Breast Cancer Detection—A Synopsis of Conventional Modalities and the Potential Role of Microwave Imaging


Abstract
:1. Introduction
- Mammography and digital breast tomosynthesis exploit the attenuation of x-rays as they pass through breast tissue measured by the attenuation coefficient of the tissue;
- Magnetic resonance imaging uses radio waves, magnetic field gradients, and contrast agents to excite and measure the location of hydrogen atoms;
- Ultrasound exploits differences in acoustic impedance between tissue types as sound waves propagate in the breast.
2. Mammography
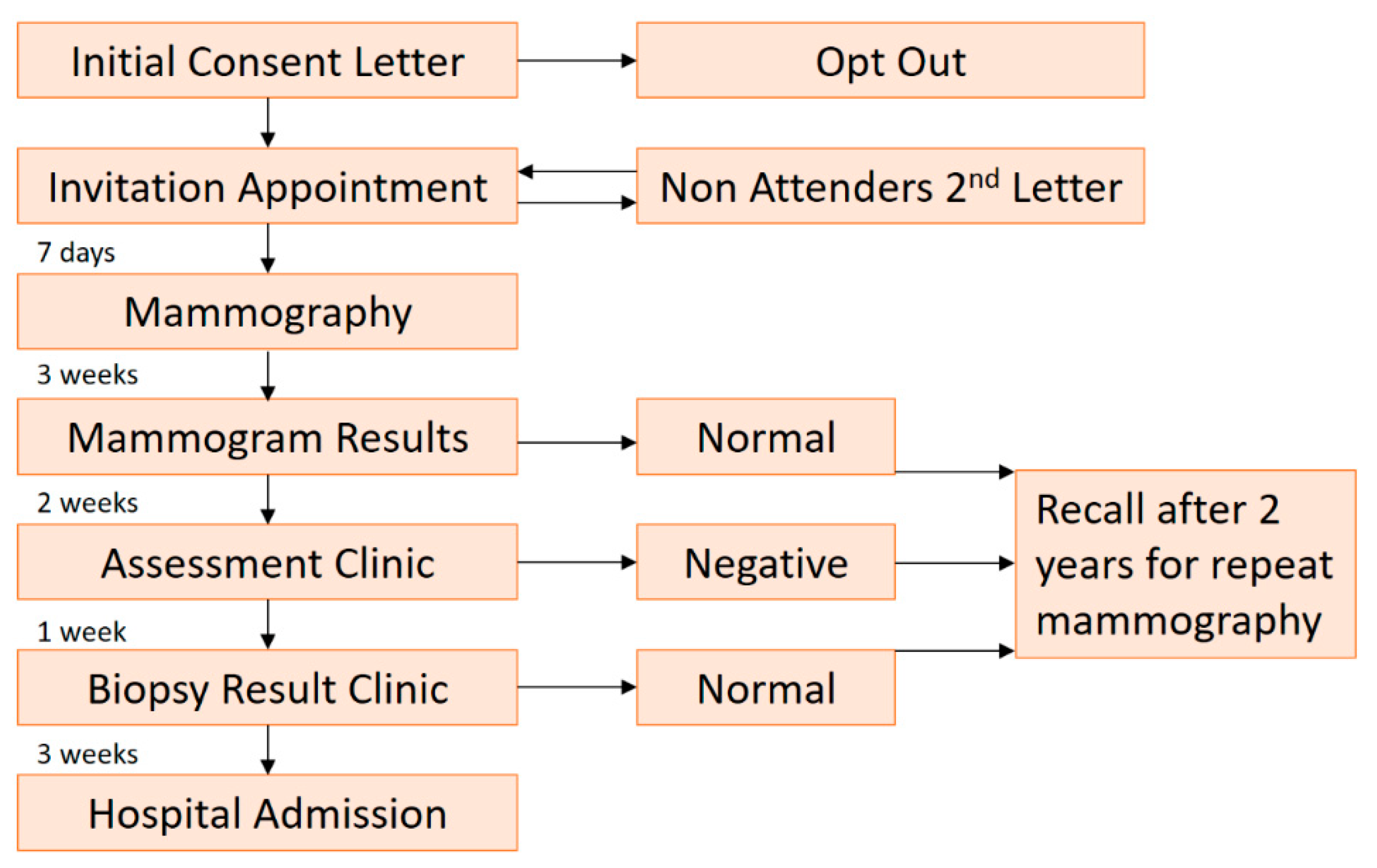
2.1. Screening Mammography
2.2. Symptomatic Breast Mammography
3. Digital Breast Tomosynthesis (DBT)
4. Breast Sonography
5. Magnetic Resonance Imaging (MRI)
6. Microwave Breast Imaging (MBI)
- Respective beam widths of the transducer and the antennas;
- The relative dielectric properties and acoustic properties of the tissues of interest which is not well-studied;
- Importance of contact between the skin and the transducer and the antenna.
7. Prospects for Microwave Breast Imaging
Author Contributions
Funding
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Feuer, EJ.; Wun, L.M.; Boring, C.C.; Flanders, W.D.; Timmel, M.J.; Tong, T. The lifetime risk of developing breast cancer. J. Natl. Cancer Inst. 1993, 85, 892–897. [Google Scholar] [CrossRef] [PubMed]
- Levi, F.; Bosetti, C.; Lucchini, F.; Negri, E.; La Vecchia, C. Monitoring the decrease in breast cancer mortality in Europe. Eur. J. Cancer Prev. 2005, 14, 497–502. [Google Scholar] [CrossRef] [PubMed]
- Myers, E.R.; Moorman, P.; Gierisch, J.M.; Havrilesky, L.J.; Grimm, L.J.; Ghate, S.; Davidson, B.; Mongtomery, R.C.; Crowley, M.J.; McCrory, D.C.; et al. Benefits and Harms of Breast Cancer Screening: A Systematic Review. JAMA 2015, 314, 1615–1634. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2016. CA Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef] [Green Version]
- Gold, R.H.; Bassett, L.W.; Widoff, B.E. Highlights from the history of mammography. Radiographics 1990, 10, 1111–1131. [Google Scholar] [CrossRef] [Green Version]
- Warren, S.L. A Roentgenologic Study of the Breast. Am. J. Roentgenol. 1930, 24, 113–124. [Google Scholar]
- Keemers-Gels, M.E.; Groenendijk, R.P.; van den Heuvel, J.H.; Boetes, C.; Peer, P.G.; Wobbes, T.H. Pain experienced by women attending breast cancer screening. Breast Cancer Res. Treat. 2000, 60, 235–240. [Google Scholar] [CrossRef]
- Bartella, L.; Smith, C.S.; Dershaw, D.D.; Liberman, L. Imaging breast cancer. Radiol. Clin. North Am. 2007, 45, 45–67. [Google Scholar] [CrossRef]
- Walter, L.C.; Schonberg, M.A. Screening mammography in older women: A review. JAMA 2014, 311, 1336–1347. [Google Scholar] [CrossRef]
- Drukteinis, J.S.; Mooney, B.P.; Flowers, C.I.; Gatenby, R.A. Beyond mammography: New frontiers in breast cancer screening. Am. J. Med. 2013, 126, 472–479. [Google Scholar] [CrossRef] [PubMed]
- Autier, P.; Hery, C.; Haukka, J.; Boniol, M.; Byrnes, G. Advanced breast cancer and breast cancer mortality in randomized controlled trials on mammography screening. J. Clin. Oncol. 2009, 27, 5919–5923. [Google Scholar] [CrossRef] [PubMed]
- Weedon-Fekjaer, H.; Romundstad, P.R.; Vatten, L.J. Modern mammography screening and breast cancer mortality: Population study. BMJ 2014, 348, g3701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shapiro, S. Periodic screening for breast cancer: The HIP Randomized Controlled Trial. Health Insurance Plan. J. Natl. Cancer Inst. Monogr. 1997, 22, 27–30. [Google Scholar] [CrossRef]
- Tabár, L.; Vitak, B.; Chen, H.H.; Duffy, S.W.; Yen, M.F.; Chiang, C.F.; Krusemo, U.B.; Tot, T.; Smith, R.A. The Swedish Two-County Trial twenty years later. Updated mortality results and new insights from long-term follow-up. Radiol. Clin. North Am. 2000, 38, 625–651. [Google Scholar] [CrossRef]
- Andersson, I.; Nystrom, L. Mammography screening. J. Natl. Cancer Inst. 1995, 87, 1263–1264. [Google Scholar]
- Nystrom, L.; Andersson, I.; Bjurstam, N.; Frisell, J.; Nordenskjold, B.; Rutqvist, L.E. Long-term effects of mammography screening: Updated overview of the Swedish randomised trials. Lancet 2002, 359, 909–919. [Google Scholar] [CrossRef]
- Bjurstam, N.; Bjorneld, L.; Warwick, J.; Sala, E.; Duffy, S.W.; Nystrom, L.; Walker, N.; Cahlin, E.; Eriksson, O.; Hafstrom, L.O.; et al. The Gothenburg Breast Screening Trial. Cancer 2003, 97, 2387–2396. [Google Scholar] [CrossRef]
- Miller, A.B.; To, T.; Baines, C.J.; Wall, C. The Canadian National Breast Screening Study-1: Breast cancer mortality after 11 to 16 years of follow-up. A randomized screening trial of mammography in women age 40 to 49 years. Ann. Intern. Med. 2002, 137, 305–312. [Google Scholar] [CrossRef] [Green Version]
- Miller, A.B.; To, T.; Baines, C.J.; Wall, C. Canadian National Breast Screening Study-2: 13-year results of a randomized trial in women aged 50–59 years. J. Natl. Cancer Inst. 2000, 92, 1490–1499. [Google Scholar] [CrossRef]
- Moss, S.M.; Cuckle, H.; Evans, A.; Johns, L.; Waller, M.; Bobrow, L. Effect of mammographic screening from age 40 years on breast cancer mortality at 10 years’ follow-up: A randomised controlled trial. Lancet 2006, 368, 2053–2060. [Google Scholar] [CrossRef]
- Early Breast Cancer Trialists’ Collaborative Group. Effects of adjuvant tamoxifen and of cytotoxic therapy on mortality in early breast cancer. An overview of 61 randomized trials among 28,896 women. New Engl. J. Med. 1988, 319, 1681–1692. [Google Scholar] [CrossRef] [PubMed]
- Bleyer, A.; Welch, H.G. Effect of three decades of screening mammography on breast-cancer incidence. New Engl. J. Med. 2012, 367, 1998–2005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gotzsche, P.C.; Nielsen, M. Screening for breast cancer with mammography. Cochrane Database Syst. Rev. 2006, 6, CD001877. [Google Scholar]
- Biller-Andorno, N.; Juni, P. Abolishing mammography screening programs? A view from the Swiss Medical Board. New Engl. J. Med. 2014, 370, 1965–1967. [Google Scholar] [CrossRef] [Green Version]
- Swiss Medical Board stellt systematisches Mammographie-Screening in Frage. Bulletin des médecins suisses 2014, 95, 196.
- De Koning, H.J.; Heijnsdijk, E.A. Swiss Medical Board Mammography screening predictions for Switzerland: Importance of time-periods. J. Med. Screen. 2015, 22, 201–206. [Google Scholar] [CrossRef]
- Independent UK Panel on Breast Cancer Screening. The benefits and harms of breast cancer screening: An independent review. Lancet 2012, 380, 1778–1786. [Google Scholar] [CrossRef]
- Nelson, H.D.; O’Meara, E.S.; Kerlikowske, K.; Balch, S.; Miglioretti, D. Factors Associated With Rates of False-Positive and False-Negative Results From Digital Mammography Screening: An Analysis of Registry Data. Ann. Intern. Med. 2016, 164, 226–235. [Google Scholar] [CrossRef]
- US Preventive Services Task Force. Screening for breast cancer: U.S. Preventive Services Task Force recommendation statement. Ann. Intern. Med. 2009, 151, 716. [Google Scholar] [CrossRef] [Green Version]
- BreastCheck. Annual Report 2017/8. Available online: https://www.breastcheck.ie/content/annual_reports (accessed on 1 November 2019).
- Hanley, J.A.; Hannigan, A.; O’Brien, K.M. Mortality reductions due to mammography screening: Contemporary population-based data. PLoS ONE 2017, 12, e0188947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Health Information and Quality Authority. National Quality Assurance Standards for Symptomatic Breast Disease Services; HIQA: Dublin, Ireland, 2006. [Google Scholar]
- Helvie, M.A. Digital mammography imaging: Breast tomosynthesis and advanced applications. Radiol. Clin. North Am. 2010, 48, 917–929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pattacini, P.; Nitrosi, A.; Giorgi Rossi, P.; Iotti, V.; Ginocchi, V.; Ravaioli, S.; Vacondio, R.; Braglia, L.; Cavuto, S.; Campari, C. Digital Mammography versus Digital Mammography Plus Tomosynthesis for Breast Cancer Screening: The Reggio Emilia Tomosynthesis Randomized Trial. Radiology 2018, 288, 375–385. [Google Scholar] [CrossRef] [PubMed]
- Houssami, N.; Irwig, L.; Simpson, J.M.; McKessar, M.; Blome, S.; Noakes, J. Sydney Breast Imaging Accuracy Study: Comparative sensitivity and specificity of mammography and sonography in young women with symptoms. AJR Am. J. Roentgenol. 2003, 180, 935–940. [Google Scholar] [CrossRef]
- Weinstein, S.P.; Conant, E.F.; Sehgal, C. Technical Advances in Breast Ultrasound Imaging. Seminars in Ultrasound, CT and MRI 2006, 27, 273–283. [Google Scholar] [CrossRef]
- Joshi, S.; Dialani, V.; Marotti, J.; Mehta, T.S.; Slanetz, P.J. Breast disease in the pregnant and lactating patient: Radiological-pathological correlation. Insights Imaging 2013, 4, 527–538. [Google Scholar] [CrossRef] [Green Version]
- Ciatto, S.; Bravetti, P.; Bonardi, R.; Rosselli del Turco, M. The role of mammography in women under 30. Radiol. Med. 1990, 80, 676–678. [Google Scholar]
- Checka, C.M.; Chun, J.E.; Schnabel, F.R.; Lee, J.; Toth, H. The relationship of mammographic density and age: Implications for breast cancer screening. AJR Am. J. Roentgenol. 2012, 198, W292–W295. [Google Scholar] [CrossRef]
- Pinsky, R.W.; Helvie, M.A. Mammographic breast density: Effect on imaging and breast cancer risk. J. Natl. Compr. Cancer Netw. 2010, 8, 1157–1164. [Google Scholar] [CrossRef]
- Berg, W.A.; Gutierrez, L.; NessAiver, M.S.; Carter, W.B.; Bhargavan, M.; Lewis, R.S.; Ioffe, O.B. Diagnostic accuracy of mammography, clinical examination,, U.S.; and MR imaging in preoperative assessment of breast cancer. Radiology 2004, 233, 830–849. [Google Scholar] [CrossRef]
- Menezes, G.L.; Knuttel, F.M.; Stehouwer, B.L.; Pijnappel, R.M.; van den Bosch, M.A. Magnetic resonance imaging in breast cancer: A literature review and future perspectives. World J. Clin. Oncol. 2014, 5, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Sardanelli, F.; Boetes, C.; Borisch, B.; Decker, T.; Federico, M.; Gilbert, F.J.; Helbich, T.; Heywang-Köbrunner, S.H.; Kaiser, W.A.; Kerin, M.J.; et al. Magnetic resonance imaging of the breast: Recommendations from the EUSOMA working group. Eur. J. Cancer 2010, 46, 1296–1316. [Google Scholar] [CrossRef] [PubMed]
- Garcia, E.M.; Storm, E.S.; Atkinson, L.; Kenny, E.; Mitchell, L.S. Current breast imaging modalities, advances, and impact on breast care. Obstet. Gynecol. Clin. North Am. 2013, 40, 429–457. [Google Scholar] [CrossRef] [PubMed]
- Berg, W.A.; Zhang, Z.; Lehrer, D.; Jong, R.A.; Pisano, E.D.; Barr, R.G.; Böhm-Vélez, M.; Mahoney, M.C.; Evans, W.P., 3rd; Larsen, L.H.; et al. Detection of breast cancer with addition of annual screening ultrasound or a single screening MRI to mammography in women with elevated breast cancer risk. JAMA 2012, 307, 1394–1404. [Google Scholar] [PubMed] [Green Version]
- Bassett, L.W.; Dhaliwal, S.G.; Eradat, J.; Khan, O.; Farria, D.F.; Brenner, R.J.; Sayre, J.W. National trends and practices in breast MRI. AJR Am. J. Roentgenol. 2008, 191, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Turnbull, L.; Brown, S.; Harvey, I.; Olivier, C.; Drew, P.; Napp, V.; Hanby, A.; Brown, J. Comparative effectiveness of MRI in breast cancer (COMICE) trial: A randomised controlled trial. Lancet 2010, 375, 563–571. [Google Scholar] [CrossRef] [Green Version]
- Houssami, N.; Turner, R.M.; Morrow, M. Meta-analysis of pre-operative magnetic resonance imaging (MRI) and surgical treatment for breast cancer. Breast Cancer Res. Treat. 2017, 165, 273–283. [Google Scholar] [CrossRef]
- Brennan, M.E.; Houssami, N.; Lord, S.; Macaskill, P.; Irwig, L.; Dixon, J.M.; Warren, R.M.; Ciatto, S. Magnetic resonance imaging screening of the contralateral breast in women with newly diagnosed breast cancer: Systematic review and meta-analysis of incremental cancer detection and impact on surgical management. J. Clin. Oncol. 2009, 27, 5640–5649. [Google Scholar] [CrossRef] [Green Version]
- Houssami, N.; Hayes, D.F. Review of preoperative magnetic resonance imaging (MRI) in breast cancer: Should MRI be performed on all women with newly diagnosed, early stage breast cancer? CA Cancer J. Clin. 2009, 59, 290–302. [Google Scholar] [CrossRef]
- Morrow, M.; Waters, J.; Morris, E. MRI for breast cancer screening, diagnosis, and treatment. Lancet 2011, 378, 1804–1811. [Google Scholar] [CrossRef]
- Preece, A.W.; Craddock, I.; Shere, M.; Jones, L.; Winton, H.L. MARIA M4: Clinical evaluation of a prototype ultrawideband radar scanner for breast cancer detection. J. Med. Imaging 2016, 3, 033502. [Google Scholar] [CrossRef] [PubMed]
- Meaney, P.M.; Kaufman, P.A.; Muffly, L.S.; Click, M.; Poplack, S.P.; Wells, W.A.; Schwartz, G.N.; di Florio-Alexander, R.M.D.; Tosteson, T.; Li, Z.; et al. Microwave imaging for neoadjuvant chemotherapy monitoring: Initial clinical experience. Breast Cancer Res. 2013, 15, R35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Loughlin, D.; O’Halloran, M.; Moloney, B.M.; Glavin, M.; Jones, E.; Elahi, M.A. Microwave Breast Imaging: Clinical Advances and Remaining Challenges. IEEE Trans. Biomed. Eng. 2018, 65, 2580–2590. [Google Scholar]
- Kwon, S.; Lee, S. Recent Advances in Microwave Imaging for Breast Cancer Detection. Int. J. Biomed. Imaging 2016, 2016, 5054912. [Google Scholar] [CrossRef] [PubMed]
- Larsen, L.; Jacobi, J. Microwaves offer promise as imaging modality. Diagn. Imaging 1982, 11, 44–47. [Google Scholar]
- Golnabi, A.H.; Meaney, P.M.; Epstein, N.R.; Paulsen, K.D. Microwave imaging for breast cancer detection: Advances in three--dimensional image reconstruction. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 5730–5733. [Google Scholar]
- Conceicao, R.C.; Mohr, J.J.; O’Halloran, M. An Introduction to Microwave Imaging for Breast Cancer Detection; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- McIntyre, G.I. Increased cell hydration promotes both tumor growth and metastasis: A biochemical mechanism consistent with genetic signatures. Med. Hypotheses 2007, 69, 1127–1130. [Google Scholar] [CrossRef]
- Modiri, A.; Goudreau, S.; Rahimi, A.; Kiasaleh, K. Review of breast screening: Toward clinical realization of microwave imaging. Med. Phys. 2017, 44, e446–e458. [Google Scholar] [CrossRef]
- Dean, L. Blood Groups and Red Cell Antigens; NCBI: Bethesda, MD, USA, 2005. [Google Scholar]
- Joines, W.T.; Zhang, Y.; Li, C.; Jirtle, R.L. The measured electrical properties of normal and malignant human tissues from 50 to 900 MHz. Med. Phys. 1994, 21, 547–550. [Google Scholar] [CrossRef]
- Meaney, P.M. A clinical prototype for active microwave imaging of the breast. IEEE Trans. Microwave Theory Tech. 2000, 48, 12. [Google Scholar]
- Meaney, P.M.; Fanning, M.W.; Raynolds, T.; Fox, C.J.; Fang, Q.; Kogel, C.A.; Poplack, S.P.; Paulsen, K.D. Initial clinical experience with microwave breast imaging in women with normal mammography. Acad Radiol. 2007, 14, 207–218. [Google Scholar] [CrossRef] [Green Version]
- Poplack, S.P.; Tosteson, T.D.; Wells, W.A.; Pogue, B.W.; Meaney, P.M.; Hartov, A.; Kogel, C.A.; Soho, S.K.; Gibson, J.J.; Paulsen, K.D. Electromagnetic breast imaging: Results of a pilot study in women with abnormal mammograms. Radiology 2007, 243, 350–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poplack, S.P.; Paulsen, K.D.; Hartov, A.; Meaney, P.M.; Pogue, B.W.; Tosteson, T.D.; Grove, M.R.; Soho, S.K.; Wells, W.A. Electromagnetic breast imaging: Average tissue property values in women with negative clinical findings. Radiology 2004, 231, 571–580. [Google Scholar] [CrossRef] [PubMed]
- Massey, H.; Ridley, N.; Lyburn, I. Radiowave Detection of Breast Cancer In The Symptomatic Clinic—A Multi-Centre Study. In Proceedings of the International Cambridge Conference on Breast Imaging, Cambridge, UK, 3–4 July 2017. [Google Scholar]
- Fear, E.C.; Bourqui, J.; Curtis, C.F. Microwave Breast Imaging With a Monostatic Radar-Based System: A Study of Application to Patients. IEEE Trans. Microwave Theory Tech. 2013, 61, 9. [Google Scholar] [CrossRef]
- Kurrant, D.; Bourqui, J.; Fear, E. Surface Estimation for Microwave Imaging. Sensors 2017, 17, 1658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavoie, B.R.; Okoniewski, M.; Fear, E.C. Estimating the Effective Permittivity for Reconstructing Accurate Microwave-Radar Images. PLoS ONE 2016, 11, e0160849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, F.S.L.; Hu, Z. A Large-Scale Clinical Trial of Radarbased Microwave Breast Imaging for Asian Women: Phase, I. In Proceedings of the International Symposium on Antennas and Propagation (APSURSI), San Diego, CA, USA, 9–15 July 2017; IEEE: San Diego, CA, USA, 2017; pp. 781–783. [Google Scholar]
- Song, H.; Sasada, S.; Kadoya, T.; Okada, M.; Arihiro, K.; Xiao, X.; Kikkawa, T. Detectability of Breast Tumor by a Hand-held Impulse-Radar Detector: Performance Evaluation and Pilot Clinical Study. Sci. Rep. 2017, 7, 16353. [Google Scholar] [CrossRef] [Green Version]
- Porter, E.D.K.; Popovic, M. Investigation of Time-Domain Microwave Radar With Breast Clinic Patients. In Proceedings of the 10th European Conference on Antennas and Propagation (EuCAP), Davos, Switzerland, 10–15 April 2016; 2016; pp. 1–3. [Google Scholar]
- Kuwahara, Y. Microwave Imaging for Early Breast Cancer Detection. New Perspect. Breast Imaging. IntechOpen. 2017, pp. 45–71. Available online: https://www.intechopen.com/books/new-perspectives-in-breast-imaging/microwave-imaging-for-early-breast-cancer-detection (accessed on 4 October 2017).
- Fasoula, A.; Duchesne, L.; Gil Cano, J.D.; Lawrence, P.; Robin, G.; Bernard, J.G. On-Site Validation of a Microwave Breast Imaging System, before First Patient Study. Diagnostics 2018, 8, 53. [Google Scholar] [CrossRef] [Green Version]
- Fasoula, A.; Moloney, B.M.; Duchesne, L.; Cano, J.D.G.; Oliveira, B.L.; Bernard, J.G.; Kerin, M. Super-Resolution Radar Imaging for Breast Cancer Detection with Microwaves: The Integrated Information Selection Criteria. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 2019; pp. 1868–1874. [Google Scholar]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Trial | Country |
|---|---|
| Greater New York Health Insurance Plan (HIP) [14] | United States |
| Two-County Trial (TCT) [15] | Sweden |
| Malmo Mammography Screening Trial (MMST) [16] | Sweden |
| 18-year follow-up meta-analysis of Swedish RCTs [17] | Sweden |
| Goteborg trial [18] | Sweden |
| National Breast Screening Study-1 (NBSS-1) [19] | Canada |
| National Breast Screening Study-2 (NBSS-2) [20] | Canada |
| Trial on women 40 years old at entry [21] | United Kingdom |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moloney, B.M.; O’Loughlin, D.; Abd Elwahab, S.; Kerin, M.J. Breast Cancer Detection—A Synopsis of Conventional Modalities and the Potential Role of Microwave Imaging. Diagnostics 2020, 10, 103. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10020103
Moloney BM, O’Loughlin D, Abd Elwahab S, Kerin MJ. Breast Cancer Detection—A Synopsis of Conventional Modalities and the Potential Role of Microwave Imaging. Diagnostics. 2020; 10(2):103. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10020103
Chicago/Turabian StyleMoloney, Brian M., Declan O’Loughlin, Sami Abd Elwahab, and Michael J. Kerin. 2020. "Breast Cancer Detection—A Synopsis of Conventional Modalities and the Potential Role of Microwave Imaging" Diagnostics 10, no. 2: 103. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10020103