
Role of Ultrasound Evaluation of Temporomandibular Joint in Juvenile Idiopathic Arthritis: A Systematic Review


1
Unit of Pediatric Rheumatology, ASST G. Pini-CTO, Via Gaetano Pini 9, 20122 Milan, Italy
2
Division of Clinical Rheumatology, ASST G. Pini-CTO, Via Gaetano Pini 9, 20122 Milan, Italy
3
Department of Clinical Sciences and Community Health, Research Center for Pediatric and Adult Rheumatic Diseases (RECAP.RD), University of Milan, Via della Commenda 19, 20122 Milan, Italy
*
Author to whom correspondence should be addressed.
Children 2022, 9(8), 1254; https://0-doi-org.brum.beds.ac.uk/10.3390/children9081254
Submission received: 3 August 2022
/
Revised: 13 August 2022
/
Accepted: 16 August 2022
/
Published: 19 August 2022
(This article belongs to the Special Issue Advances in Juvenile Idiopathic Arthritis)
Abstract
:Background: Juvenile idiopathic arthritis (JIA) is childhood’s most frequent chronic rheumatic disease. JIA is a broad term that includes all arthritides starting before 16 years, lasting at least six weeks, and of unknown cause. The temporomandibular joint (TMJ) could be involved in JIA both at onset and during the disease course. The presence of TMJ synovitis might severely impair dentofacial maturation in pediatric patients. The ultrasound (US) application to detect early signs of TMJ synovitis in children with JIA has provided contradictory results. We sought to assess the current role of TMJ US in JIA through a systematic literature review. Methods: The systematic review was conducted according to the recommendations of the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA). Results: The literature search found 345 records. After duplicates removal, 253 records were screened, 20 full-text articles were reviewed to assess their eligibility, and 7 of them were included in the qualitative analysis. Joint effusion was the most recorded parameter, followed by bony condylar abnormalities. Compared to contrast enhancement MRI, the capability to detect signs of active synovitis of TMJ by US is low, especially at the early stages. Conclusion: Understanding how US may help diagnose and manage children with JIA is advisable for several reasons. MRI cannot be frequently repeated, may need sedation, and is expensive. The constant technical improvement of US will undoubtedly allow for better evaluation of what, in the past, was not clear or not even captured by sonography. So far, the role of US in the assessment of TMJ involvement in JIA is indubitably secondary to the MRI. Even so, we think that a baseline MRI of TMJ and the repetition of the sonography over time might both help the interpretation of US images and intercept significative changes.
1. Introduction
Juvenile idiopathic arthritis (JIA) is childhood’s most frequent chronic rheumatic disease, with a prevalence estimated between 16 and 150 per 100,000. JIA is a broad term that includes all arthritides starting before 16 years, lasting at least six weeks, and of unknown cause [1,2]. According to specific characteristics displayed in the first six months of the disease, the International League of Associations for Rheumatology (ILAR) recognizes seven main categories: oligoarticular JIA, polyarticular rheumatoid factor (RF) negative JIA, polyarticular RF positive JIA, psoriatic arthritis, enthesitis-related arthritis, systemic JIA, undifferentiated JIA [3]. Nevertheless, efforts are currently ongoing to develop a new classification of inflammatory arthritis with particular regard to biological phenotypes [4].
The temporomandibular joint (TMJ) could be involved in JIA both at onset and during the disease course; TMJ arthritis may affect a substantial number of JIA patients (up to 87%) [5,6,7]. The presence of TMJ synovitis might severely impair dentofacial maturation in pediatric patients. The condyle is the principal center of mandibular growth; the cartilage ossification at this level causes an increase in the vertical height of the ramus, and puberty accelerates mandibular growth, which usually ends by the age of 18 years [8,9]. Indeed, the growth site lies on the mandibular condyle in the intracapsular joint space and can be easily damaged by arthritis [10].
In the general population, the causes of temporomandibular disorders (TMD) are various; indeed, several factors may influence the development of this alteration: traumatic or post-traumatic abnormalities, intrinsic anatomic factors, and systemic conditions [11].
In JIA patients, the term dentofacial deformity refers to the alteration in facial bone growth, development, and structure due to TMJ arthritis [12]. Micrognathia, retrognathia, and frontal facial asymmetry are the most frequently reported dentofacial deformities in JIA patients, as well as the deviation of the mandible on maximal mouth opening [13,14,15,16].
Therefore, the early recognition and adequate treatment of TMJ arthritis are advocated. Unfortunately, the assessment of TMJ involvement in JIA is still challenging. Indeed, signs of TMJ synovitis can be absent at onset, and patients might develop symptoms afterward when the damage is already present. Therefore, clinical examination is not enough to exclude active arthritis, nor to rule out other diagnoses [17,18]. In this setting, imaging plays a crucial role in the diagnosis of TMJ involvement, both for acute arthritis and residual damage. Gadolinium-enhanced MRI (Gd-MRI) represents the gold standard for the diagnosis of active synovitis of TMJ in JIA patients, even for early stages, and efforts are still ongoing to develop a validated TMJ-MRI scoring system [19,20].
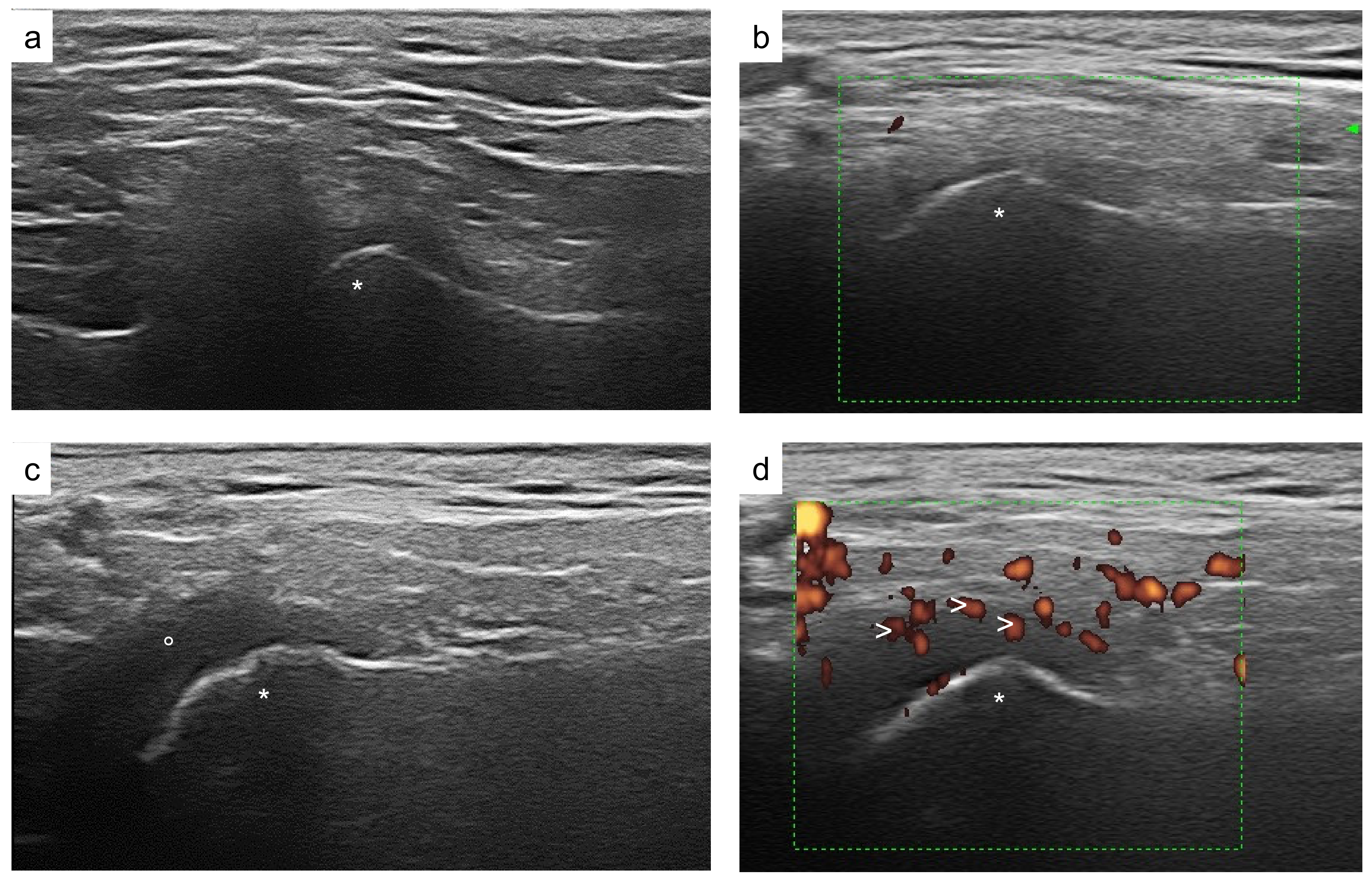
Nevertheless, the high cost, the exam length, and the frequent need for sedation are considered significant disadvantages of this imaging modality, limiting its application in daily clinical practice. Furthermore, doubts have been raised regarding the sensitivity of an abnormal TMJ-MRI exam. Indeed, a slight effusion (<1 mm of diameter) and/or contrast enhancement, in the absence of chronic changes, has been reported in healthy children as well [21]; therefore, a careful interpretation of Gd-MRI images is always advisable. Ultrasound (US) represents a rather appealing way to look at the joints since it is inexpensive, fast, noninvasive, free of ionizing radiation, and can be frequently repeated. However, US does need an expert sonographer; from a technical point of view, it cannot penetrate through both bones and dense, soft tissue structures. The US application to detect early signs of TMJ synovitis in children with JIA has provided contradictory results [22,23,24,25,26,27,28,29]. Figure 1 shows US images of TMJ. We sought to assess the current role of TMJ US in JIA through a systematic literature review. The PICO table (population, intervention, comparison, and outcome) is herein reported (Table 1).
2. Materials and Methods
A systematic review was conducted according to the recommendations of the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) [30]. This review aimed to report the current role of US in the assessment of TMJ arthritis in children with JIA.
2.1. Search Strategy
A literature search was developed first for a MEDLINE search and then adapted, if needed, to comply with the syntaxes of the following databases: EMBASE, WEB OF SCIENCE, and SCOPUS. The following keywords were used for the search: “juvenile idiopathic arthritis” OR “juvenile rheumatoid arthritis” OR “juvenile chronic arthritis” OR “juvenile idiopathic arthritides” OR “juvenile chronic arthritis” OR “Still disease” OR “still disease” OR JIA OR JCA OR JRA AND “temporomandibular joint” OR “temporomandibular joints” OR TMJ AND “Ultrasound” OR “Ultrasonography” OR “Sonography” OR “US”. The literature search was conducted through March 2022.
2.2. Inclusion/Exclusion Criteria
The inclusion criteria were randomized clinical trials, cohort studies, observational studies, and case series using ultrasound for TMJ involvement assessment in JIA patients. The exclusion criteria were the following: insufficient data regarding US use; lack of comparison indicators (either TMJ-MRI or healthy controls); non-peer-reviewed studies (e.g., conference abstracts); articles mainly reporting on JIA patients older than 20 years of age; case series reporting fewer than five JIA patients; and non-English-written studies.
2.3. Study Selection and Quality Assessment
Two reviewers (AM and ODL) reviewed the results independently. Duplicates were removed. The first evaluation relied on titles only, and then abstracts of the included titles were screened. Results considered relevant were reviewed in full text and evaluated if they met selection criteria. Two authors (AM and ODL) manually evaluated the references of each full paper assessed. In case of disagreement, a third reviewer (RC) helped to make the final decision. A discussion of the original article was conducted, and if no accord could be reached, RC was then involved. Bias criteria were adapted according to the low level of evidence within this field using Cochrane guidelines as reference [31,32]. Table 2 shows the evaluated items.
3. Results
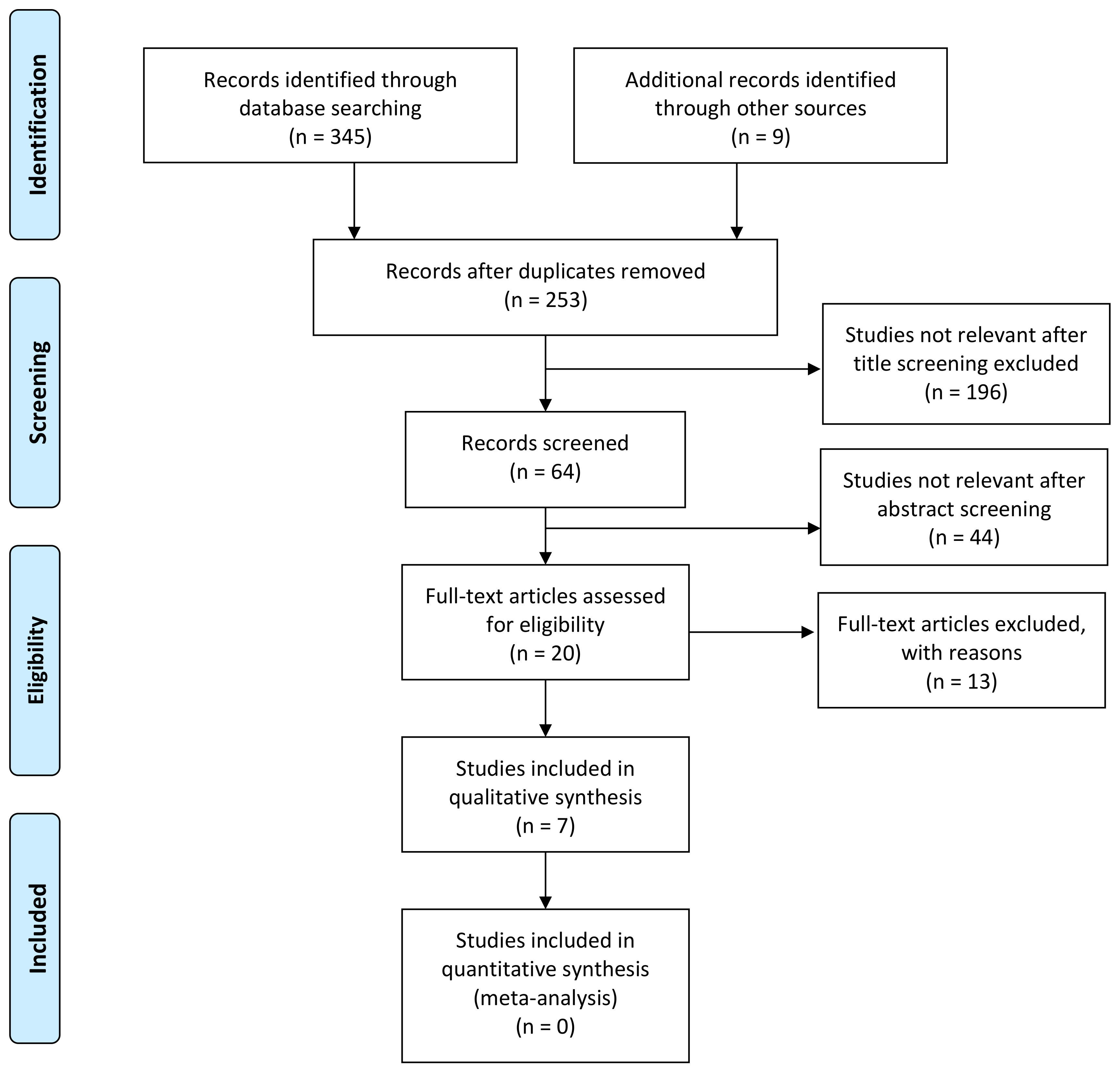
The literature search found 345 records: 183 from Medline, 28 from Embase, 86 from Web of Science, and 48 from Scopus. Nine articles were added from the reference list of records considered interesting. After duplicate removal, 253 records were screened, and 20 full-text articles were reviewed to assess their eligibility [22,23,24,25,26,27,28,29,33,34,35,36,37,38,39,40,41,42,43,44]. In total, 13 of them were excluded: 10 because they did not report enough US data, and 3 because of the lack of comparison indicators. Therefore, seven records were finally assessed for qualitative analysis (Table 3).
Figure 2 shows a PRISMA diagram. All were prospective studies; one had no TMJ-MRI done but had a control group of healthy age- and sex-matched children [25], and one single study had both TMJ-MRI assessment and a control group [29]. The median number of included subjects was 32, ranging between 8 and 92 patients. The age of the enrolled patients was comparable among the studies. The US scan was performed by a radiologist in all but one study, in which a rheumatologist performed the procedure [25]. Joint effusion was the most recorded parameter (six studies), followed by bony condylar abnormalities (four studies). The only other two parameters evaluated were synovial thickening (two studies) and power doppler signal (one study). Joint effusion and bony condylar abnormalities were recorded in four studies [23,24,25,26], with one of them also analyzing the simultaneous presence of synovial thickening [26]. One study analyzed the presence of joint effusion and synovial thickening [29]. Conversely, two studies only analyzed one parameter each (power doppler signal and joint effusion, respectively) [27,28]. Given the heterogeneity in the studies, no meta-analysis has been performed.
3.1. Joint Effusion
Joint effusion was clearly defined in three out of the six studies in which this parameter was evaluated: capsular width was used in three studies, but with different cut-offs [25,27].
Weiss et al. defined acute arthritis as the presence of joint effusion, but they did not observe any joint effusion among the 24/32 patients of their cohort who showed acute TMJ arthritis at MRI [23].
Muller et al., using a capsular cut-off of 2 mm, detected the presence of joint effusion in 8/29 (28%) patients and 10/58 (17%) joints. At the same time, signs of active TMJ synovitis were documented in 19/30 patients (63%) and 32/60 joints (53%) at MRI [24]. Melchiorre et al. reported a high rate of joint effusion (capsular cut-off of 1.5 mm) among newly diagnosed JIA patients (68%). Unfortunately, no TMJ-MRI assessment was performed, but no joint effusion was detected among the 40 healthy controls [25]. In the study by Assaf et al., US images of 20 patients with TMJ involvement previously diagnosed by MRI were analyzed. Four images of each TMJ were evaluated. Joint effusion was detected in 20 out of 160 images. Unfortunately, study results were reported in terms of positive images only, making abstracting patients’ rates impossible [26]. Kirkhus et al. compared MRI findings with US scans in 55 JIA patients; the capsular width was measured both at condylar and subcondylar levels and compared with different degrees of synovitis documented by MRI. The ROC curve showed a better performance when capsular width was measured at the subcondylar level with a proposed cut-off of 1.2 mm, a sensitivity of 72%, and a specificity of 70% [27]. Tonni et al. analyzed US findings of eight JIA patients with MRI confirmed TMJ involvement and seven healthy controls. They did not detect joint effusion by US either in the JIA patients or in the healthy controls [29].
3.2. Condylar Changes
In the study by Weiss et al., chronic TMJ arthritis, defined as the presence of condylar changes and/or erosions, was found in 9 patients (28%) by US and in 22 (69%) by MRI [23].
Deformities of the mandibular condyle (surface irregularity, erosion, flattening, and acute angulation at the transition point from the lateral to the superior condylar surface) were detected in 7/29 (24%) patients by US and in 9/30 (30%) in the study by Muller et al. [24]. Melchiorre et al. observed the presence of erosion, osteophyte formation, and bone remodeling. Condylar remodeling was observed in 62/68 patients, with bilateral involvement in the majority of them (37 cases). Erosions were found in 18 out of 124 TMJs, while 14/124 TMJs had osteophytes [25]. In the study by Assaf et al., surface irregularities and erosions were observed in 40 and 124 out of 160 images, respectively. In the same study, the thickness of the condylar disc was also evaluated (cut-off value of 1.57 mm), with 48 abnormal images out of 160 being recorded [26].
3.3. Synovial Thickening
Assaf et al. assessed the synovial thickening using a cut-off value of 1.56 mm. They found 55/160 abnormal images that documented a concurrent narrowing of the joint space [26].
Tonni et al. used the lateral periarticular joint space (LPAS) measured from the condyle’s cortical contour to the capsule’s contour as indirect parameters of the synovial joint space [29]. The measures of LPAS were significantly different between the JIA patients and the controls (0.086 cm and 0.0055 cm, respectively; p = 0.000); furthermore, the coronal closed-mouth position resulted in the most appropriate acquisition mode, given the narrowest confidence interval (0.022). However, the authors stated that LPAS does not help differentiate acute from chronic synovitis [29].
3.4. Power Doppler Signal
Ultrasound can document synovial vascularization and hyperemia through a power Doppler signal; this amplifies the US sensitivity for acute inflammation in several joints [45]. Only the study by Zwir et al. evaluated this parameter. In this study, 92 consecutive JIA patients were enrolled; all the patients had power Doppler US and MRI performed on the same day [28]. No power Doppler signal was documented among the study cohort. On the other hand, MRI detected contrast enhancement in 119 joints out of 184 TMJs.
3.5. Comparison Indicators
In all except one study [25], TMJ-MRI was performed; however, Assaf et al. used this imaging modality as the entry criterion (all the included patients had TMJ involvement detected by MRI without any further analysis) [26]. Weiss et al. compared US and MRI for acute and chronic changes, suggesting a poor correlation, especially for acute arthritis. They found a 23% agreement for acute arthritis (kappa value of 0) and a 50% agreement for chronic changes (kappa value of 0.12) [23]. On the other hand, Muller et al. reported a statistically significant correlation with active TMJ arthritis on MRI (chi-square p 0.047 for patients). Nevertheless, the level of the contrast enhancement at MRI influenced the correspondence between US and MRI: an 88% agreement in severe enhancement compared to 33% in moderate enhancement (chi-square p 0.003 for the difference) [24]. Kirkhus et al. found a moderate correlation in capsular width detected by US and synovitis at MRI (Spearman’s rho: 0.483 at the subcondylar level p = 0.001 and 0.347; p = 0.001 at condylar level) [27]. In comparison with MRI, the power Doppler signal alone, as analyzed by Zwir et al., showed poor sensitivity and specificity (0% and 36.4%, respectively) for TMJ inflammation [28]. The values of LPAS measured with US and MRI showed a positive correlation in the study by Tonni et al. (Spearman test: p of 0.623 and a p < 0.05) [29].
In comparison with the healthy controls, low values of TMJ capsule width (<1.4 mm) were found in the 40 controls by Melchiorre et al. [25]. In the other study with a comparison cohort, Tonni et al. reported a lower value of LPAS in healthy children than in JIA patients (0.0055 cm vs. 0.086 cm) [29].
4. Discussion
The technological improvements and accessibility, the low cost, the time-consumption advantages, and the lack of ionizing radiations all represent the main reasons for the spread of daily US usage in rheumatology. With regard to pediatric rheumatology, interpreting US images of JIA patients is particularly challenging given the changes in children’s growth. Nevertheless, the role of US as a diagnostic tool in JIA has not been exhaustively established yet [46]. Sonographers’ experience and advanced technology are crucial in avoiding misleading interpretations of US images. Furthermore, efforts have been made to standardize the physiological appearance of certain joints at US (but not TMJ) [47,48,49].
The peculiarity of the TMJ makes it hard to evaluate by US, since only the lateral aspect of this joint can be seen with this imaging modality [50]. This justifies the paucity and the low quality of studies on US as a diagnostic tool for TMJ synovitis in JIA. Furthermore, the different methodologies used and the US parameters analyzed make the herein retrieved studies challenging to compare. A timespan of more than ten years among the studies should be taken into consideration, especially when technical aspects might have changed over the years (machine brands, probe position descriptions, and frequency of linear transducers). All except one study used MRI for reference. However, there was no uniformity in the definition of active arthritis by MRI. For example, unlike other authors, Weiss et al. did not consider contrast enhancement as a sign of active inflammation. In this regard, efforts to develop a standardized TMJ-MRI scoring system are ongoing [20,51,52].
It is appropriate to highlight how a standardized image acquisition protocol for TMJ in children with JIA is necessary. Indeed, the difficulty in comparing the studies lies principally in the different parameters analyzed and their respective definitions. Even so, several considerations can be abstracted. No study demonstrated the superiority or the equivalence of US to MRI, which remains by far the best imaging modality to detect early signs of TMJ arthritis. Furthermore, a baseline MRI might be helpful for the US image interpretations. Indeed, US accuracy may be improved in light of the MRI result, as documented by a non-JIA study [53].
By analyzing the studies collected herein, the weakest point of US seems to be the capability to detect signs of active synovitis, especially at the early stages. This can partially be explained by the peculiarity of TMJ, both anatomically and functionally: a little joint set among the temporal bone and the mandible, the presence of the articular disc separating the superior from the inferior part, and the possibility of both sliding and hinge movements (ginglymoarthrodial joint). The need for synchronism with the contralateral TMJ represents a singularity that further complicates its evaluation. By the current evidence reported in this study, joint effusion does not appear to be a suitable parameter of active TMJ arthritis; nor does the analysis of the power Doppler signal. Synovial thickening seems more sensible than the abovementioned parameters. However, it is interesting to note that no study evaluated joint effusion, synovial thickness, and power Doppler signal altogether, despite these parameters being normally assessed in a routine US for evaluating the other joints. Furthermore, other specific parameters could help to characterize TMJ involvement in JIA. Disc dislocation detected by US has been found to play a role in the diagnosis of TMJ disorders; whether this is also true in JIA should be investigated [54].
Understanding how US may help diagnose and manage children with JIA is advisable for several reasons. MRI cannot be frequently repeated, may need sedation, and is expensive. Furthermore, knowledge about the gadolinium-based contrast medium effects is growing and, besides the nonallergic and allergy-like reactions, additional complications such as brain deposition are nowadays a matter of concern [46,47,48,49,50,51,52,53,54,55].
To date, few studies have analyzed the diagnostic value of US in TMJ synovitis of JIA patients. The parameters used in these studies were heterogeneous and needed clear definitions. The presence of joint effusion alone, the most frequently analyzed measure, has shown a modest correlation with MRI findings.
The constant technical improvement of US will undoubtedly allow for a better evaluation of what, in the past, was not clear or not even captured by sonography. As yet, the role of US in the assessment of TMJ involvement in JIA is indubitably secondary to the MRI. Even so, we think that a baseline MRI of TMJ and the repetition of the sonography over time might both help the interpretation of US images and intercept significative changes. Whether the US sensitivity for active synovitis shall be improved in the future, this paradigm could be inverted as US would become an exam of the first level for TMJ arthritis to select those patients who need an MRI.
The current efforts made for the standardized evaluation of TMJ-MRI could be essential to developing a US acquisition protocol. Indeed, using a shared MRI protocol as a reference may serve as a guide to understanding the more suitable parameters of normality and active synovitis by US.
Author Contributions
Conceptualization, A.M. and O.D.L.; methodology, A.M. and O.D.L.; validation, A.M., O.D.L. and R.C.; formal analysis, A.M.; investigation, A.M. and O.D.L.; resources, A.M. and O.D.L.; data curation, A.M. and O.D.L.; writing—original draft preparation, A.M.; writing—review and editing, A.M., O.D.L. and R.C.; visualization, A.M., O.D.L. and R.C.; supervision, A.M., O.D.L. and R.C.; project administration, A.M., O.D.L. and R.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are available on request to the authors.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| JIA | Juvenile idiopathic arthritis |
| ILAR | International League of Associations for Rheumatology |
| RF | Rheumatoid factor |
| TMJ | Temporomandibular joint |
| US | Ultrasound |
| MRI | Magnetic resonance imaging |
| Gd-MRI | Gadolinium-enhanced MRI |
| TMD | Temporomandibular disorder |
| PWD | Power Doppler |
| LPAS | Lateral periarticular joint space |
References
- Ravelli, A.; Martini, A. Juvenile idiopathic arthritis. Lancet 2007, 369, 767–778. [Google Scholar] [CrossRef]
- Cimaz, R.; Marino, A.; Martini, A. How I treat juvenile idiopathic arthritis: A state of the art review. Autoimmun. Rev. 2017, 16, 1008–1015. [Google Scholar] [CrossRef] [PubMed]
- Petty, R.E.; Southwood, T.R.; Manners, P.; Baum, J.; Glass, D.N.; Goldenberg, J.; He, X.; Maldonado-Cocco, J.; Orozco-Alcala, J.; Prieur, A.-M.; et al. International league of associations for rheumatology classification of juvenile idiopathic arthritis: Second revision, Edmonton, 2001. J. Rheumatol. 2004, 31, 390–392. [Google Scholar] [PubMed]
- Nigrovic, P.A.; Colbert, R.A.; Holers, V.M.; Ozen, S.; Ruperto, N.; Thompson, S.D.; Wedderburn, L.R.; Yeung, R.S.M.; Martini, A. Biological classification of childhood arthritis: Roadmap to a molecular nomenclature. Nat. Rev. Rheumatol. 2021, 17, 257–269. [Google Scholar] [CrossRef]
- Twilt, M.; Mobers, S.M.L.M.; Arends, L.R.; Cate, R.T.; Van Suijlekom-Smit, L. Temporomandibular involvement in juvenile idiopathic arthritis. J. Rheumatol. 2004, 31, 1418–1422. [Google Scholar] [CrossRef]
- Küseler, A.; Pedersen, T.K.; Gelineck, J.; Herlin, T. A 2 year followup study of enhanced magnetic resonance imaging and clinical examination of the temporomandibular joint in children with juvenile idiopathic arthritis. J. Rheumatol. 2005, 32, 162–169. [Google Scholar]
- Pedersen, T.K.; Küseler, A.; Gelineck, J.; Herlin, T. A prospective study of magnetic resonance and radiographic imaging in relation to symptoms and clinical findings of the temporomandibular joint in children with juvenile idiopathic arthritis. J. Rheumatol. 2008, 35, 1668–1675. [Google Scholar]
- Bender, M.E.; Lipin, R.B.; Goudy, S.L. Development of the pediatric temporomandibular joint. Oral Maxillofac. Surg. Clin. N. Am. 2018, 30, 1–9. [Google Scholar] [CrossRef]
- Nahhas, R.W.; Valiathan, M.; Sherwood, R.J. Variation in timing, duration, intensity, and direction of adolescent growth in the mandible, maxilla, and cranial base: The Fels longitudinal study. Anat. Rec. 2014, 297, 1195–1207. [Google Scholar] [CrossRef]
- Von Bremen, J.; Ruf, S. Juvenile idiopathic arthritis and now?: A systematic Literature review of changes in craniofacial morphology. J. Orofac. Orthop. 2012, 73, 265–276. [Google Scholar] [CrossRef]
- Minervini, G.; Fiorillo, L.; Russo, D.; Lanza, A.; D’Amico, C.; Cervino, G.; Meto, A.; Di Francesco, F. Prosthodontic Treatment in Patients with Temporomandibular Disorders and Orofacial Pain and/or Bruxism: A Review of the Literature. Prosthesis 2022, 4, 253–262. [Google Scholar] [CrossRef]
- Stoustrup, P.; Resnick, C.M.; Pedersen, T.K.; Abramowicz, S.; Michelotti, A.; Küseler, A.; Verna, C.; Kellenberger, C.J.; Nordal, E.B.; Caserta, G.; et al. TMJ Juvenile Arthritis Working Group. Standardizing Terminology and Assessment for Orofacial Conditions in Juvenile Idiopathic Arthritis: International, Multidisciplinary Consensus-based Recommendations. J. Rheumatol. 2019, 46, 518–522. [Google Scholar] [CrossRef]
- Chatzigianni, A.; Kyprianou, C.; Papadopoulos, M.A.; Sidiropoulou, S. Dentoalveolar characteristics in children with juvenile idiopathic arthritis. Organ./Off. J. Dtsch. Ges. Kieferorthopadie 2018, 79, 133–139. [Google Scholar] [CrossRef]
- Stoustrup, P.; Glerup, M.; Bilgrau, A.E.; Küseler, A.; Verna, C.; Christensen, A.E.; Kristensen, K.D.; Nørholt, S.E.; Twilt, M.; Herlin, T.; et al. Cumulative Incidence of Orofacial Manifestations in Early Juvenile Idiopathic Arthritis: A Regional, Three-Year Cohort Study. Arthritis Care Res. 2019, 72, 907–916. [Google Scholar] [CrossRef]
- De Sonnaville, W.; Speksnijder, C.M.; Zuithoff, N.; Verkouteren, D.; Wulffraat, N.W.; Steenks, M.H.; Rosenberg, A. Mandibular range of motion in children with juvenile idiopathic arthritis with and without clinically established temporomandibular joint involvement and in healthy children; a cross-sectional study. Pediatr. Rheumatol. Online J. 2021, 19, 106. [Google Scholar] [CrossRef]
- Cedströmer, A.L.; Andlin-Sobocki, A.; Abbu, N.; Hedenberg-Magnusson, B.; Dahlström, L.; Berntson, L. Condylar alterations and facial growth in children with juvenile idiopathic arthritis. J. Orofac. Orthop. Fortschr. Kieferorthopadie Organ/Off. J. Dtsch. Ges. Kieferorthopadie 2020, 81, 163–171. [Google Scholar] [CrossRef]
- Keller, H.; Müller, L.M.; Markic, G.; Schraner, T.; Kellenberger, C.J.; Saurenmann, R.K. Is early TMJ involvement in children with juvenile idiopathic arthritis clinically detectable? Clinical examination of the TMJ in comparison with contrast enhanced MRI in patients with juvenile idiopathic arthritis. Pediatr. Rheumatol. 2015, 13, 56. [Google Scholar] [CrossRef]
- Koos, B.; Twilt, M.; Kyank, U.; Fischer-Brandies, H.; Gaßling, V.; Tzaribachev, N. Reliability of clinical symptoms in diagnosing temporomandibular joint arthritis in juvenile idiopathic arthritis. J. Rheumatol. 2014, 41, 1871–1877. [Google Scholar] [CrossRef]
- Tolend, M.; Doria, A.S.; Meyers, A.B.; Larheim, T.A.; Abramowicz, S.; Aguet, J.; Appenzeller, S.; Arvidsson, L.Z.; Averill, L.W.; Feldman, B.M.; et al. Assessing the Reliability of the OMERACT Juvenile Idiopathic Arthritis Magnetic Resonance Scoring System for Temporomandibular Joints (JAMRIS-TMJ). J. Clin. Med. 2021, 10, 4047. [Google Scholar] [CrossRef]
- Tolend, M.A.; Twilt, M.; Cron, R.Q.; Tzaribachev, N.; Guleria, S.; von Kalle, T.; Koos, B.; Miller, E.; Stimec, J.; Vaid, Y.; et al. Toward establishing a standardized magnetic resonance imaging scoring system for temporomandibular joints in juvenile idiopathic arthritis. Arthritis Care Res. 2018, 70, 758–767. [Google Scholar] [CrossRef]
- Stoll, M.L.; Guleria, S.; Mannion, M.L.; Young, D.W.; Royal, S.A.; Cron, R.Q.; Vaid, Y.N. Defining the normal appearance of the temporomandibular joints by magnetic resonance imaging with contrast: A comparative study of children with and without juvenile idiopathic arthritis. Pediatr. Rheumatol. 2018, 16, 8. [Google Scholar] [CrossRef]
- Jank, S.; Haase, S.; Strobl, H.; Michels, H.; Häfner, R.; Missmann, M.; Bodner, G.; Mur, E.; Schroeder, D. Sonographic investigation of the temporomandibular joint in patients with juvenile idiopathic arthritis: A pilot study. Arthritis Rheum. 2007, 57, 213–218. [Google Scholar] [CrossRef]
- Weiss, P.F.; Arabshahi, B.; Johnson, A.; Bilaniuk, L.T.; Zarnow, D.; Cahill, A.M.; Feudtner, C.; Cron, R.Q. High prevalence of temporomandibular joint arthritis at disease onset in children with juvenile idiopathic arthritis, as detected by magnetic resonance imaging but not by ultrasound. Arthritis Rheum. 2008, 58, 1189–1196. [Google Scholar] [CrossRef]
- Müller, L.; Kellenberger, C.J.; Cannizzaro, E.; Ettlin, D.; Schraner, T.; Bolt, I.B.; Peltomäki, T.; Saurenmann, R.K. Early diagnosis of temporomandibular joint involvement in juvenile idiopathic arthritis: A pilot study comparing clinical examination and ultrasound to magnetic resonance imaging. Rheumatology 2009, 48, 680–685. [Google Scholar] [CrossRef]
- Melchiorre, D.; Falcini, F.; Kaloudi, O.; Bandinelli, F.; Nacci, F.; Matucci Cerinic, M. Sonographic evaluation of the temporomandibular joints in juvenile idiopathic arthritis. J. Ultrasound 2010, 13, 34–37. [Google Scholar] [CrossRef]
- Assaf, A.T.; Kahl-Nieke, B.; Feddersen, J.; Habermann, C.R. Is high-resolution ultrasonography suitable for the detection of temporomandibular joint involvement in children with juvenile idiopathic arthritis? Dentomaxillofacial Radiol. 2013, 42, 20110379. [Google Scholar] [CrossRef]
- Kirkhus, E.; Gunderson, R.B.; Smith, H.-J.; Flatø, B.; Hetlevik, S.O.; Larheim, T.A.; Arvidsson, L.Z. Temporomandibular joint involvement in childhood arthritis: Comparison of ultrasonography-assessed capsular width and MRI-assessed synovitis. Dentomaxillofacial Radiol. 2016, 45, 20160195. [Google Scholar] [CrossRef]
- Zwir, L.F.; Terreri, M.T.; do Amaral E Castro, A.; Rodrigues, W.D.R.; Fernandes, A.R.C. Is power Doppler ultrasound useful to evaluate temporomandibular joint inflammatory activity in juvenile idiopathic arthritis? Clin. Rheumatol. 2020, 39, 1237–1240. [Google Scholar] [CrossRef]
- Tonni, I.; Borghesi, A.; Tonesi, S.; Fossati, G.; Ricci, F.; Visconti, L. An ultrasound protocol for temporomandibular joint in juvenile idiopathic arthritis: A pilot study. Dentomaxillofacial Radiol. 2021, 50, 20200399. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef]
- Available online: http://www.cebm.net/oxford-centre-evidence-based-medicine-levels-evidence-march-2009/ (accessed on 3 May 2022).
- Higgins, J.P.T.; Green, S. (Eds.) The Cochrane Collaboration. In Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0; Chichester (UK): John Wiley & Son, 2011; Available online: http://www.cochrane-handbook.org (accessed on 3 May 2022).
- Chen, H.Y.; Wu, S.K.; Lu, C.C.; You, J.Y.; Lai, C.L. Assessing the mobility of the mandibular condyle by sonography. Patient Prefer. Adherence 2014, 8, 1419–1425. [Google Scholar] [CrossRef] [PubMed]
- Iordache, C.; Fatu, A.M.; Pomrleanu, C.; Scurtu, D.; Codrina, A. Temporomandibular joint in juvenile idiopathic arthritis: An imaging study and ergonomic considerations. Rom. J. Oral Rehabil. 2017, 9, 60–67. [Google Scholar]
- Von Schuckmann, L.; Klotsche, J.; Suling, A.; Kahl-Nieke, B.; Foeldvari, I. Temporomandibular joint involvement in patients with juvenile idiopathic arthritis: A retrospective chart review. Scand. J. Rheumatol. 2020, 49, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Alqanatish, J.T.; Alrewaithi, B.S.; Alsewairi, W.M.; Khan, A.H.; Alsalman, M.J.; Alrasheed, A.A. Temporomandibular joint involvement in children with juvenile idiopathic arthritis: A single tertiary-center experience. Saudi Med. J. 2021, 42, 399–404. [Google Scholar] [CrossRef]
- Parra, D.A.; Chan, M.; Krishnamurthy, G.; Spiegel, L.; Amaral, J.G.; Temple, M.J.; John, P.R.; Connolly, B.L. Use and accuracy of US guidance for image-guided injections of the temporomandibular joints in children with arthritis. Pediatr. Radiol. 2010, 40, 1498–1504. [Google Scholar] [CrossRef]
- Stoll, M.L.; Good, J.; Sharpe, T.; Beukelman, T.; Young, D.; Waite, P.D.; Cron, R.Q. Intra-articular corticosteroid injections to the temporomandibular joints are safe and appear to be effective therapy in children with juvenile idiopathic arthritis. J. Oral Maxillofac. Surg. 2012, 70, 1802–1807. [Google Scholar] [CrossRef]
- Habibi, S.; Ellis, J.; Strike, H.; Ramanan, A.V. Safety and efficacy of US-guided CS injection into temporomandibular joints in children with active JIA. Rheumatology 2011, 51, 874–877. [Google Scholar] [CrossRef]
- Young, C.M.; Shiels, W.E., II; Coley, B.D.; Hogan, M.J.; Murakami, J.W.; Jones, K.; Higgins, G.C.; Rennebohm, R.M. Ultrasound-guided corticosteroid injection therapy for juvenile idiopathic arthritis: 12-year care experience. Pediatr. Radiol. 2012, 42, 1481–1489. [Google Scholar] [CrossRef]
- Stoll, M.L.; Morlandt, A.B.; Teerawattanapong, S.; Young, D.; Waite, P.D.; Cron, R.Q. Safety and efficacy of intra-articular infliximab therapy for treatment-resistant temporomandibular joint arthritis in children: A retrospective study. Rheumatology 2012, 52, 554–559. [Google Scholar] [CrossRef]
- Olsen-Bergem, H.; Bjørnland, T. A cohort study of patients with juvenile idiopathic arthritis and arthritis of the temporomandibular joint: Outcome of arthrocentesis with and without the use of steroids. Int. J. Oral. Maxillofac. Surg. 2014, 43, 990–995. [Google Scholar] [CrossRef]
- Resnick, C.M.; Vakilian, P.M.; Kaban, L.B.; Peacock, Z.S. Is Intra-Articular Steroid Injection to the Temporomandibular Joint for Juvenile Idiopathic Arthritis More Effective and Efficient When Performed With Image Guidance? J. Oral. Maxillofac. Surg. 2017, 75, 694–700. [Google Scholar] [CrossRef] [PubMed]
- Frid, P.; Augdal, T.A.; Larheim, T.A.; Halbig, J.; Rypdal, V.; Songstad, N.T.; Rosén, A.; Tylleskär, K.B.; Berstad, J.R.; Flatø, B.; et al. Efficacy and safety of intraarticular corticosteroid injections in adolescents with juvenile idiopathic arthritis in the temporomandibular joint: A Norwegian 2-year prospective multicenter pilot study. Pediatr. Rheumatol. Online J. 2020, 18, 75. [Google Scholar] [CrossRef] [PubMed]
- Johnson, K. Imaging of juvenile idiopathic arthritis. Pediatr. Radiol. 2006, 36, 743–758. [Google Scholar] [CrossRef] [PubMed]
- Cimaz, R.; Giani, T.; Caporali, R. What is the real role of ultrasound in the management of juvenile idiopathic arthritis? Ann. Rheum. Dis. 2020, 79, 437–439. [Google Scholar] [CrossRef]
- Collado, P.; Vojinovic, J.; Nieto, J.C.; Windschall, D.; Magni-Manzoni, S.; Bruyn, G.A.W.; Iagnocco, A.; D’Agostino, M.A.; Naredo, E.; on behalf of the Omeract Ultrasound Pediatric Group. Toward standardized musculoskeletal ultrasound in pediatric rheumatology: Normal age-related ultrasound findings. Arthritis Care Res. 2016, 68, 348–356. [Google Scholar] [CrossRef]
- Collado, P.; Windschall, D.; Vojinovic, J.; Magni-Manzoni, S.; Balint, P.; Bruyn, G.A.; Hernandez-Diaz, C.; Nieto, J.C.; Ravagnani, V.; Tzaribachev, N.; et al. Amendment of the OMERACT ultrasound definitions of joints’ features in healthy children when using the DOPPLER technique. Pediatr. Rheumatol. 2018, 16, 23. [Google Scholar] [CrossRef]
- Windschall, D.; Collado, P.; Vojinovic, J.; Magni-Manzoni, S.; Balint, P.; Bruyn, G.A.; Hernandez-Diaz, C.; Nieto, J.C.; Ravagnani, V.; Tzaribachev, N.; et al. Age-Related vascularization and ossification of joints in children: An international pilot study to test multi-observer ultrasound reliability. Arthritis Care Res. 2017, 72, 498–506. [Google Scholar] [CrossRef]
- Katzberg, R.W.; Conway, W.F.; Ackerman, S.J.; Gonzales, T.S.; Kheyfits, V.; Cronan, M.S. Pilot study to show the feasibility of high-resolution sagittal ultrasound imaging of the temporomandibular joint. J. Oral Maxillofac. Surg. 2017, 75, 1151–1162. [Google Scholar] [CrossRef]
- Tolend, M.; Junhasavasdikul, T.; Cron, R.Q.; Clemente, E.J.I.; von Kalle, T.; Kellenberger, C.J.; Koos, B.; Miller, E.; van Rossum, M.A.; Saurenmann, R.K.; et al. Discrete choice experiment on a magnetic resonance imaging scoring system for temporomandibular joints in juvenile idiopathic arthritis. Arthritis Care Res. 2021, 74, 308–316. [Google Scholar] [CrossRef]
- Kellenberger, C.J.; Junhasavasdikul, T.; Tolend, M.; Doria, A.S. Temporomandibular joint atlas for detection and grading of juvenile idiopathic arthritis involvement by magnetic resonance imaging. Pediatr. Radiol. 2017, 48, 411–426. [Google Scholar] [CrossRef]
- Jank, S.; Rudisch, A.; Bodner, G.; Brandlmaier, I.; Gerhard, S.; Emshoff, R. High-resolution ultrasonography of the TMJ: Helpful diagnostic approach for patients with TMJ disorders? J. Craniomaxillofac. Surg. 2001, 29, 366–371. [Google Scholar] [CrossRef]
- Klatkiewicz, T.; Gawriołek, K.; Pobudek Radzikowska, M.; Czajka-Jakubowska, A. Ultrasonography in the Diagnosis of Temporomandibular Disorders: A Meta-Analysis. Med. Sci. Monit. 2018, 24, 812–817. [Google Scholar] [CrossRef]
- Rossi Espagnet, M.C.; Bernardi, B.; Pasquini, L.; Talamanca, L.; Tom, P.; Napolitano, A. Signal intensity at unenhanced T1-weighted magnetic resonance in the globus pallidus and dentate nucleus after serial administrations of a macrocyclic gadolinium based contrast agent in children. Pediatr. Radiol. 2017, 47, 1345–1352. [Google Scholar] [CrossRef]
Figure 1.
Ultrasound images of the temporomandibular joint. Regular TMJ aspect of grayscale and Power Doppler signal (a,b); abnormal TMJ findings: TMJ effusion (c); increased intrasynovial power doppler signal (d); * mandibular condyle; ° intraarticular synovial fluid; > intrasynovial power doppler signal.
Figure 1.
Ultrasound images of the temporomandibular joint. Regular TMJ aspect of grayscale and Power Doppler signal (a,b); abnormal TMJ findings: TMJ effusion (c); increased intrasynovial power doppler signal (d); * mandibular condyle; ° intraarticular synovial fluid; > intrasynovial power doppler signal.

Figure 2.
PRISMA flow diagram.


{kind=link}
{kind=link}
Table 1.
The PICO table (population, intervention, comparison, and outcome).
| PICO |
|---|
| Patients: Patients with JIA evaluated for TMJ involvement Intervention: Use of US for assessment of TMJ involvement Comparison: Comparison with healthy controls and/or MRI for evaluation of TMJ involvement Outcome: Identify active synovitis of TMJ in JIA patients Database included: Medline via PubMed, EMBASE, WEB OF SCIENCE, SCOPUS |
Table 2.
The quality assessment of included studies.
| Study | Study Type | Level of Evidence | Uniform Inclusion Criteria | Standardized Imaging Protocol | Sufficient Outcome Variables Description | Blinded Assessor | Risk of Bias |
|---|---|---|---|---|---|---|---|
| Weiss [23] | Prospective | 3b | No | Yes | No | Unclear | High |
| Muller [24] | Prospective | 4 | Yes | Yes | Yes | Yes | Low |
| Melchiorre [25] | Prospective | 4 | No | Yes | Yes | Yes | High |
| Assaf [26] | Prospective | 3b | No | Yes | Yes | No | High |
| Kirkhus [27] | Prospective | 4 | No | Yes | No | Yes | High |
| Zwir [28] | Prospective | 4 | Yes | Yes | No | Yes | High |
| Tonni [29] | Prospective | 3b | No | Yes | Yes | Unclear | High |
Level of evidence: Oxford Centre for Evidence-Based Medicine using the protocol for differential diagnosis/symptom-prevalence studies http://www.cebm.net/oxford-centre-evidence-based-medicine-levels-evidence-march-2009/ (accessed on 3 May 2022).
Table 3.
Description of included studies.
| Weiss et al. (2008) [23] | Muller et al. (2009) [24] | Melchiorre et al. (2010) [25] | Assaf et al. (2015) [26] | Kirkhus et al. (2016) [27] | Zwir et al. (2020) [28] | Tonni et al. (2021) [29] | |
|---|---|---|---|---|---|---|---|
| N of JIA pts (female)/joints | 32 (25)/64 | 30(16)/60 | 68 (57)/136; 40 healthy controls | 20 (16)/40 | 55 (42) | 92(63)/184 | 8(7)/14; 7 healthy controls |
| Age, years | 8.6 (median) | 9.8 (median) | 11 (mean) | 11.06 (mean) | 12.4 (mean) | 12.7 (mean) | 11.6 (mean) |
| Transducer frequency | 12.5 MHz | 12 MHz | 8.5 MHz | 12 MHz | 12–18 MHz | 13 and 6.7 ** MHz | 15 MHz |
| Who did the US? | Radiologist | Radiologist | Rheumatologist | Radiologist | Radiologist | Radiologist | Radiologist |
| Joint effusion | 0 pts (Defined as fluid collection in the joint) | 8/29 (28%) pts and 10/58 (17%) joints (Defined as thickening of the joint capsule (>2 mm)) | 46/68 pts (68% (bilateral in 16 (35%) cases) (Defined as thickening of the joint capsule >1.5 mm and the presence of a hypoechoic area within the joint space) | 20 positive images/160 (12.5%) (Defined as sonographically visible fluid accumulation within the articular space) | Sensitivity 72%, specificity 70% for the capsular width at the subcondylar level * (Capsular width was measured as an indirect measurement of synovitis. Capsular cut-off of 1.2 mmL) | NE | 0 pts |
| Synovial thickening | NE | NE | NE | 55 positive images/160 (34.4%) (Defined as a value greater than 1.56 mm) | NE | NE | LPAS of JIA pts 0.086 cm LPAS of controls 0.0055 cm (Evaluated as the lateral periarticular space (LPAS) Defined as the width of the synovial joint space measured from the cortical contour of the condyle to the contour of the capsule) |
| Synovial PWD | NE | NE | NE | NE | NE | 0 pts | NE |
| Condylar changes | 9 pts (28%) | 7/29 (24%) pts and 10/58 (17%) joints | 62 (91.2%) out of 68 pts | 124 positive images/160 (77.5%) | NE | NE | NE |
| TMJ-MRI assessment and/or healthy controls comparison | 23% agreement and a kappa coefficient of 0 for acute TMJ arthritis 50% agreement and a kappa coefficient of 0.12 for chronic TMJ involvement | A pathological US was statistically significantly correlated with active TMJ arthritis on MRI (chi-square p 0.008 for all joints and p 0.047 for patients) | No TMJ-MRI assessment. In all 40 healthy controls, the TMJ capsule was less than 1.4 mm thick | For every enrolled patient the involvement of the TMJ was proven by MRI | The correlation between ultrasonography-assessed capsular width and MRI-assessed amount of synovitis was moderate both at the subcondylar and at the condylar levels (Spearman’s rho (r): 0.483; p, 0.001 and 0.347; p, 0.001, respectively). | Poor sensitivity (0%), low specificity (36.4%), very low positive predictive value (0%), and high negative predictive value (100%) when compared with MR | The Spearman test applied to the values of LPAS measured in ultrasound and the corresponding MR images showed a proportional positive correlation with a p of 0.623 and a p < 0.05 |
* No number of positive findings was recorded. ** Multi-frequency linear probe at a maximum frequency of 13 MHz for gray-scale US and 6.7 MHz for power Doppler US. JIA: juvenile idiopathic arthritis; pts: patients; PWD: power Doppler; US: ultrasound; MRI: magnetic resonance imaging; TMJ: temporomandibular joint.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Marino, A.; De Lucia, O.; Caporali, R. Role of Ultrasound Evaluation of Temporomandibular Joint in Juvenile Idiopathic Arthritis: A Systematic Review. Children 2022, 9, 1254. https://0-doi-org.brum.beds.ac.uk/10.3390/children9081254
AMA Style
Marino A, De Lucia O, Caporali R. Role of Ultrasound Evaluation of Temporomandibular Joint in Juvenile Idiopathic Arthritis: A Systematic Review. Children. 2022; 9(8):1254. https://0-doi-org.brum.beds.ac.uk/10.3390/children9081254
Chicago/Turabian StyleMarino, Achille, Orazio De Lucia, and Roberto Caporali. 2022. "Role of Ultrasound Evaluation of Temporomandibular Joint in Juvenile Idiopathic Arthritis: A Systematic Review" Children 9, no. 8: 1254. https://0-doi-org.brum.beds.ac.uk/10.3390/children9081254
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.