
Ultrasonographic Assessment for Tenosynovitis in Juvenile Idiopathic Arthritis with Ankle Involvement: Diagnostic and Therapeutic Significance

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Clinical and Laboratory Assessment
2.3. Sonographic Examination
3. Results
3.1. Clinical Results
3.2. Sonographic Results
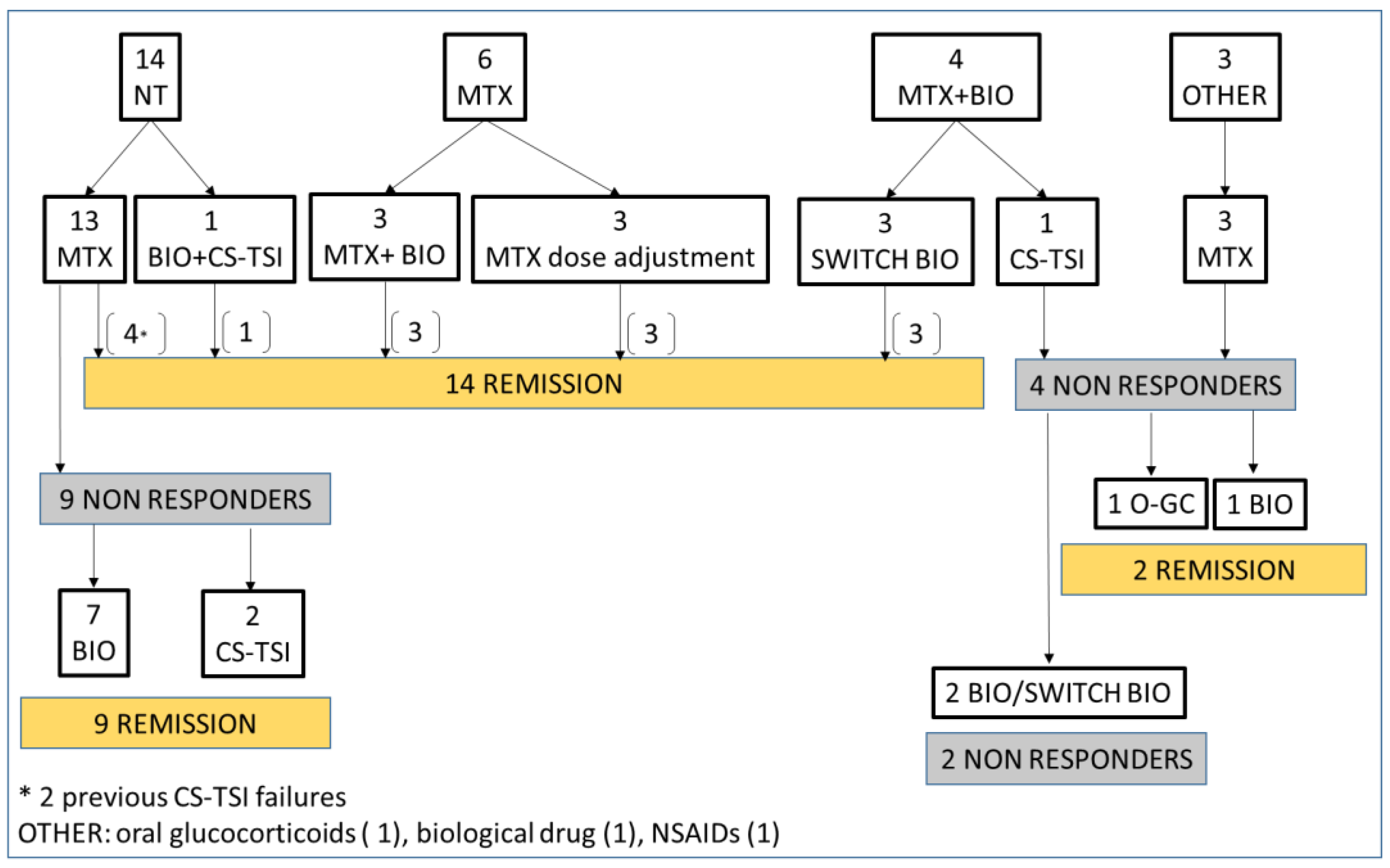
3.3. Treatment of Patients with Tenosynovitis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peters, S.E.; Laxer, R.M.; Connolly, B.L.; Parra, D.A. Ultrasound-guided steroid tendon sheath injections in juvenile idiopathic arthritis: A 10-year single-center retrospective study. Pediatric Rheumatol. Online J. 2017, 15, 22. [Google Scholar] [CrossRef] [PubMed]
- Lanni, S.; Bovis, F.; Ravelli, A.; Viola, S.; Magnaguagno, F.; Pistorio, A.; Magnano, G.M.; Martini, A.; Malattia, C. Delineating the Application of Ultrasound in Detecting Synovial Abnormalities of the Subtalar Joint in Juvenile Idiopathic Arthritis. Arthritis Care Res. 2016, 68, 1346–1353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cimaz, R.; Giani, T.; Caporali, R. What is the real role of ultrasound in the management of juvenile idiopathic arthritis? Ann. Rheum. Dis. 2020, 79, 437–439. [Google Scholar] [CrossRef] [PubMed]
- Lanni, S.; Marafon, D.P.; Civino, A.; Alongi, A.; Proverbio, E.; Agostoni, C.; Ravelli, A.; Filocamo, G. Comparison Between Clinical and Ultrasound Assessment of the Ankle Region in Children With Juvenile Idiopathic Arthritis. Arthritis Care Res. 2021, 73, 1180–1186. [Google Scholar] [CrossRef] [PubMed]
- Laurell, L.; Court-Payen, M.; Nielsen, S.; Zak, M.; Boesen, M.; Fasth, A. Ultrasonography and color Doppler in juvenile idiopathic arthritis: Diagnosis and follow-up of ultrasound-guided steroid injection in the ankle region. A descriptive interventional study. Pediatric Rheumatol. Online J. 2011, 9, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pastore, S.; Paolera, S.; Zabotti, A.; Tommasini, A.; Taddio, A. ANKLE ARTHRITIS IN JUVENILE IDIOPATHIC ARTHRITIS: DON’T MISS TENOSYNOVITIS. CLINICAL AND SONOGRAPHIC FEATURES OF ANKLE TENOSYNOVITIS IN JIA. Ann. Rheum. Dis. 2021, 80, 948.3–949. [Google Scholar] [CrossRef]
- Trincianti, C.; Van Dijkhuizen, E.H.P.; Alongi, A.; Mazzoni, M.; Swart, J.F.; Nikishina, I.; Lahdenne, P.; Rutkowska-Sak, L.; Avcin, T.; Quartier, P.; et al. Definition and Validation of the American College of Rheumatology 2021 Juvenile Arthritis Disease Activity Score Cutoffs for Disease Activity States in Juvenile Idiopathic Arthritis. Arthritis Rheumatol. 2021, 73, 1966–1975. [Google Scholar] [CrossRef] [PubMed]
- Wakefield, R.J.; Balint, P.V.; Szkudlarek, M.; Filippucci, E.; Backhaus, M.; D’Agostino, M.-A.; Sanchez, E.N.; Iagnocco, A.; Schmidt, W.A.; Bruyn, G.A.W.; et al. Musculoskeletal ultrasound including definitions for ultrasonographic pathology. J. Rheumatol. 2005, 32, 2485–2487. [Google Scholar] [PubMed]
- Backhaus, M.; Burmester, G.R.; Gerber, T.; Grassi, W.; Machold, K.P.; Swen, W.A.; Wakefield, R.J.; Manger, B. Guidelines for musculoskeletal ultrasound in rheumatology. Ann. Rheum. Dis. 2001, 60, 641–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naredo, E.; D’Agostino, M.A.; Wakefield, R.J.; Möller, I.; Balint, P.V.; Filippucci, E.; Iagnocco, A.; Karim, Z.; Terslev, L.; Bong, D.A.; et al. Reliability of a consensus-based ultrasound score for tenosynovitis in rheumatoid arthritis. Ann. Rheum. Dis. 2013, 72, 1328–1334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hendry, G.J.; Gardner-Medwin, J.; Steultjens, M.P.; Woodburn, J.; Sturrock, R.D.; Turner, D.E. Frequent discordance between clinical and musculoskeletal ultrasound examinations of foot disease in juvenile idiopathic arthritis. Arthritis Care Res. 2012, 64, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Pascoli, L.; Wright, S.; McAllister, C.; Rooney, M. Prospective evaluation of clinical and ultrasound findings in ankle disease in juvenile idiopathic arthritis: Importance of ankle ultrasound. J. Rheumatol. 2010, 37, 2409–2414. [Google Scholar] [CrossRef] [PubMed]
- Magni-Manzoni, S. Ultrasound in juvenile idiopathic arthritis. Pediatric Rheumatol. Online J. 2016, 14, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magni-Manzoni, S.; Malattia, C.; Lanni, S.; Ravelli, A. Advances and challenges in imaging in juvenile idiopathic arthritis. Nat. Rev. Rheumatol. 2012, 8, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Ammitzbøll-Danielsen, M.; Østergaard, M.; Fana, V.; Glinatsi, D.; Døhn, U.M.; Ørnbjerg, L.M.; Naredo, E.; Terslev, L. Intramuscular versus ultrasound-guided intratenosynovial glucocorticoid injection for tenosynovitis in patients with rheumatoid arthritis: A randomised, double-blind, controlled study. Ann. Rheum. Dis. 2017, 76, 666–672. [Google Scholar] [CrossRef] [PubMed]
- Di Geso, L.; Filippucci, E.; Meenagh, G.; Gutierrez, M.; Ciapetti, A.; Salaffi, F.; Grassi, W. CS injection of tenosynovitis in patients with chronic inflammatory arthritis: The role of US. Rheumatology 2012, 51, 1299–1303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoll, M.L.; Mellins, E.D. Psoriatic arthritis in childhood: A commentary on the controversy. Clin. Immunol. 2020, 214, 108396. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Tendon | Ankles No. (n = 54) | Ankles % (n = 54) | Patients No. (n = 27) | Patients % (n = 27) |
|---|---|---|---|---|
| Tibialis Posterior | 21 | 38 | 18 | 66 |
| Peroneus Longus and Brevis | 3 | 0.5 | 3 | 11 |
| Flexor Digitorum Longus | 10 | 18 | 9 | 33 |
| Flexor Hallucis Longus | 5 | 0.9 | 5 | 18 |
| Extensor Digitorum Longus | 6 | 1.1 | 6 | 22 |
| Extensor Hallucis Longus | 4 | 0.7 | 4 | 14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Della Paolera, S.; Pastore, S.; Zabotti, A.; Tommasini, A.; Taddio, A. Ultrasonographic Assessment for Tenosynovitis in Juvenile Idiopathic Arthritis with Ankle Involvement: Diagnostic and Therapeutic Significance. Children 2022, 9, 509. https://0-doi-org.brum.beds.ac.uk/10.3390/children9040509
Della Paolera S, Pastore S, Zabotti A, Tommasini A, Taddio A. Ultrasonographic Assessment for Tenosynovitis in Juvenile Idiopathic Arthritis with Ankle Involvement: Diagnostic and Therapeutic Significance. Children. 2022; 9(4):509. https://0-doi-org.brum.beds.ac.uk/10.3390/children9040509
Chicago/Turabian StyleDella Paolera, Sara, Serena Pastore, Alen Zabotti, Alberto Tommasini, and Andrea Taddio. 2022. "Ultrasonographic Assessment for Tenosynovitis in Juvenile Idiopathic Arthritis with Ankle Involvement: Diagnostic and Therapeutic Significance" Children 9, no. 4: 509. https://0-doi-org.brum.beds.ac.uk/10.3390/children9040509