Characteristics and Utility of Fluorescein Breakup Patterns among Dry Eyes in Clinic-Based Settings

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Clinical Assessment
2.2.1. Tear Function Tests and Ocular Surface Evaluation
2.2.2. Classifications of DED Subgroups
2.2.3. Subjective Eye Symptoms Questionnaire
2.3. Statistical Analyses
3. Results
3.1. Study Population
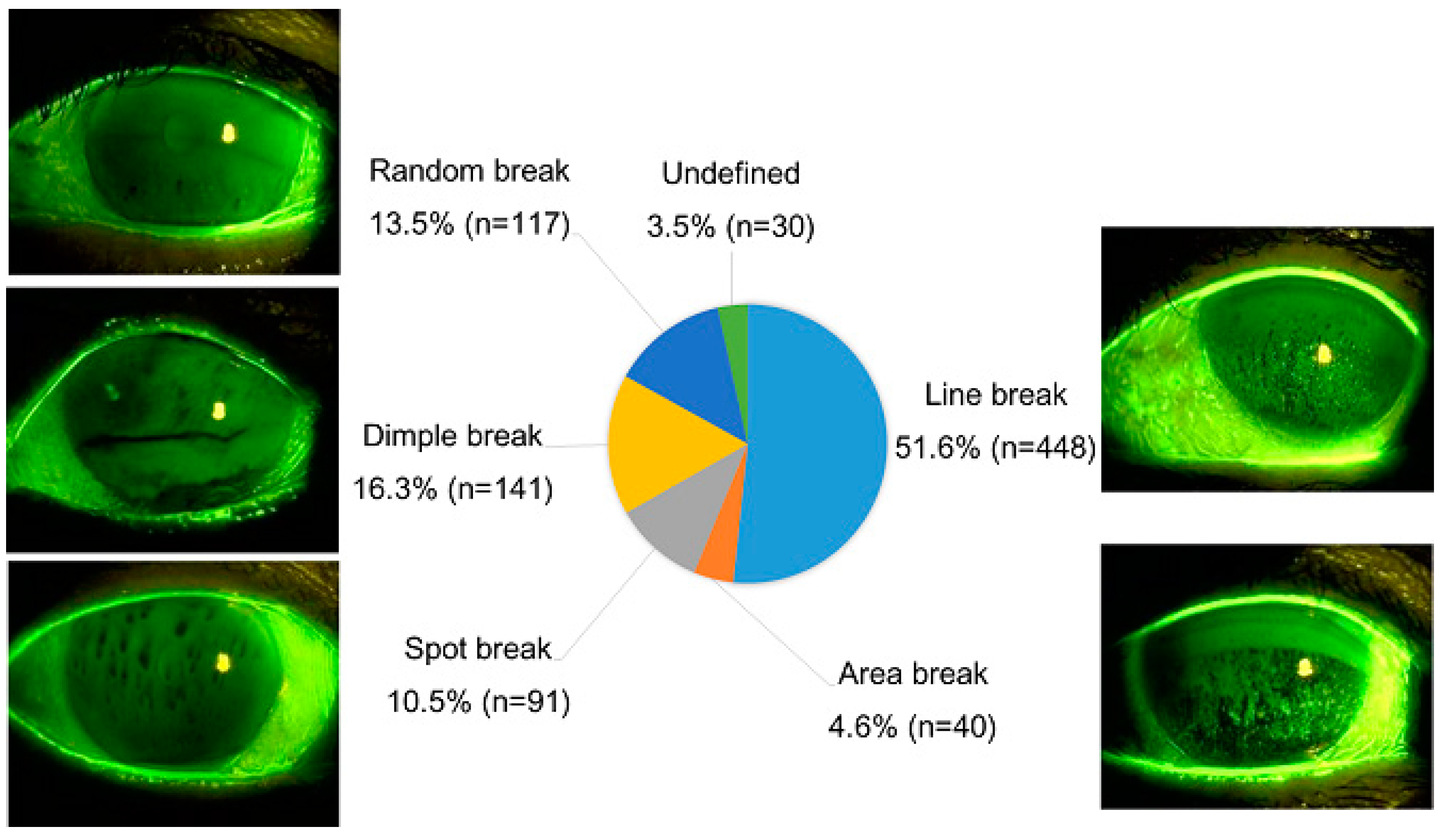
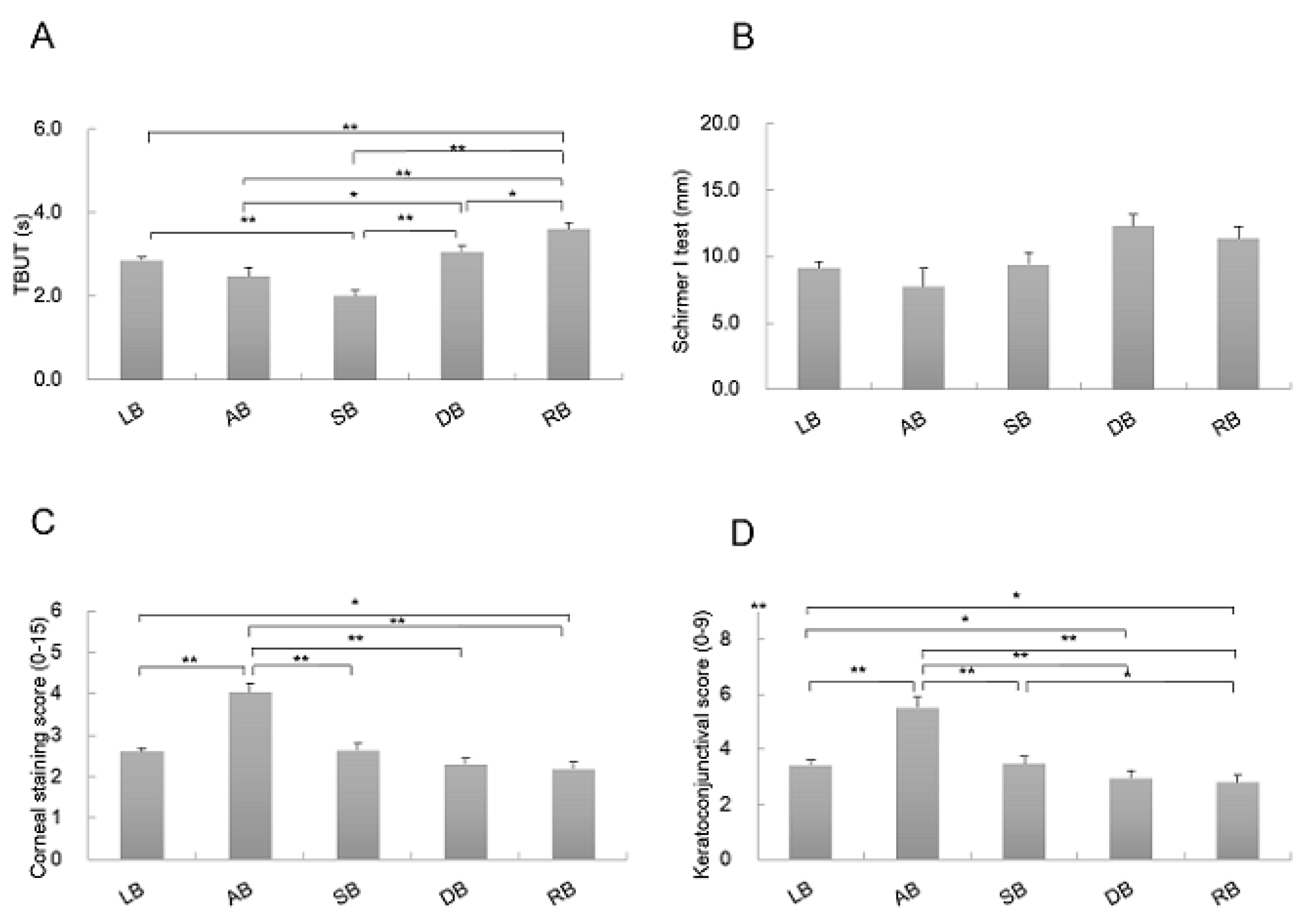
3.2. FBUPs in Relation to Tear Function Tests and Ocular Surface Evaluation
3.3. FBUPs in Relation to DED Subgroups
3.4. FBUPs of ADDE and Short FBUT-DE Subgroups
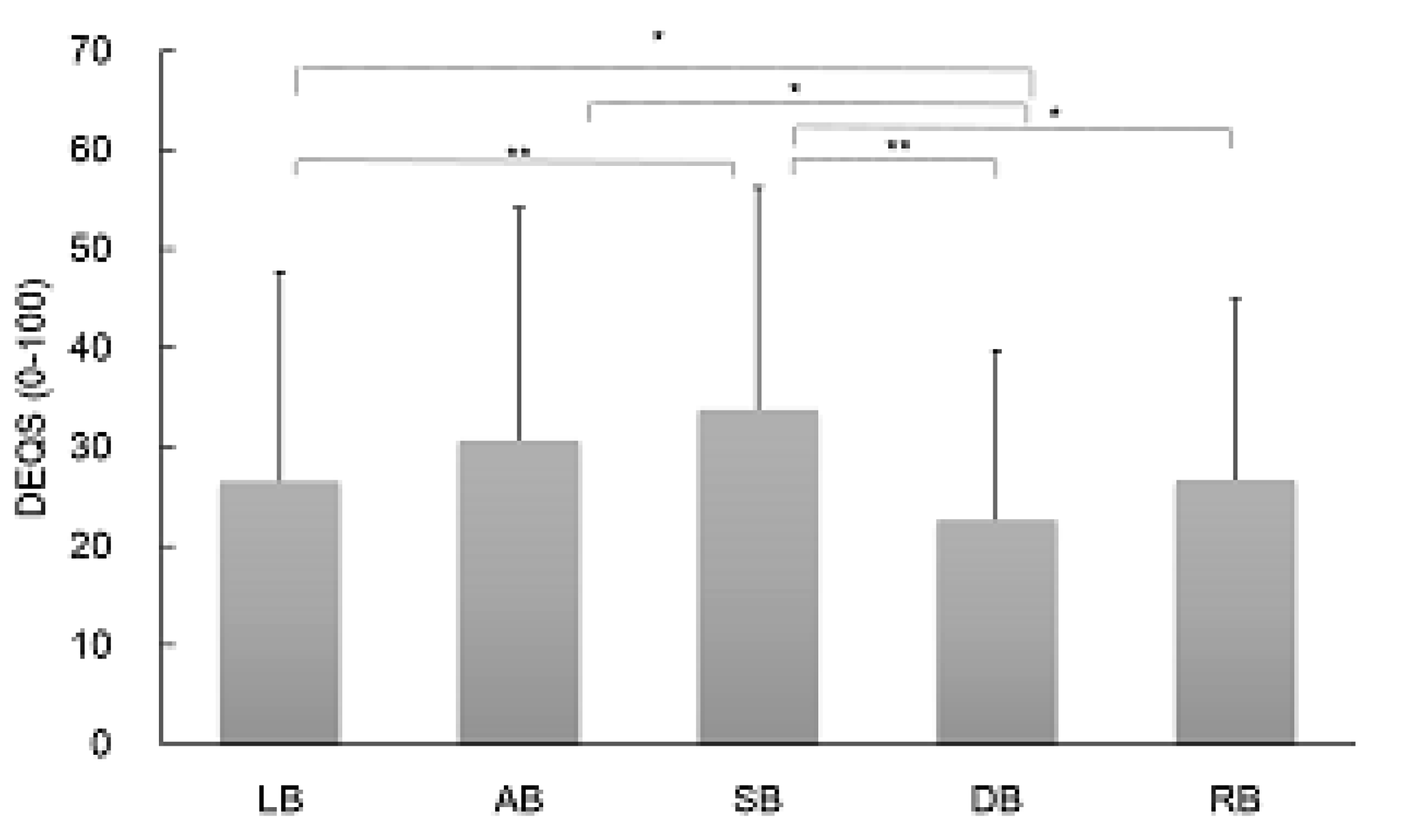
3.5. FBUPs in Relation to Subjective Eye Symptoms Questionnaire
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AB | area break |
| ADDE | aqueous-deficient dry eye |
| BUT | tear breakup time |
| CL | contact lens |
| DB | dimple break |
| DECS-J | Dry Eye Cross-Sectional Study in Japan |
| DED | dry eye disease |
| DEQS | Dry Eye-Related Quality of Life Score |
| DEWS | Dry Eye WorkShop |
| DVD | digital versatile disc |
| FBUPs | fluorescein breakup patterns |
| FBUT | fluorescein breakup time |
| IRB | institutional review board |
| LB | line break |
| MGD | meibomian gland dysfunction |
| NIBUT | non-invasive tear breakup time |
| RB | random break |
| Short FBUT-DE | short fluorescein breakup time dry eye |
| SB | spot break |
| SD | standard deviation |
| SE | standard error |
| SLK | superior limbic keratoconjunctivitis |
| TBUT | tear film breakup time |
| VDT | visual display terminal |
References
- Craig, J.P.; Nichols, K.K.; Akpek, E.K.; Caffery, B.; Dua, H.S.; Joo, C.K.; Liu, Z.; Nelson, J.D.; Nichols, J.J.; Tsubota, K.; et al. TFOS DEWS II Definition and Classification Report. Ocul. Surf. 2017, 15, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Lemp, M.A. Report of the National Eye Institute/Industry workshop on Clinical Trials in Dry Eyes. CLAO J. 1995, 21, 221–232. [Google Scholar] [PubMed]
- Workshop, I.D.E. Methodologies to diagnose and monitor dry eye disease: Report of the Diagnostic Methodology Subcommittee of the International Dry Eye WorkShop (2007). Ocul. Surf. 2007, 5, 108–152. [Google Scholar]
- Shimazaki, J.; Yokoi, N.; Watanabe, H.; Amano, S.; Ohashi, Y.; Kinoshita, S.; Shimomura, Y.; Takamura, E.; Hori, Y.; Nishida, K.; et al. Definition and Diagnosis of Dry Eye In Japan, 2016. Atarashii Ganka 2017, 34, 309–313. [Google Scholar]
- Tsubota, K.; Yokoi, N.; Shimazaki, J.; Watanabe, H.; Dogru, M.; Yamada, M.; Kinoshita, S.; Kim, H.M.; Tchah, H.W.; Hyon, J.Y.; et al. New Perspectives on Dry Eye Definition and Diagnosis: A Consensus Report by the Asia Dry Eye Society. Ocul. Surf. 2017, 15, 65–76. [Google Scholar] [CrossRef]
- Kawashima, M.; Yamada, M.; Suwaki, K.; Shigeyasu, C.; Uchino, M.; Hiratsuka, Y.; Yokoi, N.; Tsubota, K. A Clinic-based Survey of Clinical Characteristics and Practice Pattern of Dry Eye in Japan. Adv. Ther. 2017, 34, 732–743. [Google Scholar] [CrossRef]
- Uchino, M.; Yokoi, N.; Uchino, Y.; Dogru, M.; Kawashima, M.; Komuro, A.; Sonomura, Y.; Kato, H.; Kinoshita, S.; Schaumberg, D.A.; et al. Prevalence of dry eye disease and its risk factors in visual display terminal users: The Osaka study. Am. J. Ophthalmol. 2013, 156, 759–766. [Google Scholar] [CrossRef]
- Craig, J.P.; Tomlinson, A. Importance of the lipid layer in human tear film stability and evaporation. Optom. Vis. Sci. 1997, 74, 8–13. [Google Scholar] [CrossRef]
- Golding, T.R.; Bruce, A.S.; Mainstone, J.C. Relationship between tear-meniscus parameters and tear-film breakup. Cornea 1997, 16, 649–661. [Google Scholar] [CrossRef]
- Gipson, I.K. Distribution of mucins at the ocular surface. Exp. Eye Res. 2004, 78, 379–388. [Google Scholar] [CrossRef]
- Argueso, P. Glycobiology of the ocular surface: Mucins and lectins. Jpn. J. Ophthalmol. 2013, 57, 150–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsubota, K.; Yokoi, N.; Watanabe, H.; Dogru, M.; Kojima, T.; Yamada, M.; Kinoshita, S.; Kim, H.M.; Tchah, H.W.; Hyon, J.Y.; et al. A New Perspective on Dry Eye Classification: Proposal by the Asia Dry Eye Society. Eye Contact Lens 2019, 46, S2–S13. [Google Scholar] [CrossRef] [PubMed]
- Yokoi, N.; Georgiev, G.A.; Kato, H.; Komuro, A.; Sonomura, Y.; Sotozono, C.; Tsubota, K.; Kinoshita, S. Classification of Fluorescein Breakup Patterns: A Novel Method of Differential Diagnosis for Dry Eye. Am. J. Ophthalmol. 2017. [Google Scholar] [CrossRef]
- Yokoi, N.; Georgiev, G.A. Tear-film-oriented diagnosis for dry eye. Jpn. J. Ophthalmol. 2019, 63, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Yokoi, N.; Georgiev, G.A. Tear Film-Oriented Diagnosis and Tear Film-Oriented Therapy for Dry Eye Based on Tear Film Dynamics. Investig. Ophthalmol. Vis. Sci. 2018, 59, DES13–DES22. [Google Scholar] [CrossRef]
- Wolffsohn, J.S.; Arita, R.; Chalmers, R.; Djalilian, A.; Dogru, M.; Dumbleton, K.; Gupta, P.K.; Karpecki, P.; Lazreg, S.; Pult, H.; et al. TFOS DEWS II Diagnostic Methodology report. Ocul. Surf. 2017, 15, 539–574. [Google Scholar] [CrossRef] [PubMed]
- Paugh, J.R.; Tse, J.; Nguyen, T.; Sasai, A.; Chen, E.; De Jesus, M.T.; Kwan, J.; Nguyen, A.L.; Farid, M.; Garg, S.; et al. Efficacy of the Fluorescein Tear Breakup Time Test in Dry Eye. Cornea 2020, 39, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Vu, C.H.V.; Kawashima, M.; Yamada, M.; Suwaki, K.; Uchino, M.; Shigeyasu, C.; Hiratsuka, Y.; Yokoi, N.; Tsubota, K. Influence of Meibomian Gland Dysfunction and Friction-Related Disease on the Severity of Dry Eye. Ophthalmology 2018, 125, 1181–1188. [Google Scholar] [CrossRef]
- Shigeyasu, C.; Yamada, M.; Kawashima, M.; Suwaki, K.; Uchino, M.; Hiratsuka, Y.; Yokoi, N.; Tsubota, K. Quality of life measures and health utility values among dry eye subgroups. Health Qual. Life Outcomes 2018, 16, 170. [Google Scholar] [CrossRef] [Green Version]
- Van Bijsterveld, O.P. Diagnostic tests in the Sicca syndrome. Arch. Ophthalmol. 1969, 82, 10–14. [Google Scholar] [CrossRef]
- Amano, S.; Arita, R.; Kinoshita, S.; Yokoi, N.; Sotozono, C.; Komuro, A.; Suzuki, T.; Shimazaki, J.; Den, S.; Maeda, N.; et al. Definition and diagnostic criteria for meibomian gland dysfunction. Atarashii Ganka 2010, 27, 627–631. [Google Scholar]
- Sakane, Y.; Yamaguchi, M.; Yokoi, N.; Uchino, M.; Dogru, M.; Oishi, T.; Ohashi, Y.; Ohashi, Y. Development and validation of the Dry Eye-Related Quality-of-Life Score questionnaire. JAMA Ophthalmol. 2013, 131, 1331–1338. [Google Scholar] [CrossRef] [PubMed]
- Willcox, M.D.P.; Argueso, P.; Georgiev, G.A.; Holopainen, J.M.; Laurie, G.W.; Millar, T.J.; Papas, E.B.; Rolland, J.P.; Schmidt, T.A.; Stahl, U.; et al. TFOS DEWS II Tear Film Report. Ocul. Surf. 2017, 15, 366–403. [Google Scholar] [CrossRef] [Green Version]
- King-Smith, P.E.; Fink, B.A.; Hill, R.M.; Koelling, K.W.; Tiffany, J.M. The thickness of the tear film. Curr. Eye Res. 2004, 29, 357–368. [Google Scholar] [CrossRef] [PubMed]
- Yokoi, N.; Takehisa, Y.; Kinoshita, S. Correlation of tear lipid layer interference patterns with the diagnosis and severity of dry eye. Am. J. Ophthalmol. 1996, 122, 818–824. [Google Scholar] [CrossRef]
- Goto, E.; Ishida, R.; Kaido, M.; Dogru, M.; Matsumoto, Y.; Kojima, T.; Tsubota, K. Optical aberrations and visual disturbances associated with dry eye. Ocul. Surf. 2006, 4, 207–213. [Google Scholar] [CrossRef]
- Koh, S.; Maeda, N.; Kuroda, T.; Hori, Y.; Watanabe, H.; Fujikado, T.; Tano, Y.; Hirohara, Y.; Mihashi, T. Effect of tear film break-up on higher-order aberrations measured with wavefront sensor. Am. J. Ophthalmol. 2002, 134, 115–117. [Google Scholar] [CrossRef]
- Georgiev, G.A.; Eftimov, P.; Yokoi, N. Contribution of Mucins towards the Physical Properties of the Tear Film: A Modern Update. Int. J. Mol. Sci. 2019, 20, 6132. [Google Scholar] [CrossRef] [Green Version]
- Yokoi, N.; Uchino, M.; Uchino, Y.; Dogru, M.; Kawashima, M.; Komuro, A.; Sonomura, Y.; Kato, H.; Tsubota, K.; Kinoshita, S. Importance of tear film instability in dry eye disease in office workers using visual display terminals: The Osaka study. Am. J. Ophthalmol. 2015, 159, 748–754. [Google Scholar] [CrossRef]
- Shimazaki-Den, S.; Dogru, M.; Higa, K.; Shimazaki, J. Symptoms, visual function, and mucin expression of eyes with tear film instability. Cornea 2013, 32, 1211–1218. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patients Eyes (%) | Age (yrs) | p Value (vs. Line) | Woman Eyes (%) | p Value (vs. Line) | |
|---|---|---|---|---|---|
| All | 867 (100) | 62.5 ± 15.8 | 749 (86.4) | ||
| Line break | 448 (51.6) | 64.3 ± 14.6 | N/A | 384 (85.7) | N/A |
| Area break | 40 (4.6) | 65.3 ± 17.6 | 0.71 | 33 (82.5) | 0.58 |
| Spot break | 91 (10.5) | 57.4 ± 16.1 * | 0.0001 | 83 (91.2) | 0.16 |
| Dimple break | 141 (16.3) | 61.6 ± 17.5 | 0.07 | 126 (89.4) | 0.27 |
| Random break | 117 (13.5) | 59.0 ± 16.0 * | <0.01 | 103 (88.0) | 0.52 |
| Undefined | 30 (3.5) | 64.4 ± 15.6 | 0.99 | 20 (66.7) * | <0.01 |
| Sjögren Syndrome | Aqueous Deficiency | Short FBUT | MGD | CL | Friction | |
|---|---|---|---|---|---|---|
| Line break | 10.2 | 47.0 | 26.9 | 5.6 | 6.3 | 4.2 |
| Area break | 15.0 | 60.0 | 5.0 | 2.5 | 12.5 | 5.0 |
| Spot break | 8.6 | 30.9 | 38.3 | 6.2 | 7.4 | 8.6 |
| Dimple break | 1.5 | 17.8 | 51.9 | 13.3 | 8.9 | 6.7 |
| Random break | 6.0 | 25.3 | 18.1 | 16.9 | 18.1 | 15.7 |
| Undefined | 8.0 | 32.0 | 16.0 | 16.0 | 8.0 | 20.0 |
| Area Break | Line Break | Spot Break | Dimple Break | Random Break | Undefined | |
|---|---|---|---|---|---|---|
| ADDE | 8.1 | 66.6 | 8.6 | 7.0 | 7.0 | 2.7 |
| short FBUT-DE | 0.8 | 48.7 | 13.0 | 29.4 | 6.3 | 1.7 |
| FBUPs | ADDE | Short FBUT-DE |
| Area, Line | Spot, Dimple | |
| Sensitivity | 0.747 | 0.416 |
| Specificity | 0.541 | 0.794 |
| Pre-test probability | 0.466 | 0.299 |
| Post-test probability | 0.587 | 0.463 |
| Positive likelihood ratio | 1.627 | 2.018 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shigeyasu, C.; Yamada, M.; Yokoi, N.; Kawashima, M.; Suwaki, K.; Uchino, M.; Hiratsuka, Y.; Tsubota, K.; on behalf of the DECS-J Study Group. Characteristics and Utility of Fluorescein Breakup Patterns among Dry Eyes in Clinic-Based Settings. Diagnostics 2020, 10, 711. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10090711
Shigeyasu C, Yamada M, Yokoi N, Kawashima M, Suwaki K, Uchino M, Hiratsuka Y, Tsubota K, on behalf of the DECS-J Study Group. Characteristics and Utility of Fluorescein Breakup Patterns among Dry Eyes in Clinic-Based Settings. Diagnostics. 2020; 10(9):711. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10090711
Chicago/Turabian StyleShigeyasu, Chika, Masakazu Yamada, Norihiko Yokoi, Motoko Kawashima, Kazuhisa Suwaki, Miki Uchino, Yoshimune Hiratsuka, Kazuo Tsubota, and on behalf of the DECS-J Study Group. 2020. "Characteristics and Utility of Fluorescein Breakup Patterns among Dry Eyes in Clinic-Based Settings" Diagnostics 10, no. 9: 711. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10090711