
Importance of Dyslipidaemia Treatment in Individuals with Type 2 Diabetes Mellitus—A Narrative Review
 , , ,
, , ,
Abstract
:1. Introduction
2. Pathophysiology
3. Type 2 Diabetes Mellitus and Dyslipidemia Interconnection
4. Target Lipid Levels in Type 2 Diabetes Mellitus
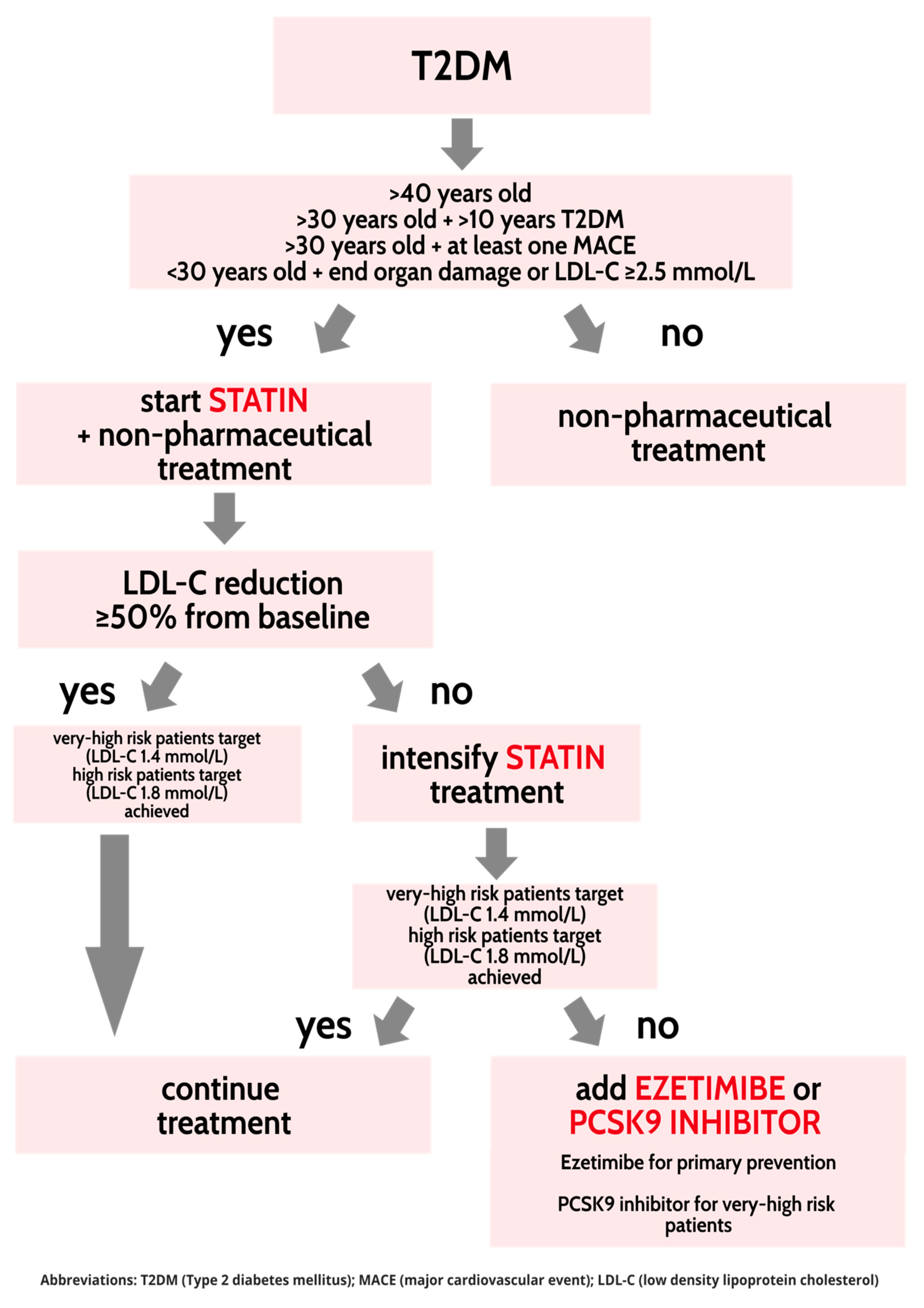
5. Treatment of Dyslipidaemia in Type 2 Diabetes Mellitus
5.1. Statins
5.2. Ezetimibe
5.3. PCSK9 Inhibitors
5.4. Fibrates
5.5. Omega-3 Fatty Acids
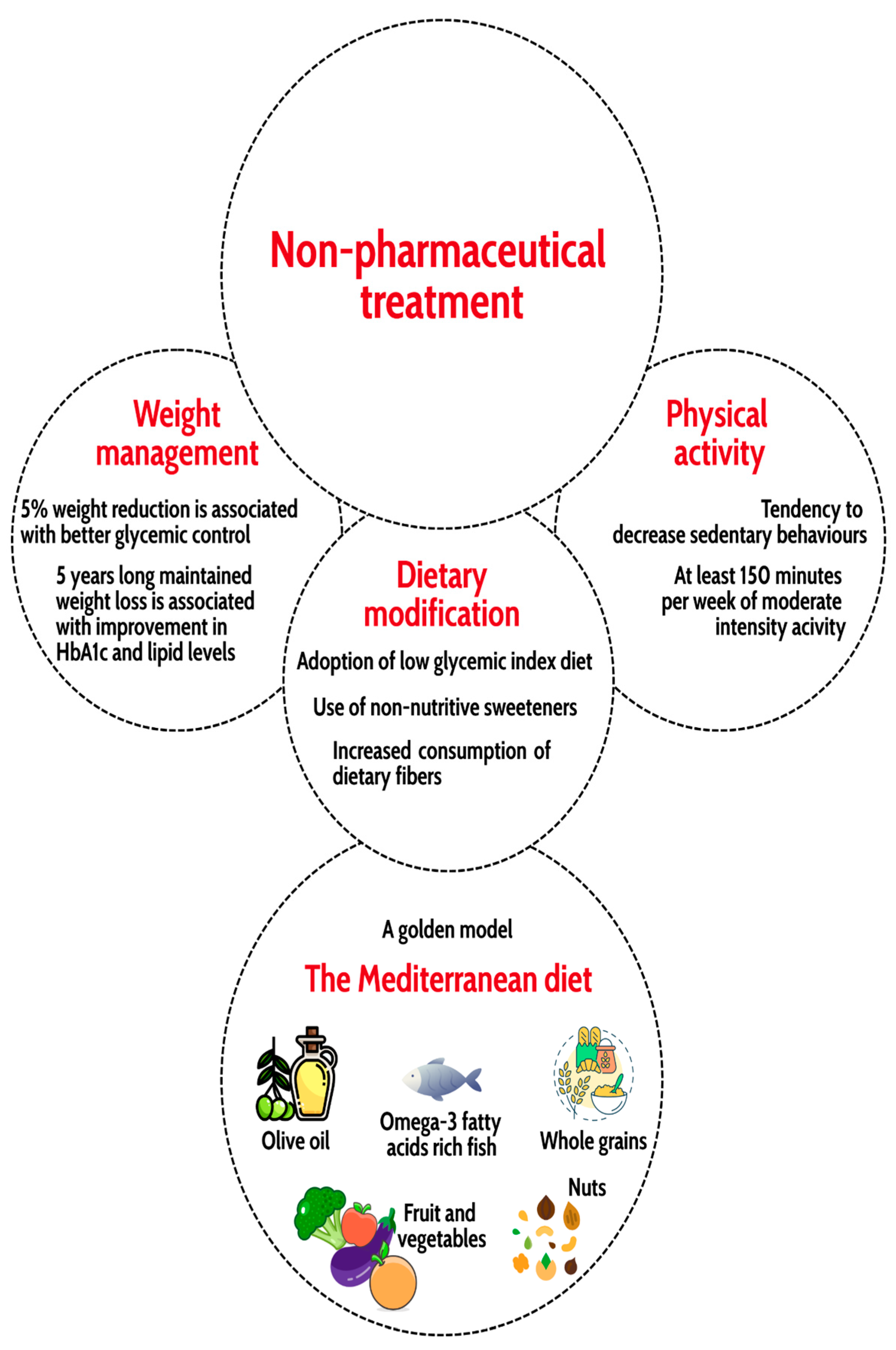
5.6. Non-Pharmaceutical Treatment
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Khan, M.A.B.; Hashim, M.J.; King, J.K.; Govender, R.D.; Mustafa, H.; Al Kaabi, J. Epidemiology of Type 2 Diabetes—Global Burden of Disease and Forecasted Trends. J. Epidemiol. Glob. Health 2019, 10, 107. [Google Scholar] [CrossRef] [PubMed]
- Andersson, E.; Persson, S.; Hallén, N.; Ericsson, Å.; Thielke, D.; Lindgren, P.; Steen Carlsson, K.; Jendle, J. Costs of diabetes complications: Hospital-based care and absence from work for 392,200 people with type 2 diabetes and matched control participants in Sweden. Diabetologia 2020, 63, 2582–2594. [Google Scholar] [CrossRef] [PubMed]
- Poznyak, A.; Grechko, A.V.; Poggio, P.; Myasoedova, V.A.; Alfieri, V.; Orekhov, A.N. The Diabetes Mellitus–Atherosclerosis Connection: The Role of Lipid and Glucose Metabolism and Chronic Inflammation. Int. J. Mol. Sci. 2020, 21, 1835. [Google Scholar] [CrossRef] [PubMed]
- Henning, R.J. Type-2 diabetes mellitus and cardiovascular disease. Future Cardiol. 2018, 14, 491–509. [Google Scholar] [CrossRef]
- Gardner, D.G.; Shoback, D. Greenspan’s Basic & Clinical Endocrinology, 10th ed.; McGrawHill: New York, NY, USA, 2018. [Google Scholar]
- Low Wang, C.C.; Hess, C.N.; Hiatt, W.R.; Goldfine, A.B. Clinical Update: Cardiovascular Disease in Diabetes Mellitus: Atherosclerotic Cardiovascular Disease and Heart Failure in Type 2 Diabetes Mellitus—Mechanisms, Management, and Clinical Considerations. Circulation 2016, 133, 2459–2502. [Google Scholar] [CrossRef]
- Faselis, C.; Katsimardou, A.; Imprialos, K.; Deligkaris, P.; Kallistratos, M.; Dimitriadis, K. Microvascular Complications of Type 2 Diabetes Mellitus. Curr. Vasc. Pharmacol. 2019, 18, 117–124. [Google Scholar] [CrossRef]
- Kaur, R.; Kaur, M.; Singh, J. Endothelial dysfunction and platelet hyperactivity in type 2 diabetes mellitus: Molecular insights and therapeutic strategies. Cardiovasc. Diabetol. 2018, 17, 121. [Google Scholar] [CrossRef]
- Vergès, B. Pathophysiology of diabetic dyslipidaemia: Where are we? Diabetologia 2015, 58, 886–899. [Google Scholar] [CrossRef]
- Wang, J.; Stančáková, A.; Soininen, P.; Kangas, A.J.; Paananen, J.; Kuusisto, J.; Ala-Korpela, M.; Laakso, M. Lipoprotein Subclass Profiles in Individuals with Varying Degrees of Glucose Tolerance: A Population-Based Study of 9399 Finnish Men: Lipids and Glucose Tolerance. J. Intern. Med. 2012, 272, 562–572. [Google Scholar] [CrossRef]
- Nogueira, J.P.; Maraninchi, M.; Béliard, S.; Padilla, N.; Duvillard, L.; Mancini, J.; Nicolay, A.; Xiao, C.; Vialettes, B.; Lewis, G.F.; et al. Absence of acute inhibitory effect of insulin on chylomicron production in type 2 diabetes. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 1039–1044. [Google Scholar] [CrossRef]
- Vergès, B. Intestinal lipid absorption and transport in type 2 diabetes. Diabetologia 2022, 65, 1587–1600. [Google Scholar] [CrossRef] [PubMed]
- Taskinen, M.-R.; Nikkilä, E.A.; Kuusi, T.; Harno, K. Lipoprotein Lipase Activity and Serum Lipoproteins in Untreated Type 2 (Insulin-Independent) Diabetes Associated with Obesity. Diabetologia 1982, 22, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Adiels, M.; Taskinen, M.-R.; Packard, C.; Caslake, M.J.; Soro-Paavonen, A.; Westerbacka, J.; Vehkavaara, S.; Häkkinen, A.; Olofsson, S.-O.; Yki-Järvinen, H.; et al. Overproduction of Large VLDL Particles Is Driven by Increased Liver Fat Content in Man. Diabetologia 2006, 49, 755–765. [Google Scholar] [CrossRef] [PubMed]
- Makita, T.; Tanaka, A.; Nakano, T.; Nakajima, K.; Numano, F. Importance of Glycation in the Acceleration of Low Density Lipoprotein (LDL) Uptake into Macrophages in Patients with Diabetes Mellitus. Int. Angiol. J. Int. Union Angiol. 1999, 18, 149–153. [Google Scholar]
- Duvillard, L.; Pont, F.; Florentin, E.; Gambert, P.; Vergès, B. Inefficiency of Insulin Therapy to Correct Apolipoprotein A-I Metabolic Abnormalities in Non-Insulin-Dependent Diabetes Mellitus. Atherosclerosis 2000, 152, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Fisher, R. American Diabetes Association Releases 2023 Standards of Care in Diabetes to Guide Prevention, Diagnosis, and Treatment for People Living with Diabetes. Diabetes Care 2023, 46, 1715. [Google Scholar] [CrossRef]
- Solano, M.P.; Goldberg, R.B. Lipid Management in Type 2 Diabetes. Clin. Diabetes 2006, 24, 27–33. [Google Scholar] [CrossRef]
- Mach, F.; Baigent, C.; Catapano, A.L.; Koskinas, K.C.; Casula, M.; Badimon, L.; Chapman, M.J.; De Backer, G.G.; Delgado, V.; Ference, B.A.; et al. 2019 ESC/EAS Guidelines for the Management of Dyslipidaemias: Lipid Modification to Reduce Cardiovascular Risk. Eur. Heart J. 2020, 41, 111–188. [Google Scholar] [CrossRef]
- Mancini, G.B.J.; Hegele, R.A.; Leiter, L.A. Dyslipidemia. Can. J. Diabetes 2018, 42, S178–S185. [Google Scholar] [CrossRef]
- Cholesterol Treatment Trialists’ (CTT) Collaborators. Efficacy of Cholesterol-Lowering Therapy in 18 686 People with Diabetes in 14 Randomised Trials of Statins: A Meta-Analysis. Lancet 2008, 371, 117–125. [Google Scholar] [CrossRef]
- Colhoun, H.M.; Betteridge, D.J.; Durrington, P.N.; Hitman, G.A.; Neil, H.A.W.; Livingstone, S.J.; Thomason, M.J.; Mackness, M.I.; Charlton-Menys, V.; Fuller, J.H. Primary Prevention of Cardiovascular Disease with Atorvastatin in Type 2 Diabetes in the Collaborative Atorvastatin Diabetes Study (CARDS): Multicentre Randomised Placebo-Controlled Trial. Lancet 2004, 364, 685–696. [Google Scholar] [CrossRef] [PubMed]
- Knopp, R.H.; d’Emden, M.; Smilde, J.G.; Pocock, S.J.; on behalf of the ASPEN Study Group. Efficacy and Safety of Atorvastatin in the Prevention of Cardiovascular End Points in Subjects with Type 2 Diabetes. Diabetes Care 2006, 29, 1478–1485. [Google Scholar] [CrossRef] [PubMed]
- Ganda, O.P. Statin-Induced Diabetes: Incidence, Mechanisms, and Implications. F1000Research 2016, 5, 1499. [Google Scholar] [CrossRef] [PubMed]
- Galicia-Garcia, U.; Jebari, S.; Larrea-Sebal, A.; Uribe, K.B.; Siddiqi, H.; Ostolaza, H.; Benito-Vicente, A.; Martín, C. Statin Treatment-Induced Development of Type 2 Diabetes: From Clinical Evidence to Mechanistic Insights. Int. J. Mol. Sci. 2020, 21, 4725. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, F.; Lamendola, C.; Harris, C.S.; Harris, V.; Tsai, M.-S.; Tripathi, P.; Abbas, F.; Reaven, G.M.; Reaven, P.D.; Snyder, M.P.; et al. Statins Are Associated with Increased Insulin Resistance and Secretion. Arterioscler. Thromb. Vasc. Biol. 2021, 41, 2786–2797. [Google Scholar] [CrossRef] [PubMed]
- Davis, T.M.E.; Badshah, I.; Chubb, S.A.P.; Davis, W.A. Dose-Response Relationship between Statin Therapy and Glycaemia in Community-Based Patients with Type 2 Diabetes: The Fremantle Diabetes Study. Diabetes Obes. Metab. 2016, 18, 1143–1146. [Google Scholar] [CrossRef]
- Merćep, I.; Strikić, D.; Slišković, A.M.; Reiner, Ž. New Therapeutic Approaches in Treatment of Dyslipidaemia—A Narrative Review. Pharmaceuticals 2022, 15, 839. [Google Scholar] [CrossRef]
- Castellano, J.M.; Pocock, S.J.; Bhatt, D.L.; Quesada, A.J.; Owen, R.; Fernandez-Ortiz, A.; Sanchez, P.L.; Ortuño, F.M.; Rodriguez, J.M.V.; Domingo-Fernández, A.; et al. Polypill Strategy in Secondary Cardiovascular Prevention. N. Engl. J. Med. 2022, 387, 967–977. [Google Scholar] [CrossRef]
- Pandor, A.; Ara, R.M.; Tumur, I.; Wilkinson, A.J.; Paisley, S.; Duenas, A.; Durrington, P.N.; Chilcott, J. Ezetimibe Monotherapy for Cholesterol Lowering in 2722 People: Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Intern. Med. 2009, 265, 568–580. [Google Scholar] [CrossRef]
- Cannon, C.P.; Blazing, M.A.; Giugliano, R.P.; McCagg, A.; White, J.A.; Theroux, P.; Darius, H.; Lewis, B.S.; Ophuis, T.O.; Jukema, J.W.; et al. Ezetimibe Added to Statin Therapy after Acute Coronary Syndromes. N. Engl. J. Med. 2015, 372, 2387–2397. [Google Scholar] [CrossRef]
- Giugliano, R.P.; Cannon, C.P.; Blazing, M.A.; Nicolau, J.C.; Corbalán, R.; Špinar, J.; Park, J.-G.; White, J.A.; Bohula, E.A.; Braunwald, E. Benefit of Adding Ezetimibe to Statin Therapy on Cardiovascular Outcomes and Safety in Patients with Versus without Diabetes Mellitus: Results from IMPROVE-IT (Improved Reduction of Outcomes: Vytorin Efficacy International Trial). Circulation 2018, 137, 1571–1582. [Google Scholar] [CrossRef] [PubMed]
- Kosoglou, T.; Statkevich, P.; Johnson-Levonas, A.O.; Paolini, J.F.; Bergman, A.J.; Alton, K.B. Ezetimibe: A Review of Its Metabolism, Pharmacokinetics and Drug Interactions. Clin. Pharmacokinet. 2005, 44, 467–494. [Google Scholar] [CrossRef] [PubMed]
- Sabatine, M.S.; Giugliano, R.P.; Keech, A.C.; Honarpour, N.; Wiviott, S.D.; Murphy, S.A.; Kuder, J.F.; Wang, H.; Liu, T.; Wasserman, S.M.; et al. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N. Engl. J. Med. 2017, 376, 1713–1722. [Google Scholar] [CrossRef] [PubMed]
- Ray, K.K.; Colhoun, H.M.; Szarek, M.; Baccara-Dinet, M.; Bhatt, D.L.; Bittner, V.A.; Budaj, A.J.; Diaz, R.; Goodman, S.G.; Hanotin, C.; et al. Effects of Alirocumab on Cardiovascular and Metabolic Outcomes after Acute Coronary Syndrome in Patients with or without Diabetes: A Prespecified Analysis of the ODYSSEY OUTCOMES Randomised Controlled Trial. Lancet Diabetes Endocrinol. 2019, 7, 618–628. [Google Scholar] [CrossRef] [PubMed]
- Rana, K.; Reid, J.; Rosenwasser, J.N.; Lewis, T.; Sheikh-Ali, M.; Choksi, R.R.; Goldfaden, R.F. A Spotlight on Alirocumab in High Cardiovascular Risk Patients with Type 2 Diabetes and Mixed Dyslipidemia: A Review on the Emerging Data. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 1897–1911. [Google Scholar] [CrossRef] [PubMed]
- Carugo, S.; Sirtori, C.R.; Corsini, A.; Tokgozoglu, L.; Ruscica, M. PCSK9 Inhibition and Risk of Diabetes: Should We Worry? Curr. Atheroscler. Rep. 2022, 24, 995–1004. [Google Scholar] [CrossRef] [PubMed]
- Memon, R.; Malek, R.; Munir, K.M. Doubling of Hemoglobin A1c on PCSK9 Inhibitor Therapy. Am. J. Med. 2019, 132, e17–e18. [Google Scholar] [CrossRef]
- Civeira, F.; Pedro-Botet, J. Cost-Effectiveness Evaluation of the Use of PCSK9 Inhibitors. Endocrinol. Diabetes Nutr. Engl. Ed. 2021, 68, 369–371. [Google Scholar] [CrossRef]
- Staels, B.; Dallongeville, J.; Auwerx, J.; Schoonjans, K.; Leitersdorf, E.; Fruchart, J.-C. Mechanism of Action of Fibrates on Lipid and Lipoprotein Metabolism. Circulation 1998, 98, 2088–2093. [Google Scholar] [CrossRef]
- FIELD Study Investigators. Effects of Long-Term Fenofibrate Therapy on Cardiovascular Events in 9795 People with Type 2 Diabetes Mellitus (the FIELD Study): Randomised Controlled Trial. Lancet 2005, 366, 1849–1861. [Google Scholar] [CrossRef]
- The ACCORD Study Group. Effects of Combination Lipid Therapy in Type 2 Diabetes Mellitus. N. Engl. J. Med. 2010, 362, 1563–1574. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.C. The Role of Dietary N-6 Fatty Acids in the Prevention of Cardiovascular Disease. J. Cardiovasc. Med. 2007, 8 (Suppl. S1), S42–S45. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, M.; Origasa, H.; Matsuzaki, M.; Matsuzawa, Y.; Saito, Y.; Ishikawa, Y.; Oikawa, S.; Sasaki, J.; Hishida, H.; Itakura, H.; et al. Effects of Eicosapentaenoic Acid on Major Coronary Events in Hypercholesterolaemic Patients (JELIS): A Randomised Open-Label, Blinded Endpoint Analysis. Lancet 2007, 369, 1090–1098. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, D.L.; Steg, P.G.; Miller, M.; Brinton, E.A.; Jacobson, T.A.; Ketchum, S.B.; Doyle, R.T., Jr.; Juliano, R.A.; Jiao, L.; Granowitz, C.; et al. Cardiovascular Risk Reduction with Icosapent Ethyl for Hypertriglyceridemia. N. Engl. J. Med. 2019, 380, 11–22. [Google Scholar] [CrossRef] [PubMed]
- ASCEND Study Collaborative Group; Bowman, L.; Mafham, M.; Wallendszus, K.; Stevens, W.; Buck, G.; Barton, J.; Murphy, K.; Aung, T.; Haynes, R.; et al. Effects of Aspirin for Primary Prevention in Persons with Diabetes Mellitus. N. Engl. J. Med. 2018, 379, 1529–1539. [Google Scholar]
- Backes, J.; Anzalone, D.; Hilleman, D.; Catini, J. The Clinical Relevance of Omega-3 Fatty Acids in the Management of Hypertriglyceridemia. Lipids Health Dis. 2016, 15, 118. [Google Scholar] [CrossRef]
- Gonzalez, J.S.; Tanenbaum, M.L.; Commissariat, P.V. Psychosocial Factors in Medication Adherence and Diabetes Self-Management: Implications for Research and Practice. Am. Psychol. 2016, 71, 539–551. [Google Scholar] [CrossRef]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease. J. Am. Coll. Cardiol. 2019, 74, e177–e232. [Google Scholar] [CrossRef]
- Löfvenborg, J.E.; Andersson, T.; Carlsson, P.-O.; Dorkhan, M.; Groop, L.; Martinell, M.; Tuomi, T.; Wolk, A.; Carlsson, S. Sweetened Beverage Intake and Risk of Latent Autoimmune Diabetes in Adults (LADA) and Type 2 Diabetes. Eur. J. Endocrinol. 2016, 175, 605–614. [Google Scholar] [CrossRef]
- Boule, N.G.; Haddad, E.; Kenny, G.P.; Wells, G.A.; Sigal, R.J. Effects of Exercise on Glycemic Control and Body Mass in Type 2 Diabetes Mellitus: A Meta-Analysis of Controlled Clinical Trials: Sports Medicine Update. Scand. J. Med. Sci. Sports 2002, 12, 60–61. [Google Scholar] [CrossRef]
- Couillard, C.; Després, J.-P.; Lamarche, B.; Bergeron, J.; Gagnon, J.; Leon, A.S.; Rao, D.C.; Skinner, J.S.; Wilmore, J.H.; Bouchard, C. Effects of Endurance Exercise Training on Plasma HDL Cholesterol Levels Depend on Levels of Triglycerides: Evidence From Men of the Health, Risk Factors, Exercise Training and Genetics (HERITAGE) Family Study. Arterioscler. Thromb. Vasc. Biol. 2001, 21, 1226–1232. [Google Scholar] [CrossRef] [PubMed]
- Kraus, W.E.; Houmard, J.A.; Duscha, B.D.; Knetzger, K.J.; Wharton, M.B.; McCartney, J.S.; Bales, C.W.; Henes, S.; Samsa, G.P.; Otvos, J.D.; et al. Effects of the Amount and Intensity of Exercise on Plasma Lipoproteins. N. Engl. J. Med. 2002, 347, 1483–1492. [Google Scholar] [CrossRef] [PubMed]
- Sarzynski, M.A.; Ruiz-Ramie, J.J.; Barber, J.L.; Slentz, C.A.; Apolzan, J.W.; McGarrah, R.W.; Harris, M.N.; Church, T.S.; Borja, M.S.; He, Y.; et al. Effects of Increasing Exercise Intensity and Dose on Multiple Measures of HDL (High-Density Lipoprotein) Function. Arterioscler. Thromb. Vasc. Biol. 2018, 38, 943–952. [Google Scholar] [CrossRef] [PubMed]
- Roberts, C.K.; Ng, C.; Hama, S.; Eliseo, A.J.; Barnard, R.J. Effect of a Short-Term Diet and Exercise Intervention on Inflammatory/Anti-Inflammatory Properties of HDL in Overweight/Obese Men with Cardiovascular Risk Factors. J. Appl. Physiol. 2006, 101, 1727–1732. [Google Scholar] [CrossRef]
- Zhou, C.; Wang, M.; Liang, J.; He, G.; Chen, N. Ketogenic Diet Benefits to Weight Loss, Glycemic Control, and Lipid Profiles in Overweight Patients with Type 2 Diabetes Mellitus: A Meta-Analysis of Randomized Controlled Trails. Int. J. Environ. Res. Public. Health 2022, 19, 10429. [Google Scholar] [CrossRef]
- Leow, Z.Z.X.; Guelfi, K.J.; Davis, E.A.; Jones, T.W.; Fournier, P.A. The Glycaemic Benefits of a Very-Low-Carbohydrate Ketogenic Diet in Adults with Type 1 Diabetes Mellitus May Be Opposed by Increased Hypoglycaemia Risk and Dyslipidaemia. Diabet. Med. 2018, 35, 1258–1263. [Google Scholar] [CrossRef]
- Elhayany, A.; Lustman, A.; Abel, R.; Attal-Singer, J.; Vinker, S. A Low Carbohydrate Mediterranean Diet Improves Cardiovascular Risk Factors and Diabetes Control among Overweight Patients with Type 2 Diabetes Mellitus: A 1-Year Prospective Randomized Intervention Study. Diabetes Obes. Metab. 2010, 12, 204–209. [Google Scholar] [CrossRef]
- Mazzocchi, A.; Leone, L.; Agostoni, C.; Pali-Schöll, I. The Secrets of the Mediterranean Diet. Does [Only] Olive Oil Matter? Nutrients 2019, 11, 2941. [Google Scholar] [CrossRef]
- Covas, M.-I.; Nyyssönen, K.; Poulsen, H.E.; Kaikkonen, J.; Zunft, H.-J.F.; Kiesewetter, H.; Gaddi, A.; de la Torre, R.; Mursu, J.; Bäumler, H.; et al. The Effect of Polyphenols in Olive Oil on Heart Disease Risk Factors. Ann. Intern. Med. 2006, 145, 333–341. [Google Scholar] [CrossRef]
- Torres-Peña, J.D.; Garcia-Rios, A.; Delgado-Casado, N.; Gomez-Luna, P.; Alcala-Diaz, J.F.; Yubero-Serrano, E.M.; Gomez-Delgado, F.; Leon-Acuña, A.; Lopez-Moreno, J.; Camargo, A.; et al. Mediterranean Diet Improves Endothelial Function in Patients with Diabetes and Prediabetes: A Report from the CORDIOPREV Study. Atherosclerosis 2018, 269, 50–56. [Google Scholar] [CrossRef]
- Companys, J.; Pla-Pagà, L.; Calderón-Pérez, L.; Llauradó, E.; Solà, R.; Pedret, A.; Valls, R.M. Fermented Dairy Products, Probiotic Supplementation, and Cardiometabolic Diseases: A Systematic Review and Meta-analysis. Adv. Nutr. 2020, 11, 834–863. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.A.; Kim, J. Effect of Probiotics on Blood Lipid Concentrations: A Meta-Analysis of Randomized Controlled Trials. Medicine 2015, 94, e1714. [Google Scholar] [CrossRef] [PubMed]
- Moroti, C.; Souza Magri, L.F.; de Rezende Costa, M.; Cavallini, D.C.; Sivieri, K. Effect of the consumption of a new symbiotic shake on glycemia and cholesterol levels in elderly people with type 2 diabetes mellitus. Lipids Health Dis. 2012, 11, 29. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Shang, J.; Zhou, Y.; Liu, W.; Tian, Y.; Shang, H. Effects of probiotics on nonalcoholic fatty liver disease: A systematic review and meta-analysis. Expert. Rev. Gastroenterol. Hepatol. 2021, 15, 1401–1409. [Google Scholar] [CrossRef]
- Spooner, H.C.; Derrick, S.A.; Maj, M.; Manjarín, R.; Hernandez, G.V.; Tailor, D.S.; Bastani, P.S.; Fanter, R.K.; Fiorotto, M.L.; Burrin, D.G.; et al. High-Fructose, High-Fat Diet Alters Muscle Composition and Fuel Utilization in a Juvenile Iberian Pig Model of Non-Alcoholic Fatty Liver Disease. Nutrients 2021, 13, 4195. [Google Scholar] [CrossRef]
- Sikalidis, A.K.; Maykish, A. The Gut Microbiome and Type 2 Diabetes Mellitus: Discussing a Complex Relationship. Biomedicines 2020, 8, 8. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| TD2M Individuals | |||||||
|---|---|---|---|---|---|---|---|
| >40 years old | |||||||
| >10 years T2DM | |||||||
| At least one MACE | |||||||
| T2DM end organ damage | |||||||
| LDL-C >2.5 | |||||||
| <40 years old | |||||||
| >40 years old | >10 years T2DM | At least one MACE | T2DM end organ damage | LDL-C >2.5 | |||
| Index | N/A | Moderate intensity statin treatment | High intensity statin treatment | ||||
| Pharmacological Approach to Dyslipidaemia in T2DM Individuals | ||||
|---|---|---|---|---|
| Drug | Dosage | Mechanism of Action | Common Adverse Events | Monitoring (Except Lipid Profile) |
| Statins | 10–80 mg Oral use/daily | HMG-3-CoA reductase antagonist | Statin-associated muscle disease Fatigue Hepatic dysfunction | Serum aminotransferases Serum creatine-kinase Regular blood count |
| Ezetimibe | 10 mg Oral use/daily | NPC1L1 transporter inhibitor | Hepatic dysfunction Muscle-related effects | Serum aminotransferases Serum creatine-kinase |
| Alirocumab Evolocumab | 140 mg 75–300 mg Subcutaneous injections/2–4 weeks | PCSK9 inhibitors—monoclonal antibodies | Local injection reactions | - |
| Fibrates | 145–215 mg Oral use/daily | PPARs activators | Hepatic dysfunction Muscle-related effects Renal dysfunction | Serum aminotransferases Serum creatine-kinase Serum renal function tests Regular blood count |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Strikić, D.; Vujević, A.; Perica, D.; Leskovar, D.; Paponja, K.; Pećin, I.; Merćep, I. Importance of Dyslipidaemia Treatment in Individuals with Type 2 Diabetes Mellitus—A Narrative Review. Diabetology 2023, 4, 538-552. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology4040048
Strikić D, Vujević A, Perica D, Leskovar D, Paponja K, Pećin I, Merćep I. Importance of Dyslipidaemia Treatment in Individuals with Type 2 Diabetes Mellitus—A Narrative Review. Diabetology. 2023; 4(4):538-552. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology4040048
Chicago/Turabian StyleStrikić, Dominik, Andro Vujević, Dražen Perica, Dunja Leskovar, Kristina Paponja, Ivan Pećin, and Iveta Merćep. 2023. "Importance of Dyslipidaemia Treatment in Individuals with Type 2 Diabetes Mellitus—A Narrative Review" Diabetology 4, no. 4: 538-552. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology4040048