BRCAness as an Important Prognostic Marker in Patients with Triple-Negative Breast Cancer Treated with Neoadjuvant Chemotherapy: A Multicenter Retrospective Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. DNA Isolation and MLPA
2.3. Data Analysis
2.4. Statistical Analysis
2.5. Statement of Ethics
3. Results
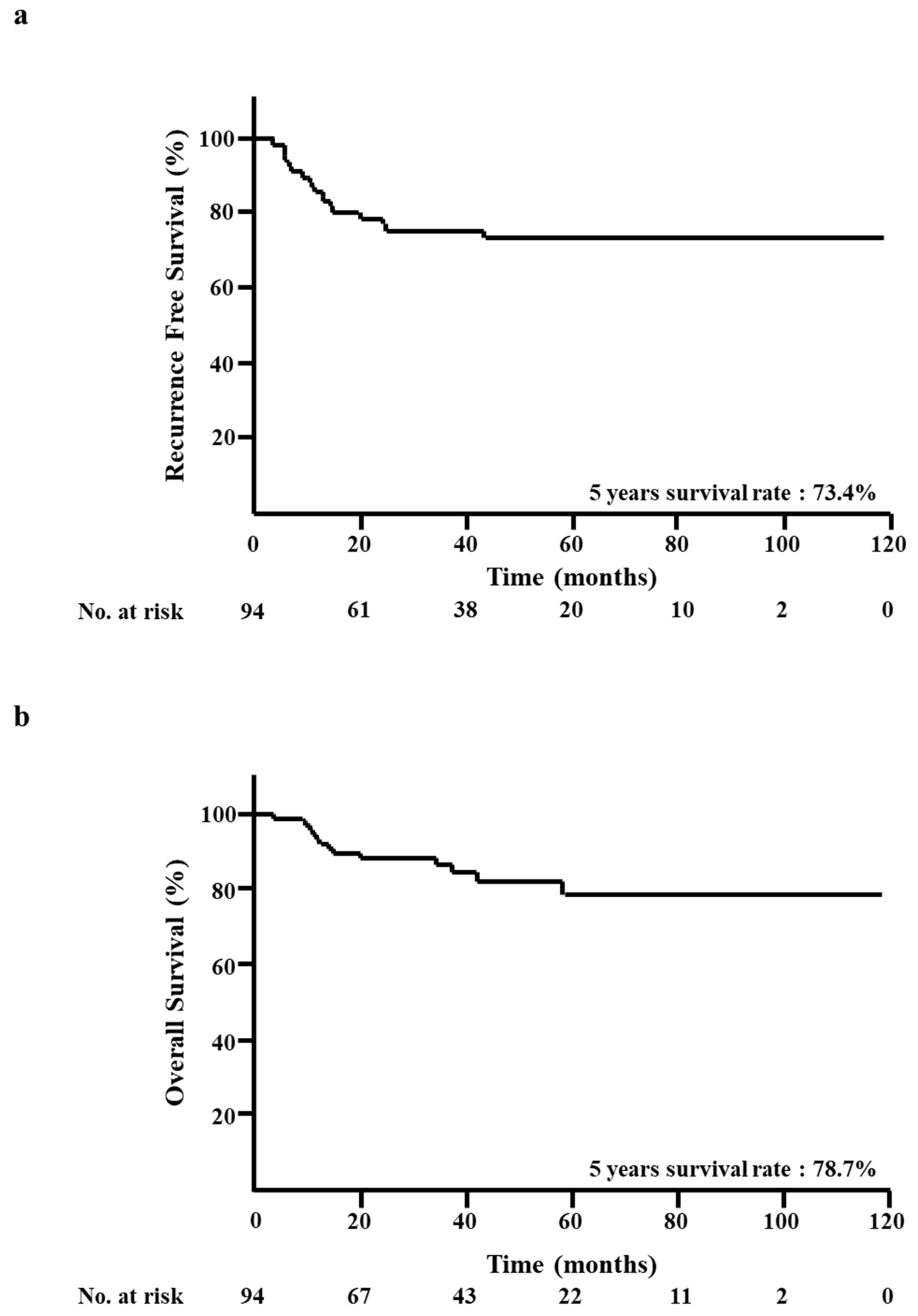
3.1. RFS and OS of all Patients
3.2. BRCAness of CNB Specimens and Clinicopathological Factors
3.3. BRCAness of Surgical Specimens and Clinicopathological Factors
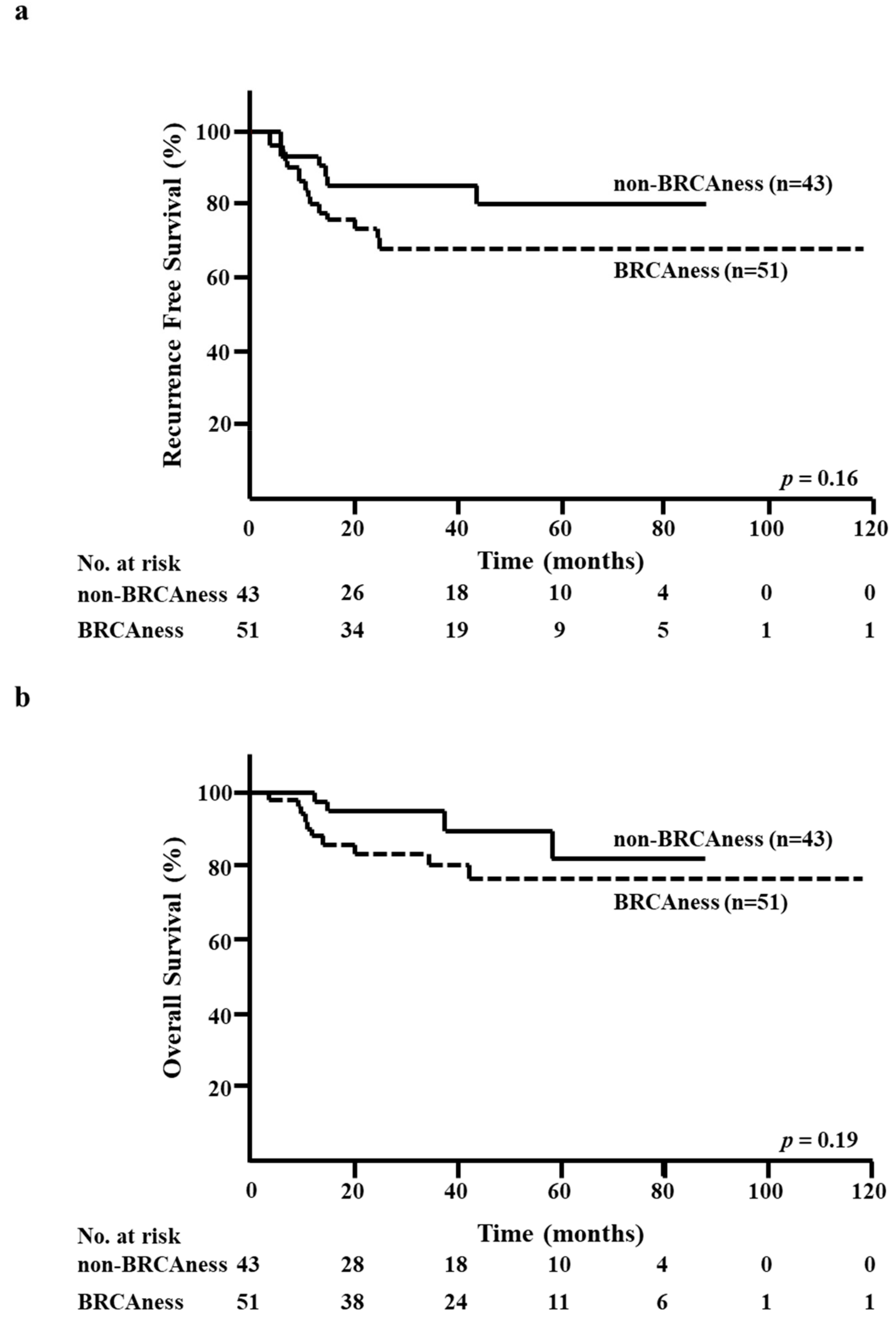
3.4. BRCAness of CNB Specimens and RFS/OS
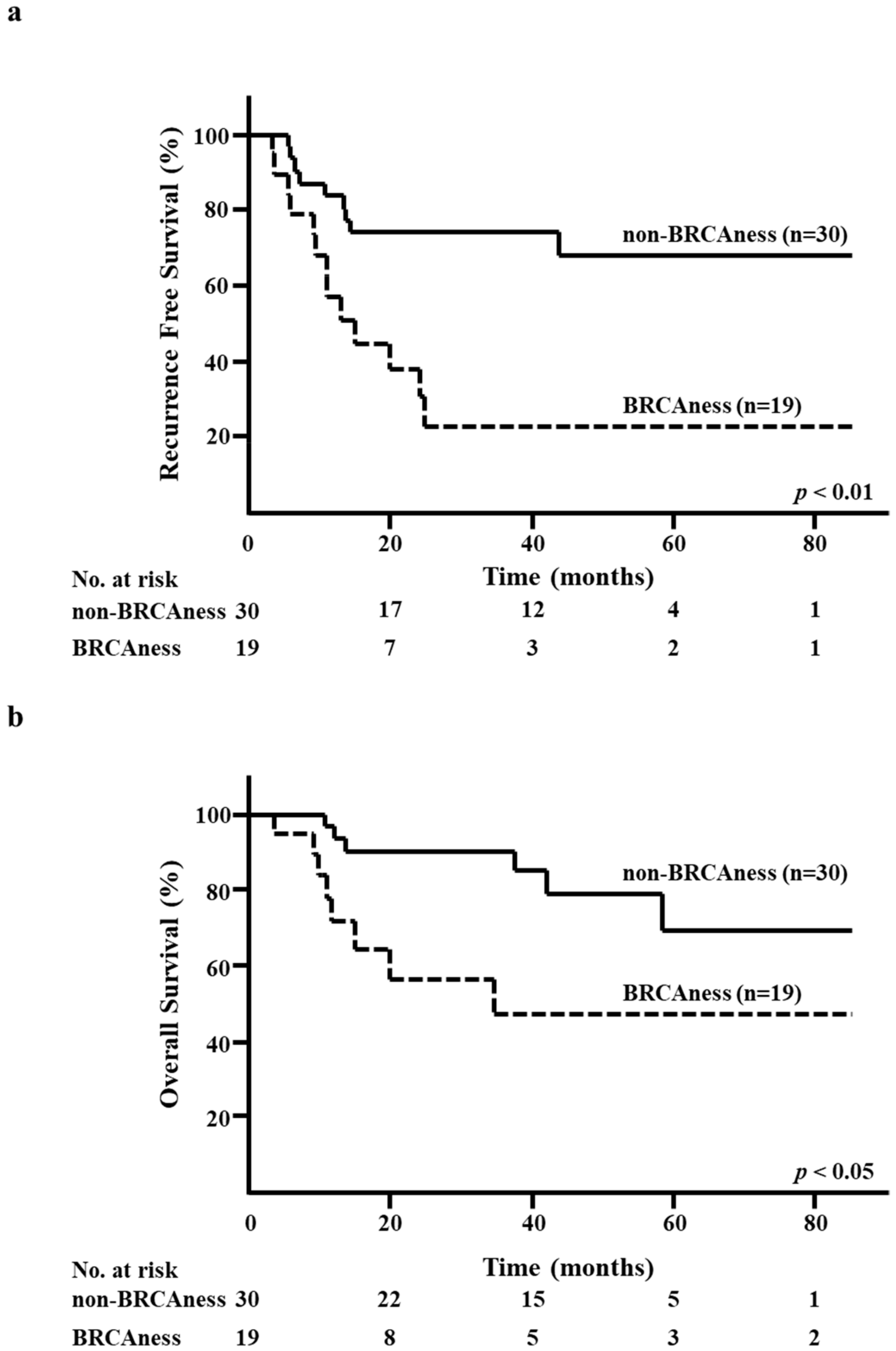
3.5. BRCAness of Surgical Specimens and RFS/OS
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA A Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [Green Version]
- Lam, S.W.; Jimenez, C.R.; Boven, E. Breast cancer classification by proteomic technologies: Current state of knowledge. Cancer Treat. Rev. 2014, 40, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Carey, L.A.; Perou, C.M.; Livasy, C.A.; Dressler, L.G.; Cowan, D.; Conway, K.; Karaca, G.; Troester, M.A.; Tse, C.K.; Edmiston, S.; et al. Race, breast cancer subtypes, and survival in the Carolina Breast Cancer Study. Jama 2006, 295, 2492–2502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perou, C.M.; Sorlie, T.; Eisen, M.B.; van de Rijn, M.; Jeffrey, S.S.; Rees, C.A.; Pollack, J.R.; Ross, D.T.; Johnsen, H.; Akslen, L.A.; et al. Molecular portraits of human breast tumours. Nature 2000, 406, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Reis-Filho, J.S.; Pusztai, L. Gene expression profiling in breast cancer: Classification, prognostication, and prediction. Lancet 2011, 378, 1812–1823. [Google Scholar] [CrossRef]
- Sorlie, T.; Perou, C.M.; Tibshirani, R.; Aas, T.; Geisler, S.; Johnsen, H.; Hastie, T.; Eisen, M.B.; van de Rijn, M.; Jeffrey, S.S.; et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc. Natl. Acad. Sci. USA 2001, 98, 10869–10874. [Google Scholar] [CrossRef] [Green Version]
- Cortazar, P.; Zhang, L.; Untch, M.; Mehta, K.; Costantino, J.P.; Wolmark, N.; Bonnefoi, H.; Cameron, D.; Gianni, L.; Valagussa, P.; et al. Pathological complete response and long-term clinical benefit in breast cancer: The CTNeoBC pooled analysis. Lancet 2014, 384, 164–172. [Google Scholar] [CrossRef] [Green Version]
- Von Minckwitz, G.; Untch, M.; Blohmer, J.U.; Costa, S.D.; Eidtmann, H.; Fasching, P.A.; Gerber, B.; Eiermann, W.; Hilfrich, J.; Huober, J.; et al. Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J. Clin. Oncol.Off. J. Am. Soc. Clin. Oncol. 2012, 30, 1796–1804. [Google Scholar] [CrossRef] [Green Version]
- Lehmann, B.D.; Bauer, J.A.; Chen, X.; Sanders, M.E.; Chakravarthy, A.B.; Shyr, Y.; Pietenpol, J.A. Identification of human triple-negative breast cancer subtypes and preclinical models for selection of targeted therapies. J. Clin. Investig. 2011, 121, 2750–2767. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Angulo, A.M.; Timms, K.M.; Liu, S.; Chen, H.; Litton, J.K.; Potter, J.; Lanchbury, J.S.; Stemke-Hale, K.; Hennessy, B.T.; Arun, B.K.; et al. Incidence and outcome of BRCA mutations in unselected patients with triple receptor-negative breast cancer. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2011, 17, 1082–1089. [Google Scholar] [CrossRef] [Green Version]
- Byrski, T.; Dent, R.; Blecharz, P.; Foszczynska-Kloda, M.; Gronwald, J.; Huzarski, T.; Cybulski, C.; Marczyk, E.; Chrzan, R.; Eisen, A.; et al. Results of a phase II open-label, non-randomized trial of cisplatin chemotherapy in patients with BRCA1-positive metastatic breast cancer. Breast Cancer Res. BCR 2012, 14, R110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lips, E.H.; Laddach, N.; Savola, S.P.; Vollebergh, M.A.; Oonk, A.M.; Imholz, A.L.; Wessels, L.F.; Wesseling, J.; Nederlof, P.M.; Rodenhuis, S. Quantitative copy number analysis by Multiplex Ligation-dependent Probe Amplification (MLPA) of BRCA1-associated breast cancer regions identifies BRCAness. Breast Cancer Res. BCR 2011, 13, R107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vollebergh, M.A.; Lips, E.H.; Nederlof, P.M.; Wessels, L.F.; Schmidt, M.K.; van Beers, E.H.; Cornelissen, S.; Holtkamp, M.; Froklage, F.E.; de Vries, E.G.; et al. An aCGH classifier derived from BRCA1-mutated breast cancer and benefit of high-dose platinum-based chemotherapy in HER2-negative breast cancer patients. Ann. Oncol. Off. J. Eur. Soc. Med Oncol. 2011, 22, 1561–1570. [Google Scholar] [CrossRef] [PubMed]
- Vollebergh, M.A.; Lips, E.H.; Nederlof, P.M.; Wessels, L.F.; Wesseling, J.; Vd Vijver, M.J.; de Vries, E.G.; van Tinteren, H.; Jonkers, J.; Hauptmann, M.; et al. Genomic patterns resembling BRCA1- and BRCA2-mutated breast cancers predict benefit of intensified carboplatin-based chemotherapy. Breast Cancer Res. BCR 2014, 16, R47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner, N.; Tutt, A.; Ashworth, A. Hallmarks of ‘BRCAness’ in sporadic cancers. Nat. Rev. Cancer 2004, 4, 814–819. [Google Scholar] [CrossRef]
- Tanino, H.; Kosaka, Y.; Nishimiya, H.; Tanaka, Y.; Minatani, N.; Kikuchi, M.; Shida, A.; Waraya, M.; Katoh, H.; Enomoto, T.; et al. BRCAness and Prognosis in Triple-Negative Breast Cancer Patients Treated with Neoadjuvant Chemotherapy. PLoS ONE 2016, 11, e0165721. [Google Scholar] [CrossRef] [Green Version]
- Oonk, A.M.; van Rijn, C.; Smits, M.M.; Mulder, L.; Laddach, N.; Savola, S.P.; Wesseling, J.; Rodenhuis, S.; Imholz, A.L.; Lips, E.H. Clinical correlates of ‘BRCAness’ in triple-negative breast cancer of patients receiving adjuvant chemotherapy. Ann. Oncol. Off. J. Eur. Soc. Med Oncol. ESMO 2012, 23, 2301–2305. [Google Scholar] [CrossRef]
- Gross, E.; van Tinteren, H.; Li, Z.; Raab, S.; Meul, C.; Avril, S.; Laddach, N.; Aubele, M.; Propping, C.; Gkazepis, A.; et al. Identification of BRCA1-like triple-negative breast cancers by quantitative multiplex-ligation-dependent probe amplification (MLPA) analysis of BRCA1-associated chromosomal regions: A validation study. BMC Cancer 2016, 16, 811. [Google Scholar] [CrossRef] [Green Version]
- Masuda, N.; Lee, S.J.; Ohtani, S.; Im, Y.H.; Lee, E.S.; Yokota, I.; Kuroi, K.; Im, S.A.; Park, B.W.; Kim, S.B.; et al. Adjuvant Capecitabine for Breast Cancer after Preoperative Chemotherapy. N. Engl. J. Med. 2017, 376, 2147–2159. [Google Scholar] [CrossRef]
- Von Minckwitz, G.; Huang, C.S.; Mano, M.S.; Loibl, S.; Mamounas, E.P.; Untch, M.; Wolmark, N.; Rastogi, P.; Schneeweiss, A.; Redondo, A.; et al. Trastuzumab Emtansine for Residual Invasive HER2-Positive Breast Cancer. N. Engl. J. Med. 2018. [Google Scholar] [CrossRef]
- Akashi-Tanaka, S.; Watanabe, C.; Takamaru, T.; Kuwayama, T.; Ikeda, M.; Ohyama, H.; Mori, M.; Yoshida, R.; Hashimoto, R.; Terumasa, S.; et al. BRCAness predicts resistance to taxane-containing regimens in triple negative breast cancer during neoadjuvant chemotherapy. Clin. Breast Cancer 2015, 15, 80–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mori, H.; Kubo, M.; Nishimura, R.; Osako, T.; Arima, N.; Okumura, Y.; Okido, M.; Yamada, M.; Kai, M.; Kishimoto, J.; et al. BRCAness as a Biomarker for Predicting Prognosis and Response to Anthracycline-Based Adjuvant Chemotherapy for Patients with Triple-Negative Breast Cancer. PLoS ONE 2016, 11, e0167016. [Google Scholar] [CrossRef] [PubMed]
- Tutt, A.; Tovey, H.; Cheang, M.C.U.; Kernaghan, S.; Kilburn, L.; Gazinska, P.; Owen, J.; Abraham, J.; Barrett, S.; Barrett-Lee, P.; et al. Carboplatin in BRCA1/2-mutated and triple-negative breast cancer BRCAness subgroups: The TNT Trial. Nat. Med. 2018, 24, 628–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Telli, M. Optimizing chemotherapy in triple-negative breast cancer: The role of platinum. Am. Soc. Clin. Oncol. Educ. Book. Am. Soc. Clin. Oncology. Annu. Meet. 2014, e37–e42. [Google Scholar] [CrossRef] [PubMed]
- Tutt, A.; Robson, M.; Garber, J.E.; Domchek, S.M.; Audeh, M.W.; Weitzel, J.N.; Friedlander, M.; Arun, B.; Loman, N.; Schmutzler, R.K.; et al. Oral poly(ADP-ribose) polymerase inhibitor olaparib in patients with BRCA1 or BRCA2 mutations and advanced breast cancer: A proof-of-concept trial. Lancet 2010, 376, 235–244. [Google Scholar] [CrossRef]
- Robson, M.; Im, S.A.; Senkus, E.; Xu, B.; Domchek, S.M.; Masuda, N.; Delaloge, S.; Li, W.; Tung, N.; Armstrong, A.; et al. Olaparib for Metastatic Breast Cancer in Patients with a Germline BRCA Mutation. N. Engl. J. Med. 2017, 377, 523–533. [Google Scholar] [CrossRef] [PubMed]
- Litton, J.K.; Rugo, H.S.; Ettl, J.; Hurvitz, S.A.; Goncalves, A.; Lee, K.H.; Fehrenbacher, L.; Yerushalmi, R.; Mina, L.A.; Martin, M.; et al. Talazoparib in Patients with Advanced Breast Cancer and a Germline BRCA Mutation. N. Engl. J. Med. 2018, 379, 753–763. [Google Scholar] [CrossRef]
- McCann, K.E.; Hurvitz, S.A. Advances in the use of PARP inhibitor therapy for breast cancer. Drugs Context 2018, 7, 212540. [Google Scholar] [CrossRef]
- Jiao, S.; Xia, W.; Yamaguchi, H.; Wei, Y.; Chen, M.K.; Hsu, J.M.; Hsu, J.L.; Yu, W.H.; Du, Y.; Lee, H.H.; et al. PARP Inhibitor Upregulates PD-L1 Expression and Enhances Cancer-Associated Immunosuppression. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2017, 23, 3711–3720. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.M.; Cimino-Mathews, A.; Peer, C.J.; Zimmer, A.; Lipkowitz, S.; Annunziata, C.M.; Cao, L.; Harrell, M.I.; Swisher, E.M.; Houston, N.; et al. Safety and Clinical Activity of the Programmed Death-Ligand 1 Inhibitor Durvalumab in Combination With Poly (ADP-Ribose) Polymerase Inhibitor Olaparib or Vascular Endothelial Growth Factor Receptor 1-3 Inhibitor Cediranib in Women’s Cancers: A Dose-Escalation, Phase I Study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2017, 35, 2193–2202. [Google Scholar] [CrossRef]
- Garutti, M.; Pelizzari, G.; Bartoletti, M.; Malfatti, M.C.; Gerratana, L.; Tell, G.; Puglisi, F. Platinum Salts in Patients with Breast Cancer: A Focus on Predictive Factors. Int. J. Mol. Sci. 2019, 20, 3390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mio, C.; Gerratana, L.; Bolis, M.; Caponnetto, F.; Zanello, A.; Barbina, M.; Di Loreto, C.; Garattini, E.; Damante, G.; Puglisi, F. BET proteins regulate homologous recombination-mediated DNA repair: BRCAness and implications for cancer therapy. Int. J. Cancer 2019, 144, 755–766. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Factors | No. | % |
|---|---|---|
| Patient | 94 | 100 |
| Age (mean ± SD) | 51.3 ± 11.4 | |
| cT | No. | % |
| T1 | 10 | 10.6 |
| T2 | 62 | 66 |
| T3 | 9 | 9.6 |
| T4 | 13 | 13.8 |
| cN | No. | % |
| N0 | 33 | 35.1 |
| N1 | 53 | 56.4 |
| N2 | 6 | 6.4 |
| N3 | 2 | 2.1 |
| cStage | No. | % |
| I | 7 | 7.4 |
| II | 64 | 68.1 |
| III | 23 | 24.5 |
| Neoadjuvant chemotherapy | No. | % |
| Anthracycline followed by taxane | 86 | 91.5 |
| Anthracycline alone | 3 | 3.2 |
| Taxane alone | 5 | 5.3 |
| Pathological complete response | No. | % |
| No | 49 | 52.1 |
| Yes | 45 | 47.9 |
| Factors | Total | non-BRCAness | BRCAness | p | ||
|---|---|---|---|---|---|---|
| (n = 43) | (n = 51) | |||||
| No. | % | No. | % | |||
| Age (mean ± SD) | 51.2 ± 11.2 | 51.4 ± 11.6 | NS | |||
| Tumor size | Total | No. | % | No. | % | p |
| cT1-cT2 | 72 | 33 | 76.7 | 39 | 76.5 | NS |
| cT3-cT4 | 22 | 10 | 23.3 | 12 | 23.5 | |
| Lymph node metastasis | Total | No. | % | No. | % | p |
| Negative (cN0) | 33 | 14 | 32.6 | 19 | 37.3 | NS |
| Positive (cN1-cN3) | 61 | 29 | 67.4 | 32 | 62.7 | |
| cStage | Total | No. | % | No. | % | p |
| I | 7 | 4 | 9.3 | 3 | 5.9 | NS |
| II | 64 | 29 | 67.4 | 35 | 68.6 | |
| III | 23 | 10 | 23.3 | 13 | 25.5 | |
| Response | Total | No. | % | No. | % | p |
| pCR | 45 | 25 | 58.1 | 20 | 39.2 | NS |
| non-pCR | 49 | 18 | 41.9 | 31 | 60.8 | |
| Factors | Total | non-BRCAness | BRCAness | p | ||
|---|---|---|---|---|---|---|
| (n = 30) | (n = 19) | |||||
| No. | % | No. | % | |||
| Age (mean ± SD) | 53.5 ± 10.4 | 47.0 ± 11.6 | < 0.05 | |||
| Tumor size | Total | No. | % | No. | % | p |
| cT1-cT2 | 35 | 22 | 73.3 | 13 | 68.4 | NS |
| cT3-cT4 | 14 | 8 | 26.7 | 6 | 31.6 | |
| Lymph node metastasis | Total | No. | % | No. | % | p |
| Negative (cN0) | 15 | 9 | 30.0 | 6 | 31.6 | NS |
| Positive (cN1-cN3) | 34 | 21 | 70.0 | 13 | 68.4 | |
| cStage | Total | No. | % | No. | % | p |
| I | 2 | 2 | 6.7 | 0 | 0.0 | NS |
| II | 32 | 19 | 63.3 | 13 | 68.4 | |
| III | 15 | 9 | 30.0 | 6 | 31.6 | |
| Recurrence | Total | No. | % | No. | % | p |
| No | 27 | 21 | 70.0 | 6 | 31.6 | < 0.05 |
| Yes | 22 | 9 | 30.0 | 13 | 68.4 | |
| Factors | Total | non-pCR | pCR | p | ||
|---|---|---|---|---|---|---|
| (n = 49) | (n = 45) | |||||
| No. | % | No. | % | |||
| Age (mean ± SD) | 51.0 ± 11.2 | 51.6 ± 11.7 | NS | |||
| Tumor size | Total | No. | % | No. | % | p |
| cT1-cT2 | 72 | 35 | 71.4 | 37 | 82.2 | NS |
| cT3-cT4 | 22 | 14 | 28.6 | 8 | 17.8 | |
| Lymph node metastasis | Total | No. | % | No. | % | p |
| Negative (cN0) | 33 | 15 | 30.6 | 18 | 40.0 | NS |
| Positive (cN1-3) | 61 | 34 | 69.4 | 27 | 60.0 | |
| Stage | Total | No. | % | No. | % | p |
| I | 7 | 2 | 4.1 | 5 | 11.1 | NS |
| II | 64 | 32 | 65.3 | 32 | 71.1 | |
| III | 23 | 15 | 30.6 | 8 | 17.8 | |
| Recurrence | Total | No. | % | No. | % | p |
| No | 72 | 27 | 55.1 | 45 | 100.0 | < 0.0001 |
| Yes | 22 | 22 | 44.9 | 0 | 0.0 | |
| Overall survival | Total | No. | % | No. | % | p |
| Alive | 80 | 35 | 71.4 | 45 | 100.0 | < 0.0001 |
| Dead | 14 | 14 | 28.6 | 0 | 0.0 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kosaka, Y.; Yamamoto, Y.; Tanino, H.; Nishimiya, H.; Yamamoto-Ibusuki, M.; Hirota, Y.; Iwase, H.; Nakamura, S.; Akashi-Tanaka, S. BRCAness as an Important Prognostic Marker in Patients with Triple-Negative Breast Cancer Treated with Neoadjuvant Chemotherapy: A Multicenter Retrospective Study. Diagnostics 2020, 10, 119. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10020119
Kosaka Y, Yamamoto Y, Tanino H, Nishimiya H, Yamamoto-Ibusuki M, Hirota Y, Iwase H, Nakamura S, Akashi-Tanaka S. BRCAness as an Important Prognostic Marker in Patients with Triple-Negative Breast Cancer Treated with Neoadjuvant Chemotherapy: A Multicenter Retrospective Study. Diagnostics. 2020; 10(2):119. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10020119
Chicago/Turabian StyleKosaka, Yoshimasa, Yutaka Yamamoto, Hirokazu Tanino, Hiroshi Nishimiya, Mutsuko Yamamoto-Ibusuki, Yuko Hirota, Hirotaka Iwase, Seigo Nakamura, and Sadako Akashi-Tanaka. 2020. "BRCAness as an Important Prognostic Marker in Patients with Triple-Negative Breast Cancer Treated with Neoadjuvant Chemotherapy: A Multicenter Retrospective Study" Diagnostics 10, no. 2: 119. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10020119