 | ||
| Malignant disease, n (%) | 31 (76) | 10 (71) | 21 (78) | ||
| Hepatoblastoma | 27 (87) | 7 (70) | 20 (95) | ||
| Embryonal sarcoma | 4 (23) | 3 (30) | 1 (5) | ||
| Rupture (R) and/or metastases | n = 31 | n = 10 | n = 21 | ||
| (M) at diagnosis | |||||
| R– M–, n (%) | 19 (61) | 6 (60) | 13 (62) | ||
| R+ M–, n (%) | 7 (23) | 1 (10) | 6 (28) | ||
| R– M+, n (%) | 4 (13) | 2 (20) | 2 (10) | ||
| R+M+, n (%) | 1 (3) | 1 (10) | 0 (0) | ||
| Before Centralization (n = 14) | After Centralization (n = 27) | p-Value | ||
|---|---|---|---|---|
| Cycles neoadjuvant chemotherapy | n = 10 | n = 21 | ||
| Median (IQR) | 2 (0–4) | 4 (3–4) | 0.76 | |
| GCSF administration before surgery, n (%) | 1 (7) | 3 (11) | 1.00 | |
| Embolization before surgery, n (%) | 2 (14) | 2 (7) | 0.60 | |
| Prior abdominal surgery before hepatic surgery, n (%) | 1 (7) | 1 (4) | 1.00 | |
| Type of resection, n (%) | ||||
| Right lobectomy | 3 (21) | 7 (26) | 1.00 | |
| Left lobectomy | 2 (14) | 6 (22) | 0.69 | |
| Extended right lobectomy | 3 (21) | 3 (11) | 0.39 | |
| Left lateral segmentectomy | 2 (14) | 5 (19) | 1.00 | |
| Extended left lobectomy | 2 (14) | 1 (4) | 0.26 | |
| Segmentectomy | 1 (7) | 3 (11) | 1.00 | |
| Atypical resection | 1 (7) | 2 (7) | 1.00 | |
| Surgical margins, n (%) | Negative | 14 (100) | 27 (100) | 1.00 |
| Positive | 0 (0) | 0 (0) | ||
| Operative time in minutes, median (IQR) | 366 (302–496) | 270 (219–335) | 0.17 | |
| Vascular exclusion | Number, n (%) | 4 (29) | 0 (0) | 0.01 |
| Minutes, median (IQR) | 71 (55–81) | - (-) | ||
| Days of postoperative stay, median (IQR) | 7.0 (7.0–10.0) | 8.0 (7.0–9.5) | 0.37 | |
| Post-operative’s cycles chemotherapy, median (IQR) | n = 10 | n = 21 | ||
| 2 (1–3) | 2 (2–2) | 0.29 | ||
| Surgical complications, n (%) | 8 (57) | 4 (15) | 0.01 | |
| Duration of follow-up in months, median (IQR) | 5 (1–23) | 47 (12–60) | 0.15 | |
| 30-day mortality, n (%) | 0 (0) | 0 (0) | ||
| Before Centralization (n = 14) | After Centralization (n = 27) | p-Value | |
|---|---|---|---|
| All complications, n (%) | 8 (57) | 4 (15) | 0.01 |
| Complications Clavien III and higher, n (%) | 7 (50) | 2 (7) | <0.00 |
| Early (<1 month), n (%) | 4 (50) | 3 (75) | 0.21 |
| Respiratory, n (Clavien classification) | 2 (IIIb) | 2 (I) | |
| Infectious, n (Clavien classification) | 1 (II) | 0 (-) | |
| Biliary, n (Clavien classification) | 1 (IIIb) | 0 (-) | |
| Intestinal, n (Clavien classification) | 0 (-) | 1 (IIIb) | |
| Late (>1 month), n (%) | 4 (50) | 1 (25) | 0.04 |
| Surgical complications | 0 | 0 | |
| Malignant tumors | n = 10 | n = 21 | 0.03 |
| Hepatic relapses, n (%) | 4 (40) | 1 (5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leoni, J.; Rougemont, A.-L.; Calinescu, A.M.; Ansari, M.; Compagnon, P.; Wilde, J.C.H.; Wildhaber, B.E. Effect of Centralization on Surgical Outcome of Children Operated for Liver Tumors in Switzerland: A Retrospective Comparative Study. Children 2022, 9, 217. https://0-doi-org.brum.beds.ac.uk/10.3390/children9020217
Leoni J, Rougemont A-L, Calinescu AM, Ansari M, Compagnon P, Wilde JCH, Wildhaber BE. Effect of Centralization on Surgical Outcome of Children Operated for Liver Tumors in Switzerland: A Retrospective Comparative Study. Children. 2022; 9(2):217. https://0-doi-org.brum.beds.ac.uk/10.3390/children9020217
Chicago/Turabian StyleLeoni, Jasmine, Anne-Laure Rougemont, Ana M. Calinescu, Marc Ansari, Philippe Compagnon, Jim C. H. Wilde, and Barbara E. Wildhaber. 2022. "Effect of Centralization on Surgical Outcome of Children Operated for Liver Tumors in Switzerland: A Retrospective Comparative Study" Children 9, no. 2: 217. https://0-doi-org.brum.beds.ac.uk/10.3390/children9020217