
Impact of Differing Language Background Exposures on Bayley-III Language Assessment in a National Cohort of Children Born Less than 29 Weeks’ Gestation

 , , and
, , and
Abstract
:1. Introduction
2. Methods
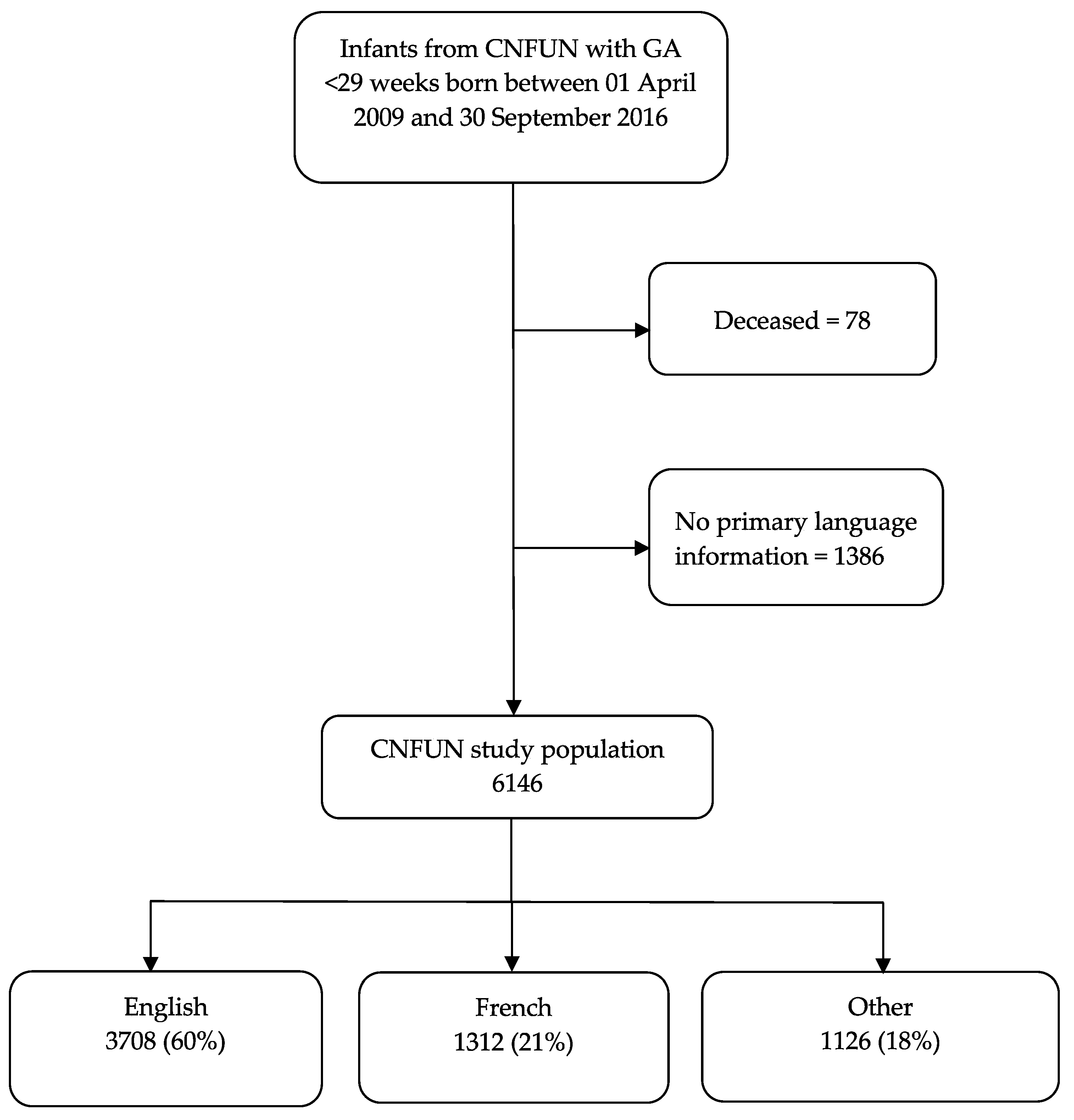
2.1. Participants
2.2. Materials
2.3. Procedures
2.4. Data Analyses
3. Results
3.1. Sociodemographic and Language Group Characteristics
3.2. Neurodevelopmental Outcomes by Language Groups
3.3. Bayley-III Administration Characteristics
3.4. Univariate Analyses
3.5. Multivariate Analyses
4. Discussion
4.1. Bayley-III Language Composite Scores and Primary Language at Home
4.2. Language of Administration of the Bayley-III
4.3. Multilingualism and Impact on Language Development
4.4. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vohr, B. Speech and Language Outcomes of Very Preterm Infants. Semin. Fetal Neonatal Med. 2013, 19, 78–83. [Google Scholar] [CrossRef] [PubMed]
- van Noort-van der Spek, I.L.; Franken, M.-C.J.P.; Weisglas-Kuperus, N. Language Functions in Preterm-Born Children: A Systematic Review and Meta-Analysis. Pediatrics 2012, 129, 745–754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barre, N.; Morgan, A.; Doyle, L.W.; Anderson, P.J. Language Abilities in Children Who Were Very Preterm and/or Very Low Birth Weight: A Meta-Analysis. J. Pediatr. 2011, 158, 766–774.e1. [Google Scholar] [CrossRef] [PubMed]
- Synnes, A.; Luu, T.M.; Moddemann, D.; Church, P.; Lee, D.; Vincer, M.; Ballantyne, M.; Majnemer, A.; Creighton, D.; Yang, J.; et al. Determinants of Developmental Outcomes in a Very Preterm Canadian Cohort. Arch. Dis. Child.-Fetal Neonatal Ed. 2017, 102, F234–F235. [Google Scholar] [CrossRef] [PubMed]
- Eadie, P.; Bavin, E.L.; Bretherton, L.; Cook, F.; Gold, L.; Mensah, F.; Wake, M.; Reilly, S. Predictors in Infancy for Language and Academic Outcomes at 11 Years. Pediatrics 2021, 147, e20201712. [Google Scholar] [CrossRef]
- Johnson, C.J.; Beitchman, J.H.; Brownlie, E.B. Twenty-Year Follow-Up of Children with and Without Speech-Language Impairments: Family, Educational, Occupational, and Quality of Life Outcomes. Am. J. Speech-Lang. Pat. 2010, 19, 51–65. [Google Scholar] [CrossRef] [Green Version]
- Conti-Ramsden, G.; Durkin, K. Postschool Educational and Employment Experiences of Young People with Specific Language Impairment. Lang. Speech Hear Serv. Sch. 2012, 43, 507–520. [Google Scholar] [CrossRef]
- Schoon, I.; Parsons, S.; Rush, R.; Law, J. Children’s Language Ability and Psychosocial Development: A 29-Year Follow-up Study. Pediatrics 2010, 126, e73–e80. [Google Scholar] [CrossRef] [Green Version]
- Gianní, M.L.; Picciolini, O.; Ravasi, M.; Gardon, L.; Vegni, C.; Fumagalli, M.; Mosca, F. The Effects of an Early Developmental Mother–Child Intervention Program on Neurodevelopment Outcome in Very Low Birth Weight Infants: A Pilot Study. Early Hum. Dev. 2006, 82, 691–695. [Google Scholar] [CrossRef]
- Meijssen, D.; Wolf, M.-J.; Koldewijn, K.; Houtzager, B.A.; van Wassenaer, A.; Tronick, E.; Kok, J.; van Baar, A. The Effect of the Infant Behavioral Assessment and Intervention Program on Mother-Infant Interaction after Very Preterm Birth: Effect of an Early Intervention on Mother-Infant Interaction after Very Preterm Birth. J. Child Psychol. Psyc. 2010, 51, 1287–1295. [Google Scholar] [CrossRef]
- Nordhov, S.M.; Rønning, J.A.; Ulvund, S.E.; Dahl, L.B.; Kaaresen, P.I. Early Intervention Improves Behavioral Outcomes for Preterm Infants: Randomized Controlled Trial. Pediatrics 2011, 129, e9–e16. [Google Scholar] [CrossRef] [PubMed]
- Ravn, I.H.; Smith, L.; Lindemann, R.; Smeby, N.A.; Kyno, N.M.; Bunch, E.H.; Sandvik, L. Effect of Early Intervention on Social Interaction between Mothers and Preterm Infants at 12 Months of Age: A Randomized Controlled Trial. Infant. Behav. Dev. 2011, 34, 215–225. [Google Scholar] [CrossRef] [PubMed]
- Vohr, B.; Wright, L.L. Follow-up Care of High-Risk Infants. Pediatrics 2011, 114, 1377–1397. [Google Scholar] [CrossRef] [Green Version]
- Bayley, N. Manual for the Bayley Scales of Infant and Toddler Development, 3rd ed.; The Psychological Corporation: San Antonio, TX, USA, 2006; ISBN 0158027833. [Google Scholar]
- Kinsella-Ritter, A.; Gibson, F.L.; Wyver, S. The Clinical Use of the Bayley Scales of Infant and Toddler Development, Third Edition (Bayley-III) in Australia. Aust. Educ. Dev. Psychol. 2009, 26, 154–164. [Google Scholar] [CrossRef]
- McHenry, M.S.; Oyungu, E.; Yang, Z.; Hines, A.C.; Ombitsa, A.R.; Vreeman, R.C.; Abubakar, A.; Monahan, P.O. Cultural Adaptation of the Bayley Scales of Infant and Toddler Development, 3rd Edition for Use in Kenyan Children Aged 18–36 Months: A Psychometric Study. Res. Dev. Disabil 2021, 110, 103837. [Google Scholar] [CrossRef]
- Lowe, J.R.; Nolen, T.L.; Vohr, B.; Adams-Chapman, I.; Duncan, A.F.; Watterberg, K. Effect of Primary Language on Developmental Testing in Children Born Extremely Preterm. Acta Paediatr. 2013, 102, 896–900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams-Chapman, I.; Bann, C.; Carter, S.L.; Stoll, B.J. Network, for the N.N.R. Language Outcomes among ELBW Infants in Early Childhood. Early Hum. Dev. 2015, 91, 373–379. [Google Scholar] [CrossRef] [Green Version]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Canadian Neonatal Follow-Up Network. 18-Month Corrected Age Assessment Manual 2018 Version 6. April 2018. Available online: https://cnfun.ca/resources/ (accessed on 31 May 2022).
- Rosenbaum, P.; Paneth, N.; Leviton, A.; Goldstein, M.; Bax, M.; Damiano, D.; Dan, B.; Jacobsson, B. A Report: The Definition and Classification of Cerebral Palsy April 2006. Dev. Med. Child Neurol. Suppl. 2007, 109, 8–14. [Google Scholar]
- Sansavini, A.; Zuccarini, M.; Gibertoni, D.; Bello, A.; Caselli, M.C.; Corvaglia, L.; Guarini, A. Language Profiles and Their Relation to Cognitive and Motor Skills at 30 Months of Age: An Online Investigation of Low-Risk Preterm and Full-Term Children. J. Speech Lang. Hear Res. 2021, 64, 2715–2733. [Google Scholar] [CrossRef]
- Loeb, D.F.; Imgrund, C.M.; Lee, J.; Barlow, S.M. Language, Motor, and Cognitive Outcomes of Toddlers Who Were Born Preterm. Am. J. Speech-Lang. Pat. 2020, 29, 625–637. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.V.; Lekhal, R.; Aaro, L.E.; Holte, A.; Schjolberg, S. The Developmental Relationship between Language and Motor Performance from 3 to 5 Years of Age: A Prospective Longitudinal Population Study. BMC Psychol. 2014, 2, 34. [Google Scholar] [CrossRef] [Green Version]
- Conti-Ramsden, G.; Durkin, K. What Factors Influence Language Impairment Considering Resilience as Well as Risk. Folia Phoniatr. Logo 2016, 67, 293–299. [Google Scholar] [CrossRef] [PubMed]
- American Speech-Language Hearing Association (n.d.). Bilingual Service Delivery (Practice Portal). Available online: www.asha.org/Practice-Portal/Professional-Issues/Bilingual-Service-Delivery/ (accessed on 27 May 2022).
- Madaschi, V.; Mecca, T.P.; Macedo, E.C.; Paula, C.S. Bayley-III Scales of Infant and Toddler Development: Transcultural Adaptation and Psychometric Properties*. Paid. Ribeirão Preto 2015, 26, 189–197. [Google Scholar] [CrossRef] [Green Version]
- Duncan, A.F.; Watterberg, K.L.; Nolen, T.L.; Vohr, B.R.; Adams-Chapman, I.; Das, A.; Lowe, J. Effect of Ethnicity and Race on Cognitive and Language Testing at Age 18-22 Months in Extremely Preterm Infants. J. Pediatr. 2012, 160, 966–971.e2. [Google Scholar] [CrossRef] [Green Version]
- Reilly, S.; Wake, M.; Ukoumunne, O.C.; Bavin, E.; Prior, M.; Cini, E.; Conway, L.; Eadie, P.; Bretherton, L. Predicting Language Outcomes at 4 Years of Age: Findings From Early Language in Victoria Study. Pediatrics 2010, 126, e1530–e1537. [Google Scholar] [CrossRef]
- Van Veen, S.; Remmers, S.; Aarnoudse-Moens, C.S.H.; Oosterlaan, J.; van Kaam, A.H.; van Wassenaer-Leemhuis, A.G. Multilingualism Was Associated with Lower Cognitive Outcomes in Children Who Were Born Very and Extremely Preterm. Acta Paediatr. 2019, 108, 479–485. [Google Scholar] [CrossRef] [Green Version]
- Werker, J. Perceptual Foundations of Bilingual Acquisition in Infancy. Ann. N. Y. Acad. Sci. 2012, 1251, 50–61. [Google Scholar] [CrossRef]
- Portocarrero, J.S.; Burright, R.G.; Donovick, P.J. Vocabulary and Verbal Fluency of Bilingual and Monolingual College Students. Arch. Clin. Neuropsychol. Off. J. Natl. Acad. Neuropsychol. 2007, 22, 415–422. [Google Scholar] [CrossRef] [Green Version]
- Luo, L.; Luk, G.; Bialystok, E. Effect of Language Proficiency and Executive Control on Verbal Fluency Performance in Bilinguals. Cognition 2010, 114, 29–41. [Google Scholar] [CrossRef]
- Li, H.; Wu, D.; Yang, J.; Xie, S.; Chang, C.; Luo, J. Bilinguals Have More Effective Executive Function: Evidence from an FNIRS Study of the Neural Correlates of Cognitive Shifting. Int. J. Bilingual. 2022, 136700692210763. [Google Scholar] [CrossRef]
- Akhtar, N.; Menjivar, J.A. Chapter 2 Cognitive and Linguistic Correlates of Early Exposure to More than One Language. Adv. Child Dev. Behav. 2012, 42, 41–78. [Google Scholar] [CrossRef] [PubMed]
- Nosarti, C.; Rushe, T.M.; Woodruff, P.W.R.; Stewart, A.L.; Rifkin, L.; Murray, R.M. Corpus Callosum Size and Very Preterm Birth: Relationship to Neuropsychological Outcome. Brain J. Neurol. 2004, 127, 2080–2089. [Google Scholar] [CrossRef] [Green Version]
- Murray, A.L.; Scratch, S.E.; Thompson, D.K.; Inder, T.E.; Doyle, L.W.; Anderson, J.F.I.; Anderson, P.J. Neonatal Brain Pathology Predicts Adverse Attention and Processing Speed Outcomes in Very Preterm and/or Very Low Birth Weight Children. Neuropsychology 2014, 28, 552–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woods, P.L.; Rieger, I.; Wocadlo, C.; Gordon, A. Predicting the Outcome of Specific Language Impairment at Five Years of Age through Early Developmental Assessment in Preterm Infants. Early Hum. Dev. 2014, 90, 613–619. [Google Scholar] [CrossRef] [PubMed]
- Paul, L.K. Developmental Malformation of the Corpus Callosum: A Review of Typical Callosal Development and Examples of Developmental Disorders with Callosal Involvement. J. Neurodev. Disord. 2010, 3, 3–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandormael, C.; Schoenhals, L.; Hüppi, P.S.; Filippa, M.; Tolsa, C.B. Language in Preterm Born Children: Atypical Development and Effects of Early Interventions on Neuroplasticity. Neural. Plast. 2019, 2019, 6873270. [Google Scholar] [CrossRef] [Green Version]
- Shinya, Y.; Kawai, M.; Niwa, F.; Kanakogi, Y.; Imafuku, M.; Myowa, M. Cognitive Flexibility in 12-Month-Old Preterm and Term Infants Is Associated with Neurobehavioural Development in 18-Month-Olds. Sci. Rep. 2022, 12, 3. [Google Scholar] [CrossRef]
- Jansson-Verkasalo, E.; Ruusuvirta, T.; Huotilainen, M.; Alku, P.; Kushnerenko, E.; Suominen, K.; Rytky, S.; Luotonen, M.; Kaukola, T.; Tolonen, U.; et al. Atypical Perceptual Narrowing in Prematurely Born Infants Is Associated with Compromised Language Acquisition at 2 Years of Age. BMC Neurosci. 2010, 11, 88. [Google Scholar] [CrossRef] [Green Version]
- Speech-Language and Audiology Canada. Learning an Additional Language in the Context of Language Disorder 2021. Available online: https://www.sac-oac.ca/sites/default/files/Position_Statement_Learning_an_Additional_Language_in_the_Context_of_Language_Disorder_EN.pdf (accessed on 27 May 2022).
- Grunau, R.V.E.; Kearney, S.M.; Whitfield, M.F. Language Development at 3 Years in Pre-term Children of Birth Weight below 1000 g. Int. J. Lang. Comm. Dis. 1990, 25, 173–182. [Google Scholar] [CrossRef]
- Sanchez, K.; Spittle, A.J.; Cheong, J.L.; Thompson, D.K.; Doyle, L.W.; Anderson, P.J.; Morgan, A.T. Language in 2-Year-Old Children Born Preterm and Term: A Cohort Study. Arch. Dis. Child 2019, 104, 647. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Entire Cohort N = 6146 | English N = 3708 | French N = 1312 | Other N = 1126 | p Value | |
|---|---|---|---|---|---|
| Patient Variables | |||||
| Gestational age, weeks, mean (SD) | 26.3 (1.4) | 26.3 (1.4) | 26.4 (1.4) | 26.3 (1.4) | 0.13 |
| Socioeconomic Variables | |||||
| Caregiver 1 level of education N (%): | |||||
| Did not complete high school | 572 (9.7) | 281 (7.9) | 170 (13.3) | 121 (11.3) | <0.01 |
| Completed high school only | 2007 (34.0) | 1272 (35.8) | 401 (31.3) | 334 (31.2) | |
| Completed post-secondary | 3320/5899 (56.3) | 1996/3549 (56.2) | 710/1281 (55.4) | 614/1069 (57.4) | |
| Caregiver 2 level of education N (%): | |||||
| Did not complete high school | 621 (11.5) | 303 (9.4) | 193 (16.2) | 125 (12.2) | <0.01 |
| Completed high school only | 2089 (38.5) | 1293 (40.2) | 431 (36.3) | 365 (35.8) | |
| Completed post-secondary | 2714/5424 (50.0) | 1618/3214 (50.3) | 565/1189 (47.5) | 531/1021 (52.0) | |
| Employed caregiver N (%) | 5489/5997 (91.5) | 3291/3604 (91.3) | 1212/1300 (93.2) | 986/1093 (90.2) | 0.02 |
| Single caregiver N (%) | 407/6146 (6.6) | 300/3708 (8.1) | 69/1312 (5.3) | 38/1126 (3.4) | <0.01 |
| Number of people in the home, median (IQR) | 4 (3, 5) | 4 (3, 5) | 4 (3, 4) | 4 (3, 5) | <0.01 |
| Number of adults in the home N (%): | |||||
| One | 382 (7.5) | 258 (8.7) | 88 (7.6) | 36 (3.7) | <0.01 |
| Two | 4085 (80.5) | 2380 (80.4) | 1002 (87.0) | 703 (73.1) | |
| Three | 319 (6.3) | 191 (6.5) | 40 (3.5) | 88 (9.2) | |
| Four or more | 288/5074 (5.7) | 131/2960 (4.4) | 22/1152 (1.9) | 135/962 (14.0) | |
| Childcare N (%): | |||||
| In the home | 793 (16.7) | 480 (17.7) | 115 (10.1) | 198 (22.5) | <0.01 |
| Outside the home | 1638 (34.6) | 780 (28.8) | 697 (61.1) | 161 (18.2) | |
| None | 2303/4734 (48.7) | 1451/2711 (53.5) | 329/1141 (28.8) | 523/882 (59.3) | |
| Rural residence | 662/4934 (13.4) | 379/2881 (13.2) | 239/1113 (21.5) | 44/940 (4.7) | <0.01 |
| Language Variables | |||||
| Number of languages exposed to N (%): | |||||
| One | 2742 (56.1) | 1828 (65.1) | 789 (70.1) | 125 (13.1) | <0.01 |
| Two | 1827 (37.4) | 850 (30.2) | 274 (24.3) | 703 (73.9) | |
| Three or more | 318/4887 (6.5) | 132/2810 (4.7) | 63/1126 (5.6) | 123/951 (12.9) | |
| At least one caregiver born in Canada N (%) | 3835/5157 (74.4) | 2576/2964 (86.9) | 1069/1291 (82.8) | 190/902 (21.1) | <0.01 |
| Caregiver 1 ethnic group N (%): | |||||
| Caucasian | 3238 (57.5) | 2042 (61.4) | 996 (77.0) | 200 (19.8) | <0.01 |
| Black | 525 (9.3) | 272 (8.2) | 204 (15.8) | 49 (4.9) | |
| Asian | 796 (14.2) | 323 (9.7) | 21 (1.6) | 452 (44.8) | |
| First Nations | 200 (3.5) | 166 (5.0) | 10 (0.8) | 24 (2.4) | |
| Other | 296 (5.3) | 91 (2.7) | 51 (3.9) | 154 (15.3) | |
| Unknown | 571/5626 (10.2) | 429/3323 (12.9) | 12/1294 (0.9) | 130/1009 (12.9) | |
| Caregiver 2 ethnic group N (%): | |||||
| Caucasian | 3119 (59.6) | 1970 (64.5) | 945 (77.9) | 204 (21.0) | <0.01 |
| Black | 457 (8.7) | 234 (7.7) | 177 (14.6) | 46 (4.8) | |
| Asian | 691 (13.2) | 241 (7.9) | 23 (1.9) | 427 (44.1) | |
| First Nations | 153 (2.9) | 127 (4.2) | 3 (0.3) | 23 (2.4) | |
| Other | 279 (5.3) | 87 (2.8) | 49 (4.0) | 143 (14.8) | |
| Unknown | 536/5235 (10.2) | 394/3053 (12.9) | 16/1213 (1.3) | 126/969 (13.0) | |
| Bayley-III Language | |||||
| Language Composite Score, median (IQR) | 91 (79, 100) | 91 (79, 100) | 91 (79, 100) | 86 (74, 97) | <0.01 |
| Language Composite < 85 N (%) | 1960/5442 (36.0) | 1151/3319 (34.7) | 397/1181 (33.6) | 412/942 (43.7) | <0.01 |
| Language Composite < 70 N (%) | 643/5442 (11.8) | 383/3319 (11.5) | 114/1181 (9.7) | 146/942 (15.5) | <0.01 |
| Other Impairments | |||||
| Hearing N (%): | |||||
| Sensorineural | 75 (1.2) | 51 (1.4) | 9 (0.7) | 15 (1.3) | <0.01 |
| Conductive | 156 (2.5) | 67 (1.8) | 71 (5.4) | 18 (1.6) | |
| Mixed | 10 (0.2) | 6 (0.2) | 3 (0.2) | 1 (0.1) | |
| Auditory Neuropathy | 29 (0.5) | 16 (0.4) | 2 (0.1) | 11 (1.0) | |
| Unknown | 40/6146 (0.7) | 26/3708 (0.7) | 10/1312 (0.8) | 4/1126 (0.4) | |
| Hearing aids or cochlear implant | 125/5957 (2.1) | 89/3579 (2.5) | 15/1288 (1.2) | 21/1090 (1.9) | 0.02 |
| Motor: | |||||
| Definitive CP N (%) | 387/6019 (6.4) | 250/3619 (6.9) | 73/1300 (5.6) | 64/1100 (5.8) | 0.17 |
| Bayley-III Motor Composite, median (IQR) | 94 (85, 100) | 94 (85, 100) | 94 (85, 100) | 94 (85, 100) | 0.05 |
| Bayley-III Motor Composite < 85 N (%) | 1164/5423 (21.5) | 727/3309 (22.0) | 231/1148 (20.1) | 206/966 (21.3) | 0.42 |
| Cognitive: | |||||
| Bayley-III Cognitive, median (IQR) | 95 (90, 105) | 95 (90, 105) | 95 (90, 105) | 95 (85, 100) | <0.01 |
| Bayley-III Cognitive < 85 N (%) | 856/5638 (15.2) | 528/3429 (15.4) | 149/1202 (12.4) | 179/1007 (17.8) | <0.01 |
| English or French N = 5020 | Other N = 1126 | |
|---|---|---|
| Bayley-III Language administered, n (%) | 4500 (89.6) | 942 (83.7) |
| Bayley-III Cognitive administered, n (%) | 4631 (92.3) | 1007 (89.4) |
| Bayley-III Motor administered, n (%) | 4457 (88.8) | 966 (85.8) |
| Primary Language at Home | |||
|---|---|---|---|
| Language of Bayley-III Administration | English N = 2705 | French N = 995 | Other N = 816 |
| English, n (%) | 2672 (98.8) | 52 (5.2) | 594 (72.8) |
| French, n (%) | 24 (0.9) | 932 (93.7) | 70 (8.6) |
| Interpreter or parent interpreter, n (%) | 9 (0.3) | 11 (1.1) | 152 (18.6) |
| Variable | Odds Ratio (95% CI 1) |
|---|---|
| English or French as a primary language | 0.67 (0.58, 0.78) |
| Language of administration | |
| French vs. English | 0.93 (0.80, 1.08) |
| Interpreter vs. English | 1.41 (1.03, 1.93) |
| Number of languages exposed to (vs. one) | |
| Two | 1.54 (1.35, 1.76) |
| More than two | 1.69 (1.31, 2.18) |
| Gestational age | 0.84 (0.80, 0.87) |
| Caregiver 1 education (vs. completed post-secondary) | |
| Did not complete high school | 2.18 (1.80, 2.65) |
| Completed high school only | 1.59 (1.41, 1.80) |
| Caregiver 2 education (vs. completed post-secondary) | |
| Did not complete high school | 1.59 (1.31, 1.92) |
| Completed high school only | 1.41 (1.24, 1.60) |
| One or two employed caregiver(s) | 0.44 (0.36, 0.53) |
| Urban vs. rural residence | 1.17 (0.97, 1.40) |
| At least one caregiver born in Canada | 0.51 (0.44, 0.59) |
| Bayley-III Motor Composite Score < 85 | 0.93 (0.93, 0.94) |
| Bayley-III Cognitive Score < 85 | 0.90 (0.90, 0.91) |
| Variable | Adjusted Odds Ratio (95% CI 1) |
|---|---|
| English or French as a primary language | 0.84 (0.68, 1.04) |
| Number of languages exposed to (vs. one) | |
| Two | 1.45 (1.21, 1.73) |
| More than two | 1.62 (1.18, 2.23) |
| Gestational age | 0.93 (0.88, 0.98) |
| Caregiver 1 education (vs. completed post-secondary) | |
| Did not complete high school | 2.16 (1.67, 2.80) |
| Completed high school only | 1.58 (1.34, 1.87) |
| Single caregiver | 1.69 (1.23, 2.32) |
| Rural residence | 1.04 (0.83, 1.31) |
| Hearing aids or cochlear implants | 2.49 (1.37, 4.49) |
| Bayley-III Motor Composite < 85 | 3.22 (2.64, 3.93) |
| Bayley-III Cognitive < 85 | 7.83 (6.04, 10.1) |
| Variable | Adjusted Odds Ratio (95% CI 1) |
|---|---|
| Language of administration | |
| French vs. English | 1.05 (0.88, 1.26) |
| Interpreter vs. English | 1.13 (0.76, 1.67) |
| Number of languages exposed to (vs. one) | |
| Two | 1.53 (1.29, 1.81) |
| More than two | 1.70 (1.24, 2.32) |
| Gestational age | 0.92 (0.88, 0.98) |
| Caregiver 1 education (vs. completed post-secondary) | |
| Did not complete high school | 2.12, (1.64, 2.76) |
| Completed high school only | 1.55 (1.31, 1.84) |
| Single caregiver | 1.62 (1.18, 2.23) |
| Rural residence | 1.04 (0.83, 1.31) |
| Hearing aids or cochlear implants | 2.42 (1.33, 4.38) |
| Motor Composite < 85 | 3.25 (2.65, 3.97) |
| Cognitive < 85 | 7.91 (6.10, 10.3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, N.H.-M.; Synnes, A.; Grunau, R.E.; Colby, L.; Petrie, J.; Elfring, T.; Richter, L.; Hendson, L.; Banihani, R.; Luu, T.M.; et al. Impact of Differing Language Background Exposures on Bayley-III Language Assessment in a National Cohort of Children Born Less than 29 Weeks’ Gestation. Children 2022, 9, 1048. https://0-doi-org.brum.beds.ac.uk/10.3390/children9071048
Chan NH-M, Synnes A, Grunau RE, Colby L, Petrie J, Elfring T, Richter L, Hendson L, Banihani R, Luu TM, et al. Impact of Differing Language Background Exposures on Bayley-III Language Assessment in a National Cohort of Children Born Less than 29 Weeks’ Gestation. Children. 2022; 9(7):1048. https://0-doi-org.brum.beds.ac.uk/10.3390/children9071048
Chicago/Turabian StyleChan, Natalie Hoi-Man, Anne Synnes, Ruth E. Grunau, Lindsay Colby, Julie Petrie, Tracy Elfring, Lindsay Richter, Leonora Hendson, Rudaina Banihani, Thuy Mai Luu, and et al. 2022. "Impact of Differing Language Background Exposures on Bayley-III Language Assessment in a National Cohort of Children Born Less than 29 Weeks’ Gestation" Children 9, no. 7: 1048. https://0-doi-org.brum.beds.ac.uk/10.3390/children9071048