Biobanks—A Platform for Scientific and Biomedical Research

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
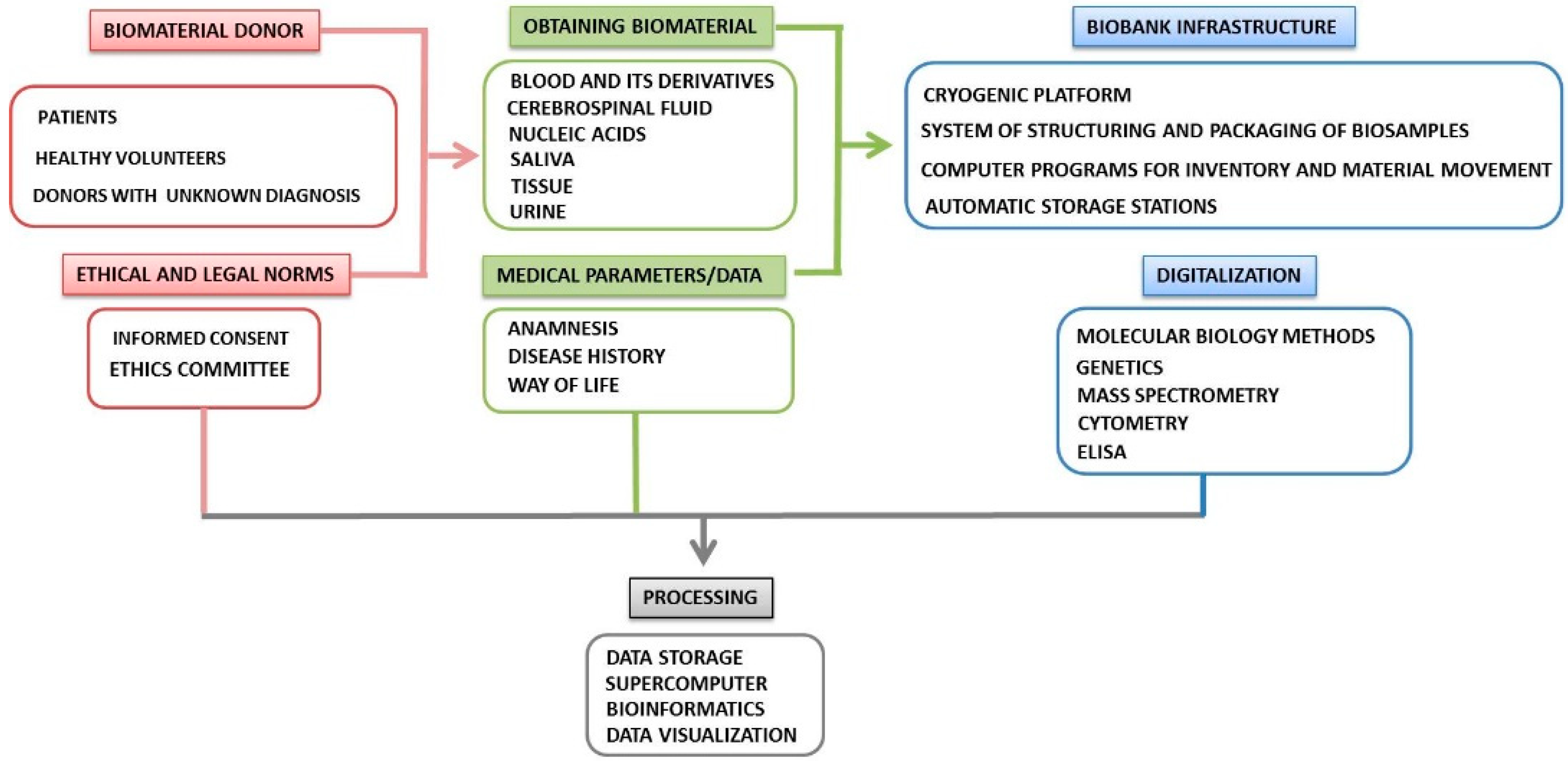
2. Organization of a Biobank
3. Pre-Analytical Sample Handling
- The phase preceding the biological material collection. Here, factors related to the subject (genotype, lifestyle, nutrition, medication, concomitant diseases, surgical interventions, etc.), as well as conditions of samples obtaining (for example, on an empty stomach or postprandial), are of great importance. Most of these variables cannot be standardized because they relate to individual subject and specific treatment methods. However, all of these parameters may affect subsequent analytical results of research and diagnosis.
- The collection phase of biological material begins when the biobank’s staff receive samples. At the moment, the state of the samples is influenced by conditions, transportation (compliance with the cold chain regime, duration) and chain of custody in the laboratory.
- The phase after collecting includes registering and proper annotation of samples in the biobank database. Different storage conditions and time, control of the archived samples, procedures for isolating of analytes for subsequent research can influence the total outcome of studies.
- Terms and definitions in the field of biobank;
- Biobanks and biological resources;
- Analytical methods;
- Bioprocessing;
- Data processing, including annotations, analysis, validation, comparability and data integration [35].
4. Collection and Storage of Biomaterial
4.1. Tissue Biobanks
4.2. Blood Biobanks
4.3. Cell Biobanks
4.4. Organoid Biobanks
4.5. Imaging Biobanks
4.6. Digital Biobanks
5. The Heterogeneity of Biobanks
6. Ethical Aspects of Human Biobanks
- (1)
- The main page of the IP should contain the most important aspects, such as the purpose of the document, a description of the biobank, and the rights of participants (for example, the opportunity not to participate in the study or to refuse to participate at any time, etc.).
- (2)
- The main section of the document should contain information on the nature and functioning of the biobank, the collection and storage of data, the rights of participants, etc.
- (3)
- The process of biobank donation and further research should be illustrated.
- (4)
- Information about the concepts of “long-term storage”, “random data relevant to your health”, and the ability to communicate with the participants should be more clearly and thoroughly explained.
- (5)
- Sentences that are too long and lengthy wordings should be deleted.
- (6)
- Definitions of technical terms, such as “biomaterials”, “Research ethics committee”, “pseudonymization”, and so on, should be the most accurate and understandable [84].
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Charmantier, I.; Müller-Wille, S. Carl Linnaeus’s Botanical Paper Slips (1767-1773). Intellect. Hist. Rev. 2014, 24, 215–238. [Google Scholar] [CrossRef] [Green Version]
- Porteri, C. Management of the Ethical Aspects of a Local Mental Diseases Biobank for Research Purposes: The Italian Experience. In Ethics, Law and Governance of Biobanking: National, European and International Approaches; Mascalzoni, D., Ed.; Springer: Dordrecht, The Netherlands, 2015; pp. 219–225. [Google Scholar] [CrossRef]
- Yuzbasioglu, A.; Kesikli, B.; Ozguc, M. Biobanks as basis if individualized medicine: Challenges toward harmonization. In Precision Medicine: Tools and Quantitative Approaches; Deigner, H.-P., Kohl, M.E., Fedor, J., Eds.; Academic Press: London, UK, 2018; Volume 4, pp. 57–77. [Google Scholar]
- Creation and Governance of Human Genetic Research Databases. Available online: https://stats.oecd.org/glossary/detail.asp?ID=7220 (accessed on 23 July 2007).
- 2012 Best Practices for Repositories Collection, Storage, Retrieval, and Distribution of Biological Materials for Research International Society for Biological and Environmental Repositories. Biopreserv. Biobank. 2012, 10, 79–161. [CrossRef] [PubMed] [Green Version]
- Zika, E.; Paci, D.; Schulte in den Bäumen, T.; Braun, A.; Rijkers-Defrasne, S.; Deschênes, M.; Fortier, I.; Laage-Hellman, J.; Scerri, C.A.; Ibarreta, D. Institute for Prospective Technological Studies. In Biobanks in Europe: Prospects for Harmonisation and Networking; Publications Office: Luxembourg, 2010. [Google Scholar]
- Jang, T.H.; Park, S.C.; Yang, J.H.; Kim, J.Y.; Seok, J.H.; Park, U.S.; Choi, C.W.; Lee, S.R.; Han, J. Cryopreservation and Its Clinical Applications. Integr. Med. Res. 2017, 6, 12–18. [Google Scholar] [CrossRef]
- Lehmann, S.; Guadagni, F.; Moore, H.; Ashton, G.; Barnes, M.; Benson, E.; Clements, J.; Koppandi, I.; Coppola, D.; Demiroglu, S.Y.; et al. International Society for Biological and Environmental Repositories (ISBER) Working Group on Biospecimen Science. Standard Preanalytical Coding for Biospecimens: Review and Implementation of the Sample PREanalytical Code (SPREC). Biopreserv. Biobank. 2012, 10, 366–374. [Google Scholar] [CrossRef] [PubMed]
- Zinchenko, L.P.; Ryzhov, A.L.; Tkhostov, A.S.; Bryzgalina, E.V. Problems of the Evaluation of Psychological Characteristics of Biobank Donors: Theoretical and Practical Aspects. Russ. Psychol. J. 2016, 13, 140–151. [Google Scholar]
- Carey, D.J.; Fetterolf, S.N.; Davis, F.D.; Faucett, W.A.; Kirchner, H.L.; Mirshahi, U.; Murray, M.F.; Smelser, D.T.; Gerhard, G.S.; Ledbetter, D.H. The Geisinger MyCode Community Health Initiative: An Electronic Health Record-Linked Biobank for Precision Medicine Research. Genet. Med. Off. J. Am. Coll. Med. Genet. 2016, 18, 906–913. [Google Scholar] [CrossRef] [Green Version]
- Chen, R.; Mias, G.I.; Li-Pook-Than, J.; Jiang, L.; Lam, H.Y.K.; Chen, R.; Miriami, E.; Karczewski, K.J.; Hariharan, M.; Dewey, F.E.; et al. Personal Omics Profiling Reveals Dynamic Molecular and Medical Phenotypes. Cell 2012, 148, 1293–1307. [Google Scholar] [CrossRef] [Green Version]
- Pakharukova, N.A.; Pastushkova, L.K.; Trifonova, O.P.; Moshkovskii, S.A.; Larina, I.M. Variability in Low/Molecular Subproteome of Blood Serum of Healthy Man in Normal Life Conditions. Pfiziologiya Cheloveka 2011, 37, 77–85. (In Russian) [Google Scholar]
- Botti, G.; Franco, R.; Cantile, M.; Ciliberto, G.; Ascierto, P.A. Tumor Biobanks in Translational Medicine. J. Transl. Med. 2012, 10, 204. [Google Scholar] [CrossRef] [Green Version]
- Samot, J.; Moon, S.; Shao, L.; Zhang, X.; Xu, F.; Song, Y.; Keles, H.; Matloff, L.; Markel, J.; Demirci, U. Blood Banking in Living Droplets. PLoS ONE 2011, 6, e17530. [Google Scholar] [CrossRef] [Green Version]
- Patel, A. Tissue Banking for Research--Bench to Bedside and Back--Myth, Reality or Fast Fading Reality at the Dawn of a Personalised Healthcare Era. Cell Tissue Bank. 2011, 1, 19–21. [Google Scholar] [CrossRef] [PubMed]
- Dillner, J.; Andersson, K. Biobanks collected for routine healthcare purposes: Build-up and use for epidemiologic research. Methods Mol. Biol. 2011, 675, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Liu, A.; Pollard, K. Biobanking for Personalized Medicine. Adv. Exp. Med. Biol. 2015, 864, 55–68. [Google Scholar] [CrossRef] [PubMed]
- Peakman, T.; Elliott, P. Current Standards for the Storage of Human Samples in Biobanks. Genome Med. 2010, 2, 72. [Google Scholar] [CrossRef]
- Allocca, C.M.; Bledsoe, M.J.; Furuta, K.; Ramirez, N.C. ISO/TC276/WG2 Biobanks and Bioresources: Draft International Standard Is Now Available for Comment. Biopreserv. Biobank. 2017, 15, 399–401. [Google Scholar] [CrossRef]
- ISO 20387:2018 Biotechnology—Biobanking—General Requirements for Biobanking. Available online: https://www.iso.org/standard/67888.html (accessed on 20 May 2020).
- ISBER. ISO/DIS 20387 Biotechnology–Biobanking–General Requirements for Biobanking. Available online: https://www.isber.org/page/ISODIS20387_NonMem (accessed on 20 May 2020).
- International Society for Biological and Environmental Repositories. Best Practices for Repositories: Collection, Storage, Retrieval and Distribution of Biological Materials for Research; ISBER: Vancouver, BC, Canada, 2011. [Google Scholar]
- Cervo, S.; De Paoli, P.; Mestroni, E.; Perin, T.; Escoffier, L.; Canzonieri, V.; Steffan, A. Drafting Biological Material Transfer Agreement: A Ready-to-Sign Model for Biobanks and Biorepositories. Int. J. Biol. Markers 2016, 31, e211–e217. [Google Scholar] [CrossRef] [Green Version]
- Lovegrove, J.; Hodson, L.; Sharma, S.; Lanham-New, S. Nutrition Research Methodologies; John Wiley & Sons: Hoboken, NJ, USA, 2015. [Google Scholar]
- Standardization and Improvement of Generic Pre-Analytical Tools and Procedures for in Vitro Diagnostics. Available online: https://www.spidia.eu/ (accessed on 20 May 2020).
- Cacciatore, S.; Hu, X.; Viertler, C.; Kap, M.; Bernhardt, G.A.; Mischinger, H.-J.; Riegman, P.; Zatloukal, K.; Luchinat, C.; Turano, P. Effects of Intra- and Post-Operative Ischemia on the Metabolic Profile of Clinical Liver Tissue Specimens Monitored by NMR. J. Proteome Res. 2013, 12, 5723–5729. [Google Scholar] [CrossRef]
- ISO 20184-1:2018 Molecular In Vitro Diagnostic Examinations—Specifications for Pre-Examination Processes for Frozen Tissue—Part 1: Isolated RNA. Available online: https://www.iso.org/standard/67215.html (accessed on 20 May 2020).
- ISO 20184-2:2018 Molecular In Vitro Diagnostic Examinations—Specifications for Pre-Examination Processes for Frozen Tissue—Part 2: Isolated Proteins. Available online: https://www.iso.org/standard/69801.html (accessed on 20 May 2020).
- ISO 20166-1:2018 Molecular In Vitro Diagnostic Examinations—Specifications for Pre-Examination Processes for Formalin-Fixed and Paraffin-Embedded (FFPE) Tissue—Part 1: Isolated RNA. Available online: https://www.iso.org/standard/67179.html (accessed on 20 May 2020).
- ISO 20166-2:2018 Molecular in Vitro Diagnostic Examinations—Specifications for Pre-Examinations Processes for Formalin-Fixed and Paraffin-Embedded (FFPE) Tissue—Part 2: Isolated Proteins. Available online: https://www.iso.org/standard/69802.html (accessed on 20 May 2020).
- ISO 20166-3:2018 Molecular in Vitro Diagnostic Examinations—Specifications for Pre-Examination Processes for Formalin-Fixed and Paraffin-Embedded (FFPE) Tissue—Part 3: Isolated DNA. Available online: https://www.iso.org/ru/standard/69803.html (accessed on 20 May 2020).
- ISO 20186-1:2019 Molecular In Vitro Diagnostic Examinations—Specifications for Pre-Examination Processes for Venous Whole Blood—Part 1: Isolated Cellular RNA. Available online: https://www.iso.org/standard/67217.html (accessed on 20 May 2020).
- ISO 20186-2:2019 Molecular in Vitro Diagnostic Examinations—Specifications for Pre-Examination Processes for Venous Whole Blood—Part 2: Isolated Genomic DNA. Available online: https://www.iso.org/standard/69799.html (accessed on 20 May 2020).
- ISO 20186-3:2019 Molecular In Vitro Diagnostic Examinations—Specifications for Pre-Examination Processes for Venous Whole Blood—Part 3: Isolated Circulating Cell Free DNA from Plasma. Available online: https://www.iso.org/standard/69800.html (accessed on 23 May 2020).
- Furuta, K.; Schacter, B. Report on Status of ISO276/WG2 on Biobanks and Bioresources: International Standards for Biobanking. Biopreserv. Biobank. 2015, 13, 452–453. [Google Scholar] [CrossRef]
- Mester, J.L.; Mercer, M.; Goldenberg, A.; Moore, R.A.; Eng, C.; Sharp, R.R. Communicating with Biobank Participants: Preferences for Receiving and Providing Updates to Researchers. Cancer Epidemiol. Biomark. Prev. 2015, 24, 708–712. [Google Scholar] [CrossRef] [Green Version]
- Izumi, M.; Zhang, B.-X.; Dean, D.D.; Lin, A.L.; Saunders, M.J.; Hazuda, H.P.; Yeh, C.-K. Secretion of Salivary Statherin Is Compromised in Uncontrolled Diabetic Patients. BBA Clin. 2015, 3, 135–140. [Google Scholar] [CrossRef] [Green Version]
- Ma, Y.; Chen, H.; Lei, R.; Ren, J. Biobanking for Human Microbiome Research: Promise, Risks, and Ethics. Asian Bioeth. Rev. 2017, 9, 311–324. [Google Scholar] [CrossRef]
- Peakman, T.C.; Elliott, P. The UK Biobank Sample Handling and Storage Validation Studies. Int. J. Epidemiol. 2008, 37, i2–i6. [Google Scholar] [CrossRef]
- Paskal, W.; Paskal, A.M.; Dębski, T.; Gryziak, M.; Jaworowski, J. Aspects of Modern Biobank Activity—Comprehensive Review. Pathol. Oncol. Res. 2018, 24, 771–785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burke, W.; Khoury, M.J.; Stewart, A.; Zimmern, R.L. The Path from Genome-Based Research to Population Health: Development of an International Public Health Genomics Network. Genet. Med. 2006, 8, 451–458. [Google Scholar] [CrossRef]
- Council of Europe. Recommendation Rec (2006)4 of the Committee of Ministers to Member States on Research on Biological Materials of Human Origin and Its Explanatory Memorandum. Available online: https://search.coe.int/cm/Pages/result_details.aspx?ObjectID=09000016805d84de (accessed on 15 March 2020).
- De Souza, Y.G.; Greenspan, J.S. Biobanking Past, Present and Future: Responsibilities and Benefits. AIDS 2013, 27, 303–312. [Google Scholar] [CrossRef]
- Mareninov, S.; De Jesus, J.; Sanchez, D.E.; Kay, A.B.; Wilson, R.W.; Babic, I.; Chen, W.; Telesca, D.; Lou, J.J.; Mirsadraei, L.; et al. Lyophilized Brain Tumor Specimens Can Be Used for Histologic, Nucleic Acid, and Protein Analyses after 1 Year of Room Temperature Storage. J. Neurooncol. 2013, 113, 365–373. [Google Scholar] [CrossRef] [Green Version]
- Manne, U.; Myers, R.B.; Srivastava, S.; Grizzle, W.E. Re: Loss of Tumor Marker-Immunostaining Intensity on Stored Paraffin Slides of Breast Cancer. J. Natl. Cancer Inst. 1997, 89, 585–586. [Google Scholar] [CrossRef] [Green Version]
- Fergenbaum, J.H.; Garcia-Closas, M.; Hewitt, S.M.; Lissowska, J.; Sakoda, L.C.; Sherman, M.E. Loss of Antigenicity in Stored Sections of Breast Cancer Tissue Microarrays. Cancer Epidemiol. Biomark. Prev. 2004, 13, 667–672. [Google Scholar]
- Shabihkhani, M.; Lucey, G.M.; Wei, B.; Mareninov, S.; Lou, J.J.; Vinters, H.V.; Singer, E.J.; Cloughesy, T.F.; Yong, W.H. The Procurement, Storage, and Quality Assurance of Frozen Blood and Tissue Biospecimens in Pathology, Biorepository, and Biobank Settings. Clin. Biochem. 2014, 47, 258–266. [Google Scholar] [CrossRef] [Green Version]
- Maruyama, M.; Kenmochi, T.; Sakamoto, K.; Arita, S.; Iwashita, C.; Kashiwabara, H. Simplified Method for Cryopreservation of Islets Using Hydroxyethyl Starch and Dimethyl Sulfoxide as Cryoprotectants. Transplant. Proc. 2004, 36, 1133–1134. [Google Scholar] [CrossRef]
- Onofre, J.; Baert, Y.; Faes, K.; Goossens, E. Cryopreservation of Testicular Tissue or Testicular Cell Suspensions: A Pivotal Step in Fertility Preservation. Hum. Reprod. Update 2016, 22, 744–761. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Tan, J.-C.; Li, L.-S. Comparison of Three Methods for Cryopreservation of Human Embryonic Stem Cells. Fertil. Steril. 2010, 93, 999–1005. [Google Scholar] [CrossRef] [PubMed]
- Holland, N.T.; Smith, M.T.; Eskenazi, B.; Bastaki, M. Biological Sample Collection and Processing for Molecular Epidemiological Studies. Mutat. Res. 2003, 543, 217–234. [Google Scholar] [CrossRef]
- Elliott, P.; Peakman, T.C.; UK Biobank. The UK Biobank Sample Handling and Storage Protocol for the Collection, Processing and Archiving of Human Blood and Urine. Int. J. Epidemiol. 2008, 37, 234–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsieh, S.-Y.; Chen, R.-K.; Pan, Y.-H.; Lee, H.-L. Systematical Evaluation of the Effects of Sample Collection Procedures on Low-Molecular-Weight Serum/Plasma Proteome Profiling. Proteomics 2006, 6, 3189–3198. [Google Scholar] [CrossRef] [PubMed]
- Boyanton, B.L.; Blick, K.E. Stability Studies of Twenty-Four Analytes in Human Plasma and Serum. Clin. Chem. 2002, 48, 2242–2247. [Google Scholar] [CrossRef]
- Coppola, L.; Cianflone, A.; Grimaldi, A.M.; Incoronato, M.; Bevilacqua, P.; Messina, F.; Baselice, S.; Soricelli, A.; Mirabelli, P.; Salvatore, M. Biobanking in Health Care: Evolution and Future Directions. J. Transl. Med. 2019, 1, 172. [Google Scholar] [CrossRef] [Green Version]
- Nederhand, R.J.; Droog, S.; Kluft, C.; Simoons, M.L.; de Maat, M.P.M.; Investigators of the EUROPA trial. Logistics and Quality Control for DNA Sampling in Large Multicenter Studies. J. Thromb. Haemost. 2003, 1, 987–991. [Google Scholar] [CrossRef]
- Von Ahlfen, S.; Missel, A.; Bendrat, K.; Schlumpberger, M. Determinants of RNA Quality from FFPE Samples. PLoS ONE 2007, 2, e1261. [Google Scholar] [CrossRef]
- Steinberg, K.; Beck, J.; Nickerson, D.; Garcia-Closas, M.; Gallagher, M.; Caggana, M.; Reid, Y.; Cosentino, M.; Ji, J.; Johnson, D.; et al. DNA Banking for Epidemiologic Studies: A Review of Current Practices. Epidemiology 2002, 13, 246–254. [Google Scholar] [CrossRef]
- Identity Crisis. Nature 2009, 457, 935–936. [CrossRef] [PubMed] [Green Version]
- Corral-Vázquez, C.; Aguilar-Quesada, R.; Catalina, P.; Lucena-Aguilar, G.; Ligero, G.; Miranda, B.; Carrillo-Ávila, J.A. Cell Lines Authentication and Mycoplasma Detection as Minimun Quality Control of Cell Lines in Biobanking. Cell Tissue Bank. 2017, 18, 271–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boers, S.N.; van Delden, J.J.; Clevers, H.; Bredenoord, A.L. Organoid Biobanking: Identifying the Ethics: Organoids Revive Old and Raise New Ethical Challenges for Basic Research and Therapeutic Use. EMBO Rep. 2016, 17, 938–941. [Google Scholar] [CrossRef] [Green Version]
- Sato, T.; Clevers, H. Growing Self-Organizing Mini-Guts from a Single Intestinal Stem Cell: Mechanism and Applications. Science 2013, 340, 1190–1194. [Google Scholar] [CrossRef] [Green Version]
- Willyard, C. The Boom in Mini Stomachs, Brains, Breasts, Kidneys and More. Nature 2015, 523, 520–522. [Google Scholar] [CrossRef] [Green Version]
- Dekkers, J.F.; van der Ent, C.K.; Beekman, J.M. Novel Opportunities for CFTR-Targeting Drug Development Using Organoids. Rare Dis. 2013, 1, e27112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van de Wetering, M.; Francies, H.E.; Francis, J.M.; Bounova, G.; Iorio, F.; Pronk, A.; van Houdt, W.; van Gorp, J.; Taylor-Weiner, A.; Kester, L.; et al. Prospective Derivation of a Living Organoid Biobank of Colorectal Cancer Patients. Cell 2015, 161, 933–945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sachs, N.; de Ligt, J.; Kopper, O.; Gogola, E.; Bounova, G.; Weeber, F.; Balgobind, A.V.; Wind, K.; Gracanin, A.; Begthel, H.; et al. A Living Biobank of Breast Cancer Organoids Captures Disease Heterogeneity. Cell 2018, 172, 373–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, V.; Gu, Y.; Basu, S.; Berglund, A.; Eschrich, S.A.; Schabath, M.B.; Forster, K.; Aerts, H.J.W.L.; Dekker, A.; Fenstermacher, D.; et al. Radiomics: The Process and the Challenges. Magn. Reason. Imaging 2012, 30, 1234–1248. [Google Scholar] [CrossRef] [Green Version]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [Green Version]
- Capocasa, M.; Anagnostou, P.; D’Abramo, F.; Matteucci, G.; Dominici, V.; Destro Bisol, G.; Rufo, F. Samples and Data Accessibility in Research Biobanks: An Explorative Survey. PeerJ 2016, 4, e1613. [Google Scholar] [CrossRef] [Green Version]
- Aiello, M.; Cavaliere, C.; D’Albore, A.; Salvatore, M. The Challenges of Diagnostic Imaging in the Era of Big Data. J. Clin. Med. 2019, 8, 316. [Google Scholar] [CrossRef] [Green Version]
- Neri, E.; Regge, D. Imaging Biobanks in Oncology: European Perspective. Future Oncol. 2017, 13, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Clark, K.; Vendt, B.; Smith, K.; Freymann, J.; Kirby, J.; Koppel, P.; Moore, S.; Phillips, S.; Maffitt, D.; Pringle, M.; et al. The Cancer Imaging Archive (TCIA): Maintaining and Operating a Public Information Repository. J. Digit. Imaging 2013, 26, 1045–1057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Society of Radiology (ESR). ESR Position Paper on Imaging Biobanks. Insights Imaging 2015, 6, 403–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobs, G.; Wolf, A.; Krawczak, M.; Lieb, W. Biobanks in the Era of Digital Medicine. Clin. Pharmacol. Ther. 2018, 103, 761–762. [Google Scholar] [CrossRef]
- Ransohoff, D.F.; Gourlay, M.L. Sources of Bias in Specimens for Research about Molecular Markers for Cancer. J. Clin. Oncol. 2010, 28, 698–704. [Google Scholar] [CrossRef] [Green Version]
- Lermen, D.; Gwinner, F.; Bartel-Steinbach, M.; Mueller, S.C.; Habermann, J.K.; Balwir, M.-B.; Smits, E.; Virgolino, A.; Fiddicke, U.; Berglund, M.; et al. Towards Harmonized Biobanking for Biomonitoring: A Comparison of Human Biomonitoring-Related and Clinical Biorepositories. Biopreserv. Biobank. 2020, 18, 122–135. [Google Scholar] [CrossRef] [PubMed]
- Takai-Igarashi, T.; Kinoshita, K.; Nagasaki, M.; Ogishima, S.; Nakamura, N.; Nagase, S.; Nagaie, S.; Saito, T.; Nagami, F.; Minegishi, N.; et al. Security Controls in an Integrated Biobank to Protect Privacy in Data Sharing: Rationale and Study Design. BMC Med. Inform. Decis. Mak. 2017, 17, 100. [Google Scholar] [CrossRef] [PubMed]
- Grady, C. Enduring and Emerging Challenges of Informed Consent. N. Engl. J. Med. 2015, 372, 855–862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Neill, O. Some Limits of Informed Consent. J. Med. Eth. 2003, 29, 4–7. [Google Scholar] [CrossRef] [Green Version]
- Hallinan, Z.P.; Forrest, A.; Uhlenbrauck, G.; Young, S.; McKinney, R. Barriers to Change in the Informed Consent Process: A Systematic Literature Review. IRB 2016, 38, 1–10. [Google Scholar] [PubMed]
- Nishimura, A.; Carey, J.; Erwin, P.J.; Tilburt, J.C.; Murad, M.H.; McCormick, J.B. Improving Understanding in the Research Informed Consent Process: A Systematic Review of 54 Interventions Tested in Randomized Control Trials. BMC Med. Eth. 2013, 14, 28. [Google Scholar] [CrossRef] [Green Version]
- Bossert, S.; Kahrass, H.; Heinemeyer, U.; Prokein, J.; Strech, D. Participatory Improvement of a Template for Informed Consent Documents in Biobank Research—Study Results and Methodological Reflections. BMC Med. Eth. 2017, 18, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Budimir, D.; Polašek, O.; Marušić, A.; Kolčić, I.; Zemunik, T.; Boraska, V.; Jerončić, A.; Boban, M.; Campbell, H.; Rudan, I. Ethical aspects of human biobanks: A systematic review. Croat Med J. 2011, 52, 262–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norgaard-Pedersen, B.; Simonsen, H. Biological Specimen Banks in Neonatal Screening. Acta Paediatr. 1999, 88, 106–109. [Google Scholar] [CrossRef]
- Cambon-Thomsen, A. The Social and Ethical Issues of Post-Genomic Human Biobanks. Nat. Rev. Genet. 2004, 5, 866–873. [Google Scholar] [CrossRef]
- Rothstein, M. Expanding the Ethical Analysis of Biobanks. J. Law Med. Eth. 2005, 33, 89–101. [Google Scholar] [CrossRef]
- Roden, D.; Pulley, J.; Basford, M.; Bernard, G.; Clayton, E.; Balser, J.; Masys, D. Development of a Large-Scale De-Identified DNA Biobank to Enable Personalized Medicine. Clin. Pharmacol. Ther. 2008, 84, 362–369. [Google Scholar] [CrossRef] [Green Version]
- Baumen, T.; Paci, D.; Ibarreta, D. Data Protection in Biobanks—A European Challenge for the Long-Term Sustainability of Biobanking. Rev. Derecho Genoma Hum. 2009, 31, 13–25. [Google Scholar]
- Glantz, L.H.; Roche, P.; Annas, G.J. Gift Giving to Biobanks. Am. J. Bioeth. 2010, 10, 33–34. [Google Scholar] [CrossRef]
- Hawkins, A.K. Biobanks: Importance, Implications and Opportunities for Genetic Counselors. J. Genet. Couns. 2010. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, S. Stewardship of Human Biospecimens, DNA, Genotype, and Clinical Data in the GWAS Era. Annu. Rev. Genom. Hum. Genet. 2009, 10, 193–209. [Google Scholar] [CrossRef] [PubMed]
- Hansson, M. Ethics and Biobanks. Br. J. Cancer 2008, 100, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Truyers, C.; Kellen, E.; Arbyn, M.; Trommelmans, L.; Nys, H.; Hensen, K.; Aertgeerts, B.; Bartholomeeusen, S.; Hansson, M.; Buntinx, F. The Use of Human Tissue in Epidemiological Research; Ethical and Legal Considerations in Two Biobanks in Belgium. Med. Health Care Philos. 2009, 13, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, D.J.; Murphy-Bollinger, J.; Scott, J.; Hudson, K.L. Public Opinion about the Importance of Privacy in Biobank Research. Am. J. Hum. Genet. 2009, 85, 643–654. [Google Scholar] [CrossRef] [Green Version]
- Murphy, J.; Scott, J.; Kaufman, D.; Geller, G.; Leroy, L.; Hudson, K. Public Expectations for Return of Results from Large-Cohort Genetic Research. Am. J. Bioeth. 2008, 8, 36–43. [Google Scholar] [CrossRef]
- Murphy, J.; Scott, J.; Kaufman, D.; Geller, G.; LeRoy, L.; Hudson, K. Public Perspectives on Informed Consent for Biobanking. Am. J. Pub. Health 2009, 99, 2128–2134. [Google Scholar] [CrossRef]
- Hansson, M. The Need to Downregulate: A Minimal Ethical Framework for Biobank Research. Methods Mol. Biol. 2011, 675, 39–59. [Google Scholar] [CrossRef]
- Chalmers, D. Genetic Research and Biobanks. Methods Mol. Biol. 2011, 675, 1–37. [Google Scholar] [CrossRef]
- Forsberg, J.; Hansson, M.; Eriksson, S. Changing Perspectives in Biobank Research: From Individual Rights to Concerns about Public Health Regarding the Return of Results. Eur. J. Hum. Genet. 2009, 17, 1544–1549. [Google Scholar] [CrossRef] [PubMed]
- Morrell, B.; Lipworth, W.; Axler, R.; Kerridge, I.; Little, M. Cancer as Rubbish: Donation of Tumor Tissue for Research. Qual. Health Res. 2011, 21, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Treweek, S.; Doney, A.; Leiman, D. Public Attitudes to the Storage of Blood Left over from Routine General Practice Tests and Its Use in Research. J. Health Serv. Res. Policy 2009, 14, 13–19. [Google Scholar] [CrossRef]
- Allen, J.; McNamara, B. Reconsidering the Value of Consent in Biobank Research. Bioethics 2009, 25, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Toccaceli, V.; Fagnani, C.; Nisticò, L.; D’Ippolito, C.; Giannantonio, L.; Brescianini, S.; Stazi, M.A. Research Understanding, Attitude and Awareness towards Biobanking: A Survey among Italian Twin Participants to a Genetic Epidemiological Study. BMC Med. Eth. 2009, 10, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansson, M. Building on Relationships of Trust in Biobank Research. J. Med. Eth. 2005, 31, 415–418. [Google Scholar] [CrossRef] [Green Version]
- Tutton, R.; Kaye, J.; Hoeyer, K. Governing UK Biobank: The Importance of Ensuring Public Trust. Trends Biotechnol. 2004, 22, 284–285. [Google Scholar] [CrossRef]
- Levenson, D. When Should Pediatric Biobanks Share Data? Am. J. Med. Genet. A. 2010, 152A, fmvii–fmviii. [Google Scholar] [CrossRef]
- Avard, D.; Silverstein, T.; Sillon, G.; Joly, Y. Researchers’ Perceptions of the Ethical Implications of Pharmacogenomics Research with Children. Pub. Health Genom. 2009, 12, 191–201. [Google Scholar] [CrossRef] [Green Version]
- Kaiser, J. GENETICS: U.S. Hospital Launches Large Biobank of Children’s DNA. Science 2006, 312, 1584a–1585a. [Google Scholar] [CrossRef]
- Kaufman, D.; Geller, G.; LeRoy, L.; Murphy, J.; Scott, J.; Hudson, K. Ethical Implications of Including Children in a Large Biobank for Genetic-Epidemiologic Research: A Qualitative Study of Public Opinion. Am. J. Med. Genet. C Semin. Med. Genet. 2008, 148C, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Gurwitz, D.; Fortier, I.; Lunshof, J.; Knoppers, B. Children and Population Biobanks. Science 2009, 325, 818–819. [Google Scholar] [CrossRef] [PubMed]
- Hansson, M.; Maschke, K. Biobanks: Questioning Distinctions. Science 2009, 326, 797. [Google Scholar] [CrossRef] [PubMed]
- Hens, K.; Wright, J.; Dierickx, K. Biobanks: Oversight Offers Protection. Science 2009, 326, 798–799. [Google Scholar] [CrossRef]
- Brothers, K.B.; Clayton, E.W. Biobanks: Too Long to Wait for Consent. Science 2009, 326. [Google Scholar] [CrossRef]
- Hens, K.; Nys, H.; Cassiman, J.-J.; Dierickx, K. The return of individual research findings in paediatric genetic research. J. Med. Eth. 2011, 37, 179–183. [Google Scholar] [CrossRef] [Green Version]
- Davidson, A.J.; O’Brien, M. Ethics and Medical Research in Children. Pediatr. Anesth. 2009, 19, 994–1004. [Google Scholar] [CrossRef]
- Hens, K.; Nys, H.; Cassiman, J.-J.; Dierickx, K. Biological Sample Collections from Minors for Genetic Research: A Systematic Review of Guidelines and Position Papers. Eur. J. Hum. Genet. 2009, 17, 979–990. [Google Scholar] [CrossRef] [Green Version]
- Simon, J.; Robienski, J. Chapitre 2. Property, Personality Rights and Data Protection with regard to Biobanks—A layered system. J. Int. Bioéthique 2009, 20, 47. [Google Scholar] [CrossRef]
- Simon, J.; Robienski, J. Framework for Setting up and Operating Biobanks. Int. J. Bioeth. 2009, 20, 17–46. [Google Scholar] [CrossRef]
- Yassin, R.; Lockhart, N.; Gonzalez del Riego, M.; Pitt, K.; Thomas, J.W.; Weiss, L.; Compton, C. Custodianship as an Ethical Framework for Biospecimen-Based Research. Cancer Epidemiol. Biomark. Prev. 2010, 19, 1012–1015. [Google Scholar] [CrossRef] [Green Version]
- Williams, P.H.; Schepp, K.; McGrath, B.; Mitchell, P. The Stewardship Model: Current Viability for Genetic Biobank Practice Development. Adv. Nurs. Sci. 2010, 33, E41–E49. [Google Scholar] [CrossRef]
- Capron, A.M.; Mauron, A.; Elger, B.C.; Boggio, A.; Ganguli-Mitra, A.; Biller-Andorno, A. Ethical Norms and the International Governance of Genetic Databases and Biobanks: Findings from an International Study. Kennedy Inst. Eth. J. 2009, 19, 101–124. [Google Scholar] [CrossRef] [Green Version]
- Henderson, M.K.; Goldring, K.; Simeon-Dubach, D. Advancing Professionalization of Biobank Business Operations: A Worldwide Survey. Biopreserv. Biobank. 2019, 17, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Caulfield, T.; Murdoch, B. Genes, Cells, and Biobanks: Yes, There’s Still a Consent Problem. PLoS Biol. 2017, 15, e2002654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Souza, Y.G. Sustainability of Biobanks in the Future. Adv. Exp. Med. Biol. 2015, 864, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Betsou, F.; Bulla, A.; Cho, S.Y.; Clements, J.; Chuaqui, R.; Coppola, D.; De Souza, Y.; De Wilde, A.; Grizzle, W.; Guadagni, F. Assays for Qualification and Quality Stratification of Clinical Biospecimens Used in Research: A Technical Report from the ISBER Biospecimen Science Working Group. Biopreserv. Biobank. 2016, 14, 398–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| No. | ISO | Title | Ref. |
|---|---|---|---|
| 1 | ISO 20184-1:2018 | Specifications for pre-examination processes for snap frozen tissue. Part 1: Isolated RNA | [27] |
| 2 | ISO 20184-2:2018 | Specifications for pre-examination processes for snap frozen tissue. Part 2: Isolated proteins | [28] |
| 3 | ISO 20166-1:2018 | Specifications for pre-examination processes for FFPE tissue. Part 1: Isolated RNA | [29] |
| 4 | ISO 20166-2:2018 | Specifications for pre-examination processes for FFPE tissue. Part 2: Isolated proteins | [30] |
| 5 | ISO 20166-3:2018 | Specifications for pre-examination processes for FFPE tissue. Part 3: Isolated DNA | [31] |
| 6 | ISO 20186-1:2019 | Specifications for pre-examination processes for venous whole blood. Part 1: Isolated cellular RNA | [32] |
| 7 | ISO 20186-2:2019 | Specifications for pre-examination processes for venous whole blood. Part 2: Isolated genomic DNA | [33] |
| 8 | ISO 20186-3:2019 | Specifications for pre-examination processes for venous whole blood. Part 3: Isolated circulating cell free DNA from plasma | [34] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malsagova, K.; Kopylov, A.; Stepanov, A.; Butkova, T.; Sinitsyna, A.; Izotov, A.; Kaysheva, A. Biobanks—A Platform for Scientific and Biomedical Research. Diagnostics 2020, 10, 485. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10070485
Malsagova K, Kopylov A, Stepanov A, Butkova T, Sinitsyna A, Izotov A, Kaysheva A. Biobanks—A Platform for Scientific and Biomedical Research. Diagnostics. 2020; 10(7):485. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10070485
Chicago/Turabian StyleMalsagova, Kristina, Artur Kopylov, Alexander Stepanov, Tatyana Butkova, Alexandra Sinitsyna, Alexander Izotov, and Anna Kaysheva. 2020. "Biobanks—A Platform for Scientific and Biomedical Research" Diagnostics 10, no. 7: 485. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10070485