Impact of H19 Polymorphisms on Prostate Cancer Clinicopathologic Characteristics

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Specimen Collection and DNA Extraction
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Study Participants
3.2. Association of H19 Polymorphisms with Risk and Clinical Features of Prostate Cancer
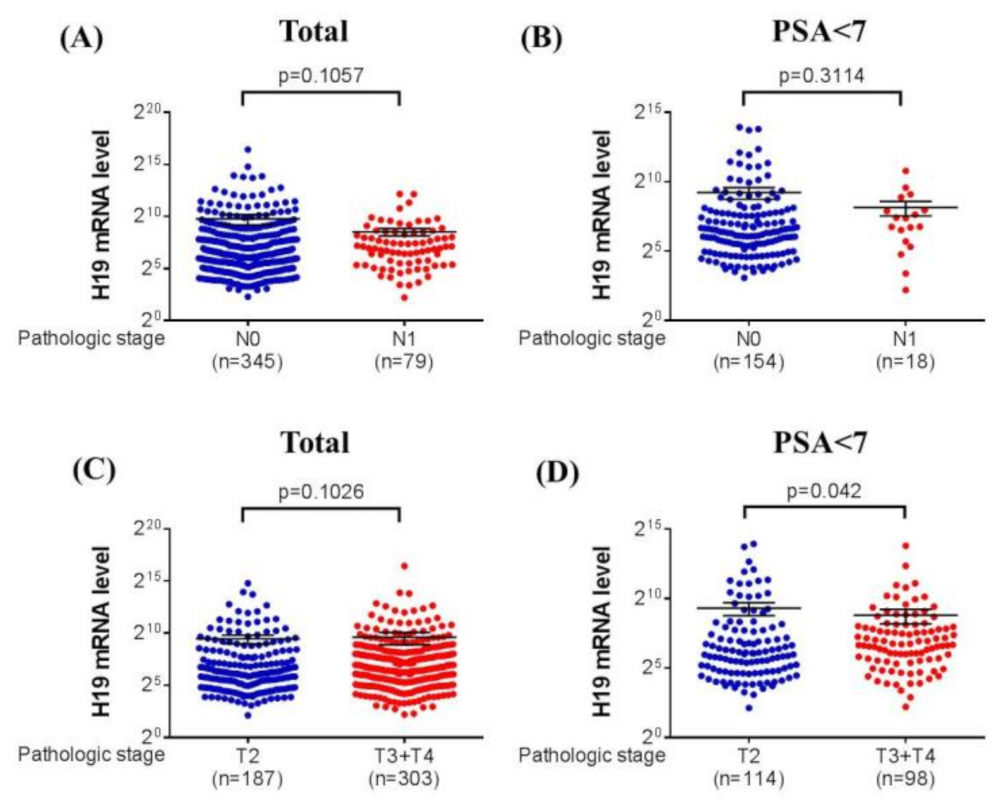
3.3. Association between H19 mRNA Expression and Clinical Characteristics of Prostate Cancer from TCGA Database
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, M.C.; Goggins, W.B.; Wang, H.H.; Fung, F.D.; Leung, C.; Wong, S.Y.; Ng, C.F.; Sung, J.J. Global incidence and mortality for prostate cancer: Analysis of temporal patterns and trends in 36 countries. Eur. Urol. 2016, 70, 862–874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [Green Version]
- Hankey, B.F.; Feuer, E.J.; Clegg, L.X.; Hayes, R.B.; Legler, J.M.; Prorok, P.C.; Ries, L.A.; Merrill, R.M.; Kaplan, R.S. Cancer surveillance series: Interpreting trends in prostate cancer—Part I: Evidence of the effects of screening in recent prostate cancer incidence, mortality, and survival rates. J. Natl. Cancer Inst. 1999, 91, 1017–1024. [Google Scholar] [CrossRef]
- Zhou, C.K.; Check, D.P.; Lortet-Tieulent, J.; Laversanne, M.; Jemal, A.; Ferlay, J.; Bray, F.; Cook, M.B.; Devesa, S.S. Prostate cancer incidence in 43 populations worldwide: An analysis of time trends overall and by age group. Int. J. Cancer 2016, 138, 1388–1400. [Google Scholar] [CrossRef] [PubMed]
- Fenton, J.J.; Weyrich, M.S.; Durbin, S.; Liu, Y.; Bang, H.; Melnikow, J. Prostate-specific antigen-based screening for prostate cancer: Evidence report and systematic review for the us preventive services task force. JAMA 2018, 319, 1914–1931. [Google Scholar] [CrossRef]
- Wallis, C.J.D.; Glaser, A.; Hu, J.C.; Huland, H.; Lawrentschuk, N.; Moon, D.; Murphy, D.G.; Nguyen, P.L.; Resnick, M.J.; Nam, R.K. Survival and complications following surgery and radiation for localized prostate cancer: An international collaborative review. Eur. Urol. 2018, 73, 11–20. [Google Scholar] [CrossRef]
- Carlsson, S.; Drevin, L.; Loeb, S.; Widmark, A.; Lissbrant, I.F.; Robinson, D.; Johansson, E.; Stattin, P.; Fransson, P. Population-based study of long-term functional outcomes after prostate cancer treatment. BJU Int. 2016, 117, E36–E45. [Google Scholar] [CrossRef]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A. The 2014 international society of urological pathology (isup) consensus conference on gleason grading of prostatic carcinoma: Definition of grading patterns and proposal for a new grading system. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef]
- Epstein, J.I.; Zelefsky, M.J.; Sjoberg, D.D.; Nelson, J.B.; Egevad, L.; Magi-Galluzzi, C.; Vickers, A.J.; Parwani, A.V.; Reuter, V.E.; Fine, S.W.; et al. A contemporary prostate cancer grading system: A validated alternative to the gleason score. Eur. Urol. 2016, 69, 428–435. [Google Scholar] [CrossRef] [Green Version]
- Caster, J.M.; Falchook, A.D.; Hendrix, L.H.; Chen, R.C. Risk of pathologic upgrading or locally advanced disease in early prostate cancer patients based on biopsy gleason score and psa: A population-based study of modern patients. Int. J. Radiat. Oncol. Biol. Phys. 2015, 92, 244–251. [Google Scholar] [CrossRef] [PubMed]
- You, J.S.; Jones, P.A. Cancer genetics and epigenetics: Two sides of the same coin? Cancer Cell 2012, 22, 9–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, D.; Van Allen, E.M.; Wu, Y.M.; Schultz, N.; Lonigro, R.J.; Mosquera, J.M.; Montgomery, B.; Taplin, M.E.; Pritchard, C.C.; Attard, G.; et al. Integrative clinical genomics of advanced prostate cancer. Cell 2015, 161, 1215–1228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pritchard, C.C.; Mateo, J.; Walsh, M.F.; De Sarkar, N.; Abida, W.; Beltran, H.; Garofalo, A.; Gulati, R.; Carreira, S.; Eeles, R.; et al. Inherited DNA-repair gene mutations in men with metastatic prostate cancer. N. Engl. J. Med. 2016, 375, 443–453. [Google Scholar] [CrossRef]
- Castro, E.; Romero-Laorden, N.; Del Pozo, A.; Lozano, R.; Medina, A.; Puente, J.; Piulats, J.M.; Lorente, D.; Saez, M.I.; Morales-Barrera, R.; et al. Prorepair-b: A prospective cohort study of the impact of germline DNA repair mutations on the outcomes of patients with metastatic castration-resistant prostate cancer. J. Clin. Oncol. 2019, 37, 490–503. [Google Scholar] [CrossRef]
- Giri, V.N.; Knudsen, K.E.; Kelly, W.K.; Abida, W.; Andriole, G.L.; Bangma, C.H.; Bekelman, J.E.; Benson, M.C.; Blanco, A.; Burnett, A.; et al. Role of genetic testing for inherited prostate cancer risk: Philadelphia prostate cancer consensus conference 2017. J. Clin. Oncol. 2018, 36, 414–424. [Google Scholar] [CrossRef]
- Wang, K.C.; Yang, Y.W.; Liu, B.; Sanyal, A.; Corces-Zimmerman, R.; Chen, Y.; Lajoie, B.R.; Protacio, A.; Flynn, R.A.; Gupta, R.A.; et al. A long noncoding rna maintains active chromatin to coordinate homeotic gene expression. Nature 2011, 472, 120–124. [Google Scholar] [CrossRef] [Green Version]
- Mancini-DiNardo, D.; Steele, S.J.; Ingram, R.S.; Tilghman, S.M. A differentially methylated region within the gene kcnq1 functions as an imprinted promoter and silencer. Hum. Mol. Genet. 2003, 12, 283–294. [Google Scholar] [CrossRef]
- Sun, M.; Kraus, W.L. From discovery to function: The expanding roles of long noncoding rnas in physiology and disease. Endocr. Rev. 2015, 36, 25–64. [Google Scholar] [CrossRef] [Green Version]
- Arriaga-Canon, C.; De La Rosa-Velazquez, I.A.; Gonzalez-Barrios, R.; Montiel-Manriquez, R.; Oliva-Rico, D.; Jimenez-Trejo, F.; Cortes-Gonzalez, C.; Herrera, L.A. The use of long non-coding rnas as prognostic biomarkers and therapeutic targets in prostate cancer. Oncotarget 2018, 9, 20872–20890. [Google Scholar] [CrossRef] [Green Version]
- Walsh, A.L.; Tuzova, A.V.; Bolton, E.M.; Lynch, T.H.; Perry, A.S. Long noncoding rnas and prostate carcinogenesis: The missing ‘linc’? Trends Mol. Med. 2014, 20, 428–436. [Google Scholar] [CrossRef] [PubMed]
- Ramnarine, V.R.; Kobelev, M.; Gibb, E.A.; Nouri, M.; Lin, D.; Wang, Y.; Buttyan, R.; Davicioni, E.; Zoubeidi, A.; Collins, C.C. The evolution of long noncoding rna acceptance in prostate cancer initiation, progression, and its clinical utility in disease management. Eur. Urol. 2019, 76, 546–559. [Google Scholar] [CrossRef] [PubMed]
- Flippot, R.; Beinse, G.; Boileve, A.; Vibert, J.; Malouf, G.G. Long non-coding rnas in genitourinary malignancies: A whole new world. Nat. Rev. Urol. 2019, 16, 484–504. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.T.; Pan, H.; Xia, G.F.; Qiu, C.; Zhu, Z.M. Prognostic and clinicopathological significance of long noncoding rna h19 overexpression in human solid tumors: Evidence from a meta-analysis. Oncotarget 2016, 7, 83177–83186. [Google Scholar] [CrossRef]
- Raveh, E.; Matouk, I.J.; Gilon, M.; Hochberg, A. The h19 long non-coding rna in cancer initiation, progression and metastasis—A proposed unifying theory. Mol. Cancer 2015, 14, 184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghafouri-Fard, S.; Esmaeili, M.; Taheri, M. H19 lncrna: Roles in tumorigenesis. Biomed. Pharmacother. 2020, 123, 109774. [Google Scholar] [CrossRef]
- Bacci, L.; Aiello, A.; Ripoli, C.; Loria, R.; Pugliese, D.; Pierconti, F.; Rotili, D.; Strigari, L.; Pinto, F.; Bassi, P.F.; et al. H19-dependent transcriptional regulation of beta3 and beta4 integrins upon estrogen and hypoxia favors metastatic potential in prostate cancer. Int. J. Mol. Sci. 2019, 20, 4012. [Google Scholar] [CrossRef] [Green Version]
- Berteaux, N.; Lottin, S.; Adriaenssens, E.; Van Coppenolle, F.; Leroy, X.; Coll, J.; Dugimont, T.; Curgy, J.J. Hormonal regulation of h19 gene expression in prostate epithelial cells. J. Endocrinol. 2004, 183, 69–78. [Google Scholar] [CrossRef]
- Bauderlique-Le Roy, H.; Vennin, C.; Brocqueville, G.; Spruyt, N.; Adriaenssens, E.; Bourette, R.P. Enrichment of human stem-like prostate cells with s-ship promoter activity uncovers a role in stemness for the long noncoding rna h19. Stem Cells Dev. 2015, 24, 1252–1262. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Zhao, Y.; Li, Y.; Zhang, J. Quantitative assessment of lncrna h19 polymorphisms and cancer risk: A meta-analysis based on 48,166 subjects. Artif. Cells Nanomed. Biotechnol. 2020, 48, 15–27. [Google Scholar] [CrossRef]
- Verhaegh, G.W.; Verkleij, L.; Vermeulen, S.H.; den Heijer, M.; Witjes, J.A.; Kiemeney, L.A. Polymorphisms in the h19 gene and the risk of bladder cancer. Eur. Urol. 2008, 54, 1118–1126. [Google Scholar] [CrossRef] [PubMed]
- Yang, P.J.; Hsieh, M.J.; Hung, T.W.; Wang, S.S.; Chen, S.C.; Lee, M.C.; Yang, S.F.; Chou, Y.E. Effects of long noncoding rna h19 polymorphisms on urothelial cell carcinoma development. Int. J. Environ. Res. Public Health 2019, 16, 1322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, E.R.; Chou, Y.E.; Liu, Y.F.; Hsueh, K.C.; Lee, H.L.; Yang, S.F.; Su, S.C. Association of lncrna h19 gene polymorphisms with the occurrence of hepatocellular carcinoma. Genes 2019, 10, 506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, M.C.; Chou, Y.H.; Shen, H.P.; Ng, S.C.; Lee, Y.C.; Sun, Y.H.; Hsu, C.F.; Yang, S.F.; Wang, P.H. The clinicopathological characteristic associations of long non-coding rna gene h19 polymorphisms with uterine cervical cancer. J. Cancer 2019, 10, 6191–6198. [Google Scholar] [CrossRef]
- D’Amico, A.V.; Whittington, R.; Malkowicz, S.B.; Schultz, D.; Blank, K.; Broderick, G.A.; Tomaszewski, J.E.; Renshaw, A.A.; Kaplan, I.; Beard, C.J.; et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA 1998, 280, 969–974. [Google Scholar] [CrossRef]
- Elshafei, A.; Li, Y.H.; Hatem, A.; Moussa, A.S.; Ethan, V.; Krishnan, N.; Li, J.; Jones, J.S. The utility of psa velocity in prediction of prostate cancer and high grade cancer after an initially negative prostate biopsy. Prostate 2013, 73, 1796–1802. [Google Scholar] [CrossRef]
- Li, X.F.; Yin, X.H.; Cai, J.W.; Wang, M.J.; Zeng, Y.Q.; Li, M.; Niu, Y.M.; Shen, M. Significant association between lncrna h19 polymorphisms and cancer susceptibility: A meta-analysis. Oncotarget 2017, 8, 45143–45153. [Google Scholar] [CrossRef] [Green Version]
- Gittelman, M.C.; Hertzman, B.; Bailen, J.; Williams, T.; Koziol, I.; Henderson, R.J.; Efros, M.; Bidair, M.; Ward, J.F. Pca3 molecular urine test as a predictor of repeat prostate biopsy outcome in men with previous negative biopsies: A prospective multicenter clinical study. J. Urol. 2013, 190, 64–69. [Google Scholar] [CrossRef]
- de la Calle, C.; Patil, D.; Wei, J.T.; Scherr, D.S.; Sokoll, L.; Chan, D.W.; Siddiqui, J.; Mosquera, J.M.; Rubin, M.A.; Sanda, M.G. Multicenter evaluation of the prostate health index to detect aggressive prostate cancer in biopsy naïve men. J. Urol. 2015, 194, 65–72. [Google Scholar] [CrossRef] [Green Version]
- Ferro, M.; De Cobelli, O.; Lucarelli, G.; Porreca, A.; Busetto, G.M.; Cantiello, F.; Damiano, R.; Autorino, R.; Musi, G.; Vartolomei, M.D.; et al. Beyond psa: The role of prostate health index (phi). Int. J. Mol. Sci. 2020, 21, 1184. [Google Scholar] [CrossRef] [Green Version]
- Ferro, M.; Musi, G.; Serino, A.; Cozzi, G.; Mistretta, F.A.; Costa, B.; Bianchi, R.; Cordima, G.; Luzzago, S.; Di Trapani, E.; et al. Neutrophil, platelets, and eosinophil to lymphocyte ratios predict gleason score upgrading in low-risk prostate cancer patients. Urol. Int. 2019, 102, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Ferro, M.; Lucarelli, G.; de Cobelli, O.; Vartolomei, M.D.; Damiano, R.; Cantiello, F.; Crocerossa, F.; Perdonà, S.; Del Prete, P.; Cordima, G.; et al. Circulating preoperative testosterone level predicts unfavourable disease at radical prostatectomy in men with international society of urological pathology grade group 1 prostate cancer diagnosed with systematic biopsies. World J. Urol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.; Ahmed, M.; Zhang, F.; Yao, C.Q.; Li, S.; Liang, Y.; Hua, J.; Soares, F.; Sun, Y.; Langstein, J.; et al. Modulation of long noncoding rnas by risk snps underlying genetic predispositions to prostate cancer. Nat. Genet. 2016, 48, 1142–1150. [Google Scholar] [CrossRef] [PubMed]
- Mouraviev, V.; Lee, B.; Patel, V.; Albala, D.; Johansen, T.E.; Partin, A.; Ross, A.; Perera, R.J. Clinical prospects of long noncoding rnas as novel biomarkers and therapeutic targets in prostate cancer. Prostate Cancer Prostatic Dis. 2016, 19, 14–20. [Google Scholar] [CrossRef]
- Lin, C.Y.; Wang, S.S.; Yang, C.K.; Li, J.R.; Chen, C.S.; Hung, S.C.; Chiu, K.Y.; Cheng, C.L.; Ou, Y.C.; Yang, S.F. Impact of gas5 genetic polymorphism on prostate cancer susceptibility and clinicopathologic characteristics. Int. J. Med. Sci. 2019, 16, 1424–1429. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.H.; Zhang, B.Y.; Zhou, B.; Zhu, C.Z.; Sun, L.Q.; Feng, Y.J. Perineural invasion of cancer: A complex crosstalk between cells and molecules in the perineural niche. Am. J. Cancer Res. 2019, 9, 1–21. [Google Scholar]
- Harnden, P.; Shelley, M.D.; Clements, H.; Coles, B.; Tyndale-Biscoe, R.S.; Naylor, B.; Mason, M.D. The prognostic significance of perineural invasion in prostatic cancer biopsies: A systematic review. Cancer 2007, 109, 13–24. [Google Scholar] [CrossRef]
- Peng, L.C.; Narang, A.K.; Gergis, C.; Radwan, N.A.; Han, P.; Marciscano, A.E.; Robertson, S.P.; He, P.; Trieu, J.; Ram, A.N.; et al. Effects of perineural invasion on biochemical recurrence and prostate cancer-specific survival in patients treated with definitive external beam radiotherapy. Urol. Oncol. 2018, 36, 309.e7–309.e14. [Google Scholar] [CrossRef]
- Zheng, S.L.; Sun, J.; Wiklund, F.; Smith, S.; Stattin, P.; Li, G.; Adami, H.O.; Hsu, F.C.; Zhu, Y.; Balter, K.; et al. Cumulative association of five genetic variants with prostate cancer. N. Engl. J. Med. 2008, 358, 910–919. [Google Scholar] [CrossRef] [Green Version]
- Loeb, S.; Carter, H.B.; Walsh, P.C.; Isaacs, W.B.; Kettermann, A.; Tanaka, T.; Ferrucci, L.; Metter, E.J. Single nucleotide polymorphisms and the likelihood of prostate cancer at a given prostate specific antigen level. J. Urol. 2009, 182, 101–104. [Google Scholar] [CrossRef]
- Li-Sheng Chen, S.; Ching-Yuan Fann, J.; Sipeky, C.; Yang, T.K.; Yueh-Hsia Chiu, S.; Ming-Fang Yen, A.; Laitinen, V.; Tammela, T.L.J.; Stenman, U.H.; Auvinen, A.; et al. Risk prediction of prostate cancer with single nucleotide polymorphisms and prostate specific antigen. J. Urol. 2019, 201, 486–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lecerf, C.; Le Bourhis, X.; Adriaenssens, E. The long non-coding rna h19: An active player with multiple facets to sustain the hallmarks of cancer. Cell Mol. Life Sci. 2019, 76, 4673–4687. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | PSA at Diagnosis (ng/mL) | ||
|---|---|---|---|
| <7 (n = 153) | 7–10 (n = 117) | >10 (n = 309) | |
| Age at diagnosis (years) | |||
| <65 | 71 (46.4%) | 61 (52.1%) | 113 (36.6%) |
| >65 | 82 (53.6%) | 56 (47.9%) | 196 (63.4%) |
| Pathologic Gleason grade group | |||
| 1 + 2 + 3 | 142 (92.8%) | 108 (92.3%) | 234 (75.7%) |
| 4 + 5 | 11 (7.2%) | 9 (7.7%) | 75 (24.3%) |
| Clinical T stage | |||
| 1 + 2 | 144 (94.1%) | 109 (93.2%) | 248 (80.3%) |
| 3 + 4 | 9 (5.9%) | 8 (6.8%) | 61 (19.7%) |
| Clinical n stage | |||
| N0 | 152 (99.3%) | 115 (98.3%) | 299 (96.8%) |
| N1 | 1 (0.7%) | 2 (1.7%) | 10 (3.2%) |
| Clinical M stage | |||
| M0 | 153 (100.0%) | 117 (100.0%) | 299 (96.8%) |
| M1 | 0 (0.0%) | 0 (0.0%) | 10 (3.2%) |
| Pathologic T stage | |||
| 2 | 114 (74.5%) | 72 (61.5%) | 120 (38.8%) |
| 3 + 4 | 39 (25.5%) | 45 (38.5%) | 189 (61.2%) |
| Pathologic n stage | |||
| N0 | 146 (95.4%) | 113 (96.6%) | 384 (87.7%) |
| N1 | 7 (4.6%) | 4 (3.4%) | 38 (12.3%) |
| Extraprostatic extension | |||
| No | 107 (69.9%) | 71 (60.7%) | 148 (47.9%) |
| Yes | 46 (30.1%) | 46 (39.3%) | 161 (52.1%) |
| Seminal vesicle invasion | |||
| No | 145 (94.8%) | 99 (84.6%) | 208 (67.3%) |
| Yes | 8 (5.2%) | 18 (15.4%) | 101 (32.7%) |
| Perineural invasion | |||
| No | 53 (34.6%) | 40 (34.2%) | 62 (20.1%) |
| Yes | 100 (65.4%) | 77 (65.8%) | 247 (79.9%) |
| Lymphovascular invasion | |||
| No | 145 (94.8%) | 101 (86.3%) | 236 (76.4%) |
| Yes | 8 (5.2%) | 16 (13.7%) | 73 (23.6%) |
| D’Amico classification | |||
| Low risk | 41 (26.8%) | 19 (16.2%) | 0 (0.0%) |
| Intermediate risk | 64 (41.8%) | 66 (56.4%) | 90 (29.1%) |
| High risk | 48 (31.4%) | 32 (27.4%) | 219 (70.9%) |
| Variable | PSA at Diagnosis (ng/mL) | ||||
|---|---|---|---|---|---|
| <7 (n = 153) | 7–10 (n = 117) | >10 (n = 309) | AOR (95% CI) a | AOR (95% CI) b | |
| rs2177727 | |||||
| CC | 69 (45.1%) | 47 (40.2%) | 133 (43.0%) | 1.00 | 1.00 |
| CT | 71 (46.4%) | 50 (42.7%) | 140 (45.3%) | 0.832 (0.475–1.460) | 0.894 (0.553–1.445) |
| TT | 13 (8.5%) | 20 (17.1%) | 36 (11.7%) | 2.197 (0.971–4.971) | 1.297 (0.583–2.887) |
| CT+TT | 84 (54.9%) | 70 (59.8%) | 176 (57.0%) | 1.054 (0.627–1.771) | 0.960 (0.609–1.514) |
| rs2107425 | |||||
| CC | 57 (37.3%) | 41 (35.0%) | 111 (35.9%) | 1.00 | 1.00 |
| CT | 75 (49.0%) | 52 (44.4%) | 143 (46.3%) | 0.839 (0.476–1.480) | 0.879 (0.535–1.446) |
| TT | 21 (13.7%) | 24 (20.5%) | 55 (17.8%) | 1.537 (0.731–3.231) | 1.121 (0.564–2.230) |
| CT+TT | 96 (62.7%) | 76 (65.0%) | 198 (64.1%) | 0.991 (0.584–1.681) | 0.934 (0.584–1.494) |
| rs2839698 | |||||
| CC | 74 (48.4%) | 56 (47.9%) | 149 (48.2%) | 1.00 | 1.00 |
| CT | 65 (42.5%) | 53 (45.3%) | 135 (43.7%) | 1.063 (0.628–1.799) | 1.108 (0.691–1.777) |
| TT | 14 (9.2%) | 8 (6.8%) | 25 (8.1%) | 0.915 (0.343–2.441) | 1.064 (0.467–2.424) |
| CT+TT | 79 (51.6%) | 61 (52.1%) | 160 (51.8%) | 1.040 (0.627–1.724) | 1.100 (0.701–1.728) |
| rs3024270 | |||||
| CC | 38 (24.8%) | 37 (31.6%) | 92 (29.8%) | 1.00 | 1.00 |
| CG | 84 (54.9%) | 55 (47.0%) | 144 (46.6%) | 0.595 (0.324–1.092) | 0.791 (0.463–1.351) |
| GG | 31 (20.3%) | 25 (21.4%) | 73 (23.6%) | 0.934 (0.449–1.941) | 1.040 (0.543–1.991) |
| CG+GG | 115 (75.2%) | 80 (68.4%) | 217 (70.2%) | 0.683 (0.387–1.206) | 0.860 (0.518–1.427) |
| rs3741219 | |||||
| AA | 69 (45.1%) | 55 (47.0%) | 146 (47.2%) | 1.00 | 1.00 |
| AG | 67 (43.8%) | 53 (45.3%) | 135 (43.7%) | 0.977 (0.575–1.661) | 1.001 (0.622–1.611) |
| GG | 17 (11.1%) | 9 (7.7%) | 28 (9.1%) | 0.819 (0.325–2.068) | 0.896 (0.408–1.967) |
| AG+GG | 84 (54.9%) | 62 (53.0%) | 163 (52.8%) | 0.949 (0.571–1.579) | 0.981 (0.623–1.544) |
| Variable | Genotypic Frequencies | |||
|---|---|---|---|---|
| rs3024270 | CC (n = 38) | CG+GG (n = 115) | OR (95% CI) | p Value |
| Pathologic Gleason grade group | ||||
| 1 + 2 + 3 | 36 (94.7%) | 106 (92.2%) | 1.00 | p = 0.732 |
| 4 + 5 | 2 (5.3%) | 9 (7.8%) | 1.528 (0.315–7.406) | |
| Clinical T stage | ||||
| 1 + 2 | 34 (89.5%) | 110 (95.7%) | 1.00 | p = 0.227 |
| 3 + 4 | 4 (10.5%) | 5 (4.3%) | 0.386 (0.098–1.520) | |
| Pathologic T stage | ||||
| 2 | 33 (86.8%) | 81 (70.4%) | 1.00 | p = 0.053 |
| 3 + 4 | 5 (13.2%) | 34 (29.6%) | 2.770 (0.997–7.701) | |
| Pathologic n stage | ||||
| N0 | 37 (97.4%) | 109 (94.8%) | 1.00 | p = 0.682 |
| N1 | 1 (2.6%) | 6 (5.2%) | 2.037 (0.237–17.478) | |
| Extraprostatic extension | ||||
| No | 34 (89.5%) | 73 (63.5%) | 1.00 | p = 0.002 * |
| Yes | 4 (10.5%) | 42 (36.5%) | 4.890 (1.622–14.741) | |
| Seminal vesicle invasion | ||||
| No | 37 (97.4%) | 108 (93.9%) | 1.00 | p = 0.680 |
| Yes | 1 (2.6%) | 7 (6.1%) | 2.398 (0.285–20.146) | |
| Perineural invasion | ||||
| No | 20 (52.6%) | 33 (28.7%) | 1.00 | p = 0.010 * |
| Yes | 18 (47.4%) | 82 (71.3%) | 2.761 (1.299–5.869) | |
| Lymphovascular invasion | ||||
| No | 37 (97.4%) | 108 (93.9%) | 1.00 | p = 0.680 |
| Yes | 1 (2.6%) | 7 (6.1%) | 2.398 (0.285–20.146) | |
| D’Amico classification | ||||
| Low/Intermediate risk | 24 (63.2%) | 81 (70.4%) | 1.00 | p = 0.425 |
| High risk | 14 (36.8%) | 34 (29.6%) | 0.720 (0.333–1.556) | |
| Total score upgrade | ||||
| No | 21 (55.3%) | 66 (57.4%) | 1.00 | p = 0.852 |
| Yes | 17 (44.7%) | 49 (42.6%) | 0.917 (0.438–1.919) | |
| Grade group upgrade | ||||
| No | 20 (52.6%) | 64 (55.7%) | 1.00 | p = 0.851 |
| Yes | 18 (47.4%) | 51 (44.3%) | 0.885 (0.424–1.847) | |
| Variable | Genotypic Frequencies | |||
|---|---|---|---|---|
| rs3741219 | AA (n = 69) | AG+GG (n = 84) | OR (95% CI) | p Value |
| Pathologic Gleason grade group | ||||
| 1 + 2 + 3 | 64 (92.8%) | 78 (92.9%) | 1.00 | p = 0.610 |
| 4 + 5 | 5 (7.2%) | 6 (7.1%) | 0.985 (0.287–3.375) | |
| Clinical T stage | ||||
| 1 + 2 | 64 (92.8%) | 80 (95.2%) | 1.00 | p = 0.732 |
| 3 + 4 | 5 (7.2%) | 4 (4.8%) | 0.640 (0.165–2.482) | |
| Pathologic T stage | ||||
| 2 | 55 (79.7%) | 59 (70.2%) | 1.00 | p = 0.197 |
| 3 + 4 | 14 (20.3%) | 25 (29.8%) | 1.665 (0.287–3.375) | |
| Pathologic n stage | ||||
| N0 | 65 (94.2%) | 81 (96.4%) | 1.00 | p = 0.702 |
| N1 | 4 (5.8%) | 3 (3.6%) | 0.602 (0.130–2.785) | |
| Extraprostatic extension | ||||
| No | 48 (69.6%) | 59 (70.2%) | 1.00 | p = 0.534 |
| Yes | 21 (30.4%) | 25 (29.8%) | 0.969 (0.484–1.939) | |
| Seminal vesicle invasion | ||||
| No | 64 (92.8%) | 81 (96.4%) | 1.00 | p = 0.469 |
| Yes | 5 (7.2%) | 3 (3.6%) | 0.474 (0.109–2.059) | |
| Perineural invasion | ||||
| No | 31 (44.9%) | 22 (26.2%) | 1.00 | p = 0.018 * |
| Yes | 38 (55.1%) | 62 (73.8%) | 2.299 (1.165–4.535) | |
| Lymphovascular invasion | ||||
| No | 64 (92.8%) | 81 (96.4%) | 1.00 | p = 0.469 |
| Yes | 5 (7.2%) | 3 (3.6%) | 0.474 (0.109–2.059) | |
| D’Amico classification | ||||
| Low/Intermediate risk | 46 (66.7%) | 59 (70.2%) | 1.00 | p = 0.727 |
| High risk | 23 (33.3%) | 25 (29.8%) | 0.847 (0.427–1.681) | |
| Total score upgrade | ||||
| No | 42 (60.9%) | 45 (53.6%) | 1.00 | p = 0.414 |
| Yes | 27 (39.1%) | 39 (46.4%) | 1.348 (0.706–2.573) | |
| Grade group upgrade | ||||
| No | 40 (58.0%) | 44 (52.4%) | 1.00 | p = 0.517 |
| Yes | 29 (42.0%) | 40 (47.6%) | 1.254 (0.600–2.382) | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hu, J.-C.; Lin, C.-Y.; Wang, S.-S.; Chiu, K.-Y.; Li, J.-R.; Chen, C.-S.; Hung, S.-C.; Yang, C.-K.; Ou, Y.-C.; Cheng, C.-L.; et al. Impact of H19 Polymorphisms on Prostate Cancer Clinicopathologic Characteristics. Diagnostics 2020, 10, 656. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10090656
Hu J-C, Lin C-Y, Wang S-S, Chiu K-Y, Li J-R, Chen C-S, Hung S-C, Yang C-K, Ou Y-C, Cheng C-L, et al. Impact of H19 Polymorphisms on Prostate Cancer Clinicopathologic Characteristics. Diagnostics. 2020; 10(9):656. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10090656
Chicago/Turabian StyleHu, Ju-Chuan, Chia-Yen Lin, Shian-Shiang Wang, Kun-Yuan Chiu, Jian-Ri Li, Chuan-Shu Chen, Sheng-Chun Hung, Cheng-Kuang Yang, Yen-Chuan Ou, Chen-Li Cheng, and et al. 2020. "Impact of H19 Polymorphisms on Prostate Cancer Clinicopathologic Characteristics" Diagnostics 10, no. 9: 656. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10090656