
Food as Medicine: FOODRx for Patients with Diabetes and Cardiovascular Disease in Central Minnesota—A PILOT STUDY
 ,
,
Abstract
:1. Introduction
2. Program Overview: Materials and Methods
2.1. Materials
2.2. Food Box
2.3. Clinic Selection
2.4. Participant Selection
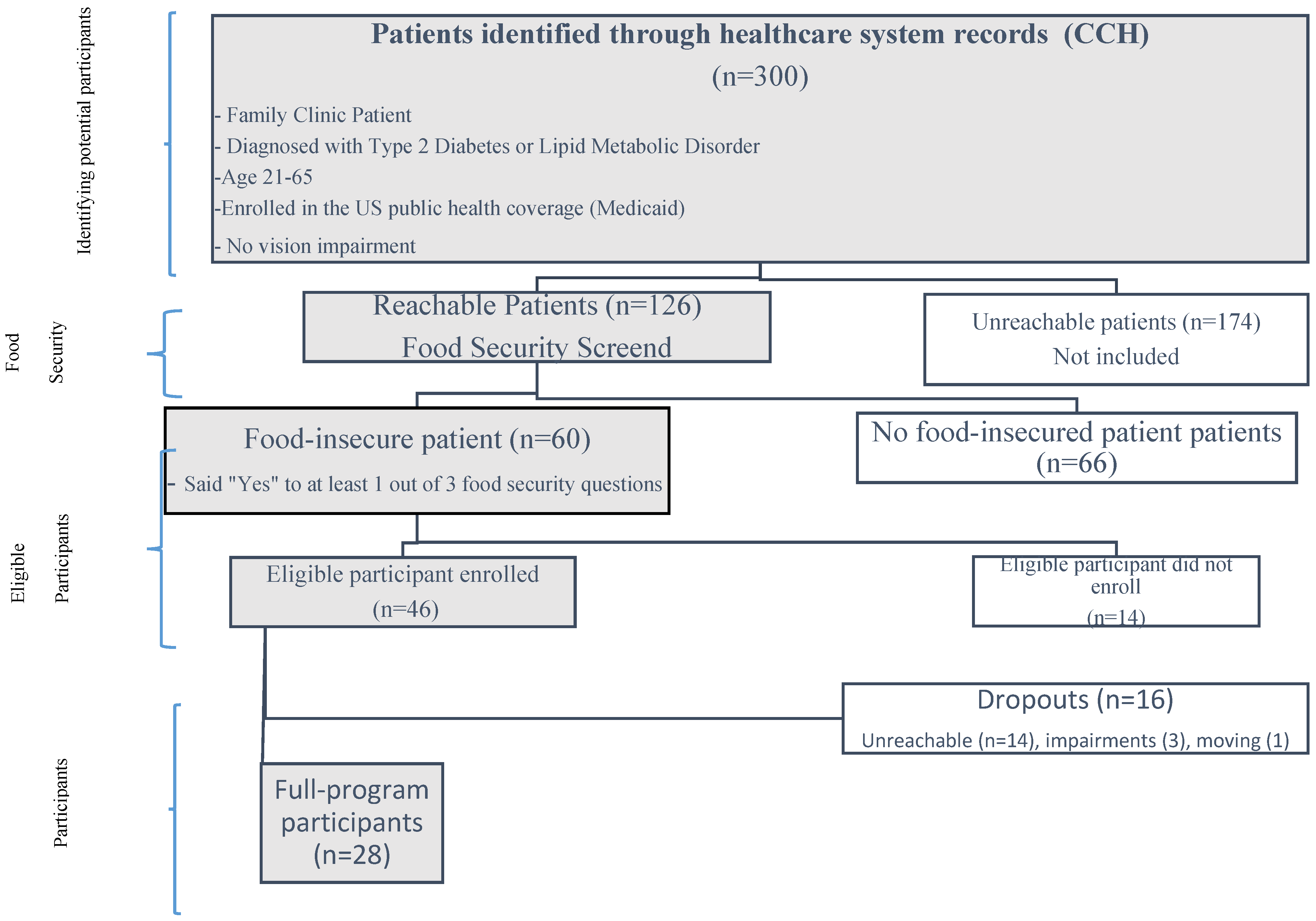
2.4.1. Potential Participants Identification
- a.
- Exclusion Criteria:
- b.
- Inclusion Criteria:
2.4.2. Food Insecurity
2.4.3. Eligible Participants Enrollment
2.4.4. Final Participants
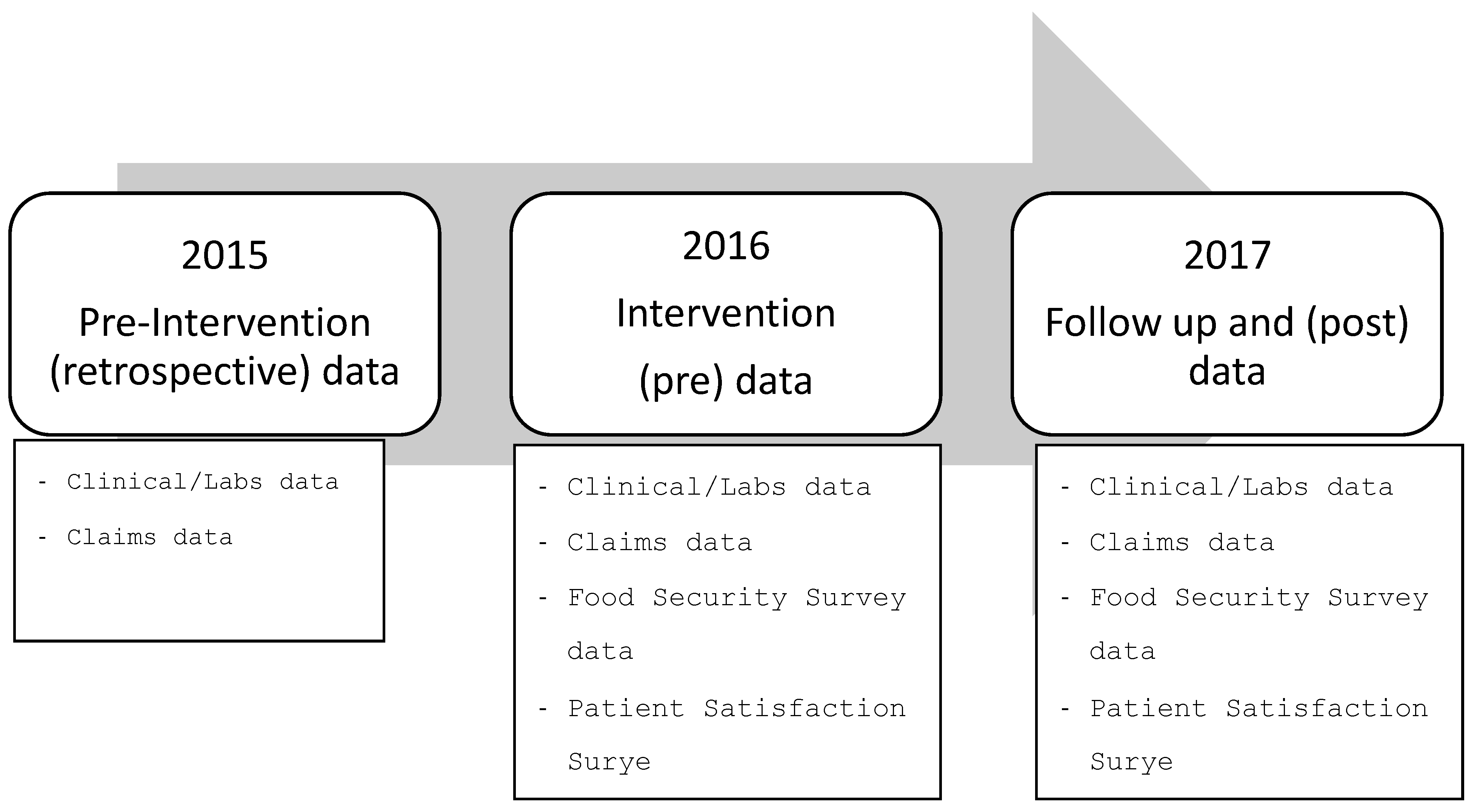
2.5. Study Data
2.5.1. Clinic/Labs Administrative Data
2.5.2. Claims Administrative Data
2.5.3. Survey Instruments
2.6. Target Outcomes
2.6.1. Primary Target Outcomes
2.6.2. Secondary Target Outcomes
2.7. Impact Analysis Methodology
3. Results
3.1. Laboratory and Other Health Measures
3.2. Health Services Utilization and Costs
3.3. Food Security, Self-Care Management, and Patient Satisfaction
4. Discussion
5. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ADA | American Diabetes Association |
| CCH | CentraCare Health |
| SHH | Second Harvest Heartland |
| CDC | Center for Disease Control |
| MN | Minnesota |
| USA/US | United States of America |
| AHRQ | Agency for Healthcare Research and Quality |
| HIPAA | Health Insurance Portability and Accountability act |
| HgbA1c | Hemoglobin A1c Levels |
| LDL | Low-Density Lipoprotein |
| BMI | Body Max Index |
| ER visits | Emergency room visits |
Appendix A. Online Appendix

{kind=link}
{kind=link}
| Category | Values | Optimal Level or Variations | Source |
|---|---|---|---|
| HbA1c | Laboratory | <7/0% | Laboratory |
| Fasting Glucose | Laboratory | >126 mg/dl | Laboratory |
| LDL/HDL | Laboratory | <100/45 mg/dL | Laboratory |
| Blood Pressure | Doctor visit/lab | <130/80 mm Hg | Doctor visit/lab |
| Triglycerides | Laboratory | <150 mg/dL | Laboratory |
| Heart Failure event | Inpatient/outpatient admin. Data. 1: Yes, 2: No | Categorical | Clinical/admin. data |
| Height | Doctor visit | Continuous | Clinical/admin. data |
| Weight | Doctor visit | Continuous | Clinical/admin. data |
| Date of Birth (age) | DD/MM/YYYY | Continuous | Clinical/admin. data |
| Sex | Male; Female | Categorical | Clinical/admin. data |
| Race/Ethnicity | White/Black/Hispanic/Other | Categorical | Clinical/admin. data |
| Language Written Preference | English/Somali/Spanish/Arabic/Other | Categorical | Clinical/admin. data |
| Marital Status | Married/Non-Married | Categorical | Clinical/admin. data |
| Insurance Status | Open-ended | Depends on system | Clinical/admin. data |
| Diabetes diagnostic | Yes or No | Participants are already diabetic patients | Clinical/admin. data |
| CVD diagnostic | Yes or No | Categorical | Clinical/admin. data |
| Other Chronic diseases? | Yes or No | Categorical | Clinical/admin. data |
| Tobacco Use | Yes, No, Never used | Categorical | Clinical/admin. data |
| Aspirin Use | Yes, No, Not Applicable | Categorical | Clinical/admin. data |
| Variables | Measure | Comments and Source |
|---|---|---|
| Inpatient Services | ||
| Hospital inpatient days and costs | Days and claimed insurance cost | Claims insurance data |
| Outpatient Services | ||
| Office Visits | number of visits, length, and estimated costs | Claims insurance data and Minnesota Community Measurement |
| ER visits | number of visits, length, and estimated costs | Claims insurance data and Minnesota Community Measurement |
| Hospital Outpatient | Days and claimed insurance cost | Claims insurance data |
| Average Commercial Cost | Average | |
|---|---|---|
| Office visit, Established Patient, 5 min | USD 45 | |
| Office visit, Established Patient, 10 min | USD 87 | |
| Office visit, Established Patient, 15 min | USD 146 | |
| Short Office Visit Average Cost | USD $93 | |
| Office visit, Established Patient, 25 min | USD 232 | |
| Office visit, Established Patient, 40 min | USD 313 | |
| Long Office Visit Average Cost | USD $273 | |
| Office visit, New Patient, 10 min | USD 92 | |
| Office visit, New Patient, 20 min | USD 161 | |
| Office visit, New Patient, 30 min | USD 240 | |
| Short Office Visit Average Cost, New Patient | USD $164 | |
| Office visit, New Patient, 45 min | USD 365 | |
| Office visit, New Patient, 60 min | USD 457 | |
| Long Office Visit Average Cost, New Patient | $411 |
| Question | Answer | Source |
|---|---|---|
| The first statement is, “The food that (I/we) bought just didn’t last, and (I/we) didn’t have money to get more”. Was that often, sometimes, or never true for (you/your household) in the last 12 months? | 1: Often true | [24] |
| 2: Sometimes true | ||
| 3: Never true | ||
| 4: DON’T KNOW | ||
| “(I/we) couldn’t afford to eat balanced meals”. Was that often, sometimes, or never true for (you/your household) in the last 12 months? [SURVEYOR: Show card #2 and circle number client points to below; if client asks what a “balanced meal” means, respond: “you can define balanced meal in whatever way you think is best”] | 1: Often true | [24] |
| 2: Sometimes true | ||
| 3: Never true | ||
| 4: DON’T KNOW | ||
| In the last 12 months, since last (name of current month), did (you/you or other adults in your household) ever cut the size of your meals or skip meals because there wasn’t enough money for food? | 1: Yes; 2:No; 3:DK | [24] |
| How often did this happen—almost every month, some months but not every month, or in only 1 or 2 months? | 1: Almost every month | [24] |
| 2: Some months but not every month | ||
| 3: Only 1 or 2 months | ||
| 4: DON’T KNOW | ||
| In the last 12 months, did you ever eat less than you felt you should because there wasn’t enough money for food? | 1: Yes; 2:No; 3:DK | [24] |
| In the last 12 months, were you every hungry but didn’t eat because there wasn’t enough money for food? | 1: Yes; 2:No; 3:DK | [24] |
| In the last four weeks how often did you eat any fresh fruit, canned fruit, or fruit in smoothies? Don’t count juices. | 1: Less than once per WEEK; 2: About 1 time per WEEK; 3: 2–3 times per WEEK; 4: 4–6 times per WEEK; 5:Once per DAY 6: 2 or more times per DAY | [26] |
| In the last four weeks how often did you eat green salad (such as lettuce or spinach salad)? | 1: Less than once per WEEK; 2: About 1 time per WEEK; 3: 2–3 times per WEEK; 4: 4–6 times per WEEK; 5:Once per DAY 6: 2 or more times per DAY | [26] |
| In the last four weeks how often did you eat vegetable soup or stew with vegetables? | 1: Less than once per WEEK; 2: About 1 time per WEEK; 3: 2–3 times per WEEK; 4: 4–6 times per WEEK; 5:Once per DAY 6: 2 or more times per DAY | [26] |
| During the past month, have you often been bothered by feeling down, depressed, or hopeless? | 1: Yes; 2:No; 3: Don’t Know | [27] |
| Sometimes people run out of the food they need to take care of their diabetes and don’t have enough money or resources to get more. In the last 30 days, how often did you run out of the food you needed to take care of your diabetes? Would you say… | 1: Never | [17] |
| 2: Rarely | ||
| 3: Sometimes | ||
| 4: Often | ||
| Do you ever forget to take your medicine? | 1: Yes; 2: No; 3: Don’t Know | [28] |
| Are you careless and/or confused at times about taking your medicine? | 1: Yes; 2: No; 3: Don’t Know | [28] |
| When you feel better do you sometimes stop taking your medicine? | 1: Yes; 2: No; 3: Don’t Know | [28] |
| Sometimes if you feel worse when you take the medicine, do you | 1: Yes; 2: No; 3: Don’t Know | [28] |
| stop taking it? | ||
| In the last 12 months, how often did you take less medicine than you were supposed to because you could not afford to buy more? | 1: Never, 2: Rarely, 3: Sometimes, 4: Often | [17] |
| In the last 12 months, how often did you put off buying food so that you would have money to buy your medicines? | 1: Never, 2: Rarely, 3: Sometimes, 4: Often | [17] |
| In the last 12 months, how often did you put off buying for medicines so that you would have money to buy food? | 1: Never, 2: Rarely, 3: Sometimes, 4: Often | [17] |
| Exercising regularly? | 1: So Difficult that you couldn’t do it at all | [29] |
| 2: Very Difficult, you hardly ever do it | ||
| 3: Difficult, but you could do it some of the time | ||
| 4: Not difficult, you could do it most of the time | ||
| 5: Not difficult, you got it exactly right | ||
| 6: [Don’t read] Doesn’t Apply, you don’t do it, or members of your diabetes team did not recommend it | ||
| Following your recommended eating plan? | 1: So Difficult that you couldn’t do it at all | [29] |
| 2: Very Difficult, you hardly ever do it | ||
| 3: Difficult, but you could do it some of the time | ||
| 4: Not difficult, you could do it most of the time | ||
| 5: Not difficult, you got it exactly right | ||
| 6: [Don’t read] Doesn’t Apply, you don’t do it, or members of your diabetes team did not recommend it | ||
| Checking your blood sugar? | 1: So Difficult that you couldn’t do it at all | [29] |
| 2: Very Difficult, you hardly ever do it | ||
| 3: Difficult, but you could do it some of the time | ||
| 4: Not difficult, you could do it most of the time | ||
| 5: Not difficult, you got it exactly right | ||
| 6: [Don’t read] Doesn’t Apply, you don’t do it, or members of your diabetes team did not recommend it | ||
| Checking your feet for wounds and sores? | 1: So Difficult that you couldn’t do it at all | [29]. |
| 2: Very Difficult, you hardly ever do it | ||
| 3: Difficult, but you could do it some of the time | ||
| 4: Not difficult, you could do it most of the time | ||
| 5: Not difficult, you got it exactly right | ||
| 6: [Don’t read] Doesn’t Apply, you don’t do it, or members of your diabetes team did not recommend it | ||
| Overall rating of doctor visits | Scale | [30] and Authors creation |
| 0 to 10 (0 worse to 10 Excellent) | ||
| Have you been referred to a nutritionist by your doctor before? | 1: Yes, | [30] and Authors creation |
| 2: No, | ||
| 3: Not Applicable | ||
| Have you been referred to an educational program by your doctor before? | 1: Yes, | [30] and Authors creation |
| 2: No, | ||
| 3: Not Applicable | ||
| How many times have you attended a diabetes educational workshop in the last 12 months? | Numerical Open ended. | [30] and Authors creation |
| Rate educational programs ability to give information as wanted to manage your condition | Scale | [30] and Authors creation |
| 0 to 10 (0 worse to 10 Excellent) | ||
| Rate educational programs ability to care responsive to cultural needs | Scale | [30] and Authors creation |
| 0 to 10 (0 worse to 10 Excellent) | ||
| Overall rating of nutrition counseling | Scale | [30] and Authors creation |
| 0 to 10 (0 worse to 10 Excellent) | ||
| Overall rating educational activities | Scale | [30] and Authors creation |
| 0 to 10 (0 worse to 10 Excellent) |
References
- American Diabetes Association. Fast Facts: Data and Statistics about Diabetes; American Diabetes Association: Arlington, VA, USA, 2015; Available online: https://professional.diabetes.org/sites/default/files/media/diabetes_fast_facts22322.pdf (accessed on 26 December 2023).
- NDEP Campaign Highlights the Link between Diabetes and Cardiovascular Disease. Available online: https://www.nih.gov/news-events/news-releases/ndep-campaign-highlights-link-between-diabetes-cardiovascular-disease (accessed on 26 December 2023).
- American Diabetes Association. Economic Costs of Diabetes in the U.S. in 2012. Diabetes Care 2013, 36, 1033–1046. [Google Scholar] [CrossRef]
- Osborn, B.; Morey, B.N.; Billimek, J.; Ro, A. Food Insecurity and Type 2 Diabetes among Latinos: Examining Neighborhood Cohesion as a Protective Factor. J. Racial Ethn. Health Disparities 2023, 10, 2061–2070. [Google Scholar] [CrossRef]
- The Boston Consulting Group. Improving Hunger and Health Outcomes in Minnesota: Poor Health Status & Chronic Diseases More Prevalent in Food-Insecure Populations; Hunger-Free Minnesota: Minneapolis, MN, USA, 2013. [Google Scholar]
- Gao, Y.; Yang, A.; Zurbau, A.; Gucciardi, E. The Effect of Food Is Medicine Interventions on Diabetes-Related Health Outcomes Among Low-Income and Food-Insecure Individuals: A Systematic Review and Meta-Analysis. Can. J. Diabetes 2023, 47, 143–152. [Google Scholar] [CrossRef]
- Rao, M.; Afshin, A.; Singh, G.; Mozaffarian, D. Do Healthier Foods and Diet Patterns Cost More than Less Healthy Options? A Systematic Review and Meta-Analysis. BMJ Open 2013, 3, e004277. [Google Scholar] [CrossRef]
- Gundersen, C.; Seligman, H.K. Food Insecurity and Health Outcomes. Econ. Voice 2017, 14, 1. [Google Scholar] [CrossRef]
- Mykerezi, E.K. Minnesota Cost/Benefit Hunger Impact Study; Hunger-Free Minnesota: St. Paul, MN, USA, 2010. [Google Scholar]
- Seligman, H.K.; Jacobs, E.A.; López, A.; Tschann, J.; Fernandez, A. Food Insecurity and Glycemic Control among Low-Income Patients with Type 2 Diabetes. Diabetes Care 2012, 35, 233–238. [Google Scholar] [CrossRef]
- Lyles, C.R.; Wolf, M.S.; Schillinger, D.; Davis, T.C.; Dewalt, D.; Dahlke, A.R.; Curtis, L.; Seligman, H.K. Food Insecurity in Relation to Changes in Hemoglobin A1c, Self-Efficacy, and Fruit/Vegetable Intake during a Diabetes Educational Intervention. Diabetes Care 2013, 36, 1448–1453. [Google Scholar] [CrossRef] [PubMed]
- Ford, E.S. Food Security and Cardiovascular Disease Risk among Adults in the United States: Findings from the National Health and Nutrition Examination Survey, 2003–2008. Prev. Chronic Dis. 2013, 10, E202. [Google Scholar] [CrossRef] [PubMed]
- Berkowitz, S.A.; Meigs, J.B.; DeWalt, D.; Seligman, H.K.; Barnard, L.S.; Bright, O.J.; Schow, M.; Atlas, S.J.; Wexler, D.J. Material Need Insecurities, Control of Diabetes Mellitus, and Use of Health Care Resources: Results of the Measuring Economic Insecurity in Diabetes Study. JAMA Intern. Med. 2015, 175, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Seligman, H.K.; Schillinger, D. Hunger and Socioeconomic Disparities in Chronic Disease. N. Engl. J. Med. 2010, 363, 6–9. [Google Scholar] [CrossRef] [PubMed]
- Zhuo, X.; Zhang, P.; Hoerger, T.J. Lifetime Direct Medical Costs of Treating Type 2 Diabetes and Diabetic Complications. Am. J. Prev. Med. 2013, 45, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Hanson, K.L.; Connor L., M. Food Insecurity and Dietary Quality in US adults and Children: A Systematic Review. Am. J. Clin. Nutr. 2014, 100, 684–692. [Google Scholar] [CrossRef] [PubMed]
- Seligman, H.K.; Lyles, C.; Marshall, M.B.; Prendergast, K.; Smith, M.C.; Headings, A.; Bradshaw, G.; Rosenmoss, S.; Waxman, E. A Pilot Food Bank Intervention Featuring Diabetes-Appropriate Food Improved Glycemic Control among Clients in Three States. Health Aff. 2015, 34, 1956–1963. [Google Scholar] [CrossRef] [PubMed]
- Bleich, S.N.; Dupuis, R.; Seligman, H.K. Food Is Medicine Movement—Key Actions Inside and Outside the Government. JAMA Health Forum 2023, 4, e233149. [Google Scholar] [CrossRef]
- Berkowitz, S.A.; Orr, C.J. Three Lessons About Diabetes and the Social Determinants of Health. Diabetes Care 2023, 46, 1587–1589. [Google Scholar] [CrossRef]
- Chronic Conditions in Minnesota: New Estimates of Prevalence, Cost and Geographic Variation for Insured Minnesotans. 2012. Available online: https://www.apcdcouncil.org/resource/chronic-conditions-minnesota-new-estimates-prevalence-cost-geographic-variation-insured-minnesotans (accessed on 26 December 2023).
- Center of Disease Control. Somali Refugee Health Profile. Available online: https://www.cdc.gov/immigrantrefugeehealth/profiles/somali/index.html#diabetes (accessed on 26 December 2023).
- Seligman, H.K.; Smith, M.; Rosenmoss, S.; Marshall, M.B.; Waxman, E. Comprehensive Diabetes Self-Management Support from Food Banks: A Randomized Controlled Trial. Am. J. Public Health 2018, 108, 1227–1234. [Google Scholar] [CrossRef]
- Wylie-Rosett, J.; DiMeglio, L.A. Strategies to Reduce Food Insecurity for People With Diabetes: A Call to Action. Diabetes Care 2023, 46, 245–248. [Google Scholar] [CrossRef]
- NHANES 2017–2018 Questionnaire Data Overview. U.S. Adult Food Security Survey Module: Three-State Design, with Screeners. Available online: https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/overviewquex.aspx?BeginYear=2017 (accessed on 26 December 2023).
- Minnesota Community Measurement Report on Cost and Utilization (2016–2017). Available online: https://mncmsecure.org/website/MNHealthScores%20Snapshots/2019%20MY/Appendix%20Tables/ACP_Office%20Visit%202019MY%20Results.pdf (accessed on 10 December 2023).
- Wakimoto, P.; Block, G.; Mandel, S.; Medina, N. Development and Reliability of Brief Dietary Assessment Tools for Hispanics. Prev. Chronic Dis. 2006, 3, A95. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Morisky, D.E.; Green, L.W.; Levine, D.M. Concurrent and Predictive Validity of a Self-Reported Measure of Medication Adherence. Med. Care 1986, 24, 67–74. [Google Scholar] [CrossRef]
- Heisler, M.; Bouknight, R.R.; Hayward, R.A.; Smith, D.M.; Kerr, E.A. The Relative Importance of Physician Communication, Participatory Decision Making, and Patient Understanding in Diabetes Self-Management. J. Gen. Intern. Med. 2002, 17, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Agency for Healthcare Research and Quality. ECHO Survey Measures. Available online: https://www.ahrq.gov/cahps/surveys-guidance/echo/about/survey-measures.html (accessed on 26 December 2023).
- Law, K.K.; Coyle, D.H.; Neal, B.; Huang, L.; Barrett, E.M.; Arnott, C.; Chow, C.K.; Di Tanna, G.L.; Lung, T.; Mozaffarian, D.; et al. Protocol for a Randomized Controlled Trial of Medically Tailored Meals Compared to Usual Care among Individuals with Type 2 Diabetes in Australia. Contemp. Clin. Trials 2023, 132, 107307. [Google Scholar] [CrossRef] [PubMed]
- Levi, R.; Bleich, S.N.; Seligman, H.K. Food Insecurity and Diabetes: Overview of Intersections and Potential Dual Solutions. Diabetes Care 2023, 46, 1599–1608. [Google Scholar] [CrossRef]
- Stroud, B.; Sastre, L. Impact and Acceptability of the Fresh Start Produce Rx Program on Food Literacy, Nutrition and Health. J. Nutr. Educ. Behav. 2023, 55, 79. [Google Scholar] [CrossRef]
- Walker, R.; Thorgerson, A.; Mosley-Johnson, E.; Egede, L. IDF2022-0221 The Burden of Food Insecurity on Quality of Life in Adults with Diabetes. Diabetes Res. Clin. Pract. 2023, 197 (Suppl. 1), 110507. [Google Scholar] [CrossRef]
- Lumpkin, J.R.; Taylor, L.H.; Hattori, A.; Jedele, J.M. Impact of Food Delivery and Health Coaching on Outcomes and Costs of Care: A Payer’s Perspective. NEJM Catal. Innov. Care Deliv. 2023, 4, 1–20. [Google Scholar] [CrossRef]
- U.S. Adult Food Security Survey Module: Three-Stage Design, with Screeners Economic Research Service, USDA July 2012. Available online: https://www.ers.usda.gov/media/8279/ad2012.pdf (accessed on 26 December 2023).


| Characteristic | Participants (N = 28) | Dropouts (N = 18) |
|---|---|---|
| Age | ||
| Average | 53 | 44 |
| Median | 54 | 45 |
| Maximum | 66 | 65 |
| Female (%) | 71 | 50 |
| Race/Ethnicity (%) | ||
| White | 39 | 33 |
| Black | 39 | 50 |
| Other | 18 | 11 |
| Religion (%) | ||
| Muslim | 36 | 28 |
| Christian/Catholic | 29 | 56 |
| Other | 14 | 0 |
| None or No response | 14 | 17 |
| Language Written (%) | ||
| English | 54 | 72 |
| Somali | 36 | 22 |
| Other | 7 | 0 |
| No Response | 4 | 6 |
| Marital Status (%) | ||
| Non-Married | 54 | 56 |
| Current Smoker (%) | 7 | 28 |
| Unemployed (%) | 50 | - |
| Gift Card usage (average) | 8 | - |
| Final Participant | Dropout | |||||||
|---|---|---|---|---|---|---|---|---|
| N | Before | Pre | Post | N | Before | Pre | Post | |
| Glucose levels | ||||||||
| Glucose D | 28 | 214 | 201 | 187 (*) | 16 | 170 | 177 | 178 |
| HbA1C (%) | 28 | 16 | ||||||
| Average | 9.6 | 9.2 | 9.1 (**) | 8.1 | 7.9 | 9.3 (**) | ||
| >9% | 71 | 54 | 54 (**) | 25 | 31 | 44 (**) | ||
| Experienced reduction | 71 | 61 | 20 | 40 | ||||
| Average change | −0.2 | −0.1 | 0.2 | 0.3 | ||||
| Lipids Measures (mg/dL) | ||||||||
| Cholesterol | 18 | 153 | 162 | 161 | 12 | 192 | 162 | 140 |
| LDL | 18 | 85 | 90 | 88 | 12 | 97 | 86 | 73 |
| VLDL | 18 | 30 | 32 | 32 | 12 | 38 | 32 | 29 |
| HDL | 18 | 38 | 40 | 41 | 12 | 40 | 38 | 37 |
| Triglycerides | 18 | 154 | 159 | 160 | ||||
| BMI | 28 | 36.13 | 35.93 | 36.64 | 18 | 33.58 | 33.73 | 32.95 |
| Blood Pressure(mmHg) | ||||||||
| Diastolic | 28 | 72 | 72 | 72 | 18 | 78 | 77 | 78 |
| Systolic | 28 | 120 | 119 | 120 | 18 | 123 | 121 | 127 |
| Before | During | Test | |
|---|---|---|---|
| HEALTHCARE USAGE | |||
| Hospital Encounters | |||
| Number of | |||
| ER visits | 34 | 28 | |
| Outpatient visits | 68 | 68 | |
| Inpatient visits | 6 | 5 | |
| Average | |||
| ER Visit per participant | 1.21 | 1.00 | ** |
| ER Visit per ER user | 2.48 | 2.15 | * |
| Outpatient visit per participant | 2.43 | 2.43 | |
| Outpatient visit per user | 3.57 | 4 | * |
| Office Visits | |||
| Number of | |||
| Short visits (30 or less minutes) | 271 | 468 | |
| Long visits (30+ minutes) | 75 | 51 | |
| Average | |||
| Short visits per user | 8.96 | 16.6 | *** |
| Long visits per participant | 2.68 | 1.82 | |
| Long visits per user | 3 | 2.55 | |
| Medical COSTS | |||
| Health Insurance Claims | |||
| Number of Claims | 198 | 141 | |
| Claims (USD thousand) | 597.24 | 355.62 | |
| Average Claims (USD thousand) | 3.02 | 2.55 | |
| ER-related Claims (USD thousand) | 64.77 | 48.73 | * |
| Average per user (USD thousand) | 4.98 | 3.75 | |
| Outpatient-related Claims (USD thousand) | 67.33 | 60.28 | |
| Average per user (USD thousand) | 4.21 | 4.02 |
| Pre | Post | Test | |
|---|---|---|---|
| (N = 27) | (N = 27) | ||
| Food Security | |||
| Food did not last (Often/Sometimes) | 85 | 63 | |
| Cannot afford balanced food (Often/Sometimes) | 85 | 63 | |
| Cut size/skipped meals b/c no money (Yes) | 52 | 15 | ** |
| Eat least than should b/c no money (Yes) | 59 | 19 | |
| Hungry but didn’t eat b/c no money (Yes) | 44 | 7 | *** |
| Overall Diet, Self-care and Medication Adherence | |||
| Vegetables and veggie stew (at least once per week) | 33 | 81 | |
| Ran out of disease-appropriate food b/c of money (Never) | 26 | 59 | |
| Put off buying food b/c buying medicine (Never) | 67 | 96 | *** |
| Put off buying medicine b/c buying food (Never) | 63 | 93 | ** |
| Patient Satisfaction | |||
| Overall Doctor Visits (average) | 4.3 | 4.4 | |
| Nutritionist referral (Yes) | 74 | 93 | *** |
| Educational program responds to cultural needs (average) | 2.1 | 3.4 | ** |
| Overall rating educational activities (average) | 2.6 | 4.1 | *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Pérez, M.; De Kesel Lofthus, A.; Tilstra, D.; Switzer, K.; Williamson, K. Food as Medicine: FOODRx for Patients with Diabetes and Cardiovascular Disease in Central Minnesota—A PILOT STUDY. Diabetology 2024, 5, 110-128. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology5010009
García-Pérez M, De Kesel Lofthus A, Tilstra D, Switzer K, Williamson K. Food as Medicine: FOODRx for Patients with Diabetes and Cardiovascular Disease in Central Minnesota—A PILOT STUDY. Diabetology. 2024; 5(1):110-128. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology5010009
Chicago/Turabian StyleGarcía-Pérez, Mónica, Alexandra De Kesel Lofthus, David Tilstra, Kevin Switzer, and Kristen Williamson. 2024. "Food as Medicine: FOODRx for Patients with Diabetes and Cardiovascular Disease in Central Minnesota—A PILOT STUDY" Diabetology 5, no. 1: 110-128. https://0-doi-org.brum.beds.ac.uk/10.3390/diabetology5010009