Antigen-Specific Cytokine and Chemokine Gene Expression for Diagnosing Latent and Active Tuberculosis

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Statement
2.2. Study Participants and Case Definitions
2.3. Interferon Gamma Release Assay (IGRA)
2.4. RNA Extraction and Complementary DNA (cDNA) Synthesis
2.5. Primer, Probe Designing and Optimization
2.6. Real-Time Polymerase Chain Reaction Analysis
2.7. Normality of Sample Distribution
2.8. Data Analysis
3. Results
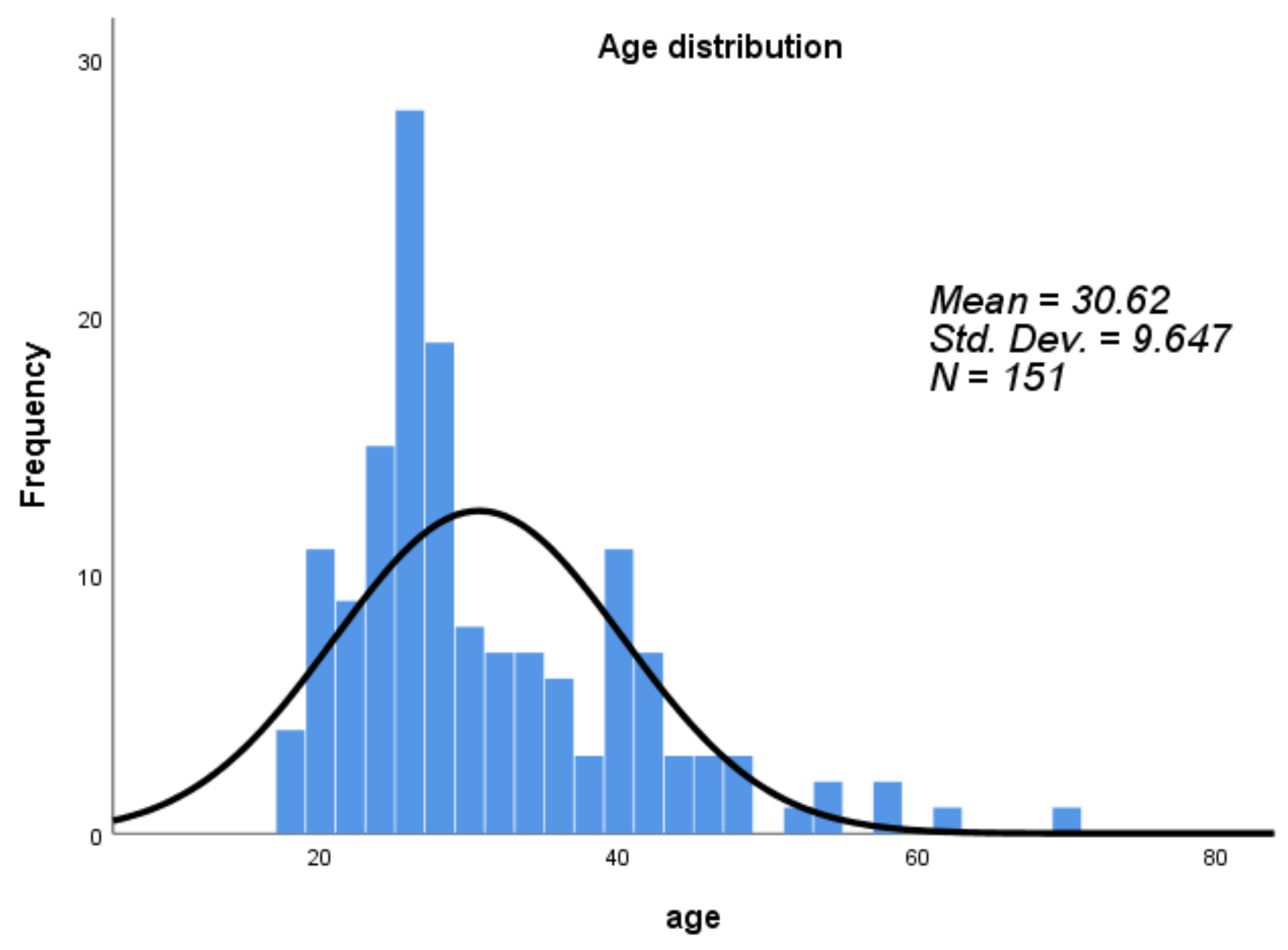
3.1. Participants Characteristics
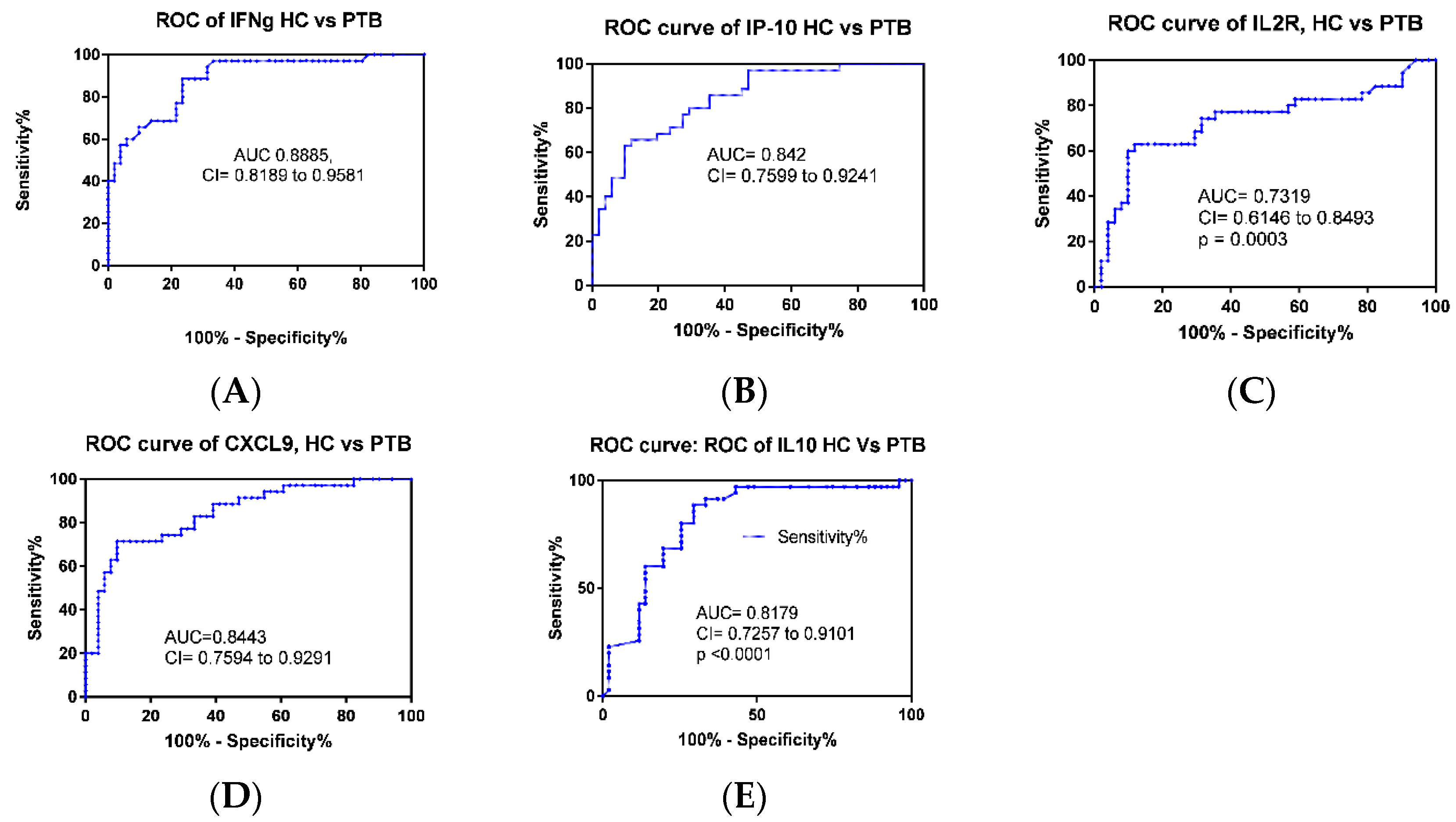
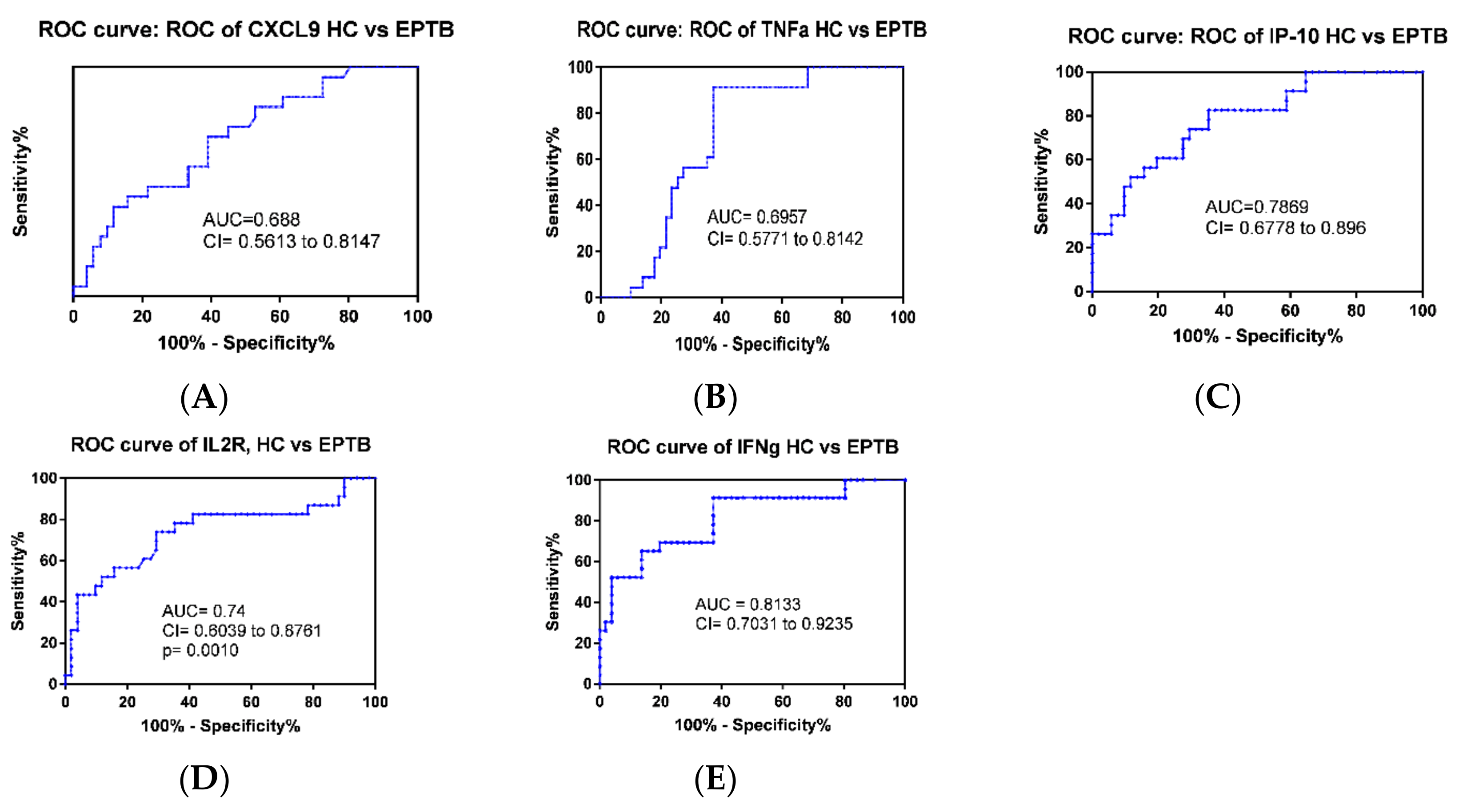
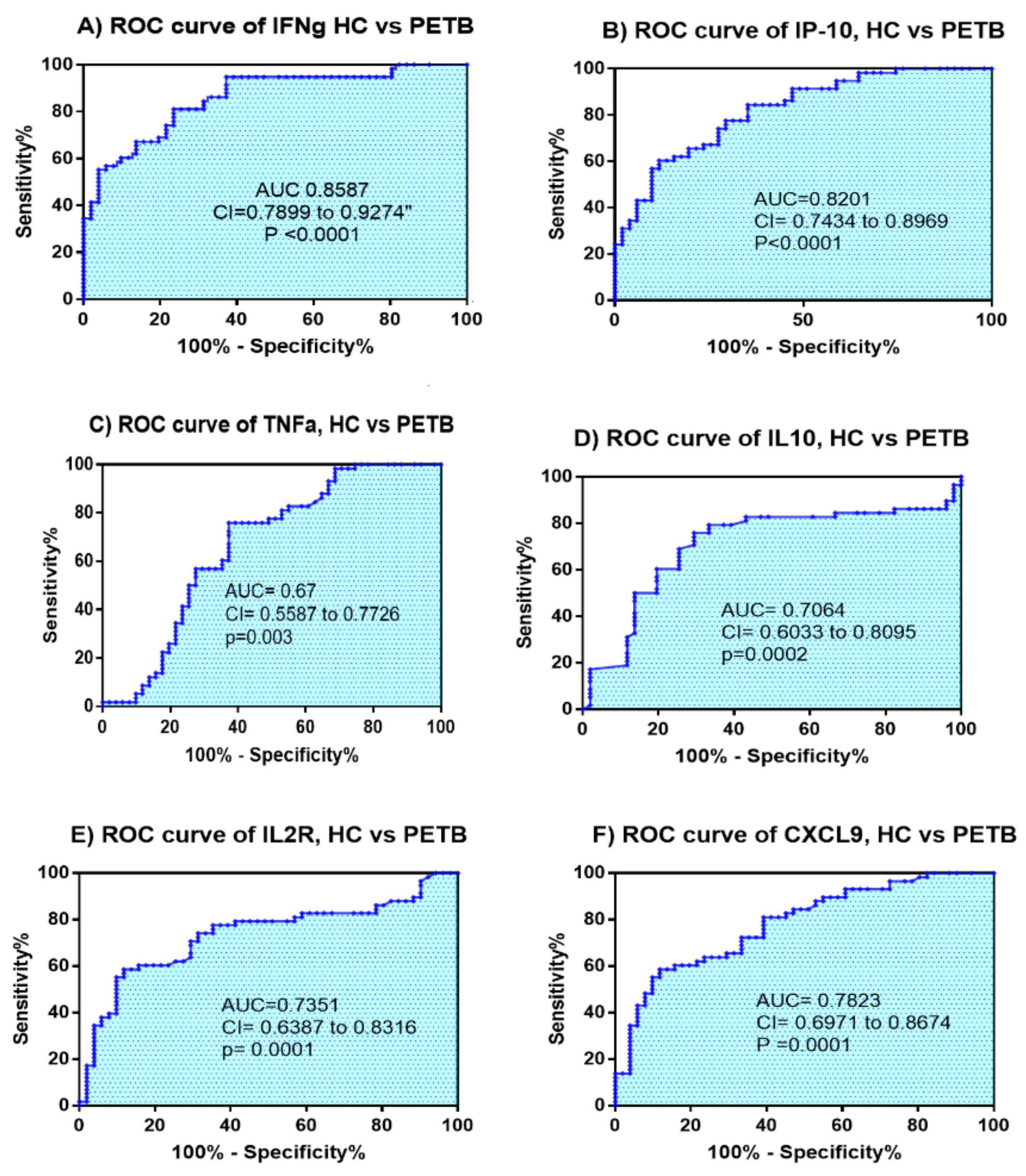
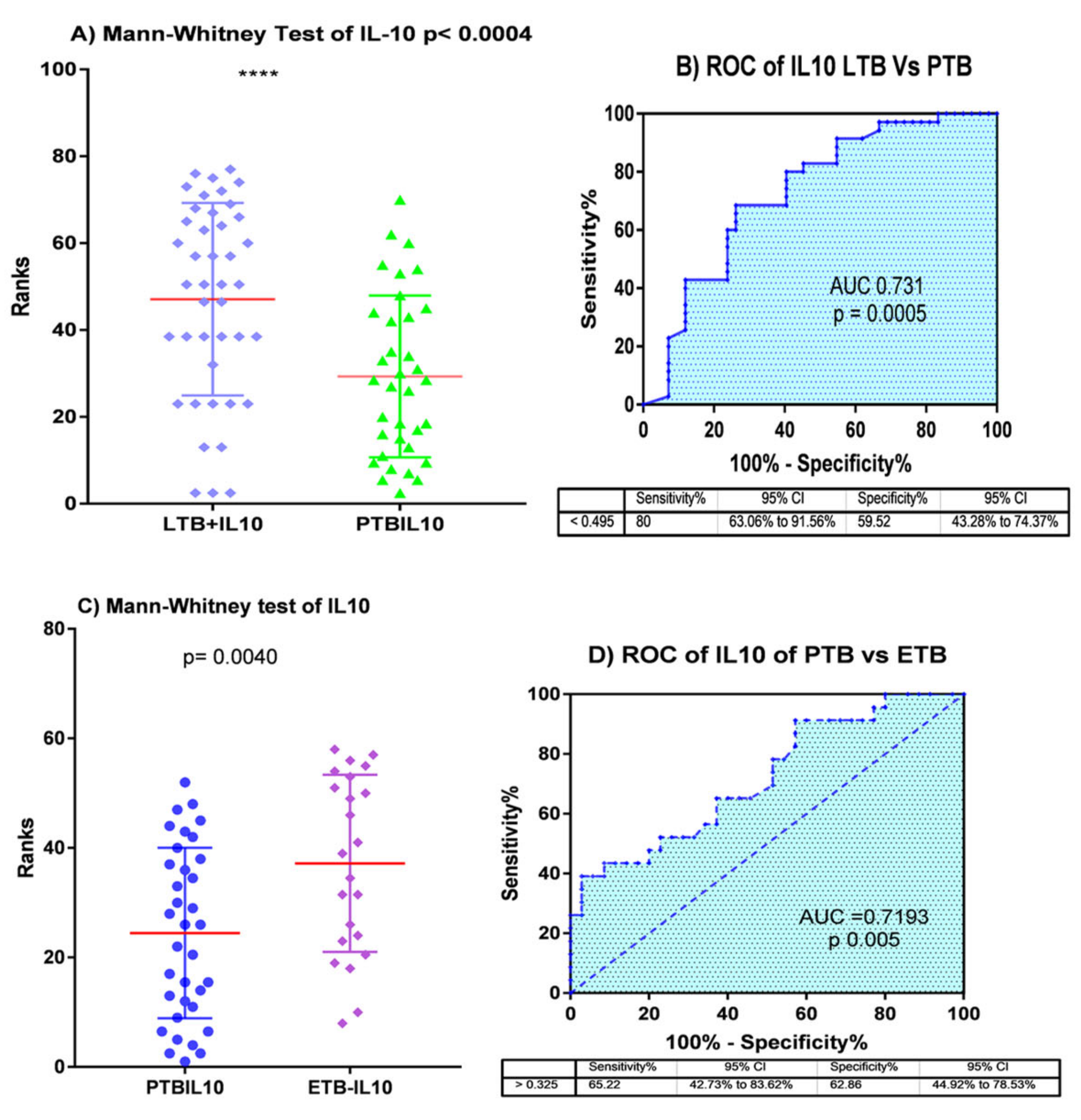
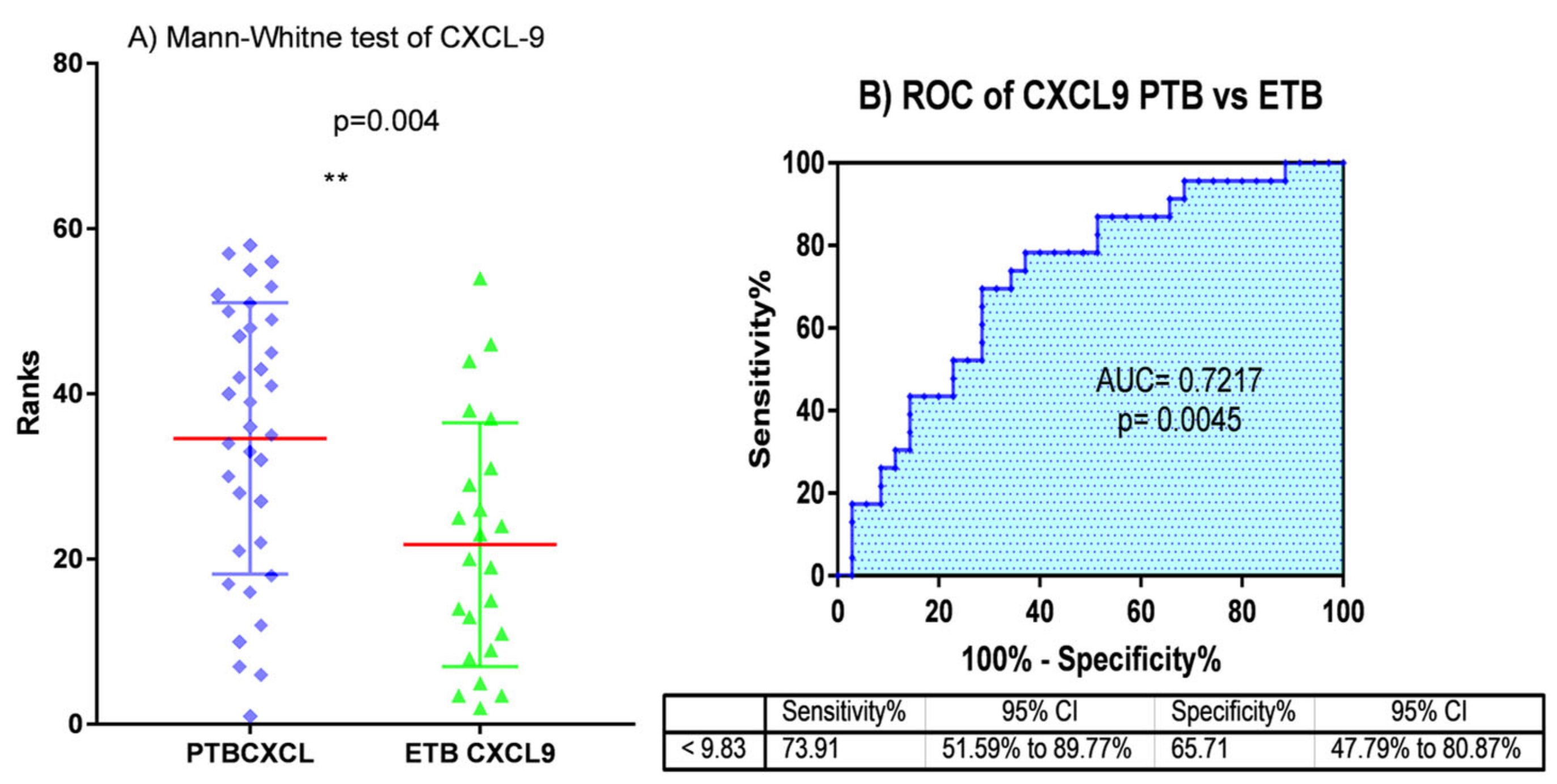
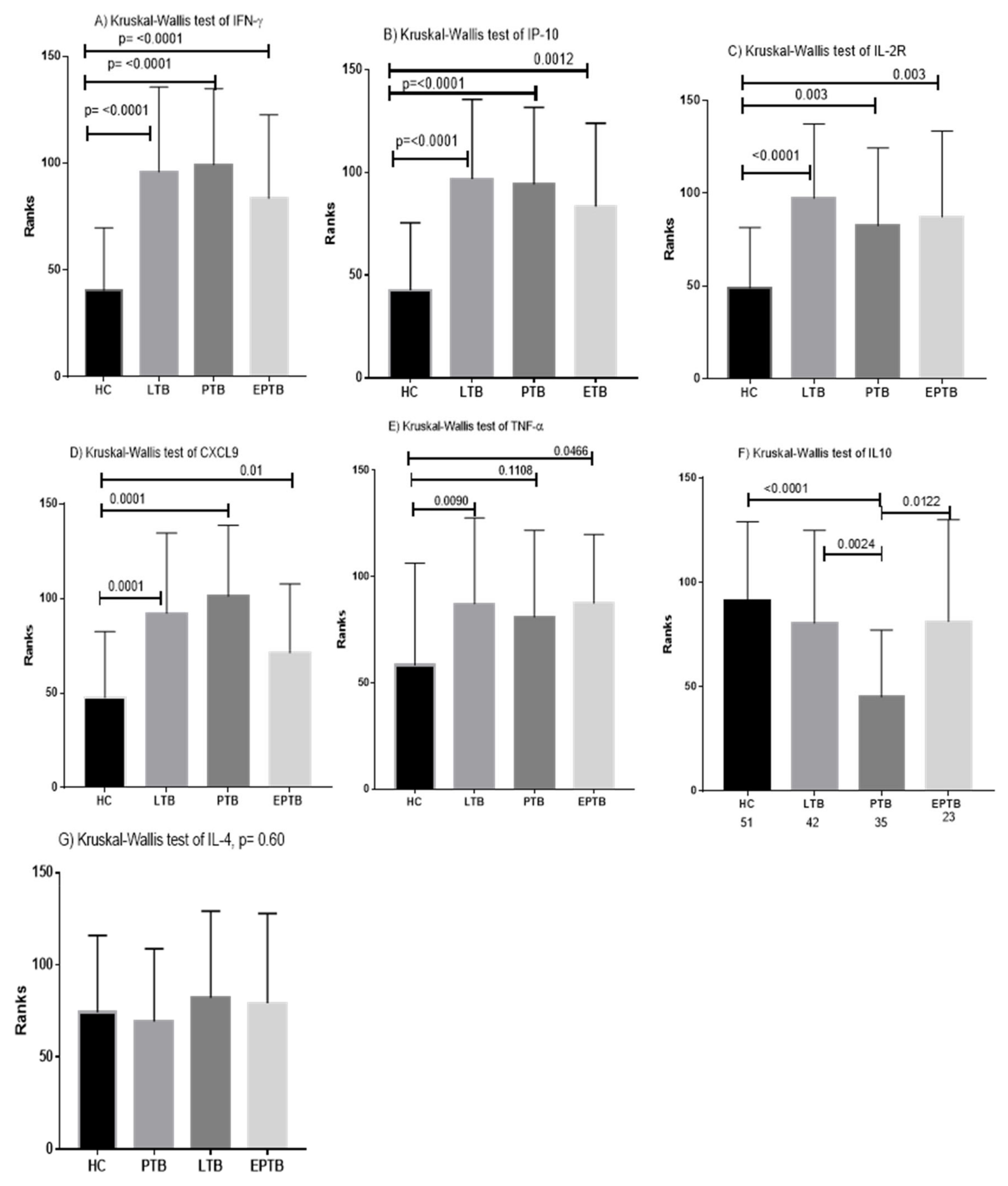
3.2. Determination of Cut off Values and Diagnostic Performance of Cytokines and Chemokines
3.3. Individual Biomarkers Identification and Validation
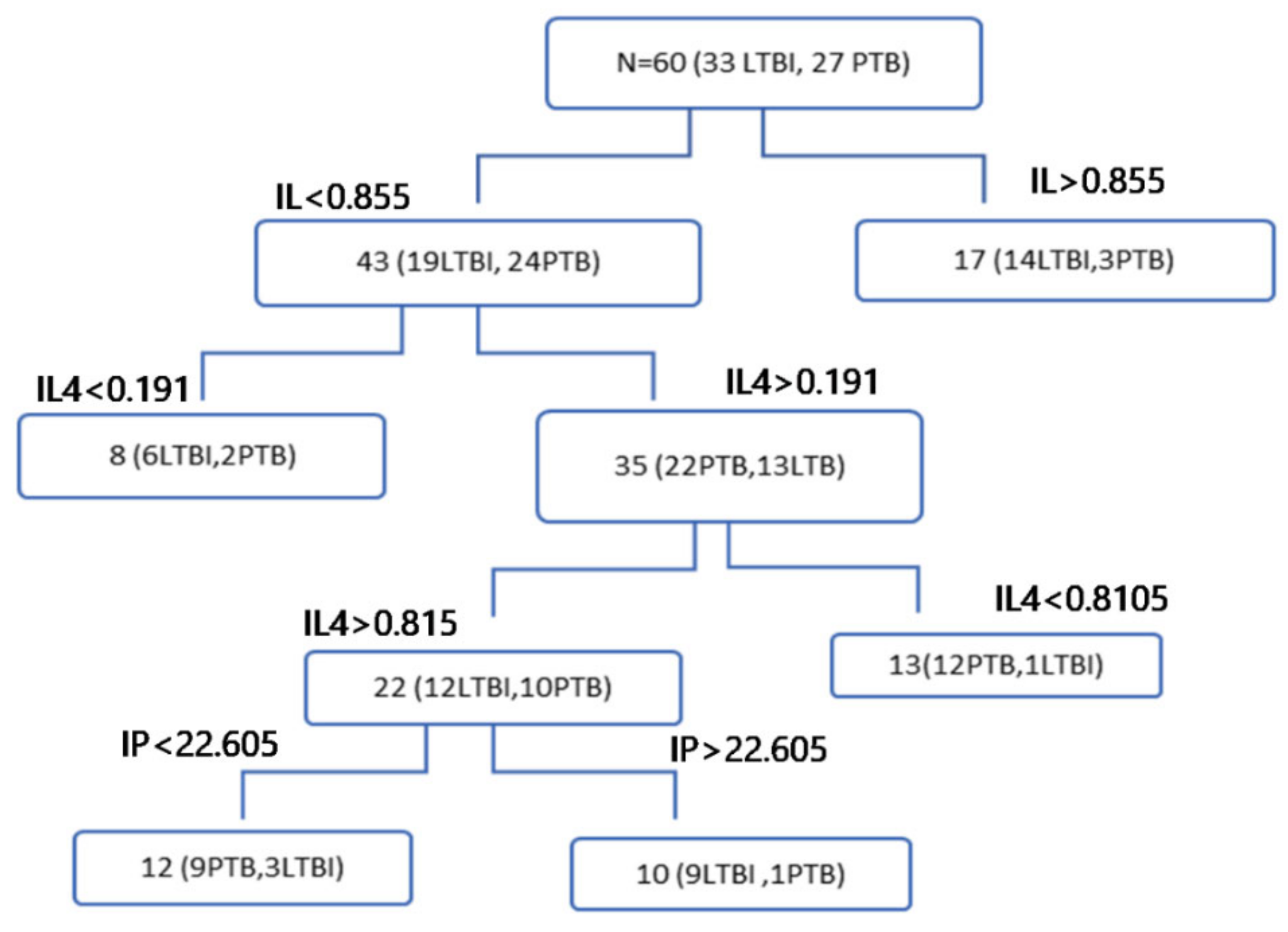
3.4. Combination of Cytokine Markers in Discriminating Tuberculosis Infection
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Annabel, B.; Anna, D.; Hannah, M. Global Tuberculosis Report 2019; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Harding, E. WHO global progress report on tuberculosis elimination. Lancet Respir. Med. 2020, 8, 19. [Google Scholar] [CrossRef]
- Lin, P.L.; Flynn, J.L. Understanding latent tuberculosis: A moving target. J. Immunol. 2010, 185, 15–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Garra, A.; Redford, P.S.; McNab, F.W.; Bloom, C.I.; Wilkinson, R.J.; Berry, M.P.R. The Immune Response in Tuberculosis. Annu. Rev. Immunol. 2013, 31, 475–527. [Google Scholar] [CrossRef] [PubMed]
- Steingart, K.R.; Ng, V.; Henry, M.; Hopewell, P.C.; Ramsay, A.; Cunningham, J.; Urbanczik, R.; Perkins, M.D.; Aziz, M.A.; Pai, M. Sputum processing methods to improve the sensitivity of smear microscopy for tuberculosis: A systematic review. Lancet Infect. Dis. 2006, 6, 664–674. [Google Scholar] [CrossRef]
- Lawn, S.D.; Mwaba, P.; Bates, M.; Piatek, A.; Alexander, H.; Marais, B.J.; Cuevas, L.E.; McHugh, T.D.; Zijenah, L.; Kapata, N.; et al. Advances in tuberculosis diagnostics: The Xpert MTB/RIF assay and future prospects for a point-of-care test. Lancet Infect. Dis. 2013, 13, 349–361. [Google Scholar] [CrossRef] [Green Version]
- Domingo-Gonzalez, R.; Prince, O.; Cooper, A.; Khader, S.A. Cytokines and Chemokines in Mycobacterium tuberculosis Infection. Microbiol. Spectr. 2016, 4. [Google Scholar] [CrossRef] [Green Version]
- Andersen, P.; Munk, M.E.; Pollock, J.M.; Doherty, T.M. Specific immune-based diagnosis of tuberculosis. Lancet 2000, 356, 1099–1104. [Google Scholar] [CrossRef]
- Harada, N. Characteristics of a diagnostic method for tuberculosis infection based on whole blood interferon-gamma assay. Kekkaku 2006, 81, 681–686. [Google Scholar]
- Herrera, V.; Perry, S.; Parsonnet, J.; Banaei, N. Clinical Application and Limitations of Interferon-γ Release Assays for the Diagnosis of Latent Tuberculosis Infection. Clin. Infect. Dis. 2011, 52, 1031–1037. [Google Scholar] [CrossRef] [Green Version]
- Ruhwald, M.; Bodmer, T.; Maier, C.; Jepsen, M.; Haaland, M.B.; Eugen-Olsen, J.; Ravn, P. Evaluating the potential of IP-10 and MCP-2 as biomarkers for the diagnosis of tuberculosis. Eur. Respir. J. 2008, 32, 1607–1615. [Google Scholar] [CrossRef] [Green Version]
- Jeong, Y.H.; Hur, Y.-G.; Lee, H.; Kim, S.; Cho, J.-E.; Chang, J.; Shin, S.J.; Lee, H.; Kang, Y.A.; Cho, S.-N.; et al. Discrimination between active and latent tuberculosis based on ratio of antigen-specific to mitogen-induced IP-10 production. J. Clin. Microbiol. 2015, 53, 504–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goyal, N.; Kashyap, B.; Kaur, I.R. Significance of IFN-ɤ/IL-2 Ratio as a Circulating Diagnostic Biomarker in Extrapulmonary Tuberculosis. Scand. J. Immunol. 2016, 83, 338–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, A.P.; Corrêa, R.D.S.; Ribeiro-Alves, M.; Soares da Silva, A.C.O.; Mafort, T.T.; Leung, J.; Pereira, G.M.B.; Rodrigues, L.S.; Rufino, R. Application of Venn’s diagram in the diagnosis of pleural tuberculosis using IFN-γ, IP-10 and adenosine deaminase. PLoS ONE 2018, 13, e0202481. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Li, Y.; Shen, Y.; Wu, J.; Gao, Y.; Zhang, S.; Shao, L.; Jin, J.; Zhang, Y.; Zhang, W. Screening and identification of a six-cytokine biosignature for detecting TB infection and discriminating active from latent TB. J. Transl. Med. 2018, 16, 206. [Google Scholar] [CrossRef] [Green Version]
- Bozzano, F.; Marras, F.; de Maria, A. Immunology of Tuberculosis. Mediterr. J. Hematol. Infect. Dis. 2014, 6, e2014027. [Google Scholar] [CrossRef]
- World Health Organization. Treatment of Tuberculosis: Guidelines; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Rodríguez, A.; Rodríguez, M.; Córdoba, J.J.; Andrade, M.J. Design of primers and probes for quantitative real-time PCR methods. Methods Mol. Biol. 2015, 1275, 31–56. [Google Scholar] [PubMed]
- Kim, S.; Lee, H.; Kim, H.; Kim, Y.; Cho, J.-E.; Jin, H.; Kim, D.Y.; Ha, S.-J.; Kang, Y.A.; Cho, S.-N.; et al. Diagnostic performance of a cytokine and IFN-γ-induced chemokine mRNA assay after Mycobacterium tuberculosis-specific antigen stimulation in whole blood from infected individuals. J. Mol. Diagn. 2015, 17, 90–99. [Google Scholar] [CrossRef]
- Barber, R.D.; Harmer, D.W.; Coleman, R.A.; Clark, B.J. GAPDH as a housekeeping gene: Analysis of GAPDH mRNA expression in a panel of 72 human tissues. Physiol. Genom. 2005, 21, 389–395. [Google Scholar] [CrossRef] [Green Version]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) Method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef]
- Suzukawa, M.; Akashi, S.; Nagai, H.; Nagase, H.; Nakamura, H.; Matsui, H.; Hebisawa, A.; Ohta, K. Combined Analysis of IFN-γ, IL-2, IL-5, IL-10, IL-1RA and MCP-1 in QFT Supernatant Is Useful for Distinguishing Active Tuberculosis from Latent Infection. PLoS ONE 2016, 11, e0152483. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Wang, S.; Lu, C.; Shao, L.; Gao, Y.; Zhou, Z.; Huang, H.; Zhang, Y.; Zhang, W. Multiple cytokine responses in discriminating between active tuberculosis and latent tuberculosis infection. Tuberculosis 2017, 102, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Ranaivomanana, P.; Raberahona, M.; Rabarioelina, S.; Borella, Y.; Machado, A.; Randria, M.J.D.D.; Rakotoarivelo, R.A.; Rasolofo, V.; Rakotosamimanana, N. Cytokine Biomarkers Associated with Human Extra-Pulmonary Tuberculosis Clinical Strains and Symptoms. Front. Microbiol. 2018, 9, 275. [Google Scholar] [CrossRef] [PubMed]
- Mihret, A.; Bekele, Y.; Bobosha, K.; Kidd, M.; Aseffa, A.; Howe, R.; Walzl, G. Plasma cytokines and chemokines differentiate between active disease and non-active tuberculosis infection. J. Infect. 2013, 66, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Jiang, J.; Cao, Z.; Yang, B.; Zhang, J.; Cheng, X. Diagnostic performance of multiplex cytokine and chemokine assay for tuberculosis. Tuberculosis 2012, 92, 513–520. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Healthy Control | Latent Tuberculosis | PTB | EPTB | ||
|---|---|---|---|---|---|
| Sex | Male | 27 | 29 | 26 | 13 |
| Female | 24 | 13 | 9 | 10 | |
| Total | 51 | 42 | 35 | 23 | |
| % | 33.8 | 27.8 | 23.2 | 15.2 | |
| QFT (+/−) | 0/51 | 42/0 | 34/1 | 23/0 |
| A Multiple Comparison ANOVA (Kruskal-Wallis Test) | ||||||
|---|---|---|---|---|---|---|
| Marker | HC vs. LTB | HC vs. PTB | HC vs. EPTB | HC vs. PTB, EPTB | LTB vs. PTB | PTB vs. EPTB |
| INF-γ | 0.0001 | 0.0001 | 0.0015 | 0.0001 | 0.999 | 0.999 |
| TNF-α | 0.0233 | 0.2582 | 0.1256 | 0.039 | 0.999 | 0.999 |
| IP-10 | 0.0001 | 0.0001 | 0.0035 | 0.0001 | 0.999 | 0.999 |
| IL-10 | 0.999 | 0.0001 | 0.999 | 0.0022 | 0.0065 | 0.0472 |
| IL-2R | 0.999 | 0.0081 | 0.006 | 0.0004 | 0.999 | 0.999 |
| IL-4 | 0.0001 | 0.999 | 0.999 | 0.999 | 0.999 | 0.999 |
| CXCL-9 | 0.0001 | 0.0001 | 0.5803 | 0.0001 | 0.999 | 0.1066 |
| B Mann-Whitney Test (Two-Sided) | ||||||
| Marker | HC vs. LTB | HC vs. PTB | HC vs. EPTB | HC vs. PTB, EPTB | LTB vs. PTB | PTB vs. EPTB |
| IFN-γ | 0.0001 | 0.0001 | 0.0001 | 0.0001 | 0.7875 | 0.1436 |
| TNF-α | 0.0012 | 0.0216 | 0.0068 | 0.0027 | 0.5033 | 0.8514 |
| IP-10 | 0.0001 | 0.0001 | 0.0001 | 0.0001 | 0.7104 | 0.2912 |
| IL-10 | 0.252 | <0.0001 | 0.6198 | 0.0002 | 0.0004 | 0.0045 |
| IL-2R | 0.0001 | 0.0002 | 0.0008 | <0.0001 | 0.1222 | 0.5781 |
| IL-4 | 0.4008 | 0.6043 | 0.6118 | 0.9265 | 0.1941 | 0.4414 |
| CXC-L-9 | 0.0001 | <0.0001 | 0.0094 | <0.0001 | 0.3839 | 0.004 |
| Decision Tree Analysis Result | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Category | Control | Patient | Total | Normality | Accuracy | Sensitivity | Specificity | Genes | |
| HC vs. LTB | Train | 40 | 33 | 73 | 54.8% | 86.3% | 75.8% | 95.0% | IFN-γ, IL2R |
| Validate | 11 | 9 | 20 | 55.0% | 100.0% | 100.0% | 100.0% | ||
| Test | 51 | 42 | 93 | 54.8% | 89.2% | 81.0% | 96.1% | ||
| Control | Patient | Total | Normality | Accuracy | Sensitivity | Specificity | |||
| HC vs. PTB | Train | 40 | 27 | 67 | 59.7% | 89.6% | 96.3% | 85.0% | IFN-γ, IL10, IL2R |
| Validate | 11 | 8 | 19 | 57.9% | 100.0% | 100.0% | 100.0% | ||
| Test | 51 | 35 | 86 | 59.3% | 91.9% | 97.1% | 88.2% | ||
| Control | Patient | Total | Normality | Accuracy | Sensitivity | Specificity | |||
| LTB vs. PTB | Training | 33 | 27 | 60 | 55.0% | 83.3% | 77.8% | 87.9% | IL10, IL4, IP10 |
| Validation | 9 | 8 | 17 | 52.9% | 82.4% | 75.0% | 88.9% | ||
| Test | 42 | 35 | 77 | 54.5% | 83.1% | 77.1% | 88.1% | ||
| Control | Patient | Total | Normality | Accuracy | Sensitivity | Specificity | |||
| EPTB vs. PTB | Training | 18 | 27 | 45 | 40.0% | 75.6% | 81.5% | 66.7% | IL10, CXCL-9 |
| Validation | 5 | 8 | 13 | 38.5% | 100.0% | 100.0% | 100.0% | ||
| Test | 23 | 35 | 58 | 39.7% | 81.0% | 85.7% | 73.9% | ||
| HC vs. PETB | Control | Patient | Total | Normality | Accuracy | Sensitivity | Specificity | ||
| Training | 40 | 46 | 86 | 46.5% | 90.7% | 87.0% | 95.0% | IFN-γ, IL-2R, IL4 | |
| Validation | 11 | 12 | 23 | 47.8% | 100.0% | 100.0% | 100.0% | ||
| Test | 51 | 58 | 109 | 46.8% | 92.7% | 89.7% | 96.1% | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korma, W.; Mihret, A.; Chang, Y.; Tarekegn, A.; Tegegn, M.; Tuha, A.; Hwang, D.; Asefa, M.; Hasen, M.O.; Kim, S.; et al. Antigen-Specific Cytokine and Chemokine Gene Expression for Diagnosing Latent and Active Tuberculosis. Diagnostics 2020, 10, 716. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10090716
Korma W, Mihret A, Chang Y, Tarekegn A, Tegegn M, Tuha A, Hwang D, Asefa M, Hasen MO, Kim S, et al. Antigen-Specific Cytokine and Chemokine Gene Expression for Diagnosing Latent and Active Tuberculosis. Diagnostics. 2020; 10(9):716. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10090716
Chicago/Turabian StyleKorma, Workneh, Adane Mihret, Yunhee Chang, Azeb Tarekegn, Metasebiya Tegegn, Adem Tuha, Dasom Hwang, Mesfin Asefa, Mahlet O. Hasen, Seoyoung Kim, and et al. 2020. "Antigen-Specific Cytokine and Chemokine Gene Expression for Diagnosing Latent and Active Tuberculosis" Diagnostics 10, no. 9: 716. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10090716