Predicting Clinical Efficacy of Vascular Disrupting Agents in Rodent Models of Primary and Secondary Liver Cancers: An Overview with Imaging-Histopathology Correlation

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Animal Models of Primary and Secondary Liver Cancers Usable for VDAs Studies
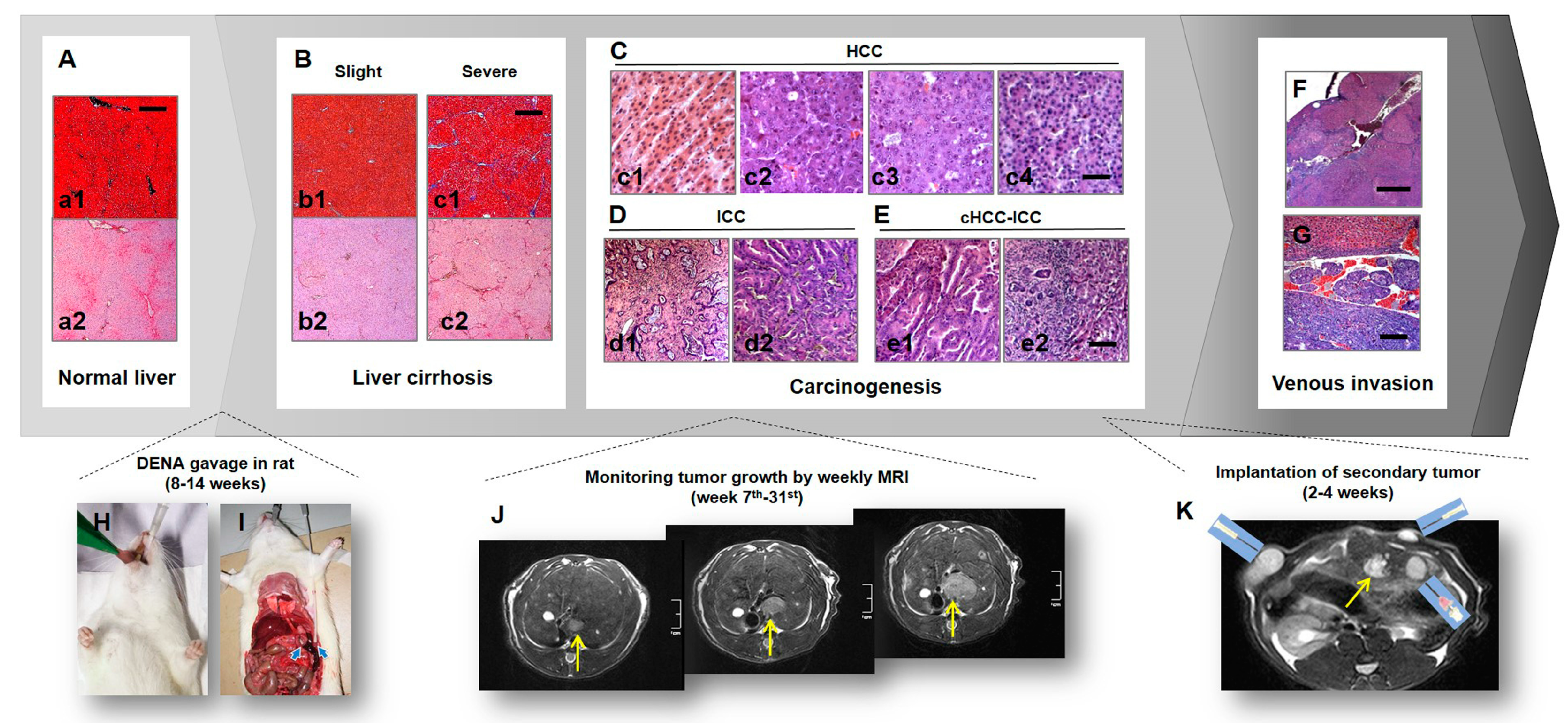
2.1. Primary Liver Cancer Model in Rats
2.2. Complex Model of Primary and Secondary Liver Tumors for Comparative VDA Studies
2.3. Clinical Relevance of Rodent Models to Human Patients on the Use of VDAs
3. Multiparametric MRI on Target/Receiver Selection and Efficacy Evaluation of VDA Therapy
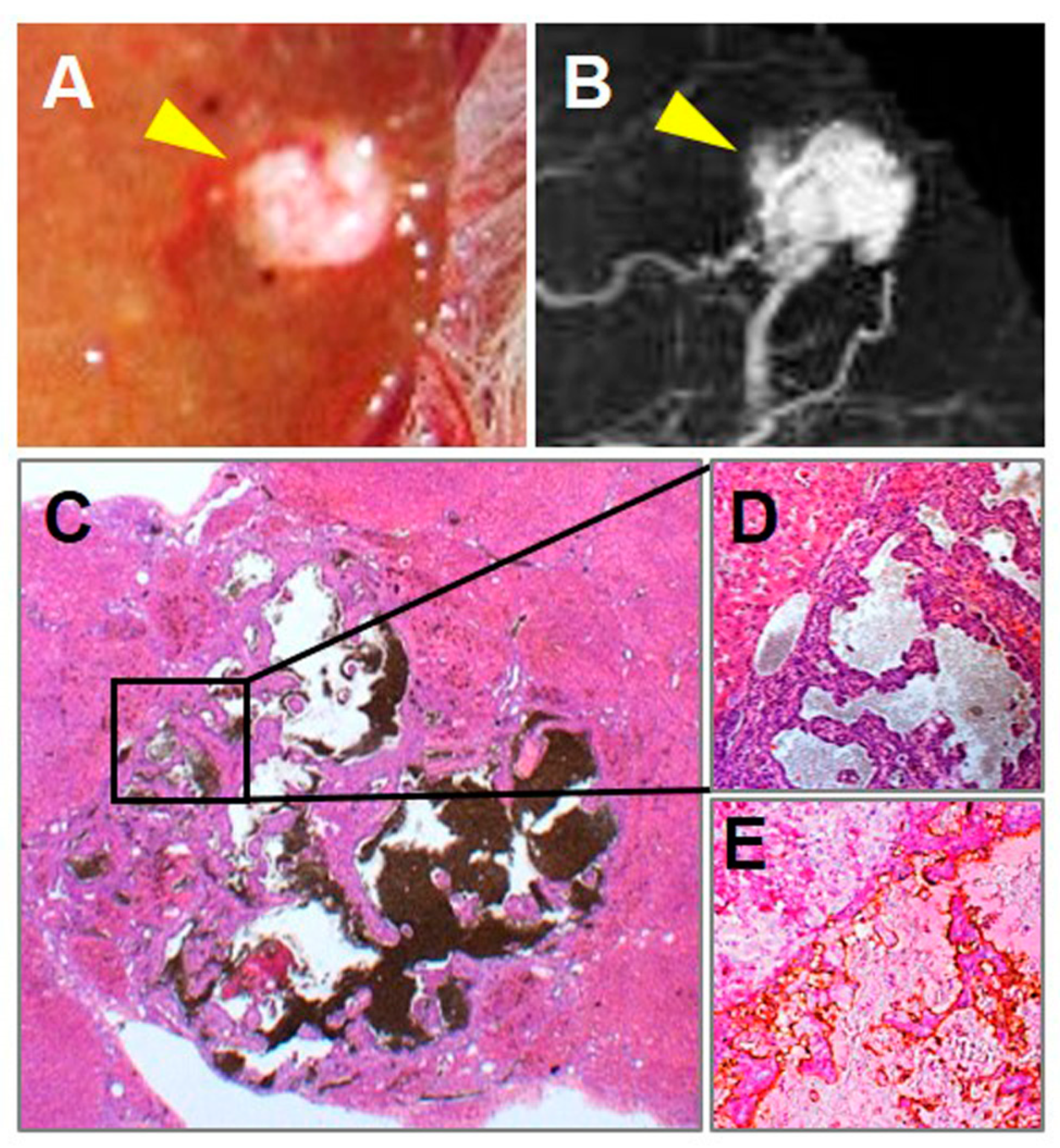
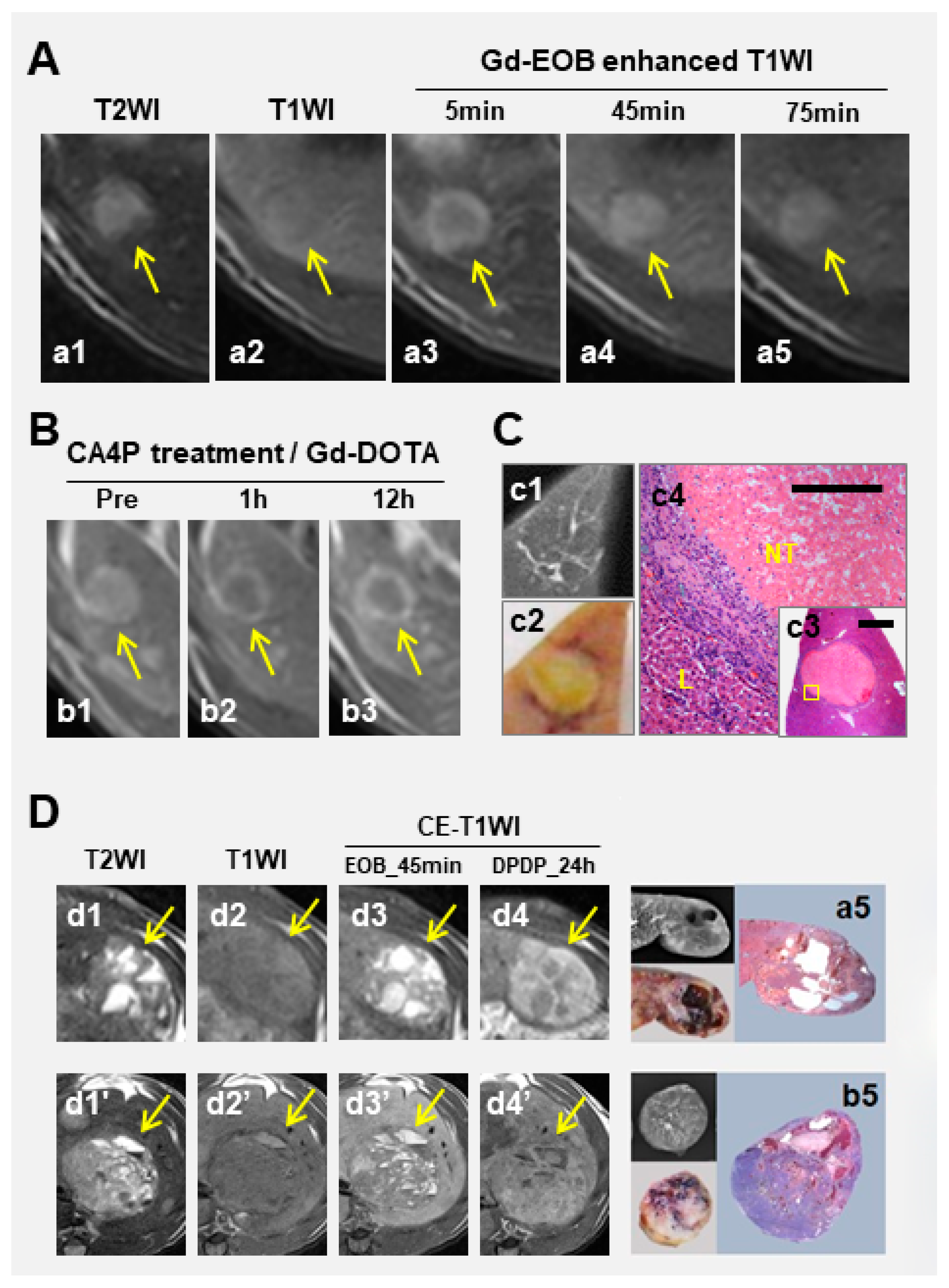
3.1. Hepatobiliary CAs
3.2. Nonspecific MRI CA
3.3. Dynamic Contrast Enhancement (DCE) MRI
3.4. Diffusion-Weighted Imaging (DWI)
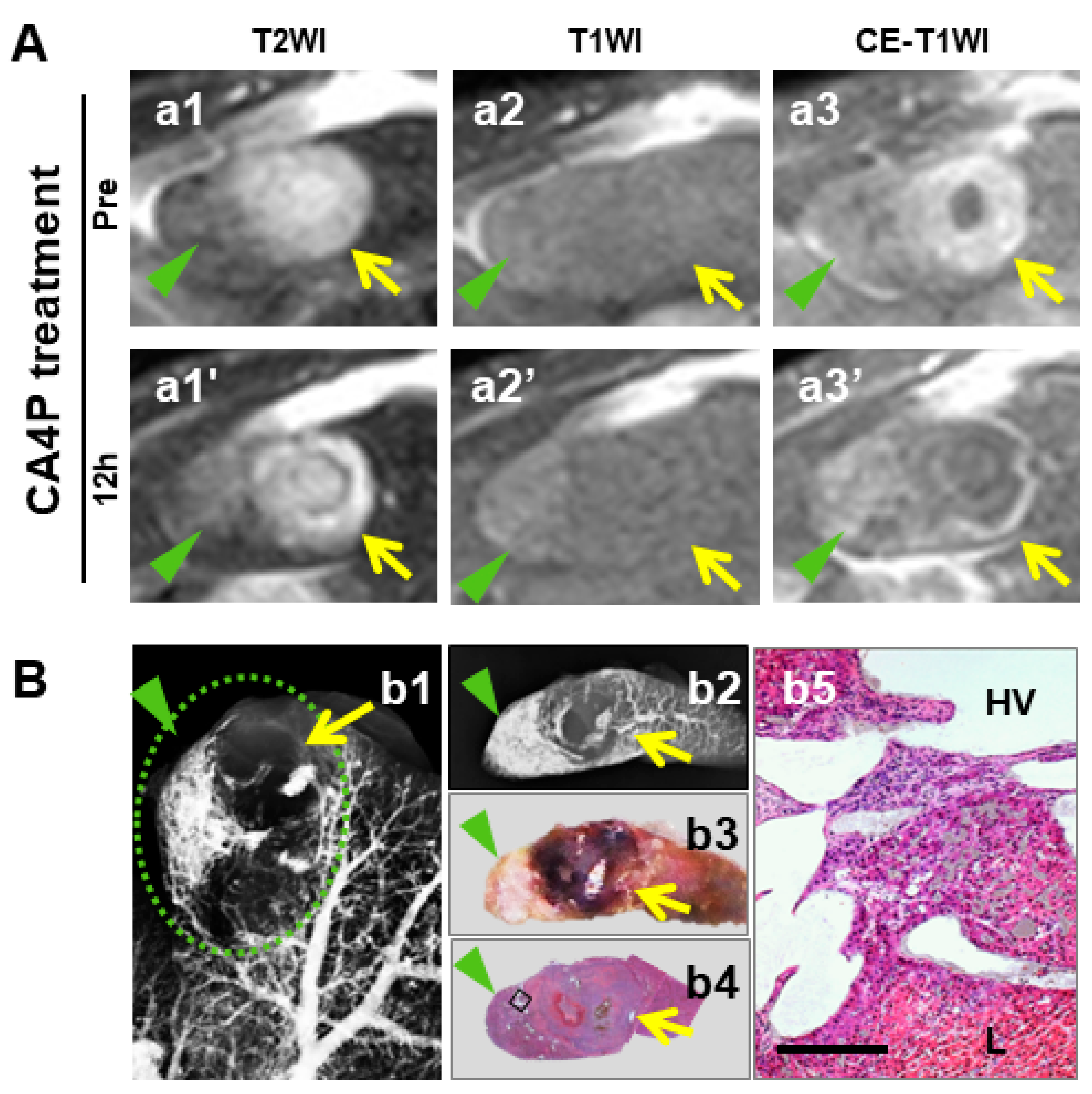
4. Update of Antitumor Effects of CA4P in Primary and Secondary Liver Cancers
4.1. CA4P Dose-Related Efficacy
4.2. Vascularity and Differentiation of HCCs in Relation to CA4P Efficacies
4.3. Distinct Volume-Efficacy Relation between Micro-HCCs and Macro-HCCs
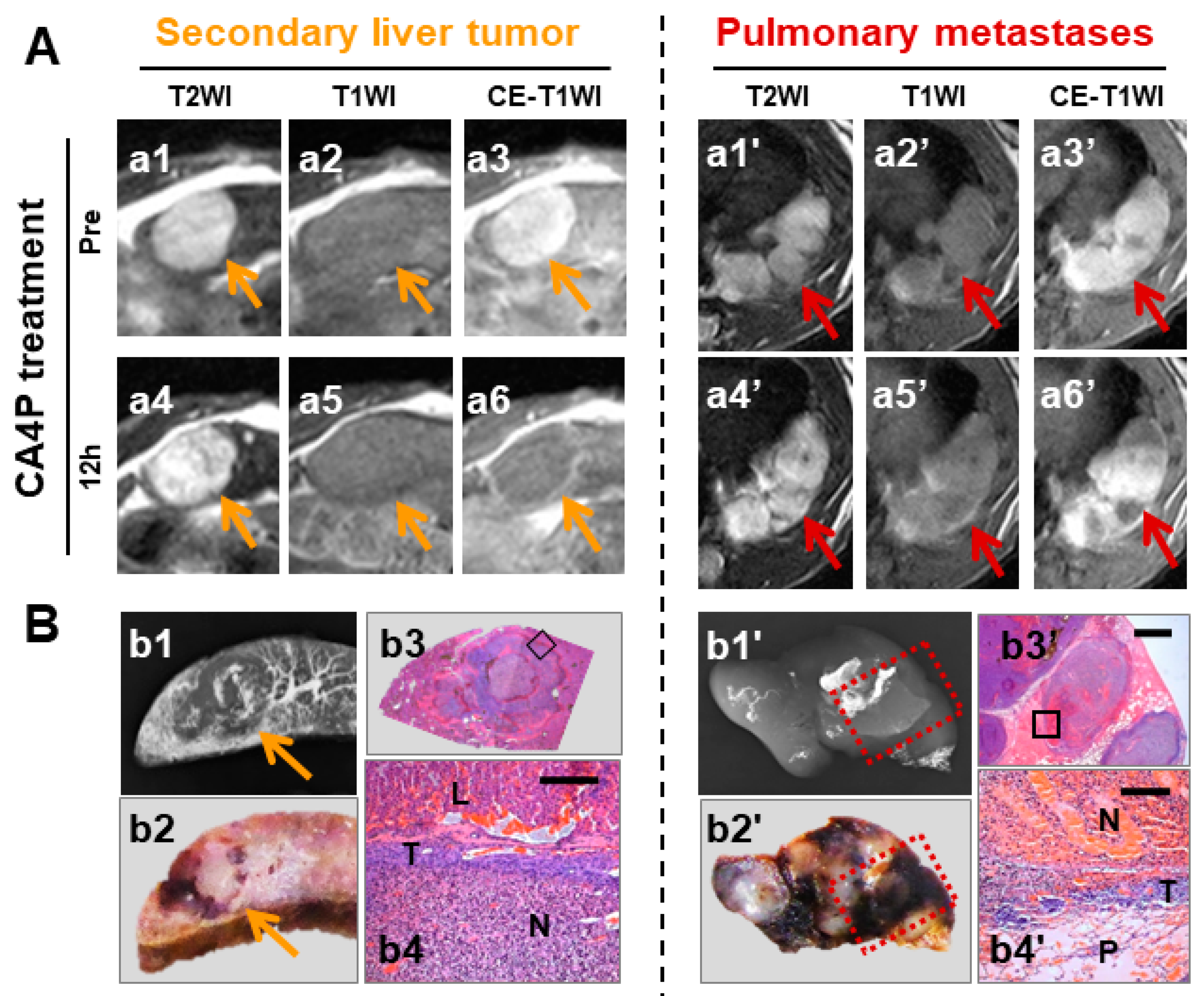
4.4. Superior Efficacy in Secondary Malignancies Shown by Intraindividual Comparison
5. Study Limitations and Practical Challenges
6. Future Perspectives of VDA in Experimental Liver Cancers
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Tozer, G.M.; Kanthou, C.; Baguley, B.C. Disrupting tumour blood vessels. Nat. Rev. Cancer 2005, 5, 423–435. [Google Scholar] [CrossRef] [PubMed]
- Cooney, M.M.; Van Heeckeren, W.; Bhakta, S.; Ortiz, J.; Remick, S.C. Drug Insight: vascular disrupting agents and angiogenesis—Novel approaches for drug delivery. Nat. Clin. Pract. Oncol. 2006, 3, 682–692. [Google Scholar] [CrossRef] [PubMed]
- Hinnen, P.; Eskens, F.A.L.M. Vascular disrupting agents in clinical development. Br. J. Cancer 2007, 96, 1159–1165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siemann, D.W.; Chaplin, D.J.; Walicke, P.A. A review and update of the current status of the vasculature-disabling agent combretastatin-A4 phosphate (CA4P). Expert Opin. Investig. Drugs 2009, 18, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Dowlati, A.; Robertson, K.; Cooney, M.; Petros, W.P.; Stratford, M.; Jesberger, J.; Rafie, N.; Overmoyer, B.; Makkar, V.; Stambler, B.; et al. A phase I pharmacokinetic and translational study of the novel vascular targeting agent combretastatin a-4 phosphate on a single-dose intravenous schedule in patients with advanced cancer. Cancer Res. 2002, 62, 3408–3416. [Google Scholar] [PubMed]
- Rustin, G.J.S.; Galbraith, S.M.; Anderson, H.; Stratford, M.; Folkes, L.K.; Sena, L.; Gumbrell, L.; Price, P.M. Phase I Clinical Trial of Weekly Combretastatin A4 Phosphate: Clinical and Pharmacokinetic Results. J. Clin. Oncol. 2003, 21, 2815–2822. [Google Scholar] [CrossRef]
- Zweifel, M.; Jayson, G.; Reed, N.S.; Osborne, R.; Hassan, B.; Ledermann, J.; Shreeves, G.; Poupard, L.; Lu, S.-P.; Balkissoon, J.; et al. Phase II trial of combretastatin A4 phosphate, carboplatin, and paclitaxel in patients with platinum-resistant ovarian cancer. Ann. Oncol. 2011, 22, 2036–2041. [Google Scholar] [CrossRef]
- Garon, E.B.; Kabbinavar, F.F.; Neidhart, J.A.; Gabrail, N.Y.; Oliveira, M.R.; Lu, S.; Balkissoon, J. A randomized phase II trial of a vascular disrupting agent (VDA) fosbretabulin tromethamine (CA4P) with carboplatin (C), paclitaxel (P), and bevacizumab (B) in stage 3B/4 nonsquamous non-small cell lung cancer (NSCLC): Analysis of safety and activity of the FALCON trial. J. Clin. Oncol. 2011, 29, 7559. [Google Scholar]
- Sosa, J.A.; Elisei, R.; Jarzab, B.; Bal, C.S.; Koussis, H.; Gramza, A.W.; Ben-Yosef, R.; Gitlitz, B.J.; Haugen, B.; Karandikar, S.M.; et al. A randomized phase II/III trial of a tumor vascular disrupting agent fosbretabulin tromethamine (CA4P) with carboplatin (C) and paclitaxel (P) in anaplastic thyroid cancer (ATC): Final survival analysis for the FACT trial. J. Clin. Oncol. 2011, 29, 5502. [Google Scholar] [CrossRef]
- Ng, Q.-S.; Mandeville, H.; Goh, V.; Alonzi, R.; Milner, J.; Carnell, D.; Meer, K.; Padhani, A.R.; Saunders, M.I.; Hoskin, P.J. Phase Ib trial of radiotherapy in combination with combretastatin-A4-phosphate in patients with non-small-cell lung cancer, prostate adenocarcinoma, and squamous cell carcinoma of the head and neck. Ann. Oncol. 2012, 23, 231–237. [Google Scholar] [CrossRef]
- Chen, F.; Feng, Y.; Zheng, K.; De Keyzer, F.; Li, J.; Feng, Y.; Cona, M.M.; Wang, H.; Jiang, Y.; Yu, J.; et al. Enhanced Antitumor Efficacy of a Vascular Disrupting Agent Combined with an Antiangiogenic in a Rat Liver Tumor Model Evaluated by Multiparametric MRI. PLoS ONE 2012, 7, e41140. [Google Scholar] [CrossRef] [PubMed]
- Koh, D.-M.; Blackledge, M.; Collins, D.J.; Padhani, A.R.; Wallace, T.; Wilton, B.; Taylor, N.J.; Stirling, J.J.; Sinha, R.; Walicke, P.; et al. Reproducibility and changes in the apparent diffusion coefficients of solid tumours treated with combretastatin A4 phosphate and bevacizumab in a two-centre phase I clinical trial. Eur. Radiol. 2009, 19, 2728–2738. [Google Scholar] [CrossRef] [PubMed]
- A Video Introduction to OncoCiDia. Available online: http://vimeo.com/44871398 (accessed on 2 January 2020).
- Ni, Y. Oncocidia: A Small Molecule Dual Targeting Pan-Anticancer Theragnostic Strategy; AACR: San Diego, CA, USA, 2014; p. 19. [Google Scholar]
- Li, J.; Sun, Z.; Zhang, J.; Shao, H.; Cona, M.M.; Wang, H.; Marysael, T.; Chen, F.; Prinsen, K.; Zhou, L.; et al. A Dual-targeting Anticancer Approach: Soil and Seed Principle. Radiol. 2011, 260, 799–807. [Google Scholar] [CrossRef]
- Li, J.; Cona, M.M.; Chen, F.; Feng, Y.; Zhou, L.; Zhang, G.; Nuyts, J.; De Witte, P.; Zhang, J.; Yu, J.; et al. Sequential Systemic Administrations of Combretastatin A4 Phosphate and Radioiodinated Hypericin Exert Synergistic Targeted Theranostic Effects with Prolonged Survival on SCID Mice Carrying Bifocal Tumor Xenografts. Theranostics 2013, 3, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Abma, E. Ugent Is Looking for Dogs with Malignant Tumors. Available online: https://www.dierenartsenwereld.be/nl/nieuws-n2/ugent-zoekt-honden-met-kwaadaardige-tumoren-i171/ (accessed on 1 January 2020).
- OncoCiDia Phase 0 Study (3M150468). Available online: https://www.kuleuven.be/onderzoek/portaal/#/projecten/3M150468?hl=en&lang=en (accessed on 1 January 2020).
- Abma, E.; Daminet, S.; Smets, P.; Ni, Y.; de Rooster, H. Combretastatin A4-phosphate and its potential in veterinary oncology: A review. Vet. Comp. Oncol. 2017, 15, 184–193. [Google Scholar] [CrossRef] [Green Version]
- Abma, E.; Smets, P.; Daminet, S.; Cornelis, I.; De Clercq, K.; Ni, Y.; Vlerick, L.; de Rooster, H. A dose-escalation study of Combretastatin A4-phosphate in healthy dogs. Vet. Comp. Oncol. 2018, 16, E16–E22. [Google Scholar] [CrossRef] [Green Version]
- Abma, E.; De Spiegelaere, W.; Vanderperren, K.; Stock, E.; Van Brantegem, L.; Cornelis, I.; Daminet, S.; Ni, Y.; Vynck, M.; Verstraete, G.; et al. A single dose of intravenous combretastatin A4-phosphate is reasonably well tolerated and significantly reduces tumour vascularisation in canine spontaneous cancers. Vet. Comp. Oncol. 2018, 16, 467–477. [Google Scholar] [CrossRef]
- Abma, E.; Peremans, K.; De Vos, F.; Bosmans, T.; Kitshoff, A.M.; Daminet, S.; Ni, Y.; Dockx, R.; De Rooster, H. Biodistribution and tolerance of intravenous iodine-131-labelled hypericin in healthy dogs. Vet. Comp. Oncol. 2018, 16, 318–323. [Google Scholar] [CrossRef]
- Aaltonen, L.A.; Hamilton, S.R. Pathology and Genetics of Tumours of the Digestive System; IARC Press Lyon: Oxford, UK, 2000. [Google Scholar]
- Liu, Y.; Yin, T.; De Keyzer, F.; Feng, Y.; Chen, F.; Liu, J.; Song, S.; Yu, J.; Vandecaveye, V.; Swinnen, J.; et al. Micro-HCCs in rats with liver cirrhosis: paradoxical targeting effects with vascular disrupting agent CA4P. Oncotarget 2017, 8, 55204–55215. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; De Keyzer, F.; Wang, Y.; Wang, F.; Feng, Y.; Chen, F.; Yu, J.; Liu, J.; Song, S.; Swinnen, J.; et al. The first study on therapeutic efficacies of a vascular disrupting agent CA4P among primary hepatocellular carcinomas with a full spectrum of differentiation and vascularity: Correlation of MRI-microangiography-histopathology in rats. Int. J. Cancer 2018, 143, 1817–1828. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.-W.; De Keyzer, F.; Feng, Y.-B.; Chen, F.; Song, S.-L.; Swinnen, J.; Bormans, G.; Oyen, R.; Huang, G.; Ni, Y.-C. Intra-individual comparison of therapeutic responses to vascular disrupting agent CA4P between rodent primary and secondary liver cancers. World J. Gastroenterol. 2018, 24, 2710–2721. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Guan, Q.; Kong, X.; De Keyzer, F.; Feng, Y.; Chen, F.; Yu, J.; Liu, J.; Song, S.; Van Pelt, J.; et al. Predicting Therapeutic Efficacy of Vascular Disrupting Agent CA4P in Rats with Liver Tumors by Hepatobiliary Contrast Agent Mn-DPDP-Enhanced MRI. Transl. Oncol. 2020, 13, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Grosios, K.; E Holwell, S.; McGown, A.T.; Pettit, G.R.; Bibby, M.C. In vivo and in vitro evaluation of combretastatin A-4 and its sodium phosphate prodrug. Br. J. Cancer 1999, 81, 1318–1327. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Li, J.; Chen, F.; De Keyzer, F.; Yu, J.; Feng, Y.; Nuyts, J.; Marchal, G.; Ni, Y. Morphological, functional and metabolic imaging biomarkers: assessment of vascular-disrupting effect on rodent liver tumours. Eur. Radiol. 2010, 20, 2013–2026. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Van De Putte, M.; Chen, F.; De Keyzer, F.; Jin, L.; Yu, J.; Marchal, G.; De Witte, P.; Ni, Y. Murine liver implantation of radiation-induced fibrosarcoma: characterization with MR imaging, microangiography and histopathology. Eur. Radiol. 2008, 18, 1422–1430. [Google Scholar] [CrossRef]
- Wang, H.; Sun, X.; Chen, F.; De Keyzer, F.; Yu, J.; Landuyt, W.; Vandecaveye, V.; Peeters, R.; Bosmans, H.; Hermans, R.; et al. Treatment of rodent liver tumor with combretastatin a4 phosphate: noninvasive therapeutic evaluation using multiparametric magnetic resonance imaging in correlation with microangiography and histology. Investig. Radiol. 2009, 44, 44–53. [Google Scholar] [CrossRef]
- Wang, H.; Marchal, G.; Ni, Y. Multiparametric MRI biomarkers for measuring vascular disrupting effect on cancer. World J. Radiol. 2011, 3, 1–16. [Google Scholar] [CrossRef]
- Ni, Y.; Marchal, G.; Van Damme, B.; Van Hecke, P.; Michiels, J.; Zhang, X.; Yu, J.; Baert, A.L. Magnetic Resonance Imaging, Microangiography, and Histology in a Rat Model of Primary Liver Cancer. Investig. Radiol. 1992, 27, 689–697. [Google Scholar] [CrossRef]
- Ni, Y.; Marchal, G. Enhanced magnetic resonance imaging for tissue characterization of liver abnormalities with hepatobiliary contrast agents: an overview of preclinical animal experiments. Top. Magn. Reson. Imaging 1998, 9, 183. [Google Scholar] [CrossRef]
- Ni, Y.; Wang, H.; Chen, F.; Li, J.; Dekeyzer, F.; Feng, Y.; Yu, J.; Bosmans, H.; Marchal, G. Tumor models and specific contrast agents for small animal imaging in oncology. Methods 2009, 48, 125–138. [Google Scholar] [CrossRef]
- Ni, Y.; Marchal, G.; Yu, J.; Mühler, A.; Lukito, G.; Baert, A.L. Prolonged positive contrast enhancement with Gd-EOB-DTPA in experimental liver tumors: Potential value in tissue characterization. J. Magn. Reson. Imaging 1994, 4, 355–363. [Google Scholar] [CrossRef]
- Galbraith, S.M.; Maxwell, R.J.; Lodge, M.A.; Tozer, G.M.; Wilson, J.; Taylor, N.J.; Stirling, J.J.; Sena, L.; Padhani, A.R.; Rustin, G.J. Combretastatin A4 Phosphate Has Tumor Antivascular Activity in Rat and Man as Demonstrated by Dynamic Magnetic Resonance Imaging. J. Clin. Oncol. 2003, 21, 2831–2842. [Google Scholar] [CrossRef]
- Zhao, D.; Richer, E.; Antich, P.P.; Mason, R.P. Antivascular effects of combretastatin A4 phosphate in breast cancer xenograft assessed using dynamic bioluminescence imaging (BLI) and confirmed by magnetic resonance imaging (MRI). Fed. Am. Soc. Exp. Biol. 2008, 22, 2445–2451. [Google Scholar] [PubMed]
- Beauregard, D.A.; Pedley, R.B.; Hill, S.A.; Brindle, K.M. Differential sensitivity of two adenocarcinoma xenografts to the anti-vascular drugs combretastatin A4 phosphate and 5,6-dimethylxanthenone-4-acetic acid, assessed using MRI and MRS. NMR Biomed. 2002, 15, 99–105. [Google Scholar] [CrossRef] [Green Version]
- Sun, X.; Wang, H.; Chen, F.; De Keyzer, F.; Yu, J.; Jiang, Y.; Feng, Y.; Li, J.; Marchal, G.; Ni, Y. Diffusion-weighted MRI of hepatic tumor in rats: Comparison between in vivo and postmortem imaging acquisitions. J. Magn. Reson. Imaging 2009, 29, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Cona, M.M.; Chen, F.; Yu, J.; Feng, Y.; Li, J.; De Keyzer, F.; Marchal, G.; Ni, Y. Comparison of two vascular-disrupting agents at a clinically relevant dose in rodent liver tumors with multiparametric magnetic resonance imaging biomarkers: Anticancer. Drugs 2012, 23, 12–21. [Google Scholar] [CrossRef]
- Thoeny, H.C.; De Keyzer, F.; Chen, F.; Vandecaveye, V.; Verbeken, E.K.; Ahmed, B.; Sun, X.; Ni, Y.; Bosmans, H.; Hermans, R.; et al. Diffusion-Weighted Magnetic Resonance Imaging Allows Noninvasive In Vivo Monitoring of the Effects of Combretastatin A-4 Phosphate after Repeated Administration. Neoplasia 2005, 7, 779–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Yin, T.; Feng, Y.; Cona, M.M.; Huang, G.; Liu, J.; Song, S.; Jiang, Y.; Xia, Q.; Swinnen, J.V.; et al. Mammalian models of chemically induced primary malignancies exploitable for imaging-based preclinical theragnostic research. Quant. Imaging Med. Surg. 2015, 5, 708–729. [Google Scholar]
- Yang, F.-C.; Zheng, S.-S.; Jiang, T.-A. A modified rat model for hepatocellular carcinoma. Hepatobiliary Pancreat. Dis. Int. 2004, 3, 585–587. [Google Scholar]
- Lee, J.-S.; Chu, I.-S.; Mikaelyan, A.; Calvisi, D.F.; Heo, J.; Reddy, J.K.; Thorgeirsson, S.S. Application of comparative functional genomics to identify best-fit mouse models to study human cancer. Nat. Genet. 2004, 36, 1306–1311. [Google Scholar] [CrossRef]
- Maier, K.P. Cirrhosis of the liver as a precancerous condition. Praxis 1998, 87, 1462–1465. [Google Scholar] [PubMed]
- Schlageter, M.; Terracciano, L.M.; D’Angelo, S.; Sorrentino, P. Histopathology of hepatocellular carcinoma. World J. Gastroenterol. 2014, 20, 15955–15964. [Google Scholar] [CrossRef] [PubMed]
- Shaohua, L.; Qiaoxuan, W.; Peng, S.; Qing, L.; Zhongyuan, Y.; Ming, S.; Wei, W.; Rongping, G. Surgical Strategy for Hepatocellular Carcinoma Patients with Portal/Hepatic Vein Tumor Thrombosis. PLoS ONE 2015, 10, e0130021. [Google Scholar] [CrossRef]
- Liu, Y.W.; Yin, T.; Chen, F.; Yu, J.; Liu, J.J.; Song, S.L.; Himmelreich, U.; Oyen, R.; Huang, G.; Ni, Y. Rodent hepatocellular carcinoma cells found in hepatic veins do not necessarily colonize the Lung: Observations in line with the “Seed and Soil” hypothesis. SM Liver J. 2016, 1, 1003. [Google Scholar]
- Subbiah, I.M.; Lenihan, D.J.; Tsimberidou, A.M. Cardiovascular Toxicity Profiles of Vascular-Disrupting Agents. Oncologist 2011, 16, 1120–1130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ni, Y.; Marchal, G.; Zhang, X.; Van Hecke, P.; Michiels, J.; Yu, J.; Rummeny, E.; Lodemann, K.-P.; Baert, A.L. The Uptake of Manganese Dipyridoxal-Diphosphate by Chemically Induced Hepatocellular Carcinoma in Rats; A Correlation between Contrast-Media-Enhanced Magnetic Resonance Imaging, Tumor Differentiation, and Vascularization. Investig. Radiol. 1993, 28, 520–527. [Google Scholar] [CrossRef]
- Ni, Y.; Marchal, G.; Yu, J.; Rummeny, E.; Zhang, X.; Lodemann, K.P.; Baert, A.L. Experimental liver cancers: Mn-DPDP-enhanced rims in MR-microangiographic-histologic correlation study. Radiology 1993, 188, 45–51. [Google Scholar] [CrossRef]
- Yang, Z.F.; Poon, R.T.P. Vascular changes in hepatocellular carcinoma. Anat. Rec. Hoboken NJ 2008, 291, 721–734. [Google Scholar] [CrossRef]
- Feng, Y.; Cona, M.M.; Vunckx, K.; Li, Y.; Chen, F.; Nuyts, J.; Gheysens, O.; Zhou, L.; Xie, Y.; Oyen, R.; et al. Detection and quantification of acute reperfused myocardial infarction in rabbits using DISA-SPECT/CT and 3.0T cardiac MRI. Int. J. Cardiol. 2013, 168, 4191–4198. [Google Scholar] [CrossRef]
- Tomino, T.; Yamashita, Y.-I.; Iguchi, T.; Itoh, S.; Ninomiya, M.; Ikegami, T.; Yoshizumi, T.; Soejima, Y.; Kawanaka, H.; Ikeda, T.; et al. Spontaneous massive necrosis of hepatocellular carcinoma with narrowing and occlusion of the arteries and portal veins. Case Rep. Gastroenterol. 2014, 8, 148–155. [Google Scholar] [CrossRef]
- Nouso, K.; Uematsu, S.; Shiraga, K.; Okamoto, R.; Harada, R.; Takayama, S.; Kawai, W.; Kimura, S.; Ueki, T.; Okano, N.; et al. Regression of hepatocellular carcinoma during vitamin K administration. World J. Gastroenterol. 2005, 11, 6722–6724. [Google Scholar] [CrossRef] [PubMed]
- Gryspeerdt, S.; Van Hoe, L.; Marchal, G.; Baert, A.L. Evaluation of hepatic perfusion disorders with double-phase spiral CT. Radiographics 1997, 17, 337–348. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Luo, Y.; Peng, Y.-L.; Cai, W.; Lu, Q.; Lin, L.; Sha, X.-X.; Li, Y.-Z.; Zhu, M. Hepatic Perfusion Disorder Associated with Focal Liver Lesions: Contrast-enhanced US Patterns—Correlation Study with Contrast-enhanced CT. Radiology 2011, 260, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; Sun, X.; De Keyzer, F.; Yu, J.; Peeters, R.; Coudyzer, W.; Vandecaveye, V.; Bosmans, H.; Van Hecke, P.; Landuyt, W.; et al. Rodent liver tumor model with implanted rhabdomyosarcoma: characterization with MR imaging, microangiography and histopathologic analysis. Radiology 2006, 239, 554–562. [Google Scholar] [CrossRef]
- Stevenson, J.P.; Rosen, M.; Sun, W.; Gallagher, M.; Haller, D.G.; Vaughn, D.; Giantonio, B.; Zimmer, R.; Petros, W.P.; Stratford, M.; et al. Phase I Trial of the Antivascular Agent Combretastatin A4 Phosphate on a 5-Day Schedule to Patients With Cancer: Magnetic Resonance Imaging Evidence for Altered Tumor Blood Flow. J. Clin. Oncol. 2003, 21, 4428–4438. [Google Scholar] [CrossRef]
- Meyer, T.; Gaya, A.M.; Dancey, G.; Stratford, M.R.L.; Othman, S.; Sharma, S.K.; Wellsted, D.; Taylor, N.J.; Stirling, J.J.; Poupard, L.; et al. A phase I trial of radioimmunotherapy with I-131-A5B7 anti-CEA antibody in combination with combretastatin-A4-phosphate in advanced gastrointestinal carcinomas. Clin. Cancer Res. 2009, 15, 4484–4492. [Google Scholar] [CrossRef] [Green Version]
- Nathan, P.; Zweifel, M.; Padhani, A.R.; Koh, D.-M.; Ng, M.; Collins, D.J.; Harris, A.; Carden, C.; Smythe, J.; Fisher, N.; et al. Phase I Trial of Combretastatin A4 Phosphate (CA4P) in Combination with Bevacizumab in Patients with Advanced Cancer. Clin. Cancer Res. 2012, 18, 3428–3439. [Google Scholar] [CrossRef] [Green Version]
- O’Connor, J.P.B.; Jackson, A.; Parker, G.J.M.; Roberts, C.; Jayson, G.C. Dynamic contrast-enhanced MRI in clinical trials of antivascular therapies. Nat. Rev. Clin. Oncol. 2012, 9, 167–177. [Google Scholar] [CrossRef]
- Yin, T.; Liu, Y.; Peeters, R.; Feng, Y.; Yu, J.; Himmelreich, U.; Oyen, R.; Ni, Y. Vascular disrupting agent in pancreatic and hepatic tumour allografts: observations of location-dependent efficacy by MRI, microangiography and histomorphology. Br. J. Cancer 2017, 117, 1529–1536. [Google Scholar] [CrossRef]
- Muhi, A.; Ichikawa, T.; Motosugi, U.; Sano, K.; Matsuda, M.; Kitamura, T.; Nakazawa, T.; Araki, T. High-b-value diffusion-weighted MR imaging of hepatocellular lesions: Estimation of grade of malignancy of hepatocellular carcinoma. J. Magn. Reson. Imaging 2009, 30, 1005–1011. [Google Scholar] [CrossRef]
- Garon, E.B.; Neidhart, J.D.; Gabrail, N.Y.; De Oliveira, M.R.; Balkissoon, J.; Kabbinavar, F. A randomized Phase II trial of the tumor vascular disrupting agent CA4P (fosbretabulin tromethamine) with carboplatin, paclitaxel, and bevacizumab in advanced nonsquamous non-small-cell lung cancer. OncoTargets Ther. 2016, 9, 7275–7283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sosa, J.A.; Elisei, R.; Jarzab, B.; Balkissoon, J.; Lu, S.; Bal, C.; Marur, S.; Gramza, A.; Yosef, R.B.; Gitlitz, B.; et al. Randomized Safety and Efficacy Study of Fosbretabulin with Paclitaxel/Carboplatin Against Anaplastic Thyroid Carcinoma. Thyroid 2013, 24, 232–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, T.; Murata, R.; Maxwell, R.J.; Stødkilde-Jørgensen, H.; Østergaard, L.; Ley, C.D.; Kristjansen, P.E.G.; Horsman, M.R. Non-invasive imaging of combretastatin activity in two tumor models: Association with invasive estimates. Acta Oncol. 2010, 49, 906–913. [Google Scholar] [CrossRef] [PubMed]
- Landuyt, W.; Verdoes, O.; O Darius, D.; Drijkoningen, M.; Nuyts, S.; Theys, J.; Stockx, L.; Wynendaele, W.; Fowler, J.F.; Maleux, G.; et al. Vascular targeting of solid tumours: a major ’inverse’ volume-response relationship following combretastatin A-4 phosphate treatment of rat rhabdomyosarcomas. Eur. J. Cancer 2000, 36, 1833–1843. [Google Scholar] [CrossRef]
- Siemann, D.W.; Rojiani, A.M. The vascular disrupting agent ZD6126 shows increased antitumor efficacy and enhanced radiation response in large, advanced tumors. Int. J. Radiat. Oncol. 2005, 62, 846–853. [Google Scholar] [CrossRef]
- Dong, Y.-H.; Lin, G. Experimental Studies of Portal Venous Embolization with Iodized Oil in Rats with Experimentally Induced Liver Cancer. J. Vasc. Interv. Radiol. 1993, 4, 621–624. [Google Scholar] [CrossRef]
- Wang, S.; Liu, Y.; Feng, Y.; Zhang, J.; Swinnen, J.; Li, Y.; Ni, Y. A Review on Curability of Cancers: More Efforts for Novel Therapeutic Options Are Needed. Cancers 2019, 11, 1782. [Google Scholar] [CrossRef] [Green Version]
- Hu, Z.; Ding, J.; Ma, Z.; Sun, R.; Seoane, J.A.; Shaffer, J.S.; Suarez, C.J.; Berghoff, A.S.; Cremolini, C.; Falcone, A.; et al. Quantitative evidence for early metastatic seeding in colorectal cancer. Nat. Genet. 2019, 51, 1113–1122. [Google Scholar] [CrossRef]
- Xu, R.-H.; Wei, W.; Krawczyk, M.; Wang, W.; Luo, H.; Flagg, K.; Yi, S.; Shi, W.; Quan, Q.; Li, K.; et al. Circulating tumour DNA methylation markers for diagnosis and prognosis of hepatocellular carcinoma. Nat. Mater. 2017, 16, 1155–1161. [Google Scholar] [CrossRef]
- Li, J.; Chen, F.; Feng, Y.; Cona, M.M.; Yu, J.; Verbruggen, A.; Zhang, J.; Oyen, R.; Ni, Y. Diverse Responses to Vascular Disrupting Agent Combretastatin A4 Phosphate: A Comparative Study in Rats with Hepatic and Subcutaneous Tumor Allografts Using MRI Biomarkers, Microangiography, and Histopathology. Transl. Oncol. 2013, 6, 42–50. [Google Scholar] [CrossRef] [Green Version]
- Tozer, G.M.; Kanthou, C.; Lewis, G.; E Prise, V.; Vojnovic, B.; A Hill, S. Tumour vascular disrupting agents: combating treatment resistance. Br. J. Radiol. 2008, 81, S12–S20. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.-Y.; Ma, W.; Gurung, K.; Guo, C.-H. Mechanisms of tumor resistance to small-molecule vascular disrupting agents: Treatment and rationale of combination therapy. J. Formos. Med. Assoc. 2013, 112, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Abbas, H.; Chang, B.; Chen, Z.J. Motion management in gastrointestinal cancers. J. Gastrointest. Oncol. 2014, 5, 223–235. [Google Scholar] [PubMed]
- Rohrer, M.; Bauer, H.; Mintorovitch, J.; Requardt, M.; Weinmann, H.-J. Comparison of magnetic properties of MRI contrast media solutions at different magnetic field strengths. Investig. Radiol. 2005, 40, 715–724. [Google Scholar] [CrossRef] [Green Version]
- Gale, E.M.; Jones, C.M.; Ramsay, I.; Farrar, C.T.; Caravan, P. A Janus Chelator Enables Biochemically Responsive MRI Contrast with Exceptional Dynamic Range. J. Am. Chem. Soc. 2016, 138, 15861–15864. [Google Scholar] [CrossRef] [Green Version]
- Takakura, K.; Oikawa, T.; Tomita, Y.; Mizuno, Y.; Nakano, M.; Saeki, C.; Torisu, Y.; Saruta, M. Mouse models for investigating the underlying mechanisms of nonalcoholic steatohepatitis-derived hepatocellular carcinoma. World J. Gastroenterol. 2018, 24, 1989–1994. [Google Scholar] [CrossRef]
- Febbraio, M.A.; Reibe, S.; Shalapour, S.; Ooi, G.J.; Watt, M.J.; Karin, M. Preclinical Models for Studying NASH-Driven HCC: How Useful Are They? Cell Metab. 2019, 29, 18–26. [Google Scholar] [CrossRef] [Green Version]
- Lou, J.; Zhang, L.; Lv, S.; Zhang, C.; Jiang, S. Biomarkers for Hepatocellular Carcinoma. Biomark. Cancer 2017, 9, 1–9. [Google Scholar] [CrossRef]
- Cona, M.M.; Koole, M.; Feng, Y.; Liu, Y.; Verbruggen, A.; Oyen, R.; Ni, Y. Biodistribution and radiation dosimetry of radioiodinated hypericin as a cancer therapeutic. Int. J. Oncol. 2014, 44, 819–829. [Google Scholar] [CrossRef] [Green Version]
- Cona, M.M.; Alpizar, Y.A.; Li, J.; Bauwens, M.; Feng, Y.; Sun, Z.; Zhang, J.; Chen, F.; Talavera, K.; de Witte, P.; et al. Radioiodinated hypericin: its biodistribution, necrosis avidity and therapeutic efficacy are influenced by formulation. Pharm. Res. 2014, 31, 278–290. [Google Scholar] [CrossRef]
- Ni, Y.; Huyghe, D.; Verbeke, K.; De Witte, P.A.; Nuyts, J.; Mortelmans, L.; Chen, F.; Marchal, G.; Verbruggen, A.M.; Bormans, G.M. First preclinical evaluation of mono-[123I]iodohypericin as a necrosis-avid tracer agent. Eur. J. Nucl. Med. Mol. Imaging 2006, 33, 595–601. [Google Scholar] [CrossRef] [PubMed]
- Fonge, H.; Vunckx, K.; Wang, H.; Feng, Y.; Mortelmans, L.; Nuyts, J.; Bormans, G.; Verbruggen, A.; Ni, Y. Non-invasive detection and quantification of acute myocardial infarction in rabbits using mono-[123I]iodohypericin microSPECT. Eur. Heart J. 2008, 29, 260–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, S.; Xiong, C.; Zhou, M.; Lu, W.; Huang, Q.; Ku, G.; Zhao, J.; Flores, L.G.; Ni, Y.; Li, C. Small-Animal PET of Tumor Damage Induced by Photothermal Ablation with 64Cu-Bis-DOTA-Hypericin. J. Nucl. Med. 2011, 52, 792–799. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.-W.; Yin, T.; Feng, Y.-B.; Chen, F.; Yu, J.; Liu, J.-J.; Song, S.-L.; Himmelreich, U.; Oyen, R.; Huang, G.; et al. In vivo anticancer efficacy assessment with an imaging-based platform: taking Brucea Javanica oil emulsion as an example. J. Unexplored Med. Data 2016, 1, 19–27. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lower Dose [26] | Higher Dose [24,25] | p Value * | |
|---|---|---|---|
| Animal number | |||
| Recruited rats | 16 | 30 | |
| Lost rats during induction | 0 | 5 | |
| DENA toxicity | 0 | 3 | |
| Tumor hemorrhage | 0 | 2 | |
| Protocol of gavage | |||
| DENA dose (mg/kg/day) | 5 | 10 | |
| DENA exposure period (week) | 14 | 8 | |
| Period of carcinogenesis (week) | |||
| Recognizable nodule (Ø > 1mm) | 16–23 | 7–11 | |
| Ready for CA4P therapy (maximum Ø ≥ 8 mm) | 21–31 | 14–22 | |
| Tumor number | 61 | 108 | |
| Primary HCC lesion (89.9%) | 56 | 96 | |
| HCC differentiation § | <0.0001 | ||
| Well-differentiated (a) | 15 (26.8%) | 12 (12.5%) | |
| Moderately-differentiated (b) | 26 (46.4%) | 28 (29.2%) | |
| Poorly-differentiated (c) | 13 (23.2%) | 44 (45.8%) | |
| Undifferentiated (d) | 2 (3.6%) | 12 (12.5%) | |
| (a + b) vs (c + d) | 73.2% vs 26.8% | 41.7% vs 58.3% | <0.0001 |
| Tumoral vascularity ¶ | =0.1256 | ||
| + | 34 (60.7%) | 41 (42.7%) | |
| ++ | 13 (23.2%) | 26 (27.1%) | |
| +++ | 7 (12.5%) | 19 (19.8%) | |
| ++++ (angioma-like HCCs) | 2 (3.6%) | 10 (10.4%) | |
| Primary ICC (2.4%) | 0 | 4 | |
| Combined HCC-ICC (7.7%) | 5 | 8 | |
| Liver cirrhosis | slightly | moderate - severe |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Y.; Wang, S.; Zhao, X.; Feng, Y.; Bormans, G.; Swinnen, J.; Oyen, R.; Huang, G.; Ni, Y.; Li, Y. Predicting Clinical Efficacy of Vascular Disrupting Agents in Rodent Models of Primary and Secondary Liver Cancers: An Overview with Imaging-Histopathology Correlation. Diagnostics 2020, 10, 78. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10020078
Liu Y, Wang S, Zhao X, Feng Y, Bormans G, Swinnen J, Oyen R, Huang G, Ni Y, Li Y. Predicting Clinical Efficacy of Vascular Disrupting Agents in Rodent Models of Primary and Secondary Liver Cancers: An Overview with Imaging-Histopathology Correlation. Diagnostics. 2020; 10(2):78. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10020078
Chicago/Turabian StyleLiu, Yewei, Shuncong Wang, Xiaohui Zhao, Yuanbo Feng, Guy Bormans, Johan Swinnen, Raymond Oyen, Gang Huang, Yicheng Ni, and Yue Li. 2020. "Predicting Clinical Efficacy of Vascular Disrupting Agents in Rodent Models of Primary and Secondary Liver Cancers: An Overview with Imaging-Histopathology Correlation" Diagnostics 10, no. 2: 78. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10020078