
Sexual Dysfunction in Female Patients with Type 2 Diabetes Mellitus—Sneak Peek on an Important Quality of Life Determinant
 , and
, and 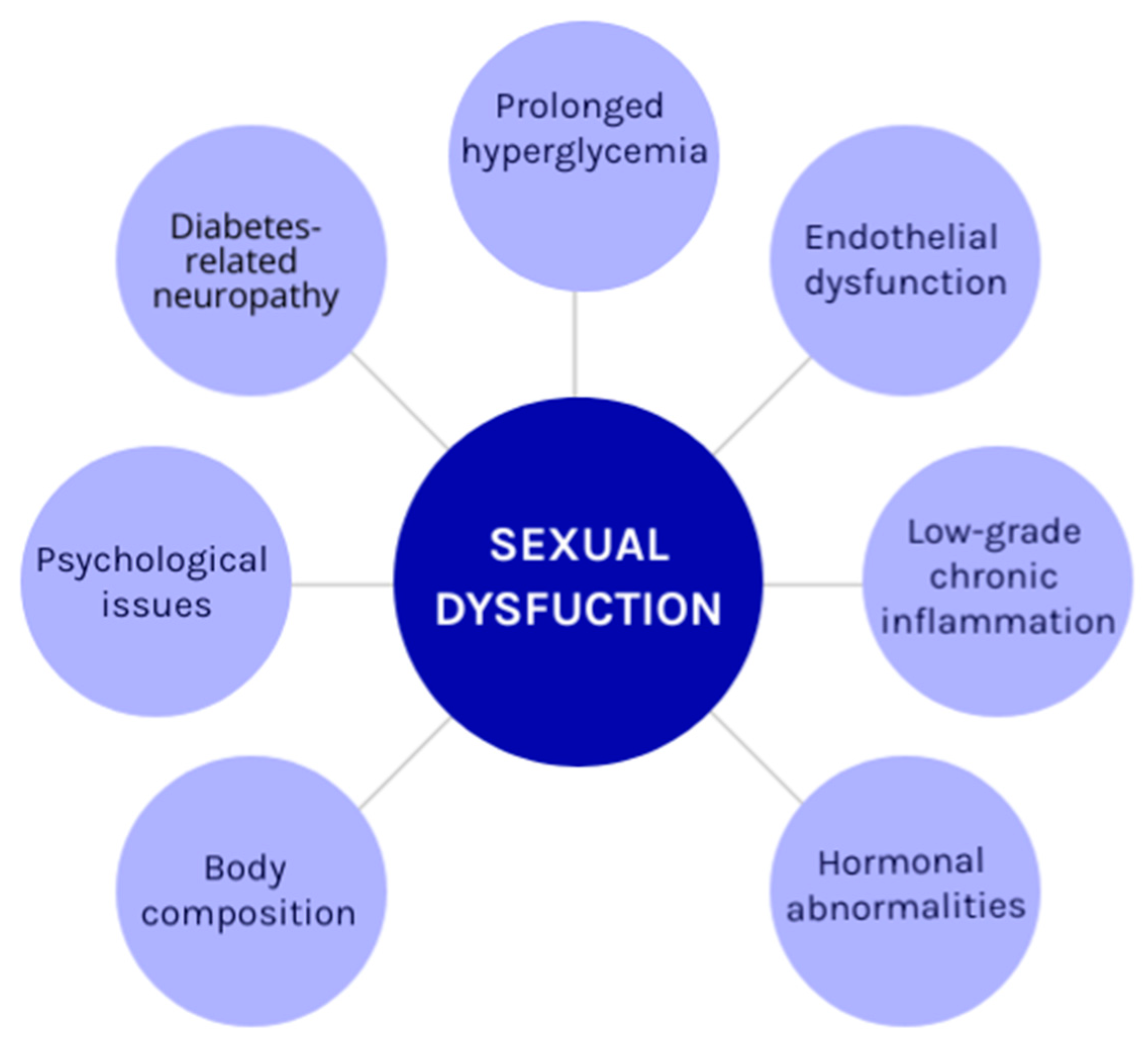{kind=link}
Abstract
:1. Introduction
2. Type 2 Diabetes Mellitus and Chronic Complications
3. Definition and Prevalence
4. Different Domains of Female Sexual Dysfunction
- Desire disorders include a persistent absence of sex-related physical desire, a lack of sexual engagement, or sexual thoughts or fantasies that cause problems to patients and their partners. There are two main desire disorders: hypoactive sexual desire disorder (HSDD) and sexual aversion disorder (SAD). The questionnaire that can be used for this type of disorder is the Sexual Function Questionnaire (SFQ-V1) [25,26].
- Arousal disorders are described as a lack of in sexual interest, interest in initiating sexual activity, pleasure, thoughts, and fantasies, including an absence of responsive desire and a lack of subjective arousal of a physical genital response to sexual stimulation: non-genital, genital, or both. The FSFI is the most used questionnaire for female arousal disorders [25,26].
- Orgasm disorders: Female orgasmic dysfunction is characterized by an orgasm that despite normal levels of subjective arousal, is absent, rare, noticeably lower in intensity, or noticeably delayed in response to stimulation. They can be primary when women have never been able to have an orgasm, and secondary when women are no longer able to experience orgasms, despite once being able to. The female Orgasm Scale is the scale used for diagnosing orgasm disorder in the female population [25,27].
- Involuntary contraction of the pelvic floor muscles when vaginal entry is attempted or completed, pain that is localized to the vestibule, at other vulvovaginal or pelvic locations, as well as fear or anxiety about penetration attempts are all symptoms of pain disorder. The Multidimensional Vaginal Penetration Disorder Questionnaire is used for determining sexual pain disorders [25,27].
5. The Effect of T2DM on Female Sexual Function
6. Sexual Disorders and Menopause
7. Sexual Dysfunction as Per Gender
8. Clinical Studies
9. Interventions and Management
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ong, K.L.; Stafford, L.K.; McLaughlin, S.A.; Boyko, E.J.; Vollset, S.E.; Smith, A.E.; Dalton, B.E.; Duprey, J.; Cruz, J.A.; Hagins, H.; et al. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: A systematic analysis for the Global Burden of Disease Study 2021. Lancet 2023, 402, 203–234. [Google Scholar] [CrossRef] [PubMed]
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Gaglia, J.L.; Hilliard, M.E.; Isaacs, D.; et al. 2 Classification and Diagnosis of Diabetes: Standards of Care in Diabetes—2023. Diabetes Care 2023, 46, S19–S40. [Google Scholar] [CrossRef] [PubMed]
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Gaglia, J.L.; Hilliard, M.E.; Isaacs, D.; et al. 3. Prevention or Delay of Type 2 Diabetes and Associated Comorbidities: Standards of Care in Diabetes—2023. Diabetes Care 2023, 46, S41–S48. [Google Scholar] [CrossRef] [PubMed]
- Gardner, D.G.; Shoback, D. Greenspan’ s Basic & Clinical Endocrinology, 10th ed.; McGraw-Hill Education: New York, NY, USA, 2018. [Google Scholar]
- Faselis, C.; Katsimardou, A.; Imprialos, K.; Deligkaris, P.; Kallistratos, M.; Dimitriadis, K. Microvascular Complications of Type 2 Diabetes Mellitus. Curr. Vasc. Pharmacol. 2019, 18, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Musicki, B.; Liu, T.; Lagoda, G.A.; Bivalacqua, T.J.; Strong, T.D.; Burnett, A.L. Endothelial Nitric Oxide Synthase Regulation in Female Genital Tract Structures. J. Sex. Med. 2009, 6, 247–253. [Google Scholar] [CrossRef]
- Parnan, A.; Tafazoli, M.; Azmoude, E. Sexual Function and Quality of Life in Diabetic Women Referring to Health Care Centers in Mashhad. J. Educ. Health Promot. 2017, 6, 25. [Google Scholar] [CrossRef]
- Maiorino, M.I.; Bellastella, G.; Esposito, K. Diabetes and Sexual Dysfunction: Current Perspectives. Diabetes Metab. Syndr. Obes. Targets Ther. 2014, 7, 95–105. [Google Scholar] [CrossRef]
- Muniyappa, R.; Norton, M.; Dunn, M.E.; Banerji, M.A. Diabetes and Female Sexual Dysfunction: Moving beyond “Benign Neglect”. Curr. Diabetes Rep. 2005, 5, 230–236. [Google Scholar] [CrossRef]
- Kizilay, F.; Gali, H.E.; Serefoglu, E.C. Diabetes and Sexuality. Sex. Med. Rev. 2017, 5, 45–51. [Google Scholar] [CrossRef]
- Vafaeimanesh, J.; Raei, M.; Hosseinzadeh, F.; Parham, M. Evaluation of Sexual Dysfunction in Women with Type 2 Diabetes. Indian J. Endocrinol. Metab. 2014, 18, 175–179. [Google Scholar] [CrossRef]
- Rahmanian, E.; Salari, N.; Mohammadi, M.; Jalali, R. Evaluation of Sexual Dysfunction and Female Sexual Dysfunction Indicators in Women with Type 2 Diabetes: A Systematic Review and Meta-Analysis. Diabetol. Metab. Syndr. 2019, 11, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Kautzky-Willer, A.; Harreiter, J.; Pacini, G. Sex and Gender Differences in Risk, Pathophysiology and Complications of Type 2 Diabetes Mellitus. Endocr. Rev. 2016, 37, 278–316. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.J.; O’connor, K.M. Female Sexual Dysfunction. Med. Clin. N. Am. 2015, 99, 607–628. [Google Scholar] [CrossRef] [PubMed]
- Shifren, J.L.; Monz, B.U.; Russo, P.A.; Segreti, A.; Johannes, C.B. Sexual Problems and Distress in United States Women: Prevalence and Correlates. Obstet. Gynecol. 2008, 112, 970–978. [Google Scholar] [CrossRef]
- Pontiroli, A.E.; Cortelazzi, D.; Morabito, A. Female Sexual Dysfunction and Diabetes: A Systematic Review and Meta-Analysis. J. Sex. Med. 2013, 10, 1044–1051. [Google Scholar] [CrossRef]
- Derosa, G.; Romano, D.; D’angelo, A.; Maffioli, P. Female Sexual Dysfunction in Subjects with Type 2 Diabetes Mellitus. Sex. Disabil. 2023, 41, 221–233. [Google Scholar] [CrossRef]
- Elnazer, H.Y.; Baldwin, D.S. Structured Review of the Use of the Arizona Sexual Experiences Scale in Clinical Settings. Hum. Psychopharmacol. Clin. Exp. 2020, 35, e2730. [Google Scholar] [CrossRef]
- Rummans, T.A.; Clark, M.M.; Sloan, J.A.; Frost, M.H.; Bostwick, J.M.; Atherton, P.J.; Johnson, M.E.; Gamble, G.; Richardson, J.; Brown, P.; et al. Impacting Quality of Life for Patients with Advanced Cancer with a Structured Multidis-Ciplinary Intervention: A Randomized Controlled Trial. J. Clin. Oncol. 2006, 24, 635–642. [Google Scholar] [CrossRef]
- Kamalifard, M.; Sattarzadeh, N.; Babapour, J.; Gholami, S. Personal and Social Predictors of Sexual Function of Women with Type Two Diabetes in Sanandaj. Crescent J. Med. Biol. Sci. 2019, 6, 196–200. [Google Scholar]
- McHorney, C.A.; Ware, J.E.J.; Raczek, A.E. The MOS 36-Item Short-Form Health Survey (SF-36): II. Psychometric and Clinical Tests of Validity. Med. Care 1993, 31, 247–263. [Google Scholar] [CrossRef]
- Symonds, T.; Boolell, M.; Quirk, F. Development of a Questionnaire on Sexual Quality of Life in Women. J. Sex Marital. Ther. 2005, 31, 385–397. [Google Scholar] [CrossRef] [PubMed]
- The Whoqol Group. World Health Organization Quality of Life Assessment (WHOQOL): Development and General Psychometric Properties. Soc. Sci. Med. 1998, 46, 1569–1585. [Google Scholar] [CrossRef] [PubMed]
- Bhugra, D.; Colombini, G. Sexual Dysfunction: Classification and Assessment. Adv. Psychiatr. Treat. 2013, 19, 48–55. [Google Scholar] [CrossRef]
- Montgomery, K.A. Sexual Desire Disorders. Psychiatry (Edgmont) 2008, 5, 50–55. [Google Scholar] [PubMed]
- Rosen, R.; Brown, C.; Heiman, J.B.; Leiblum, S.; Meston, C.; Shabsigh, R.; Ferguson, D.; D’Agostino, R., Jr. The Female Sexual Function Index (FSFI): A Multidimensional Self-Report Instrument for the Assessment of Female Sexual Function. J. Sex Marital Ther. 2000, 26, 191–208. [Google Scholar] [CrossRef] [PubMed]
- Grover, S.; Shouan, A. Assessment Scales for Sexual Disorders—A Review. J. Psychosexual Health 2020, 2, 121–138. [Google Scholar] [CrossRef]
- Giraldi, A.; Kristensen, E. Sexual Dysfunction in Women with Diabetes Mellitus. J. Sex Res. 2010, 47, 199–211. [Google Scholar] [CrossRef]
- Erol, B.; Tefekli, A.; Sanli, O.; Ziylan, O.; Armagan, A.; Kendirci, M.; Eryasar, D.; Kadioglu, A. Does Sexual Dysfunction Correlate with Deterioration of Somatic Sensory System in Diabetic Women? Int. J. Impot. Res. 2003, 15, 198–202. [Google Scholar] [CrossRef]
- Veronelli, A.; Mauri, C.; Zecchini, B.; Peca, M.G.; Turri, O.; Valitutti, M.T.; Dall’Asta, C.; Pontiroli, A.E. Sexual Dysfunction Is Frequent in Premenopausal Women with Diabetes, Obesity, and Hypothyroidism, and Correlates with Markers of Increased Cardiovascular Risk. A Preliminary Report. J. Sex. Med. 2009, 6, 1561–1568. [Google Scholar] [CrossRef]
- Erol, B.; Tefekli, A.; Ozbey, I.; Salman, F.; Dincag, N.; Kadioglu, A.; Tellaloglu, S. Sexual Dysfunction in Type II Diabetic Females: A Comparative Study. J. Sex Marital. Ther. 2002, 28 (Suppl. S1), 55–62. [Google Scholar] [CrossRef]
- Angulo, J.; Hannan, J.L. Cardiometabolic Diseases and Female Sexual Dysfunction: Animal Studies. J. Sex. Med. 2022, 19, 408–420. [Google Scholar] [CrossRef] [PubMed]
- Allahdadi, K.J.; Tostes, R.C.; Webb, R.C. Female Sexual Dysfunction: Therapeutic Options and Experimental Challenges. Cardiovasc. Hematol. Agents Med. Chem. 2009, 7, 260–269. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.G.; Lewis, M.N.; Wertz, M.C. Managing Menopausal Symptoms: Common Questions and Answers. American Family Physician 2023, 108, 28–39. [Google Scholar] [PubMed]
- Johnson, A.; Roberts, L.; Elkins, G. Complementary and Alternative Medicine for Menopause. J. Evid.-Based Integr. Med. 2019, 24, 2515690X19829380. [Google Scholar] [CrossRef]
- Esposito, K.; Maiorino, M.I.; Bellastella, G.; Giugliano, F.; Romano, M.; Giugliano, D. Determinants of Female Sexual Dysfunction in Type 2 Diabetes. Int. J. Impot. Res. 2010, 22, 179–184. [Google Scholar] [CrossRef]
- Baldassarre, M.; Alvisi, S.; Berra, M.; Martelli, V.; Farina, A.; Righi, A.; Meriggiola, M.C. Changes in Vaginal Physiology of Menopausal Women with Type 2 Diabetes. J. Sex. Med. 2015, 12, 1346–1355. [Google Scholar] [CrossRef]
- Kolodny, R.C. Sexual Dysfunction in Diabetic Females. Diabetes 1971, 20, 557–559. [Google Scholar] [CrossRef]
- Enzlin, P.; Mathieu, C.; Vanderschueren, D.; Demyttenaere, K. Diabetes Mellitus and Female Sexuality: A Review of 25 Years’ Research. Diabet. Med. 1998, 15, 809–815. [Google Scholar] [CrossRef]
- Shi, Y.F.; Shao, X.Y.; Lou, Q.Q.; Chen, Y.J.; Zhou, H.J.; Zou, J.Y. Study on Female Sexual Dysfunction in Type 2 Diabetic Chinese Women. Biomed. Environ. Sci. 2012, 25, 557–561. [Google Scholar] [CrossRef]
- Olarinoye, J.; Olarinoye, A. Determinants of Sexual Function among Women with Type 2 Diabetes in a Nigerian Population. J. Sex. Med. 2008, 5, 878–886. [Google Scholar] [CrossRef]
- Abu Ali, R.M.; Al Hajeri, R.M.; Khader, Y.S.; Shegem, N.S.; Ajlouni, K.M. Sexual Dysfunction in Jordanian Diabetic Women. Diabetes Care 2008, 31, 1580–1581. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, M.A.; Ahmed, Z.; Ahmed Khan, A. Psychological Impact on Sexual Health among Diabetic Patients: A Review. Int. J. Diabetes Res. 2012, 1, 28–31. [Google Scholar] [CrossRef]
- Kiadaliri, A.A.; Najafi, B.; Mirmalek-Sani, M. Quality of Life in People with Diabetes: A Systematic Review of Studies in Iran. J. Diabetes Metab. Disord. 2013, 12, 54. [Google Scholar] [CrossRef] [PubMed]
- Soltan, A.Z.H.; Ranjbar, H.; Kohan, M. The relationship between sexual function of diabetic omen with quality of life. J. Shahid Beheshtii Univ. Med. Sci. 2013, 23, 32–39. [Google Scholar]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rogoznica, M.; Perica, D.; Borovac, B.; Belančić, A.; Matovinović, M. Sexual Dysfunction in Female Patients with Type 2 Diabetes Mellitus—Sneak Peek on an Important Quality of Life Determinant. Diabetology 2023, 4, 527-536. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology4040046
Rogoznica M, Perica D, Borovac B, Belančić A, Matovinović M. Sexual Dysfunction in Female Patients with Type 2 Diabetes Mellitus—Sneak Peek on an Important Quality of Life Determinant. Diabetology. 2023; 4(4):527-536. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology4040046
Chicago/Turabian StyleRogoznica, Marija, Dražen Perica, Barbara Borovac, Andrej Belančić, and Martina Matovinović. 2023. "Sexual Dysfunction in Female Patients with Type 2 Diabetes Mellitus—Sneak Peek on an Important Quality of Life Determinant" Diabetology 4, no. 4: 527-536. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology4040046