
Advanced Technology (Continuous Glucose Monitoring and Advanced Hybrid Closed-Loop Systems) in Diabetes from the Perspective of Gender Differences
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Closed-Loop Systems
3. CGM
4. Gender Differences in the Epidemiology of Type 1 Diabetes
5. Gender Differences and Acute Complications in Type 1 Diabetes
6. Gender Differences and Chronic Complications in Type 1 Diabetes
7. Gender Differences and Quality of Life in Type 1 Diabetes
8. Gender Differences and Advanced Technologies
9. Technologies and Pregnancy
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kovatchev, B. A Century of Diabetes Technology: Signals, Models, and Artificial Pancreas Control. Trends Endocrinol. Metab. 2019, 30, 432–444. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.J.; Jung, I.; Park, C.I. Current Advances of Artificial Pancreas Systems: A Comprehensive Review of the Clinical Evidence. Diabetes Metab J. 2021, 45, 813–839. [Google Scholar] [CrossRef] [PubMed]
- Ceriello, A. Variabilità Glicemica e Complicanze Diabetiche: Un aggiornamento. Media 2017, 17, 190–195. [Google Scholar]
- Battellino, T.; Danne, T.; Bergenstal, R.M.; Amiel, S.A.; Beck, R.; Biester, T.; Bosi, E.; Buckingham, B.A.; Cefalu, W.T.; Close, K.L.; et al. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Reccomandations from the International Consensus of Time in Range. Diabetes Care 2019, 42, 1593–1603. [Google Scholar] [CrossRef] [PubMed]
- Maiorino, M.I.; Signoriello, S.; Maio, A.; Chiodini, P.; Bellastella, G.; Scappaticcio, L.; Longo, M.; Giugliano, D.; Esposito, K. Effects of Continuous GlucoseMonitoring on Metrics of Glycemic Control in Diabetes: A Systematic Review With Meta-analysis of Randomized Controlled Trials. Diabetes Care 2020, 43, 1146–1156. [Google Scholar] [CrossRef] [PubMed]
- Knoll, C.; Peacock, S.; Wäldchen, M.; Cooper, D.; Aulakh, S.K.; Raile, K.; Hussain, S.; Braune, K. Real-world evidence on clinical outcomes of people with type 1 diabetes using open-source and commercial automated insulin dosing systems: A systematic review. Diabet. Med. 2021, 39, e14741. [Google Scholar] [CrossRef] [PubMed]
- Pinsker, P.E.; Müller, L.; Constantin, A.; Leas, S.; Manning, M.; McElwee Malloy, M.; Singh, H.; Habif, S. Real-World Patient-Reported Outcomes and Glycemic Results with Initiation of Control-IQ Technology. Diabetes Technol. Ther. 2021, 23, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Cyranka, K.; Matejko, B.; Juza, A.; Kieć-Wilk, B.; Krzyżowska, S.; Cohen, O.; Da Silva, J.; Lushchyk, M.; Malecki, M.T.; Klupa, T. Improvement of Selected Psychological Parameters and Quality of Life of Patients With Type 1 Diabetes Mellitus Undergoing Transition From Multiple Daily Injections and Self-Monitoring of Blood Glucose Directly to the MiniMed 780G Advanced Hybrid Closed-Loop System: Post hoc Analysis of a Randomized Control Study. JMIR Form. Res. 2023, 7, e43535. [Google Scholar] [PubMed]
- Carè, A.; Marconi, M.; Masella, R.; Ortona, E. Higher Institute of Health June 2021. Available online: https://www.epicentro.iss.it/medicina-di-genere (accessed on 4 October 2023).
- Tonolo, G. Sex-Gender Awareness in Diabetes. Diabetology 2021, 2, 117–122. [Google Scholar] [CrossRef]
- Russo, G.T.; Manicardi, V.; Rossi, M.C.; Orsi, E.; Solini, A. Review Sex- and gender-differences in chronic long-term complications of type 1 and type 2 diabetes mellitus in Italy Nutrition. Metab. Cardiovasc. Dis. 2022, 32, 2297–2309. [Google Scholar] [CrossRef] [PubMed]
- Castellano-Guerrero, A.M.; Guerrero, R.; Ruiz-Aranda, D.; Perea, S.; Pumar, A.; Relimpio, F.; Mangas, M.A.; Losada, F.; Martinez-Brocca, M.A. Gender differences in quality of life in adults with long-standing type 1 diabetes mellitus. Diabetol. Metab Syndr 2020, 12, 64. [Google Scholar] [CrossRef] [PubMed]
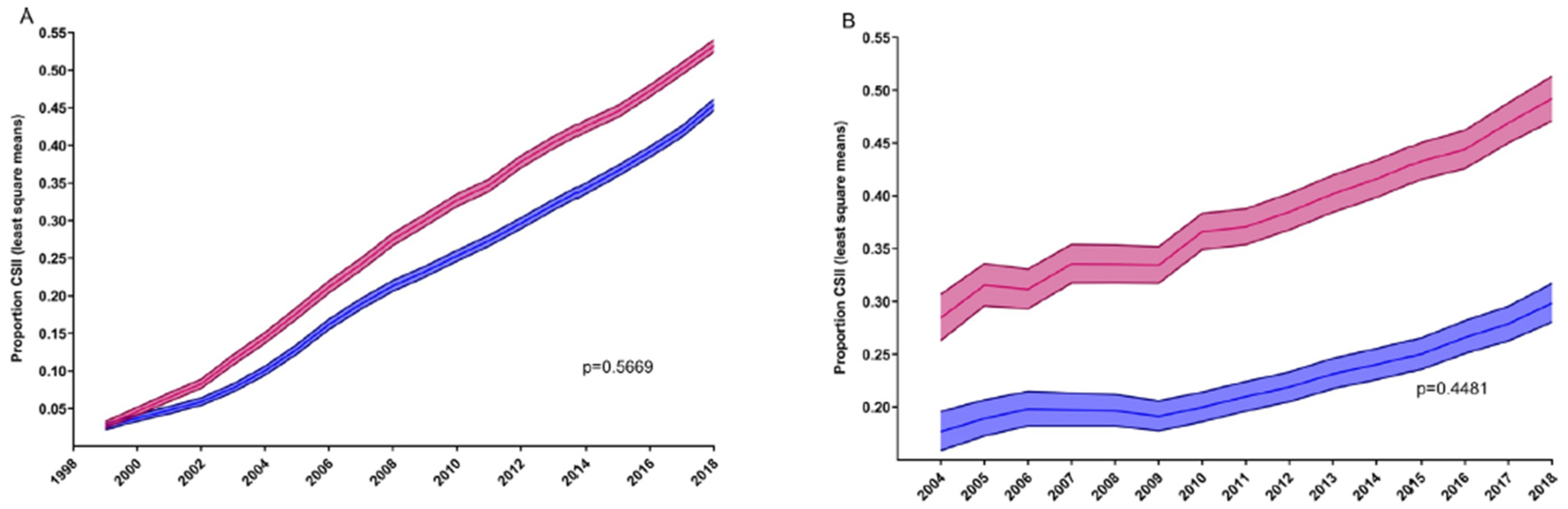
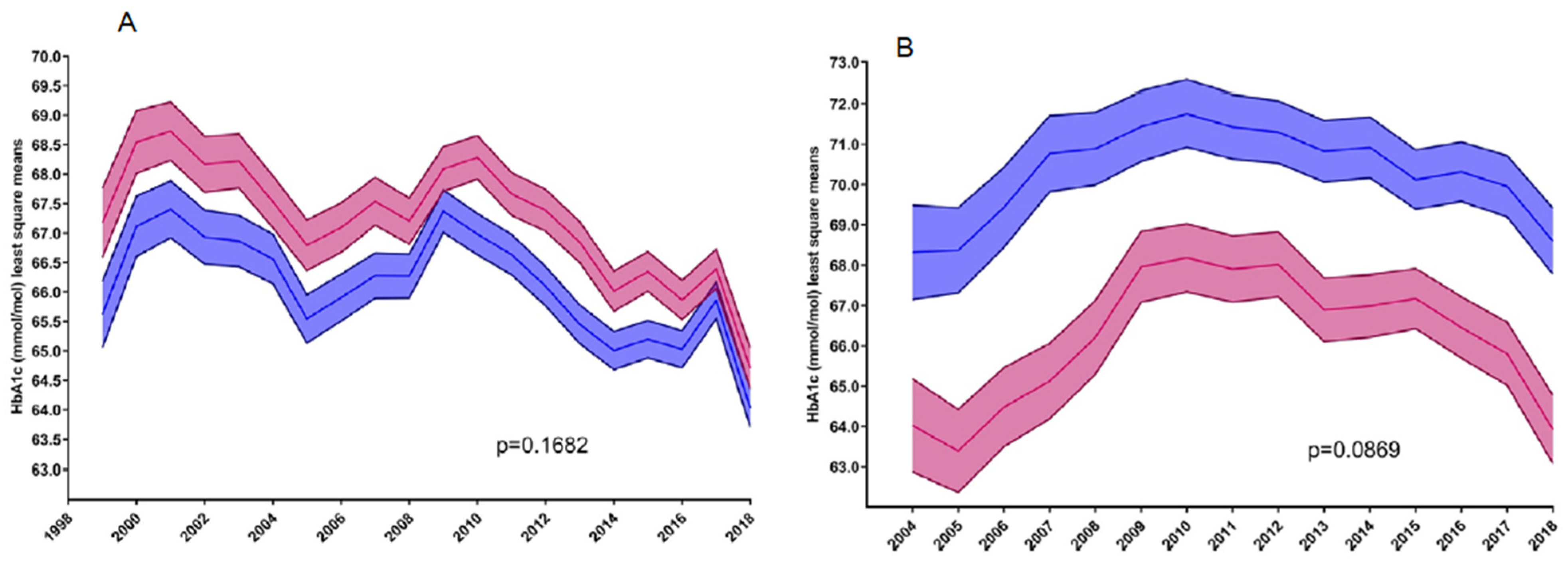
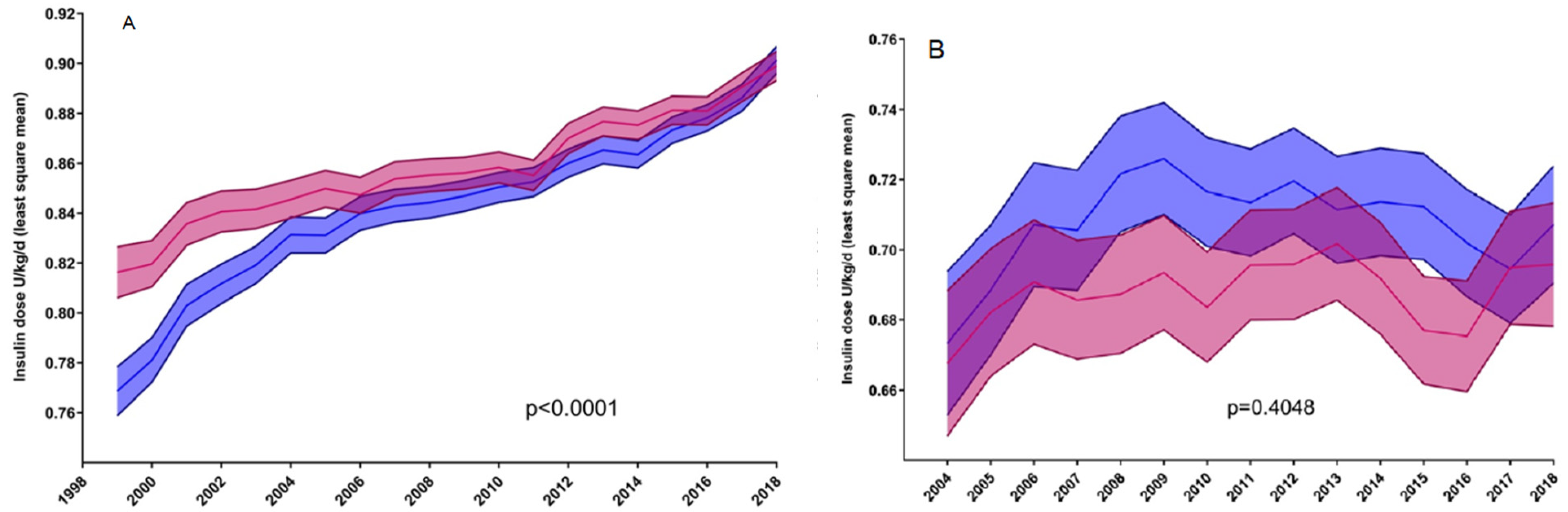
- Boettcher, C.; Tittel, S.R.; Meissner, T.; Gohlke, B.; Stachow, R.; Dost, A.; Wunderlich, S.; Lowak, I.; Lanzinger, S. Sex differences over time for glycemic control, pump use and insulin dose in patients aged 10–40 years with type 1 diabetes: A diabetes registry study. BMJ Open Diab. Res. Care 2021, 9, e002494. [Google Scholar] [CrossRef] [PubMed]
- Russo, G.; Rocca, A.; Manicardi, V. Annals AMD 2021. Available online: https://aemmedi.it/annali-amd (accessed on 4 October 2023).
- Bak, J.C.G.; Serné, E.H.; de Valk, H.W.; Valk, N.K.; Kramer, M.H.H.; Nieuwdorp, M.; Verheugt, C.L. Gender gaps in type 1 diabetes care. Acta Diabetol. 2022, 60, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Prevost, M.S.; Rabasa-Lhoret, R.; Talbo, M.K.; Yardley, J.E.; Curry, E.G.; Brazeau, A.S. Gender Differences in Strategies to Prevent Physical Activity–Related Hypoglycemia in Patients With Type 1 Diabetes: A BETTER Study. Diabetes Care 2022, 45, e51–e53. [Google Scholar] [CrossRef] [PubMed]
- Newman, C.; Ero, A.; Dunne, F.P. Glycaemic control and novel technology management strategies in pregestational diabetes mellitus. Front. Endocrinol. 2023, 13, 1109825. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nuzzo, M.G.; Schettino, M. Advanced Technology (Continuous Glucose Monitoring and Advanced Hybrid Closed-Loop Systems) in Diabetes from the Perspective of Gender Differences. Diabetology 2023, 4, 519-526. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology4040045
Nuzzo MG, Schettino M. Advanced Technology (Continuous Glucose Monitoring and Advanced Hybrid Closed-Loop Systems) in Diabetes from the Perspective of Gender Differences. Diabetology. 2023; 4(4):519-526. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology4040045
Chicago/Turabian StyleNuzzo, Maria Grazia, and Marciano Schettino. 2023. "Advanced Technology (Continuous Glucose Monitoring and Advanced Hybrid Closed-Loop Systems) in Diabetes from the Perspective of Gender Differences" Diabetology 4, no. 4: 519-526. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology4040045