Interface between Periodontal Tissues and Dental Materials: Dynamic Changes and Challenges


Department of General Surgery and Surgical-Medical Specialties, School of Dentistry, University of Catania, 95124 Catania, Italy
Coatings 2021, 11(5), 485; https://0-doi-org.brum.beds.ac.uk/10.3390/coatings11050485
Submission received: 18 April 2021
/
Accepted: 19 April 2021
/
Published: 21 April 2021
(This article belongs to the Special Issue Dental Application and Surface)
{kind=link}
{kind=link}
Editorial
Periodontal tissues play an important role in the correct aesthetics, function and comfort of the dentition. The presence of a healthy periodontium represents the key to all conservative, endodontic and prosthetic therapies as an initial requirement for clinical success. In this regard, the interaction between periodontology and restorative dentistry is present in several clinical areas, which include the interface between the position of the restoration margins, the contours of the dental crown and the subsequent response of the gingival tissues to conservative and prosthetic restorations.
In this regard, the strong relationship between iatrogenic factors due to the use of biomaterials and periodontal problems have been the subject of study in the last decades. Subsequently, for several decades many studies have focused their attention on different aspects of the interaction of the periodontal-restorative interface, such as “position of the restoration with respect to the gingival margin, presence of protrusions, presence of marginal losses, surface roughness and type of restorative material” [1].
Among the various fields of research, one of the most studied mechanisms by which dental restorations can affect periodontal health is the increase in the accumulation of bacterial plaque at the interface. However, changes in the composition of the subgingival microbiota have also been described in the presence of overflowing metal restorations with an increase in pathogenic periodontal microflora [2]. These conditions can be accelerated or worsened if associated with the presence of orthodontic treatment or in young patients. Cross-sectional data on microbiological changes occurring in subgingival flora after placement of well subgingival restorations made with different materials used in dentistry were reported by van Dijken et al. [3], while there is still no specific evidence with long-term follow-up.
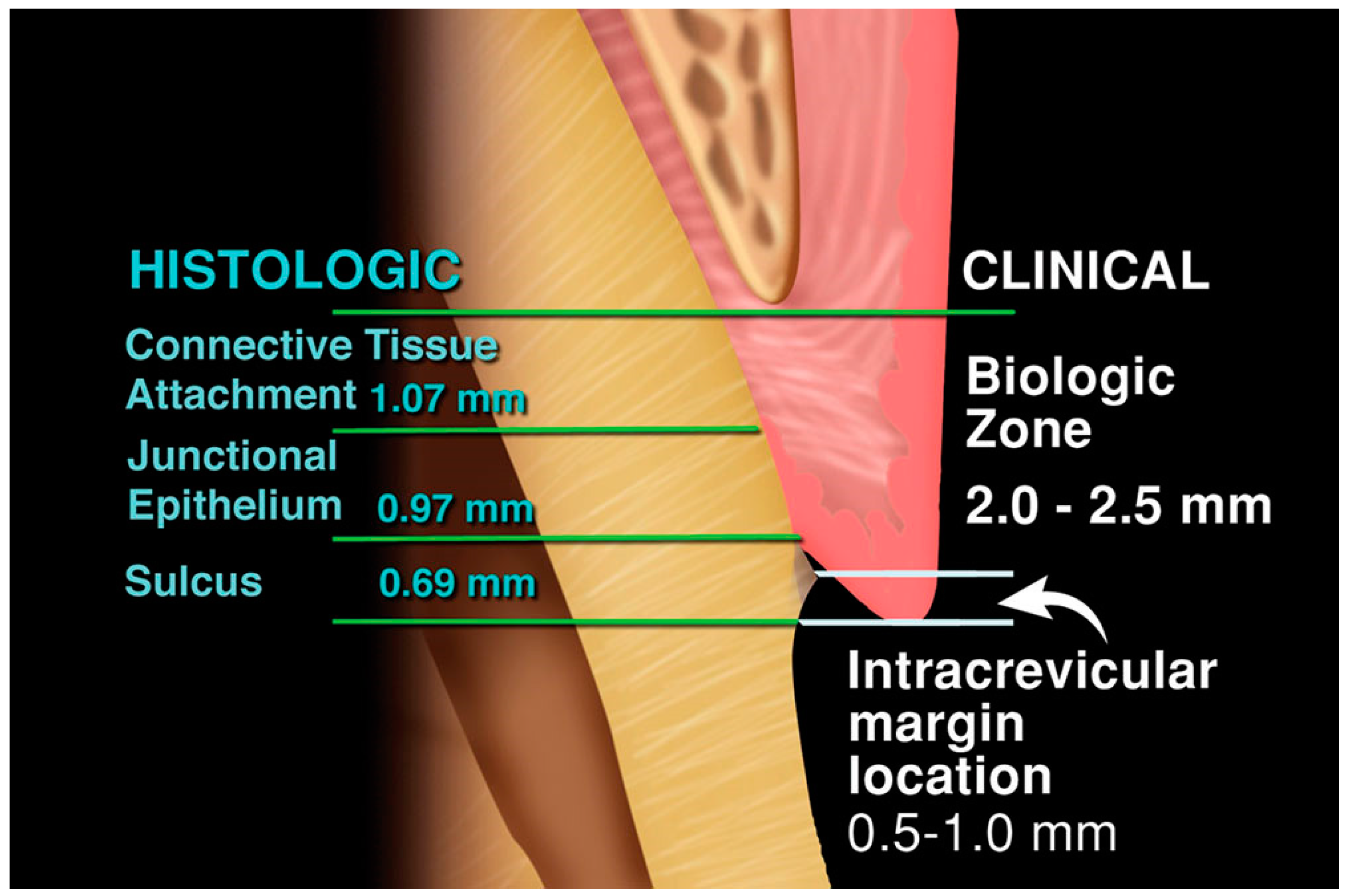
The marginal periodontium is a highly important position to be considered in restorations involving the cervical third of the dental element and prosthetic restoration (Figure 1). In this regard, much attention should be paid to the periodontium’s response to irritants resulting from imprudent techniques, which can initiate or add to existing gingival inflammation. In turn, loss of periodontal support and subsequent tooth loss can occur if the condition is not recognized and treated in its early stages [4,5,6,7,8]. Dental restorations or appliances are often associated with the development of gum inflammation, especially when they are subgingivally located. In this regard, restorations can affect biological width if they are placed deep in the sulcus or within the junctional epithelium. This can promote inflammation and loss of clinical attachment with apical migration of the junctional epithelium and reestablishment of the attachment apparatus at a more apical level [9].
Available data on the effects of composite resin restorations on gingival health is still controversial. Larato et al. [10] reported that class V composite resin restorations adjacent to the subgingival region lead to gingival inflammation. Similarly, Willershausen et al. [11] reported increased gingival bleeding and greater probing depth with the use of resin-based restorations, compared to other restorative materials.
However, van Dijken et al. [12] reported a significant increase in gingival inflammation with composite resin 3–4 years after restoration. This observation is based on the principle that surface deterioration resulting in increased plaque accumulation occurs after in vivo wear in composite resin restorations. This observation may explain the relationship between subgingival composite resin restorations and gingival health.
Additionally, several studies have documented increased inflammation or recession of the gingiva adjacent to restorations where plaque indices are low. In these studies, the products released from the materials could cause inflammation in the absence of plaque or could inhibit plaque formation and cause inflammation of the gum [13,14,15,16]. Some basic research has been conducted in vitro, showing that dental materials and plaque components can synergize to increase inflammatory reactions. The cements exhibit certain cytotoxicity in the recently set state, but this substantially decreases with time with an important action by the saliva proteins [17].
In vitro tests revealed that the initial direct contact of the composites with the gingival fibroblasts is highly cytotoxic. This cytotoxicity is mainly from uncured components in the air inhibited layer filtering from the materials [18]. Other in vitro studies, which had “aged” the composites in artificial saliva for up to six weeks, have shown that toxicity decreases in some materials but remains high in others [19].
Another problem to be analyzed is that of the alloys used for dental prostheses. Cast alloys have a long history of in vivo use with a generally good record of biocompatibility. Some questions have arisen about the biological responsibility of elemental release from many of the formulations developed over the past 10 years, but there is no clinical evidence that biomaterials can represent concerns other than hypersensitivity.
Nickel allergy is a relatively common problem, occurring in 10% to 20% of women, and is a significant risk from nickel-based alloys because the release of nickel ions from these alloys is generally greater than from noble alloys [20].
Palladium sensitivity has also been a concern in some countries, although a true palladium allergy is one-third as common as nickel allergy. However, it has been clinically documented that patients with palladium allergy are virtually always allergic to nickel. The reverse, however, is not true. In vitro, numerous articles have been published on the effects of metal ions on cells in gum tissues, such as epithelial cells, fibroblasts, and macrophages.
For the most part, the concentrations of metal ions needed to cause problems with these cells in vitro are greater than those released by most casting alloys. However, the most recent research has shown that prolonged exposures to low doses of metal ions can also have biological responsibilities.
The biocompatibility of the dental material depends on its position, composition, and interactions with the oral cavity. Metallic, ceramic, and polymeric materials [21,22,23] elicit different biological responses due to their differences in composition. Furthermore, the various biological responses to these materials are determined by the release of their components and whether these components at their released concentrations are toxic, immunogenic, or mutagenic. Its position in the oral cavity partially determines the biocompatibility of a material [24,25,26,27]. Materials that appear biocompatible in contact with the surface of the oral mucosa can cause adverse reactions if they are implanted beneath it (Figure 2). The surface characteristics of a material that promote or discourage the attachment of bacteria, host cells, or biological molecules determine whether the material will promote plaque retention, integrate with bone, or adhere to dentin.
All the above evidence demonstrates how periodontal health and dental restorations are closely related. Periodontal health is essential for the proper functioning of all restorations, while functional stimulation due to dental restorations is necessary for periodontal protection. Coronal fillings with incorrect occlusal modeling, oversized proximally or on the vestibular surfaces, or with poor interproximal contact, negatively impact the healthy periodontium and establish an additional irritation source for the periodontium already affected by the disease.
In this regard, it is essential to underline how the periodontium must remain healthy for the restorations to last for a long time, so that the teeth are maintained.
This Special Issue will provide information on the dynamic changes and challenges at the interface of biomaterials and dental technologies, aiming to improve dental treatment options and dental care.
To maintain or enhance the patient’s aesthetic appearance, the tooth/tissue interface must possess a healthy and natural appearance, with gingival tissues surrounding the properly restored teeth. For the periodontium to remain healthy, it is essential that the restoration is regularly and adequately performed to respect the periodontal tissues with a highly harmonious relationship that allows to preserve the oral tissues, the restoration itself, and the long-term clinical and biological success of the therapy.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The author declares no conflict of interest.
References
- Black, A. Preventive treatment of periodontal diseases. NW Dent. J. 1912, 10, 60–73. [Google Scholar]
- Lang, N.P.; Kiel, R.A.; Anderhalden, K. Clinical and microbiological effects of subgingival restorations with overhanging or clinically perfect margins. J. Clin. Periodontol. 1983, 10, 563–578. [Google Scholar] [CrossRef] [PubMed]
- Van Dijken, J.W.; Sjostrom, S.; Wing, K. The effect of different types of composite resin fillings on marginal gingiva. J. Clin. Periodontol. 1987, 14, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Afacan, B.; Ozturk, V.O.; Pasali, C.; Bozkurt, E.; Kose, T.; Emingil, G. Gingival crevicular fluid and salivary HIF-1alpha, VEGF, and TNF-alpha levels in periodontal health and disease. J. Periodontol. 2019, 90, 788–797. [Google Scholar] [CrossRef]
- Leonardi, R.; Perrotta, R.E.; Almeida, L.E.; Loreto, C.; Musumeci, G. Lubricin in synovial fluid of mild and severe temporomandibular joint internal derangements. Med. Oral Patol. Oral Cir. Bucal 2016, 21, e793–e799. [Google Scholar] [CrossRef] [Green Version]
- Leonardi, R.; Talic, N.F.; Loreto, C. MMP-13 (collagenase 3) immunolocalisation during initial orthodontic tooth movement in rats. Acta Histochem. 2007, 109, 215–220. [Google Scholar] [CrossRef]
- Loreto, C.; La Rocca, G.; Anzalone, R.; Caltabiano, R.; Vespasiani, G.; Castorina, S.; Ralph, D.J.; Cellek, S.; Musumeci, G.; Giunta, S.; et al. The role of intrinsic pathway in apoptosis activation and progression in Peyronie’s disease. Biomed Res Int. 2014, 2014, 616149. [Google Scholar] [CrossRef] [PubMed]
- Leonardi, R.; Almeida, L.E.; Trevilatto, P.C.; Loreto, C. Occurrence and regional distribution of TRAIL and DR5 on temporomandibular joint discs: Comparison of disc derangement with and without reduction. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, 244–251. [Google Scholar] [CrossRef] [Green Version]
- Leonardi, R.; Loreto, C.; Talic, N.; Caltabiano, R.; Musumeci, G. Immunolocalization of lubricin in the rat periodontal ligament during experimental tooth movement. Acta Histochem. 2012, 114, 700–704. [Google Scholar] [CrossRef]
- Nakahara, T.; Nakamura, T.; Kobayashi, E.; Kuremoto, K.; Matsuno, T.; Tabata, Y.; Eto, K.; Shimizu, Y. In situ tissue engineering of periodontal tissues by seeding with periodontal ligament-derived cells. Tissue Eng. 2004, 10, 537–544. [Google Scholar] [CrossRef]
- Larato, D.C. Influence of a composite resin restoration on the gingiva. J. Prosthet. Dent. 1972, 28, 402–404. [Google Scholar] [CrossRef]
- Willershausen, B.; Kottgen, C.; Ernst, C.P. The influence of restorative materials on marginal gingiva. Eur. J. Med. Res. 2001, 6, 433–439. [Google Scholar]
- Van Winkelhoff, A.J.; van der Velden, U.; de Graaff, J. Microbial succession in recolonizing deep periodontal pockets after a single course of supra- and subgingival debridement. J. Clin. Periodontol. 1988, 15, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Cosgarea, R.; Tristiu, R.; Dumitru, R.B.; Arweiler, N.B.; Rednic, S.; Sirbu, C.I.; Lascu, L.; Sculean, A.; Eick, S. Effects of non-surgical periodontal therapy on periodontal laboratory and clinical data as well as on disease activity in patients with rheumatoid arthritis. Clin. Oral Investig. 2019, 23, 141–151. [Google Scholar] [CrossRef]
- Hong, J.Y.; Lee, J.S.; Choi, S.H.; Shin, H.S.; Park, J.C.; Shin, S.I.; Chung, J.H. A randomized, double-blind, placebo-controlled multicenter study for evaluating the effects of fixed-dose combinations of vitamin C, vitamin E, lysozyme, and carbazochrome on gingival inflammation in chronic periodontitis patients. BMC Oral Health 2019, 19, 40. [Google Scholar] [CrossRef] [PubMed]
- Pedroso, J.F.; Lotfollahi, Z.; Albattarni, G.; Arrruda Schulz, M.; Monteiro, A.; Sehnem, A.L.; Gidlund, M.A.; Neto, A.M.F.; Jardini, M.A.N. Influence of Periodontal Disease on cardiovascular markers in Diabetes Mellitus patients. Sci. Rep. 2019, 9, 16138. [Google Scholar] [CrossRef]
- Shinjo, T.; Ishikado, A.; Hasturk, H.; Pober, D.M.; Paniagua, S.M.; Shah, H.; Wu, I.H.; Tinsley, L.J.; Matsumoto, M.; Keenan, H.A.; et al. Characterization of periodontitis in people with type 1 diabetes of 50 years or longer duration. J. Periodontol. 2019, 90, 565–575. [Google Scholar] [CrossRef]
- Nair, P.; Ilie, N. The long-term consequence of salivary contamination at various stages of adhesive application and clinically feasible remedies to decontaminate. Clin. Oral Investig. 2020, 24, 4413–4426. [Google Scholar] [CrossRef] [PubMed]
- Darmani, H.; Al-Hiyasat, A.S.; Milhem, M.M. Cytotoxicity of dental composites and their leached components. Quintessence Int. 2007, 38, 789–795. [Google Scholar]
- Sato, T.; Mello, D.; Vasconcellos, L.; Valente, A.J.M.; Borges, A. Chitosan-based coacervate polymers for propolis encapsulation: Release and cytotoxicity studies. Int. J. Mol. Sci. 2020, 21, 4561. [Google Scholar] [CrossRef]
- Setcos, J.C.; Babaei-Mahani, A.; Silvio, L.D.; Mjor, I.A.; Wilson, N.H. The safety of nickel containing dental alloys. Dent. Mater. 2006, 22, 1163–1168. [Google Scholar] [CrossRef]
- De Felice, M.E.; Nucci, L.; Fiori, A.; Flores-Mir, C.; Perillo, L.; Grassia, V. Accuracy of interproximal enamel reduction during clear aligner treatment. Prog. Orthod. 2020, 21, 28. [Google Scholar] [CrossRef] [PubMed]
- Grassia, V.; Lombardi, A.; Kawasaki, H.; Ferri, C.; Perillo, L.; Mosca, L.; Delle Cave, D.; Nucci, L.; Porcelli, M.; Caraglia, M. Salivary microRNAs as new molecular markers in cleft lip and palate: A new frontier in molecular medicine. Oncotarget 2018, 9, 18929–18938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camerlingo, C.; d’Apuzzo, F.; Grassia, V.; Perillo, L.; Lepore, M. Micro-Raman spectroscopy for monitoring changes in periodontal ligaments and gingival crevicular fluid. Sensors 2014, 14, 22552–22563. [Google Scholar] [CrossRef] [Green Version]
- De Avila, E.D.; van Oirschot, B.A.; van den Beucken, J. Biomaterial-based possibilities for managing peri-implantitis. J. Periodontal. Res. 2020, 55, 165–173. [Google Scholar] [CrossRef]
- Fichera, G.; Martina, S.; Palazzo, G.; Musumeci, R.; Leonardi, R.; Isola, G.; Lo Giudice, A. New Materials for Orthodontic Interceptive Treatment in Primary to Late Mixed Dentition. A Retrospective Study Using Elastodontic Devices. Materials 2021, 14, 1695. [Google Scholar] [CrossRef]
- Sterzenbach, T.; Helbig, R.; Hannig, C.; Hannig, M. Bioadhesion in the oral cavity and approaches for biofilm management by surface modifications. Clin. Oral Investig. 2020, 24, 4237–4260. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Periodontal tissue-dental materials interface.

Figure 2.
Biological differences between natural tooth and dental implant.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Isola, G. Interface between Periodontal Tissues and Dental Materials: Dynamic Changes and Challenges. Coatings 2021, 11, 485. https://0-doi-org.brum.beds.ac.uk/10.3390/coatings11050485
AMA Style
Isola G. Interface between Periodontal Tissues and Dental Materials: Dynamic Changes and Challenges. Coatings. 2021; 11(5):485. https://0-doi-org.brum.beds.ac.uk/10.3390/coatings11050485
Chicago/Turabian StyleIsola, Gaetano. 2021. "Interface between Periodontal Tissues and Dental Materials: Dynamic Changes and Challenges" Coatings 11, no. 5: 485. https://0-doi-org.brum.beds.ac.uk/10.3390/coatings11050485
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.