
Development of a Prognostic Model for Stump Healing in Major Lower Limb Amputation among the Diabetic Population

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Research Design
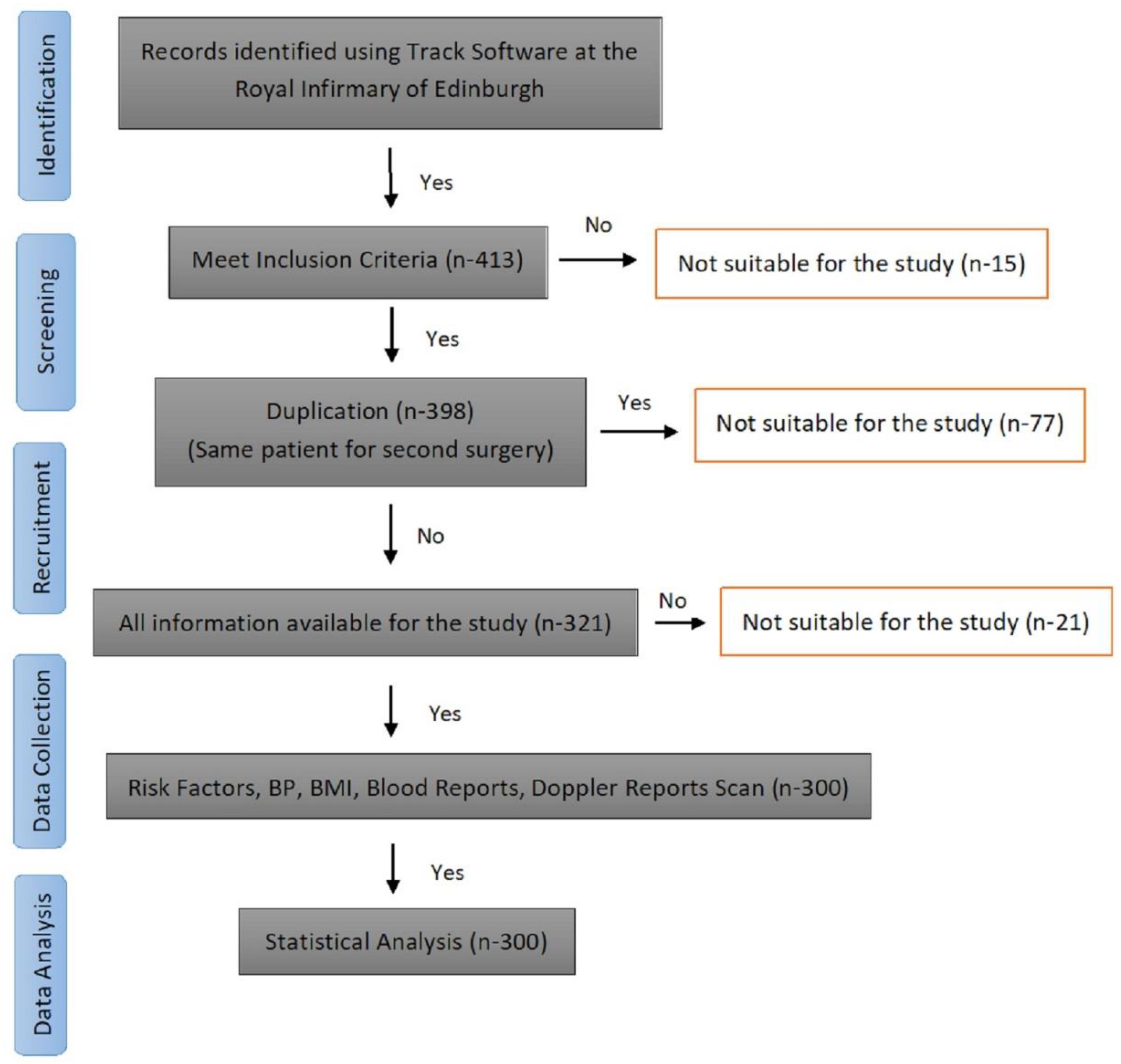
2.2. Study Participants
2.2.1. Inclusion Criteria
- -
- Patients whose age was 18 years and above.
- -
- Both genders (male and female) were eligible for the study.
- -
- Patients who had an amputation at a level of below or above knee for the first time.
2.2.2. Exclusion Criteria
2.3. Data Collection
2.4. Predictive Measure—Stump Healing
2.5. Sample Size
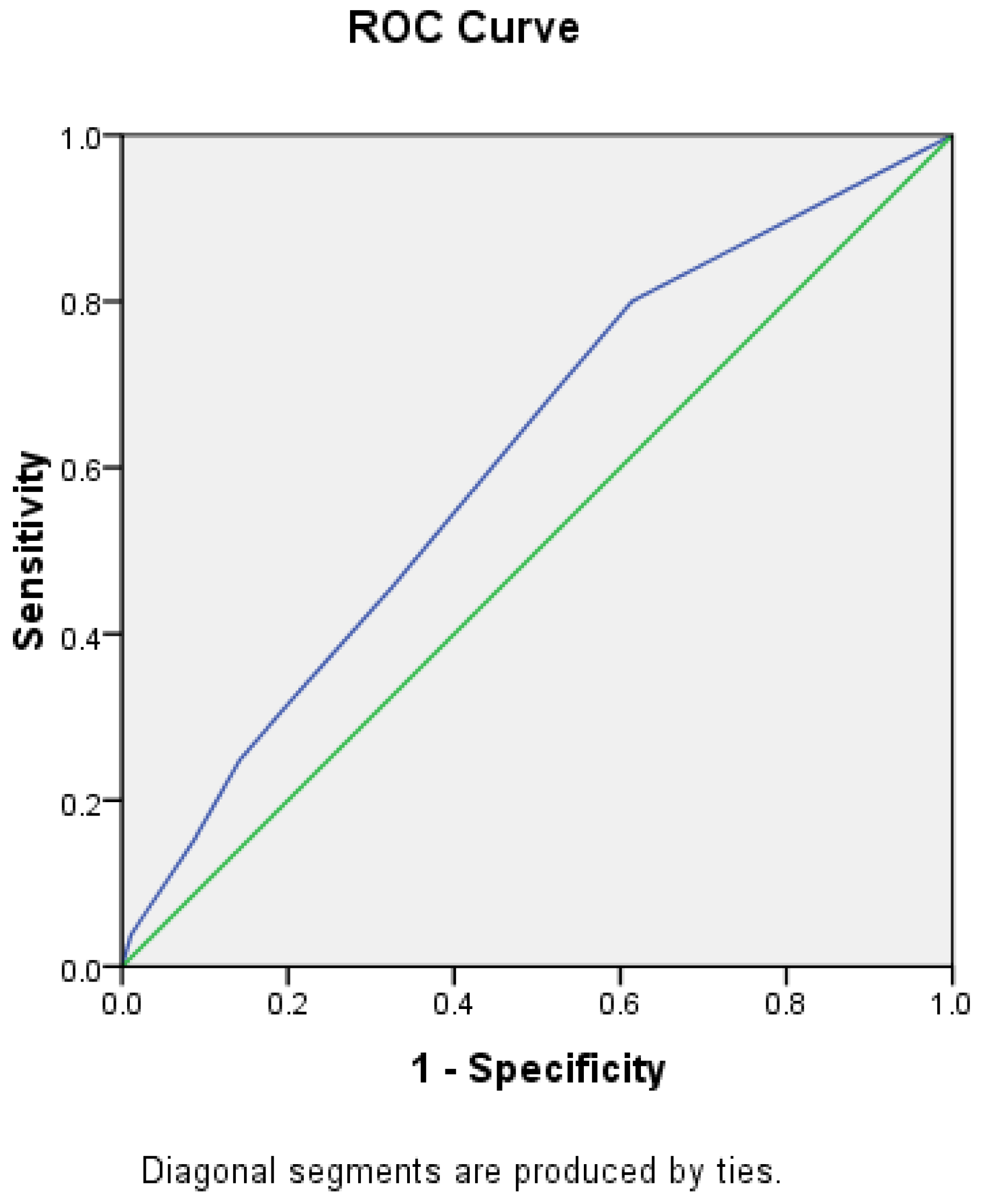
2.6. Statistical Analysis
3. Results
3.1. Univariable Associations
3.2. Multivariable Associations
+ (0.56 × Serum Sodium) + (0.51 × Serum Creatinine) + (0.56 × High Density Lipid)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hambleton, I.R.; Jonnalagadda, R.; Davis, C.R.; Fraser, H.S.; Chaturvedi, N.; Hennis, A.J. All-cause mortality after diabetes-related amputation in Barbados: A prospective case-control study. Diabetes Care 2009, 32, 306–307. [Google Scholar] [CrossRef] [Green Version]
- Boulton, A.J.; Vileikyte, L.; Ragnarson-Tennvall, G.; Apelqvist, J. The global burden of diabetic foot disease. Lancet 2005, 366, 1719–1724. [Google Scholar] [CrossRef]
- Armstrong, D.G.; Lavery, L.A. Negative pressure wound therapy after partial diabetic foot amputation: A multicentre, randomised controlled trial. Lancet 2005, 366, 1704–1710. [Google Scholar] [CrossRef]
- Schofield, C.J.; Libby, G.; Brennan, G.M.; MacAlpine, R.R.; Morris, A.D.; Leese, G.P. Mortality and hospitalization in patients after amputation: A comparison between patients with and without diabetes. Diabetes Care 2006, 29, 2252–2256. [Google Scholar] [CrossRef] [Green Version]
- Canavan, R.J.; Unwin, N.C.; Kelly, W.F.; Connolly, V.M. Diabetes- and nondiabetes-related lower extremity amputation incidence before and after the introduction of better organized diabetes foot care: Continuous longitudinal monitoring using a standard method. Diabetes Care 2008, 31, 459–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Amputee Statistical Database (NASDAB). National Amputee Statistical Database Annual Report 2005/2006. Edinburgh: NASDAB [Online]. 2006. Available online: http://www.nasdab.co.uk (accessed on 4 November 2017).
- Navarro-Flores, E.; Romero-Morales, C.; Becerro de Bengoa-Vallejo, R.; Rodríguez-Sanz, D.; Palomo-López, P.; López-López, D.; Losa-Iglesias, M.E.; Calvo-Lobo, C. Sex Differences in Frail Older Adults with Foot Pain in a Spanish Population: An Observational Study. Int. J. Environ. Res. Public Health 2020, 17, 6141. [Google Scholar] [CrossRef] [PubMed]
- UNIPOD. Limbless Statistics–Annual Report. University of Salford 2011/2012. Available online: https://shop.salford.ac.uk/product-catalogue/university-goods-and-services/limbless-statistics/limbless-statistics-annual-report-201112 (accessed on 20 June 2021).
- Nawijn, S.E.; van der Linde, H.; Emmelot, C.H.; Hofstad, C.J. Stump management after trans-tibial amputation: A systematic review. Prosthet. Orthot. Int. 2005, 29, 13–26. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Ros, P.; Navarro-Flores, E.; Julián-Rochina, I.; Martínez-Arnau, F.M.; Cauli, O. Changes in Salivary Amylase and Glucose in Diabetes: A Scoping Review. Diagnostics 2021, 11, 453. [Google Scholar] [CrossRef] [PubMed]
- Albino, F.P.; Seidel, R.; Brown, B.J.; Crone, C.G.; Attinger, C.E. Through knee amputation: Technique modifications and surgical outcomes. Arch. Plast. Surg. 2014, 41, 562–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, K.; Tang, T.; Wang, A.; Cui, S. Surgical revision for stump problems after traumatic above-ankle amputations of the lower extremity. BMC Musculoskelet. Disord. 2015, 16, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tisi, P.V.; Than, M.M. Type of incision for below knee amputation. Cochrane Database Syst. Rev. 2014, Cd003749. [Google Scholar] [CrossRef] [Green Version]
- Wong, C.K.; Edelstein, J.E. Unna and elastic postoperative dressings: Comparison of their effects on function of adults with amputation and vascular disease. Arch. Phys. Med. Rehabil. 2000, 81, 1191–1198. [Google Scholar] [CrossRef] [PubMed]
- Vergouwe, Y.; Steyerberg, E.W.; Eijkemans, M.J.; Habbema, J.D. Substantial effective sample sizes were required for external validation studies of predictive logistic regression models. J. Clin. Epidemiol. 2005, 58, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Dormandy, J.; Heeck, L.; Vig, S. Major amputations: Clinical patterns and predictors. Semin. Vasc. Surg. 1999, 12, 154–161. [Google Scholar] [PubMed]
- Steyerberg, E.W.; Vickers, A.J.; Cook, N.R.; Gerds, T.; Gonen, M.; Obuchowski, N.; Pencina, M.J.; Kattan, M.W. Assessing the performance of prediction models: A framework for traditional and novel measures. Epidemiology 2010, 21, 128–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.L.; Wang, M.; Liu, T.K. Predictors for wound healing in ischemic lower limb amputation. J. Formos. Med Assoc. 1994, 93, 849–854. [Google Scholar]
- Vanross, E.R.; Johnson, S.; Abbott, C.A. Effects of early mobilization on unhealed dysvascular transtibial amputation stumps: A clinical trial. Arch. Phys. Med. Rehabil. 2009, 90, 610–617. [Google Scholar] [CrossRef] [PubMed]
- Steen Jensen, J.; Mandrup-Poulsen, T. Success rate of prosthetic fitting after major amputations of the lower limb. Prosthet. Orthot. Int. 1983, 7, 119–121. [Google Scholar] [CrossRef] [Green Version]
- Christensen, S. Lower Extremity Amputations in the County of Aalborg 1961–1971: Population Study and Follow-Up. Acta Orthop. Scand. 1976, 47, 329–334. [Google Scholar] [CrossRef]
- Low, C.K.; Chew, W.Y.; Howe, T.S.; Tan, S.K. Factors affecting healing of below knee amputation. Singap. Med. J. 1996, 37, 392–393. [Google Scholar]
- Reiber, G.E.; Pecoraro, R.E.; Koepsell, T.D. Risk factors for amputation in patients with diabetes mellitus: A case-control study. Ann. Intern. Med. 1992, 117, 97–105. [Google Scholar] [CrossRef]
- Moss, S.E.; Klein, R.; Klein, B.E. The prevalence and incidence of lower extremity amputation in a diabetic population. Arch. Intern. Med. 1992, 152, 610–616. [Google Scholar] [CrossRef]
- Criado, E.; De Stefano, A.A.; Keagy, B.A.; Upchurch, G.R., Jr.; Johnson, G., Jr. The course of severe foot infection in patients with diabetes. Surg. Gynecol. Obstet. 1992, 175, 135–140. [Google Scholar] [PubMed]
- Apelqvist, J.; Agardh, C.D. The association between clinical risk factors and outcome of diabetic foot ulcers. Diabetes Res. Clin. Pract. 1992, 18, 43–53. [Google Scholar] [CrossRef]
- Yaghoubian, A.; de Virgilio, C.; Dauphine, C.; Lewis, R.J.; Lin, M. Use of admission serum lactate and sodium levels to predict mortality in necrotizing soft-tissue infections. Arch. Surg. 2007, 142, 840–846; discussion 844–846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nissen, S.J.; Newman, W.P. Factors influencing reintegration to normal living after amputation. Arch. Phys. Med. Rehabil. 1992, 73, 548–551. [Google Scholar]
- Chen, M.C.; Lee, S.S.; Hsieh, Y.L.; Wu, S.J.; Lai, C.S.; Lin, S.D. Influencing factors of outcome after lower-limb amputation: A five-year review in a plastic surgical department. Ann. Plast. Surg. 2008, 61, 314–318. [Google Scholar] [CrossRef]
- Sheahan, M.G.; Hamdan, A.D.; Veraldi, J.R.; McArthur, C.S.; Skillman, J.J.; Campbell, D.R.; Scovell, S.D.; LoGerfo, F.W.; Pomposelli, F.B., Jr. Lower extremity minor amputations: The roles of diabetes mellitus and timing of revascularization. J. Vasc. Surg. 2005, 42, 476–480. [Google Scholar] [CrossRef] [Green Version]
- Gaede, P.; Lund-Andersen, H.; Parving, H.H.; Pedersen, O. Effect of a multifactorial intervention on mortality in type 2 diabetes. N. Engl. J. Med. 2008, 358, 580–591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suckow, B.D.; Goodney, P.P.; Cambria, R.A.; Bertges, D.J.; Eldrup-Jorgensen, J.; Indes, J.E.; Schanzer, A.; Stone, D.H.; Kraiss, L.W.; Cronenwett, J.L. Predicting functional status following amputation after lower extremity bypass. Ann. Vasc. Surg. 2012, 26, 67–78. [Google Scholar] [CrossRef] [Green Version]
- Lazzarini, P.A.; O’Rourke, S.R.; Russell, A.W.; Clark, D.; Kuys, S.S. What are the key conditions associated with lower limb amputations in a major Australian teaching hospital? J. Foot Ankle Res. 2012, 5, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.S.; Lu, M.; Lee, V.S.; Russell, D.; Bahr, C.; Lee, E.T. Lower-extremity amputation. Incidence, risk factors, and mortality in the Oklahoma Indian Diabetes Study. Diabetes 1993, 42, 876–882. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, N.; Stevens, L.K.; Fuller, J.H.; Lee, E.T.; Lu, M. Risk factors, ethnic differences and mortality associated with lower-extremity gangrene and amputation in diabetes. The WHO Multinational Study of Vascular Disease in Diabetes. Diabetologia 2001, 44 (Suppl. 2), S65–S71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, R.; Armitage, J.; Parish, S.; Sleigh, P.; Peto, R. MRC/BHF Heart Protection Study of cholesterol-lowering with simvastatin in 5963 people with diabetes: A randomised placebo-controlled trial. Lancet 2003, 361, 2005–2016. [Google Scholar] [CrossRef]
- Rajamani, K.; Colman, P.G.; Li, L.P.; Best, J.D.; Voysey, M.; D’Emden, M.C.; Laakso, M.; Baker, J.R.; Keech, A.C. Effect of fenofibrate on amputation events in people with type 2 diabetes mellitus (FIELD study): A prespecified analysis of a randomised controlled trial. Lancet 2009, 373, 1780–1788. [Google Scholar] [CrossRef] [Green Version]
- Kern, E.F.O.; Maney, M.; Miller, D.R.; Tseng, C.-L.; Tiwari, A.; Rajan, M.; Aron, D.; Pogach, L. Failure of ICD-9-CM codes to identify patients with comorbid chronic kidney disease in diabetes. Health Serv. Res. 2006, 41, 564–580. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Clinical Characteristics | % StumpHealed | Total % | Crude OR (95% CI) | p-Value |
|---|---|---|---|---|
| Age | ||||
| ≤50 yrs | 76.9 | 4.3 | 2.01 (0.54–7.47) | 0.29 |
| >50 yrs. | 62.4 | 95.7 | ||
| Gender | ||||
| Male | 65.9 | 71.3 | 1.53 (0.97–2.49) | 0.10 * |
| Female | 55.8 | 28.7 | ||
| Type of Amputation | ||||
| AKA | 68.3 | 53.7 | 1.64 (1.02–2.63) | 0.04 * |
| BKA | 56.8 | 46.3 | ||
| Diabetes mellitus | ||||
| No | 64.2 | 54 | 0.89 (0.56–1.43) | 0.64 |
| Yes | 61.6 | 46 | ||
| Smoker | ||||
| No | 74.1 | 18.3 | 0.54 (0.28–1.05) | 0.19 * |
| Yes | 60.8 | 81.7 | ||
| HTN | ||||
| No | 82.4 | 5.7 | 0.35 (0.09–1.24) | 0.10 * |
| Yes | 61.8 | 94.3 | ||
| K+ (mmol/L) | ||||
| Abnormal | 64.6 | 16 | 0.92 (0.48–1.76) | 0.80 |
| Normal | 62.7 | 84 | ||
| Na+ (mmol/L) | ||||
| Abnormal | 54.3 | 10.7 | 1.71 (1.04–2.82) | 0.03 * |
| Normal | 67 | 89.3 | ||
| WCC | ||||
| Abnormal | 62.9 | 59.5 | 1.03 (0.639–1.665) | 0.901 |
| Normal | 63.6 | 40.5 | ||
| CRP | ||||
| ≤5 | 60 | 5.1 | 0.89 (0.31–2.57) | 0.83 |
| >5 | 62.8 | 94.9 | ||
| Creatinine (mmol/L) | ||||
| ≤120 | 65.5 | 77.3 | 1.59 (0.92–2.75) | 0.09 * |
| >120 | 54.4 | 22.7 | ||
| Urea (mmol/L) | ||||
| ≤6.6 | 62.3 | 58.3 | 0.93 (0.58–1.49) | 0.76 |
| >6.6 | 64 | 41.7 | ||
| PT (sec) | ||||
| ≤13.5 | 62.4 | 57.7 | 0.94 (0.59–1.52) | 0.81 |
| >13.5 | 63.8 | 42.3 | ||
| INR (ratio) | ||||
| ≤1.2 | 64.6 | 68.7 | 1.24 (0.79–2.04) | 0.41 |
| >1.2 | 59.6 | 31.3 | ||
| TC (mmol/L) | ||||
| ≤5 | 64.7 | 84.4 | 1.41 (0.74–2.66) | 0.29 |
| >5 | 56.5 | 15.6 | ||
| TG (mmol/L) | ||||
| ≤2.1 | 63.2 | 82.4 | 0.86 (0.45–1.62) | 0.64 |
| >2.1 | 66.7 | 17.6 | ||
| HDL(mmol/L) | ||||
| ≤1.1 | 68 | 61.6 | 1.62 (0.99–2.64) | 0.05 * |
| >1.1 | 56.8 | 38.4 |
| Predictors of Stump Healing | Test Statistics and Associated Degree of Freedom | Adjusted OR (95% CI) | p-Value |
|---|---|---|---|
| Serum Sodium (Normal) | χ2(1) = 3.89, p = 0.05 | 1.76 (0.31–0.87) | 0.03 |
| Serum Creatinine (Normal) | χ2(1) = 3.89, p = 0.05 | 1.66 (1.49–5.85) | 0.05 |
| Serum HDL (Normal) | χ2(1) = 3.89, p = 0.05 | 1.75 (2.22–11.31) | 0.03 |
| Model summary −2 log-likelihood | Cox and Snell R2 | Nagelkerke R2 | |
| 103.77 | 0.02 | 0.03 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ashraff, S.; Siddiqui, M.; Carline, T.; Rush, R.; Santos, D.; Raza, Z. Development of a Prognostic Model for Stump Healing in Major Lower Limb Amputation among the Diabetic Population. Diabetology 2021, 2, 130-140. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology2030012
Ashraff S, Siddiqui M, Carline T, Rush R, Santos D, Raza Z. Development of a Prognostic Model for Stump Healing in Major Lower Limb Amputation among the Diabetic Population. Diabetology. 2021; 2(3):130-140. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology2030012
Chicago/Turabian StyleAshraff, Suhel, Muhammad Siddiqui, Thomas Carline, Robert Rush, Derek Santos, and Zahid Raza. 2021. "Development of a Prognostic Model for Stump Healing in Major Lower Limb Amputation among the Diabetic Population" Diabetology 2, no. 3: 130-140. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology2030012