Correlation between Blood Flow and Temperature of the Ocular Anterior Segment in Normal Subjects

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Subjects
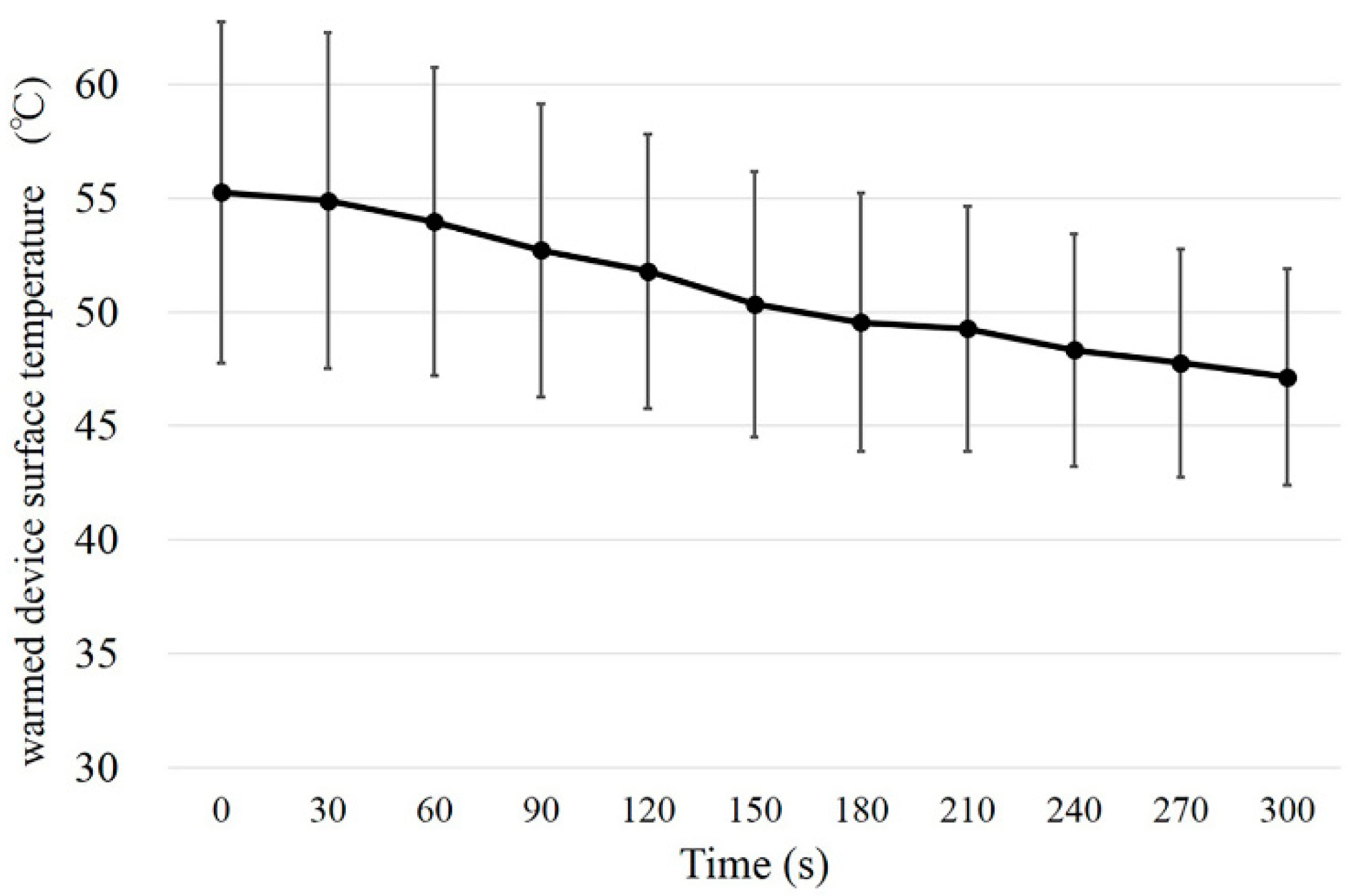
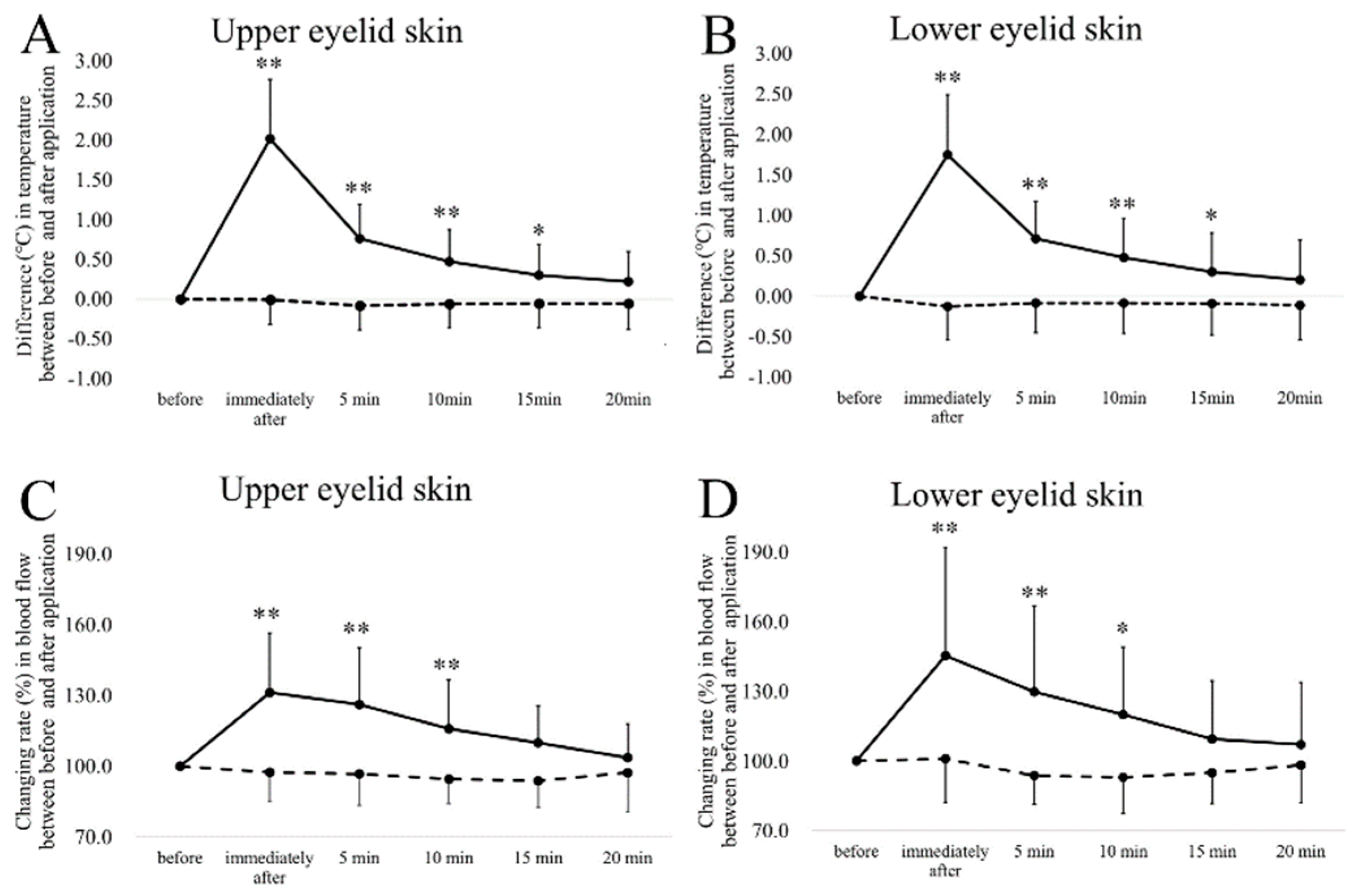
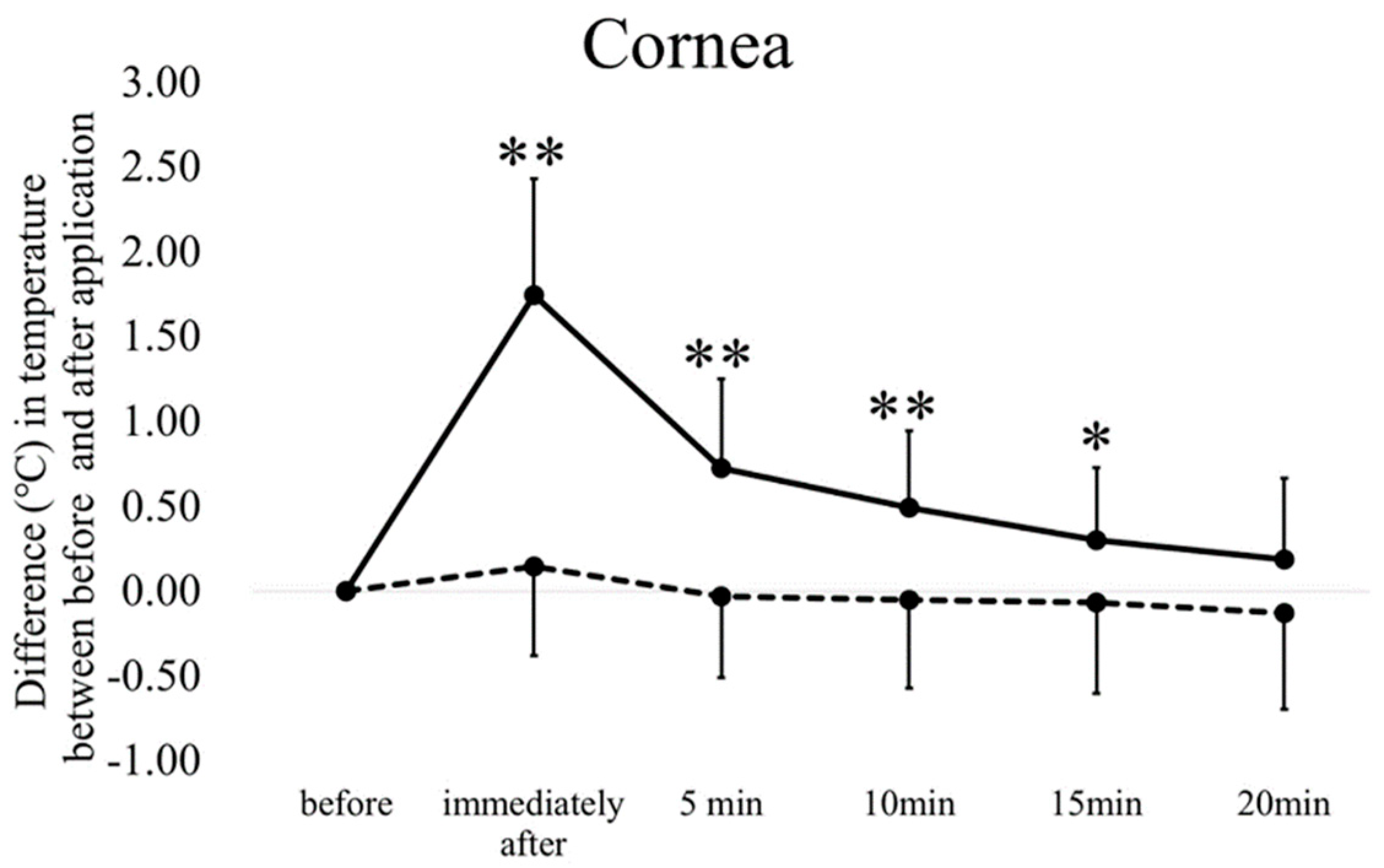
2.2. Experiment 1
2.3. Experiment 2
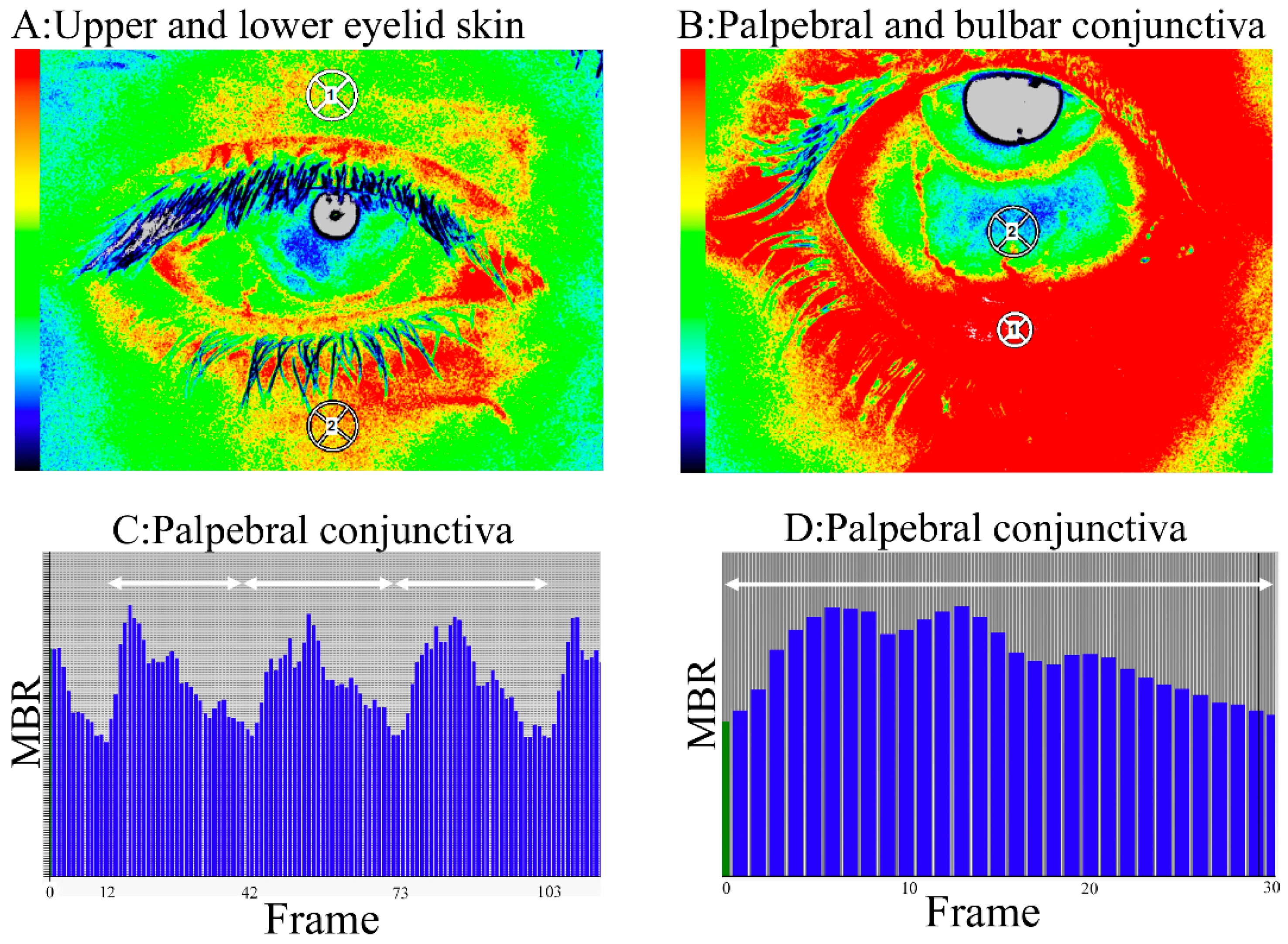
2.4. Blood flow Measurement by LSFG
2.5. Temperature Measurements
2.6. Measurement of Tear Film Stability
2.7. Statistical Analysis
3. Results
3.1. Experiment 1
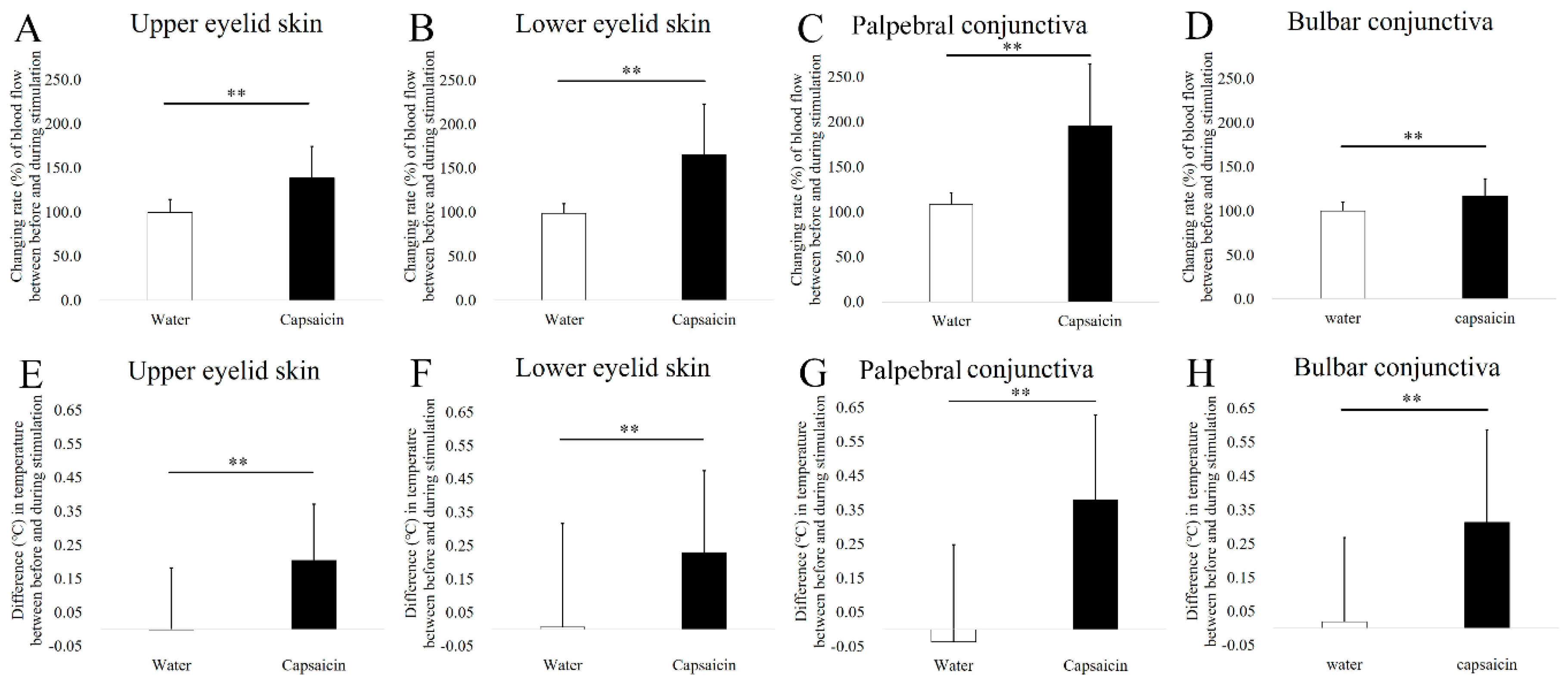
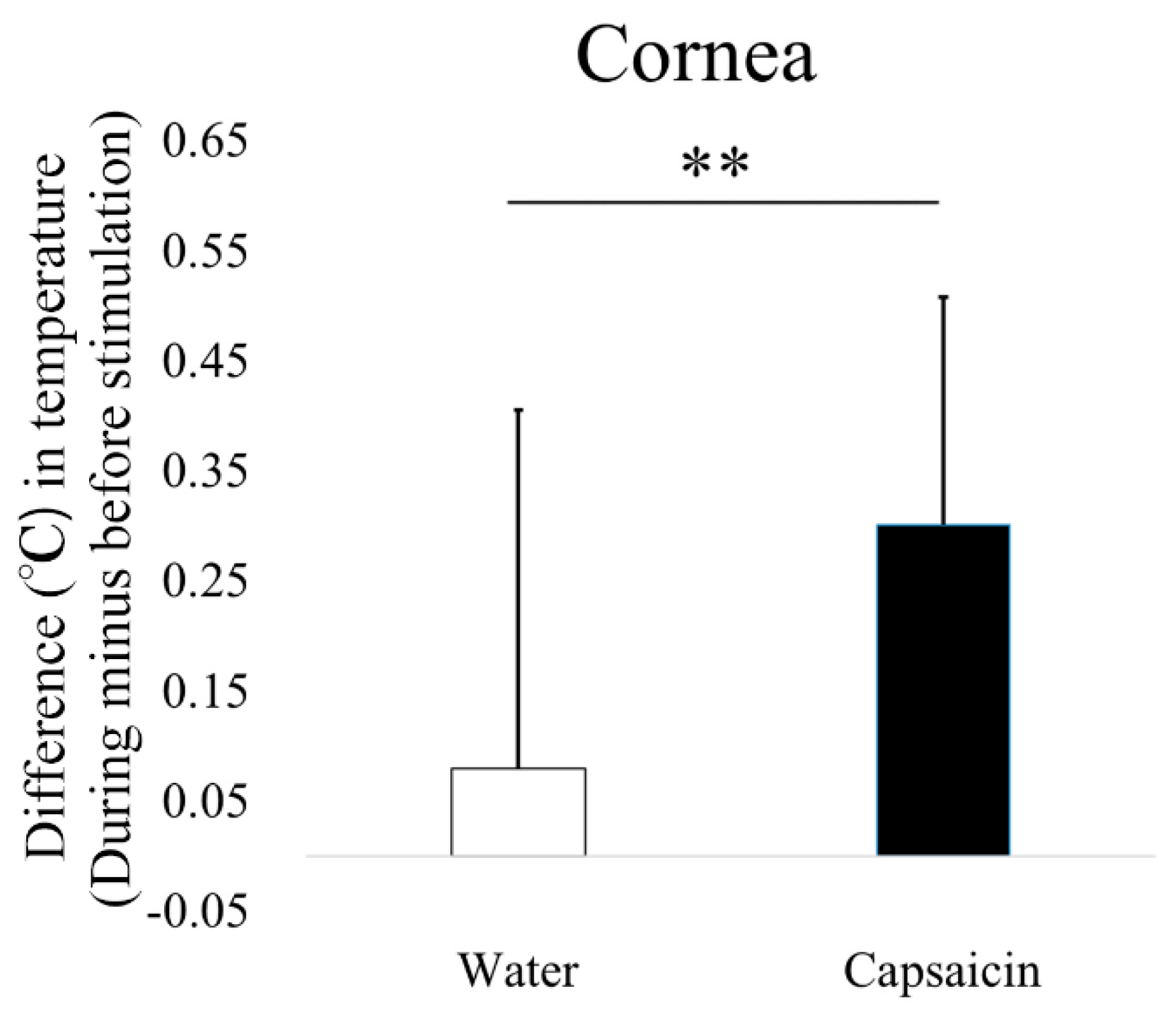
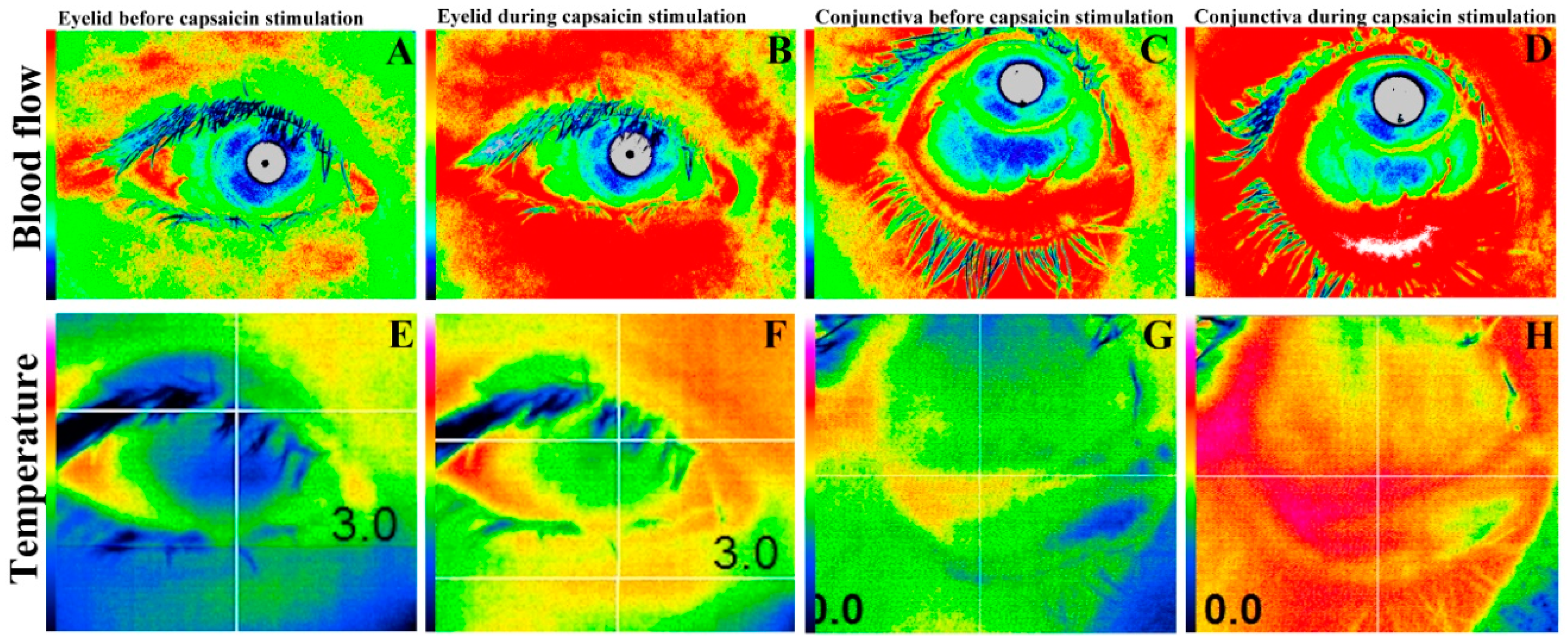
3.2. Experiment 2
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| LSFG | Laser speckle flowgraphy |
| FSLB | Functional slit-lamp biomicroscopy |
| MBR | Mean blur rate |
| NIBUT | Noninvasive tear breakup time |
| DEQS | Dry Eye-Related Quality of Life |
| MABP | Mean arterial blood pressure |
| LSFG-OAS | Laser speckle flowgraphy-ocular anterior segment |
| LSFG-PFI | LSFG-Perfusion Function Imager |
| CGRP | Calcitonin gene-related peptide |
References
- McAllen, R.M.; McKinley, M.J. Efferent thermoregulatory pathways regulating cutaneous blood flow and sweating. Handb. Clin. Neurol. 2018, 156, 305–316. [Google Scholar]
- Nakamoto, T.; Kanao, M.; Kondo, Y.; Kajiwara, N.; Masaki, C.; Takashi, T.; Hosokawa, R. Two-dimensional real-time blood flow and temperature of soft tissue around maxillary anterior implants. Implant Dent. 2012, 21, 522–527. [Google Scholar] [CrossRef]
- Toba, K.; Ouchi, Y.; Akishita, M.; Kozaki, K.; Ishikawa, M.; Nagano, K.; Etoh, M.; Hashimoto, M.; Liang, J.; Ueda, N.; et al. Improved skin blood flow and cutaneous temperature in the foot of a patient with arteriosclerosis obliterans by vasopressin V1 antagonist (OPC21268). A case report. Angiology 1995, 46, 1027–1033. [Google Scholar] [CrossRef]
- Takazawa, K.; Iketani, T.; Ibukiyama, C. Pulse wave velocity, thermography in the diagnosis of arteriosclerosis. Nihon Rinsho 1993, 51, 2074–2079. (In Japanese) [Google Scholar]
- Mongkolpun, W.; Orbegozo, D.; Cordeiro, C.P.R.; Franco, C.J.C.S.; Vincent, J.L.; Creteur, J. Alterations in skin blood flow at the fingertip are related to mortality in patients with circulatory shock. Crit. Care Med. 2020, 48, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Kamao, T.; Yamaguchi, M.; Kawasaki, S.; Mizoue, S.; Shiraishi, A.; Ohashi, Y. Screening for dry eye with newly developed ocular surface thermographer. Am. J. Ophthalmol. 2012, 151, 782–791. [Google Scholar] [CrossRef] [PubMed]
- Giannaccare, G.; Fresina, M.; Agnifili, L.; Versura, P. Ocular-surface temperature modification by cataract surgery. J. Cataract Refract. Surg. 2016, 42, 983–989. [Google Scholar] [CrossRef] [PubMed]
- Itokawa, T.; Okajima, Y.; Suzuki, T.; Kakisu, K.; Iwashita, H.; Murakami, Y.; Hori, Y. Association between ocular surface temperature and tear film stability in soft contact lens wearers. Investig. Ophthalmol. Vis. Sci. 2018, 59, 771–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Itokawa, T.; Okajima, Y.; Suzuki, T.; Kobayashi, T.; Tei, Y.; Kakisu, K.; Hori, Y. Association among blink rate, changes in ocular surface temperature, tear film stability, and functional visual acuity in patients after cataract surgery. J. Ophthalmol. 2019, 8189097. [Google Scholar] [CrossRef] [Green Version]
- Morgan, P.B.; Soh, M.P.; Efron, N. Corneal surface temperature decreases with age. Contact Lens Anter. Eye 1999, 22, 11–13. [Google Scholar] [CrossRef]
- Purslow, C.; Wolffsohn, J. The relation between physical properties of the anterior eye and ocular surface temperature. Optom. Vis. Sci. 2007, 84, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Hamano, H.; Minami, S.; Sugimori, Y. Experiments in thermometry of the anterior portion of the eye wearing a contact lens by means of infra-red thermometer. Contact 1969, 13, 12–22. [Google Scholar]
- Abusharha, A.A.; Pearce, E.I.; Fagehi, R. Effect of ambient temperature on the human tear film. Eye Contact Lens 2016, 42, 308–312. [Google Scholar] [CrossRef] [PubMed]
- Arita, R.; Shirakawa, R.; Maeda, S.; Yamaguchi, M.; Ohashi, Y.; Amano, S. Decreased surface temperature of tarsal conjunctiva in patients with meibomian gland dysfunction. JAMA Ophthalmol. 2013, 131, 818–819. [Google Scholar] [CrossRef]
- Abreau, K.; Callan, C.; Kottaiyan, R.; Zhang, A.; Toon, G.; Aquavella, J.V.; Zavislan, J.; Hindman, H.B. Temperature of the ocular surface, lid, and periorbital regions of Sjogren’s, evaporative, and aqueous-deficient dry eyes relative to normals. Ocul. Surf. 2016, 14, 64–73. [Google Scholar] [CrossRef]
- Hara, Y.; Shiraishi, A.; Yamaguchi, M.; Kawasaki, S.; Uno, T.; Ohashi, Y. Evaluation of allergic conjunctivitis by thermography. Ophthalmic Res. 2014, 51, 161–166. [Google Scholar] [CrossRef]
- Parra, A.; Madrid, R.; Echevarria, D.; Olmo, S.D.; Morenilla-Palao, C.; Acosta, M.C.; Gallar, J.; Dhaka, A.; Viana, F.; Belmonte, C. Ocular surface wetness is regulated by TRPM8-dependent cold thermoreceptors of the cornea. Nat. Med. 2010, 16, 1396–1399. [Google Scholar] [CrossRef]
- Cheung, A.T.; Hu, B.S.; Wong, S.A.; Chow, J.; Chan, M.S.; To, W.J.; Li, J.; Ramanujam, S.; Chen, P.C.Y. Microvascular abnormalities in the bulbar conjunctiva of contact lens users. Clin. Hemorheol. Microcirc. 2012, 51, 77–86. [Google Scholar] [CrossRef]
- Duench, S.; Simpson, T.; Jones, L.W.; Flanagan, J.G.; Fonn, D. Assessment of variation in bulbar conjunctival redness, temperature, and blood flow. Optom. Vis. Sci. 2007, 84, 511–516. [Google Scholar] [CrossRef]
- Chen, W.; Deng, Y.; Jiang, H.; Wang, J.; Zhong, J.; Li, S.; Peng, L.; Wang, B.; Yang, R.; Zhang, H.; et al. Microvascular abnormalities in dry eye patients. Microvasc. Res. 2018, 118, 155–161. [Google Scholar] [CrossRef]
- Chen, W.; Batawi, H.I.M.; Alava, J.R.; Galor, A.; Yuan, J.; Sarantopoulos, C.D.; McClellan, A.L.; Feuer, W.J.; Levitt, R.C.; Wang, J. Batawi HI. Bulbar conjunctival microvascular responses in dry eye. Ocul. Surf. 2017, 15, 193–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sugiyama, T. Basic technology and clinical applications of the updated model of laser speckle flowgraphy to ocular diseases. Photonics 2014, 1, 220–234. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, H.; Sugiyama, T.; Tokushige, H.; Maeno, T.; Nakazawa, T.; Ikeda, T.; Araie, M. Comparison of CCD-equipped laser speckle flowgraphy with hydrogen gas clearance method in the measurement of optic nerve head microcirculation in rabbits. Exp. Eye Res. 2013, 108, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Aizawa, N.; Nitta, F.; Kunikata, H.; Sugiyama, T.; Ikeda, T.; Araie, M.; Nakazawa, T. Laser speckle and hydrogen gas clearance measurements of optic nerve circulation in albino and pigmented rabbits with or without optic disc atrophy. Investig. Ophthalmol. Vis. Sci. 2014, 55, 7991–7996. [Google Scholar] [CrossRef] [Green Version]
- Nagashima, Y.; Ohsugi, Y.; Niki, Y.; Maeda, K.; Okamoto, T. Assessment of lase speckle flowgraphy: Development of novel cutaneous blood flow measurement technique. Proc. SPIE 2015, 9792, 979218. [Google Scholar]
- Kiyota, N.; Shiga, Y.; Suzuki, S.; Sato, M.; Takada, N.; Maekawa, S.; Omodaka, K.; Maruyama, K.; Kunikata, H.; Nakazawa, T. The effect of systemic hyperoxia on optic nerve head blood flow in primary open-angle glaucoma patients. Investig. Ophthalmol. Vis. Sci. 2017, 58, 3181–3188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukami, M.; Iwase, T.; Yamamoto, K.; Kaneko, H.; Yasuda, S.; Terasaki, H. Changes in retinal microcirculation after intravitreal ranibizumab injection in eyes with macular edema secondary to branch retinal vein occlusion. Investig. Ophthalmol. Vis. Sci. 2017, 58, 1246–1255. [Google Scholar] [CrossRef] [Green Version]
- Yamada, Y.; Suzuma, K.; Onizuka, M.; Uematsu, M.; Mohamed, Y.H.; Kitaoka, T. Evaluation of retinal blood flow before and after panretinal photocoagulation using pattern scan laser for diabetic retinopathy. Curr. Eye Res. 2017, 42, 1707–1712. [Google Scholar] [CrossRef]
- Matsumoto, T.; Itokawa, T.; Shiba, T.; Tomita, M.; Hine, K.; Mizukaki, N.; Yoda, H.; Hori, Y. Decreased ocular blood flow after photocoagulation therapy in neonatal retinopathy of prematurity. Jpn. J. Ophthalmol. 2017, 61, 484–493. [Google Scholar] [CrossRef]
- Shiba, T.; Sato, Y.; Takahashi, M. Relationship between diabetic retinopathy and slip-disordered breathing. Am. J. Ophthalmol. 2009, 147, 1017–1021. [Google Scholar] [CrossRef]
- Kikuchi, S.; Miyake, K.; Tada, Y.; Uchida, D.; Koya, A.; Saito, Y.; Ohura, T.; Azuma, N. Laser speckle flowgraphy can also be used to show dynamic changes in the blood flow of the skin of the foot after surgical revascularization. Vascular 2019, 27, 242–251. [Google Scholar] [CrossRef] [Green Version]
- Kashima, H.; Hayashi, N. Facial skin blood flow responses to irritant stimuli in the oral cavity. Auton. Neurosci. 2013, 174, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Ohsugi, Y.; Nagashima, Y.; Nakatsu, S.; Sato, K.; Chiba, A.; Fujinaka, H.; Yano, Y.; Niki, Y. Age-related changes in gingival blood flow parameters measured using laser speckle flowmetry. Microvasc. Res. 2019, 122, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Magerl, W.; Treede, R.D. Heat-evoked vasodilatation in human hairy skin: Axon reflexes due to low-level activity of nociceptive afferents. J. Physiol. 1996, 497, 837–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pozzi, A.T.D.; Miller, J.T.; Hodges, G.J. The effect of heating rate on the cutaneous vasomotion responses of forearm and leg skin in humans. Microvasc. Res. 2016, 105, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Sakane, Y.; Yamaguchi, M.; Yokoi, N.; Uchino, M.; Dogru, M.; Oishi, T.; Ohashi, Y.; Ohashi, Y. Development and validation of the dry eye-related quality-of-life score questionnaire. JAMA Ophthalmol. 2013, 131, 1331–1338. [Google Scholar] [CrossRef] [PubMed]
- Arita, R.; Morishige, N.; Shirakawa, R.; Sato, Y.; Amano, S. Effects of eyelid warming devices on tear film parameters in normal subjects and patients with meibomian gland dysfunction. Ocul. Surf. 2015, 13, 321–330. [Google Scholar] [CrossRef] [Green Version]
- Yokoi, N.; Georgiev, G.A.; Kato, H.; Komuro, A.; Sonomura, Y.; Sotozono, C.; Tsubota, K.; Kinoshita, S. Classification of fluorescein breakup patterns: A novel method of differential diagnosis for dry eye. Am. J. Ophthalmol. 2017, 180, 72–85. [Google Scholar] [CrossRef]
- Purslow, C. Evaluation of the ocular tolerance of a novel eyelid-warming device used for meibomian gland dysfunction. Contact Lens Anter. Eye 2013, 36, 226–231. [Google Scholar] [CrossRef]
- Bilkhu, P.S.; Naroo, S.A.; Wolffsohn, J.S. Effect of a commercially available warm compress on eyelid temperature and tear film in healthy eyes. Optom. Vis. Sci. 2014, 91, 163–170. [Google Scholar] [CrossRef] [Green Version]
- Barcroft, H.; Edholm, O.G. The effect of temperature on blood flow and deep temperature in the human forearm. J. Physiol. 1943, 102, 5–20. [Google Scholar] [CrossRef] [PubMed]
- Minson, C.T.; Berry, L.T.; Joyner, M.J. Nitric oxide and neutrally mediated regulation of skin blood flow during local heating. J. Appl. Physiol. 1985, 91, 1619–1626. [Google Scholar] [CrossRef] [PubMed]
- Hodges, G.J.; Jonson, J.M. Adrenergic control of the human cutaneous circulation. Appl. Physiol. Nutr. Metab. 2009, 34, 829–839. [Google Scholar] [CrossRef]
- Miyaji, A.; Hayashi, S.; Hayashi, N. Regional differences in facial skin blood flow responses to thermal stimulation. Eur. J. Appl. Physiol. 2019, 119, 1195–1201. [Google Scholar] [CrossRef] [PubMed]
- Gazerani, P.; Arendt-Nielsen, L. Cutaneous vasomotor reactions in response to controlled heat applied on various body regions of healthy humans: Evaluation of time course and application parameters. Int. J. Physiol. Pathophysiol. Pharmacol. 2011, 3, 202–209. [Google Scholar]
- Wang, M.T.; Gokul, A.; Craig, J.P. Temperature profiles of patient-applied eyelid warming therapies. Contact Lens Anter. Eye 2015, 38, 430–434. [Google Scholar] [CrossRef] [PubMed]
- Sasano, T.; Kuriwada, S.; Shoji, N.; Sanjo, D.; Izumi, H.; Karita, K. Axon reflex vasodilatation in cat dental pulp elicited by noxious stimulation of the gingiva. J. Dent. Res. 1994, 73, 1797–1802. [Google Scholar] [CrossRef]
- Drummond, P.D. Mechanisms of physiological gustatory sweating and flushing in the face. J. Auton. Nerv. Syst. 1995, 52, 117–124. [Google Scholar] [CrossRef]
- Izumi, H. Reflex parasympathetic vasodilatation in the facial skin. Gen. Pharmacol. 1995, 26, 237–244. [Google Scholar] [CrossRef]
- Price, T.J.; Patwardhan, A.M.; Flores, C.M.; Hargreaves, K.M. A role for the anandamide membrane transporter in TRPV1-mediated neurosecretion from trigeminal sensory neurons. Neuropharmacology 2005, 49, 25–39. [Google Scholar] [CrossRef] [Green Version]
- Lenners, J.K.; Ruhle, V.; Ceppa, E.P.; Neuhuber, W.L.; Bunnett, N.W.; Grady, E.F.; Messlinger, K. Calcitonin receptor-like receptor (CLR), receptor activity-modifying protein 1 (RAMP1), and calcitonin gene-related peptide (CGRP) immunoreactivity in the rat trigeminovascular system: Differences between peripheral and central CGRP receptor distribution. J. Comp. Neurol. 2008, 507, 1277–1299. [Google Scholar] [CrossRef]
- Nosch, D.S.; Pult, H.; Albon, J.; Purslow, C.; Murphy, P.J. Does air gas aesthesiometry generate a true mechanical stimulus for corneal sensitivity measurement? Clin. Exp. Optom. 2018, 101, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Fricova, J.; Janatova, M.; Anders, M.; Albrecht, J.; Rokyta, R. Thermovision: A new diagnostic method for orofacial pain? J. Pain Res. 2018, 11, 3195–3203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akagi, T.; Uji, A.; Huang, A.S.; Weinreb, R.N.; Yamada, T.; Miyata, M.; Kameda, T.; Ikeda, H.O.; Tsujikawa, A. Conjunctival and intrascleral vasculatures assessed using anterior segment optical coherence tomography angiography in normal eyes. Am. J. Ophthalmol. 2018, 196, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Explanatory Variables | r Value | p Value |
|---|---|---|
| Upper eyelid skin temperature | 0.619 | <0.001 |
| Lower eyelid skin temperature | 0.573 | <0.001 |
| Palpebral conjunctiva temperature | 0.781 | <0.001 |
| Bulbar conjunctiva temperature | 0.867 | <0.001 |
| Upper eyelid skin blood flow | 0.239 | <0.05 |
| Lower eyelid skin blood flow | 0.081 | 0.470 |
| Palpebral conjunctiva blood flow | 0.228 | <0.05 |
| Bulbar conjunctiva blood flow | 0.031 | 0.782 |
| Variable | |||
|---|---|---|---|
| Dependent | Independent | β | p Value |
| Corneal temperature | Upper eyelid skin temperature | 0.291 | <0.01 |
| Lower eyelid skin temperature | −0.369 | <0.01 | |
| Palpebral conjunctiva temperature | 0.244 | <0.05 | |
| Bulbar conjunctiva temperature | 0.762 | <0.001 | |
| Upper eyelid skin blood flow | 0.054 | 0.410 | |
| Palpebral conjunctiva blood flow | −0.159 | <0.05 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Itokawa, T.; Suzuki, T.; Okajima, Y.; Kobayashi, T.; Iwashita, H.; Gotoda, S.; Kakisu, K.; Tei, Y.; Hori, Y. Correlation between Blood Flow and Temperature of the Ocular Anterior Segment in Normal Subjects. Diagnostics 2020, 10, 695. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10090695
Itokawa T, Suzuki T, Okajima Y, Kobayashi T, Iwashita H, Gotoda S, Kakisu K, Tei Y, Hori Y. Correlation between Blood Flow and Temperature of the Ocular Anterior Segment in Normal Subjects. Diagnostics. 2020; 10(9):695. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10090695
Chicago/Turabian StyleItokawa, Takashi, Takashi Suzuki, Yukinobu Okajima, Tatsuhiko Kobayashi, Hiroko Iwashita, Satoshi Gotoda, Koji Kakisu, Yuto Tei, and Yuichi Hori. 2020. "Correlation between Blood Flow and Temperature of the Ocular Anterior Segment in Normal Subjects" Diagnostics 10, no. 9: 695. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10090695