Diagnostic Accuracy of Fine-Needle Aspiration Cytology and Core-Needle Biopsy in the Assessment of the Axillary Lymph Nodes in Breast Cancer—A Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Published Study Search and Selection Criteria
2.2. Data Extraction
2.3. Statistical Analysis
3. Results
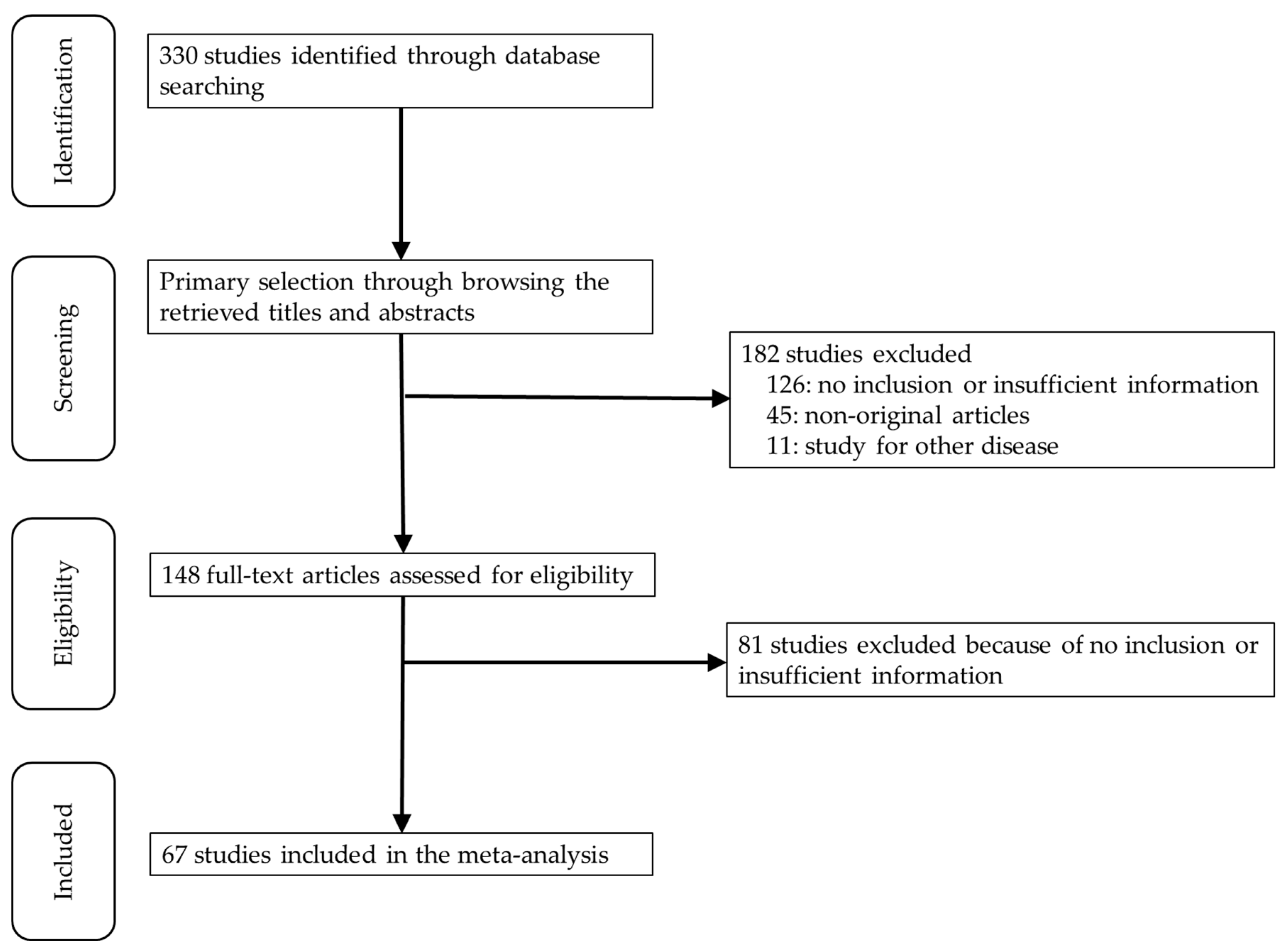
3.1. Selection and Characteristics
3.2. Comparison of Diagnostic Accuracy between Fine-Needle Aspiration Cytology and Core Needle Biopsy
3.3. Diagnostic Test Accuracy Review of Assessments for Axillary Lymph Nodes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Caudle, A.S.; Hunt, K.K.; Kuerer, H.M.; Meric-Bernstam, F.; Lucci, A.; Bedrosian, I.; Babiera, G.V.; Hwang, R.F.; Ross, M.I.; Feig, B.W.; et al. Multidisciplinary considerations in the implementation of the findings from the American College of Surgeons Oncology Group (ACOSOG) Z0011 study: A practice-changing trial. Ann. Surg. Oncol. 2011, 18, 2407–2412. [Google Scholar] [CrossRef] [Green Version]
- Senkus, E.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rutgers, E.; Zackrisson, S.; Cardoso, F. Primary breast cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2015, 26 (Suppl. 5), v8–v30. [Google Scholar] [CrossRef]
- Abe, H.; Schmidt, R.A.; Kulkarni, K.; Sennett, C.A.; Mueller, J.S.; Newstead, G.M. Axillary lymph nodes suspicious for breast cancer metastasis: Sampling with US-guided 14-gauge core-needle biopsy--clinical experience in 100 patients. Radiology 2009, 250, 41–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahn, H.S.; Kim, S.M.; Jang, M.; La Yun, B.; Kim, S.W.; Kang, E.; Park, S.Y.; Moon, W.K.; Choi, H.Y. Comparison of sonography with sonographically guided fine-needle aspiration biopsy and core-needle biopsy for initial axillary staging of breast cancer. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2013, 32, 2177–2184. [Google Scholar] [CrossRef] [PubMed]
- Attieh, M.; Jamali, F.; Berjawi, G.; Saadeldine, M.; Boulos, F. Shortcomings of ultrasound-guided fine needle aspiration in the axillary management of women with breast cancer. World J. Surg. Oncol. 2019, 17, 208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barco, I.; Chabrera, C.; García-Fernández, A.; Fraile, M.; González, S.; Canales, L.; Lain, J.M.; González, C.; Vidal, M.C.; Vallejo, E.; et al. Role of axillary ultrasound, magnetic resonance imaging, and ultrasound-guided fine-needle aspiration biopsy in the preoperative triage of breast cancer patients. Clin. Transl. Oncol. Off. Publ. Fed. Span. Oncol. Soc. Natl. Cancer Inst. Mex. 2017, 19, 704–710. [Google Scholar] [CrossRef]
- Bedrosian, I.; Bedi, D.; Kuerer, H.M.; Fornage, B.D.; Harker, L.; Ross, M.I.; Ames, F.C.; Krishnamurthy, S.; Edeiken-Monroe, B.S.; Meric, F.; et al. Impact of clinicopathological factors on sensitivity of axillary ultrasonography in the detection of axillary nodal metastases in patients with breast cancer. Ann. Surg. Oncol. 2003, 10, 1025–1030. [Google Scholar] [CrossRef]
- Bonnema, J.; van Geel, A.N.; van Ooijen, B.; Mali, S.P.; Tjiam, S.L.; Henzen-Logmans, S.C.; Schmitz, P.I.; Wiggers, T. Ultrasound-guided aspiration biopsy for detection of nonpalpable axillary node metastases in breast cancer patients: New diagnostic method. World J. Surg. 1997, 21, 270–274. [Google Scholar] [CrossRef] [Green Version]
- Boughey, J.C.; Middleton, L.P.; Harker, L.; Garrett, B.; Fornage, B.; Hunt, K.K.; Babiera, G.V.; Dempsey, P.; Bedrosian, I. Utility of ultrasound and fine-needle aspiration biopsy of the axilla in the assessment of invasive lobular carcinoma of the breast. Am. J. Surg. 2007, 194, 450–455. [Google Scholar] [CrossRef]
- Breitbach, G.P.; Uhlmann, J.H.; Bohle, R.M.; Juhasz-Böss, I.; Linxweiler, B.; Takacs, F.Z.; Solomayer, E.F.; Juhasz-Böss, S. Preoperative morphological diagnosis of axillary lymph nodes in a breast center consultation service: Evaluation of fine-needle aspiration and core biopsy techniques. Arch. Gynecol. Obstet. 2019, 300, 1659–1670. [Google Scholar] [CrossRef]
- Britton, P.D.; Goud, A.; Godward, S.; Barter, S.; Freeman, A.; Gaskarth, M.; Rajan, P.; Sinnatamby, R.; Slattery, J.; Provenzano, E.; et al. Use of ultrasound-guided axillary node core biopsy in staging of early breast cancer. Eur. Radiol. 2009, 19, 561–569. [Google Scholar] [CrossRef]
- Bruzzone, M.; Saro, F.; Bruno, S.; Celiento, T.; Mazzarella, G.; Lanata, S.; Aquilano, M.C.; Parmigiani, G.; Pollone, M.; Gandolfo, F.; et al. Synergy of cytological methods in the pathological staging of breast cancer: Axillary fine-needle aspiration and intraoperative scrape cytology of the sentinel lymph node. Diagn. Cytopathol. 2018, 46, 919–926. [Google Scholar] [CrossRef] [PubMed]
- Caretta-Weyer, H.; Sisney, G.A.; Beckman, C.; Burnside, E.S.; Salkowsi, L.R.; Strigel, R.M.; Wilke, L.G.; Neuman, H.B. Impact of axillary ultrasound and core needle biopsy on the utility of intraoperative frozen section analysis and treatment decision making in women with invasive breast cancer. Am. J. Surg. 2012, 204, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Castellano, I.; Deambrogio, C.; Muscarà, F.; Chiusa, L.; Mariscotti, G.; Bussone, R.; Gazzetta, G.; Macrì, L.; Cassoni, P.; Sapino, A. Efficiency of a preoperative axillary ultrasound and fine-needle aspiration cytology to detect patients with extensive axillary lymph node involvement. PLoS ONE 2014, 9, e106640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.S.; Han, K.H.; Kim, E.K.; Moon, H.J.; Yoon, J.H.; Kim, M.J. Fine-needle aspirate CYFRA 21-1, an innovative new marker for diagnosis of axillary lymph node metastasis in breast cancer patients. Medicine 2015, 94, e811. [Google Scholar] [CrossRef] [PubMed]
- Ciatto, S.; Brancato, B.; Risso, G.; Ambrogetti, D.; Bulgaresi, P.; Maddau, C.; Turco, P.; Houssami, N. Accuracy of fine needle aspiration cytology (FNAC) of axillary lymph nodes as a triage test in breast cancer staging. Breast Cancer Res. Treat. 2007, 103, 85–91. [Google Scholar] [CrossRef]
- Cools-Lartigue, J.; Sinclair, A.; Trabulsi, N.; Meguerditchian, A.; Mesurolle, B.; Fuhrer, R.; Meterissian, S. Preoperative axillary ultrasound and fine-needle aspiration biopsy in the diagnosis of axillary metastases in patients with breast cancer: Predictors of accuracy and future implications. Ann. Surg. Oncol. 2013, 20, 819–827. [Google Scholar] [CrossRef]
- De Coninck, C.; Noël, J.C.; Boutemy, R.; Simon, P. Preoperative axillary lymph node staging by ultrasound-guided cytology using a four-level sonographic score. BMC Med. Imaging 2016, 16, 13. [Google Scholar] [CrossRef] [Green Version]
- De Kanter, A.Y.; Menke-Pluijmers, M.B.; Henzen-Logmans, S.C.; van Geel, A.N.; van Eijck, C.J.; Wiggers, T.; Eggermont, A.M. Reasons for failure to identify positive sentinel nodes in breast cancer patients with significant nodal involvement. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2006, 32, 498–501. [Google Scholar] [CrossRef]
- Devaraj, S.; Iqbal, M.; Donnelly, J.; Corder, A.P. Axillary ultrasound in invasive breast cancer: experience of our surgeons. Breast J. 2011, 17, 191–195. [Google Scholar] [CrossRef]
- Engohan-Aloghe, C.; Hottat, N.; Noël, J.C. Accuracy of lymph nodes cell block preparation according to ultrasound features in preoperative staging of breast cancer. Diagn. Cytopathol. 2010, 38, 5–8. [Google Scholar] [CrossRef] [PubMed]
- Fayyaz, M.B.; Niazi, I.K. Diagnostic accuracy of us-fnac of axillary lymph nodes in patients with primary breast cancer using sentinel lymph node biopsy as standard reference. J. Ayub Med. Coll. Abbottabad JAMC 2019, 31, 242–247. [Google Scholar] [PubMed]
- Feng, Y.; Huang, R.; He, Y.; Lu, A.; Fan, Z.; Fan, T.; Qi, M.; Wang, X.; Cao, W.; Wang, X.; et al. Efficacy of physical examination, ultrasound, and ultrasound combined with fine-needle aspiration for axilla staging of primary breast cancer. Breast Cancer Res. Treat. 2015, 149, 761–765. [Google Scholar] [CrossRef] [PubMed]
- Fung, A.D.; Collins, J.A.; Campassi, C.; Ioffe, O.B.; Staats, P.N. Performance characteristics of ultrasound-guided fine-needle aspiration of axillary lymph nodes for metastatic breast cancer employing rapid on-site evaluation of adequacy: Analysis of 136 cases and review of the literature. Cancer Cytopathol. 2014, 122, 282–291. [Google Scholar] [CrossRef] [PubMed]
- García Fernández, A.; Fraile, M.; Giménez, N.; Reñe, A.; Torras, M.; Canales, L.; Torres, J.; Barco, I.; González, S.; Veloso, E.; et al. Use of axillary ultrasound, ultrasound-fine needle aspiration biopsy and magnetic resonance imaging in the preoperative triage of breast cancer patients considered for sentinel node biopsy. Ultrasound Med. Biol. 2011, 37, 16–22. [Google Scholar] [CrossRef]
- Genta, F.; Zanon, E.; Camanni, M.; Deltetto, F.; Drogo, M.; Gallo, R.; Gilardi, C. Cost/accuracy ratio analysis in breast cancer patients undergoing ultrasound-guided fine-needle aspiration cytology, sentinel node biopsy, and frozen section of node. World J. Surg. 2007, 31, 1155–1163. [Google Scholar] [CrossRef]
- Gipponi, M.; Fregatti, P.; Garlaschi, A.; Murelli, F.; Margarino, C.; Depaoli, F.; Baccini, P.; Gallo, M.; Friedman, D. Axillary ultrasound and Fine-Needle Aspiration Cytology in the preoperative staging of axillary node metastasis in breast cancer patients. Breast (Edinb. Scotl.) 2016, 30, 146–150. [Google Scholar] [CrossRef]
- Hayes, B.D.; Feeley, L.; Quinn, C.M.; Kennedy, M.M.; O’Doherty, A.; Flanagan, F.; O’Connell, A.M. Axillary fine needle aspiration cytology for pre-operative staging of patients with screen-detected invasive breast carcinoma. J. Clin. Pathol. 2011, 64, 338–342. [Google Scholar] [CrossRef]
- Hyun, S.J.; Kim, E.K.; Yoon, J.H.; Moon, H.J.; Kim, M.J. Adding MRI to ultrasound and ultrasound-guided fine-needle aspiration reduces the false-negative rate of axillary lymph node metastasis diagnosis in breast cancer patients. Clin. Radiol. 2015, 70, 716–722. [Google Scholar] [CrossRef]
- Imai, N.; Kitayama, M.; Shibahara, A.; Bessho, Y.; Shibusawa, M.; Noro, A.; Inakami, K.; Hanamura, N.; Imai, H.; Ogawa, T. Strategy for the accurate preoperative evaluation of the number of metastatic axillary lymph nodes in breast cancer. Asian J. Surg. 2019, 42, 228–234. [Google Scholar] [CrossRef]
- Iwamoto, N.; Aruga, T.; Horiguchi, S.; Asami, H.; Saita, C.; Onishi, M.; Goto, R.; Ishiba, T.; Honda, Y.; Miyamoto, H.; et al. Ultrasound-guided fine-needle aspiration of axillary lymph nodes in breast cancer: Diagnostic accuracy and role in surgical management. Diagn. Cytopathol. 2019, 47, 788–792. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Haisfield-Wolfe, M.E.; Lange, J.; Ahuja, N.; Khouri, N.; Tsangaris, T.; Zhang, Z.; Balch, C.; Jacobs, L.K. The role of ultrasound-guided fine-needle aspiration of axillary nodes in the staging of breast cancer. Ann. Surg. Oncol. 2008, 15, 462–471. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.; Park, H.; Park, J.; Kim, H. Accuracy of preoperative ultrasound and ultrasound-guided fine needle aspiration cytology for axillary staging in breast cancer. ANZ J. Surg. 2010, 80, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Kane, G.; Fleming, C.; Heneghan, H.; McCartan, D.; James, P.; Trueick, R.; Harrington, L.; Nally, F.; Quinn, C.; O’Doherty, A.; et al. False-negative rate of ultrasound-guided fine-needle aspiration cytology for identifying axillary lymph node metastasis in breast cancer patients. Breast J. 2019, 25, 848–852. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.J.; Park, B.W.; Lim, J.B.; Kim, H.S.; Kwak, J.Y.; Kim, S.J.; Park, S.H.; Sohn, Y.M.; Moon, H.J.; Kim, E.K. Axillary lymph node metastasis: CA-15-3 and carcinoembryonic antigen concentrations in fine-needle aspirates for preoperative diagnosis in patients with breast cancer. Radiology 2010, 254, 691–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.Y.; Kim, E.K.; Moon, H.J.; Yoon, J.H.; Kim, M.J. Is pre-operative axillary staging with ultrasound and ultrasound-guided fine-needle aspiration reliable in invasive lobular carcinoma of the breast? Ultrasound Med. Biol. 2016, 42, 1263–1272. [Google Scholar] [CrossRef]
- Koelliker, S.L.; Chung, M.A.; Mainiero, M.B.; Steinhoff, M.M.; Cady, B. Axillary lymph nodes: US-guided fine-needle aspiration for initial staging of breast cancer–correlation with primary tumor size. Radiology 2008, 246, 81–89. [Google Scholar] [CrossRef]
- Kramer, G.M.; Leenders, M.W.; Schijf, L.J.; Go, H.L.; van der Ploeg, T.; van den Tol, M.P.; Schreurs, W.H. Is ultrasound-guided fine-needle aspiration cytology of adequate value in detecting breast cancer patients with three or more positive axillary lymph nodes? Breast Cancer Res. Treat. 2016, 156, 271–278. [Google Scholar] [CrossRef]
- Krishnamurthy, S.; Sneige, N.; Bedi, D.G.; Edieken, B.S.; Fornage, B.D.; Kuerer, H.M.; Singletary, S.E.; Hunt, K.K. Role of ultrasound-guided fine-needle aspiration of indeterminate and suspicious axillary lymph nodes in the initial staging of breast carcinoma. Cancer 2002, 95, 982–988. [Google Scholar] [CrossRef]
- Kuenen-Boumeester, V.; Menke-Pluymers, M.; de Kanter, A.Y.; Obdeijn, I.M.; Urich, D.; Van Der Kwast, T.H. Ultrasound-guided fine needle aspiration cytology of axillary lymph nodes in breast cancer patients. A preoperative staging procedure. Eur. J. Cancer (Oxf. Engl. 1990) 2003, 39, 170–174. [Google Scholar] [CrossRef]
- Leenders, M.W.; Broeders, M.; Croese, C.; Richir, M.C.; Go, H.L.; Langenhorst, B.L.; Meijer, S.; Schreurs, W.H. Ultrasound and fine needle aspiration cytology of axillary lymph nodes in breast cancer. to do or not to do? Breast (Edinb. Scotl.) 2012, 21, 578–583. [Google Scholar] [CrossRef] [PubMed]
- Leenders, M.; Richir, M.; Broeders, M.; Moormann, G.; Mollema, R.; Lopes Cardozo, A.; Meijer, S.; Schreurs, H. Axillary staging by ultrasound-guided fine-needle aspiration cytology in breast cancer patients. still up to date? Breast J. 2013, 19, 637–642. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Chen, X.; Zhan, W.; Garfield, D.H.; Wu, J.; Huang, O.; Li, Y.; Zhu, L.; Chen, W.; Shen, K. Can clinically node-negative breast cancer patients with suspicious axillary lymph nodes at ultrasound but negative fine-needle aspiration be approached as having node-negative disease? Ann. Surg. Oncol. 2017, 24, 1874–1880. [Google Scholar] [CrossRef] [PubMed]
- Machida, Y.; Kubota, K.; Katayama, T.; Toriihara, A.; Shibuya, H. Diagnostic performance of fluorodeoxyglucose-positron emission tomography/computed tomography combined with ultrasonography-guided fine needle aspiration cytology for identifying axillary lymph node status in patients with breast cancer. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2013, 39, 26–30. [Google Scholar] [CrossRef] [PubMed]
- MacNeill, M.; Arnott, I.; Thomas, J. Fine needle aspiration cytology is a valuable adjunct to axillary ultrasound in the preoperative staging of breast cancer. J. Clin. Pathol. 2011, 64, 42–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marti, J.L.; Ayo, D.; Levine, P.; Hernandez, O.; Rescigno, J.; Axelrod, D.M. Nonimage-guided fine needle aspiration biopsy of palpable axillary lymph nodes in breast cancer patients. Breast J. 2012, 18, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, A.J.; Bundred, N.J.; Harvey, J.; Hunt, R.; Morris, J.; Lim, Y.Y. A randomised pilot study comparing 13 G vacuum-assisted biopsy and conventional 14 G core needle biopsy of axillary lymph nodes in women with breast cancer. Clin. Radiol. 2016, 71, 551–557. [Google Scholar] [CrossRef]
- Moorman, A.M.; Bourez, R.L.; de Leeuw, D.M.; Kouwenhoven, E.A. Pre-operative Ultrasonographic evaluation of axillary lymph nodes in breast cancer patients: For which group still of additional value and in which group cause for special attention? Ultrasound Med. Biol. 2015, 41, 2842–2848. [Google Scholar] [CrossRef]
- Motomura, K.; Inaji, H.; Komoike, Y.; Kasugai, T.; Nagumo, S.; Hasegawa, Y.; Noguchi, S.; Koyama, H. Gamma probe and ultrasonographically-guided fine-needle aspiration biopsy of sentinel lymph nodes in breast cancer patients. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2001, 27, 141–145. [Google Scholar] [CrossRef]
- Nakamura, R.; Yamamoto, N.; Miyaki, T.; Itami, M.; Shina, N.; Ohtsuka, M. Impact of sentinel lymph node biopsy by ultrasound-guided core needle biopsy for patients with suspicious node positive breast cancer. Breast Cancer (Tokyo Jpn.) 2018, 25, 86–93. [Google Scholar] [CrossRef]
- O’Leary, D.P.; O’Brien, O.; Relihan, N.; McCarthy, J.; Ryan, M.; Barry, J.; Kelly, L.M.; Redmond, H.P. Rapid on-site evaluation of axillary fine-needle aspiration cytology in breast cancer. Br. J. Surg. 2012, 99, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Kim, M.J.; Park, B.W.; Moon, H.J.; Kwak, J.Y.; Kim, E.K. Impact of preoperative ultrasonography and fine-needle aspiration of axillary lymph nodes on surgical management of primary breast cancer. Ann. Surg. Oncol. 2011, 18, 738–744. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Kim, E.K.; Park, B.W.; Kim, S.I.; Moon, H.J.; Kim, M.J. False negative results in axillary lymph nodes by ultrasonography and ultrasonography-guided fine-needle aspiration in patients with invasive ductal carcinoma. Ultraschall der Med. (Stuttg. Ger. 1980) 2013, 34, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Podkrajsek, M.; Music, M.M.; Kadivec, M.; Zgajnar, J.; Besic, N.; Pogacnik, A.; Hocevar, M. Role of ultrasound in the preoperative staging of patients with breast cancer. Eur. Radiol. 2005, 15, 1044–1050. [Google Scholar] [CrossRef] [PubMed]
- Popli, M.B.; Sahoo, M.; Mehrotra, N.; Choudhury, M.; Kumar, A.; Pathania, O.P.; Thomas, S. Preoperative ultrasound-guided fine-needle aspiration cytology for axillary staging in breast carcinoma. Australas. Radiol. 2006, 50, 122–126. [Google Scholar] [CrossRef] [PubMed]
- Rao, R.; Lilley, L.; Andrews, V.; Radford, L.; Ulissey, M. Axillary staging by percutaneous biopsy: sensitivity of fine-needle aspiration versus core needle biopsy. Ann. Surg. Oncol. 2009, 16, 1170–1175. [Google Scholar] [CrossRef]
- Rattay, T.; Muttalib, M.; Khalifa, E.; Duncan, A.; Parker, S.J. Clinical utility of routine pre-operative axillary ultrasound and fine needle aspiration cytology in patient selection for sentinel lymph node biopsy. Breast (Edinb. Scotl.) 2012, 21, 210–214. [Google Scholar] [CrossRef]
- Rautiainen, S.; Masarwah, A.; Sudah, M.; Sutela, A.; Pelkonen, O.; Joukainen, S.; Sironen, R.; Kärjä, V.; Vanninen, R. Axillary lymph node biopsy in newly diagnosed invasive breast cancer: Comparative accuracy of fine-needle aspiration biopsy versus core-needle biopsy. Radiology 2013, 269, 54–60. [Google Scholar] [CrossRef] [Green Version]
- Sapino, A.; Cassoni, P.; Zanon, E.; Fraire, F.; Croce, S.; Coluccia, C.; Donadio, M.; Bussolati, G. Ultrasonographically-guided fine-needle aspiration of axillary lymph nodes: Role in breast cancer management. Br. J. Cancer 2003, 88, 702–706. [Google Scholar] [CrossRef] [Green Version]
- Schiettecatte, A.; Bourgain, C.; Breucq, C.; Buls, N.; De Wilde, V.; de Mey, J. Initial axillary staging of breast cancer using ultrasound-guided fine needle aspiration: A liquid-based cytology study. Cytopathol. Off. J. Br. Soc. Clin. Cytol. 2011, 22, 30–35. [Google Scholar] [CrossRef]
- Swinson, C.; Ravichandran, D.; Nayagam, M.; Allen, S. Ultrasound and fine needle aspiration cytology of the axilla in the pre-operative identification of axillary nodal involvement in breast cancer. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2009, 35, 1152–1157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Topal, U.; Punar, S.; Taşdelen, I.; Adim, S.B. Role of ultrasound-guided core needle biopsy of axillary lymph nodes in the initial staging of breast carcinoma. Eur. J. Radiol. 2005, 56, 382–385. [Google Scholar] [CrossRef] [PubMed]
- Tsai, W.C.; Lin, C.K.; Wei, H.K.; Yu, B.L.; Hung, C.F.; Cheng, S.H.; Chen, C.M. Sonographic elastography improves the sensitivity and specificity of axilla sampling in breast cancer: A prospective study. Ultrasound Med. Biol. 2013, 39, 941–949. [Google Scholar] [CrossRef] [PubMed]
- Usmani, S.; Ahmed, N.; Al Saleh, N.; abu Huda, F.; Amanguno, H.G.; Amir, T.; al Kandari, F. The clinical utility of combining pre-operative axillary ultrasonography and fine needle aspiration cytology with radionuclide guided sentinel lymph node biopsy in breast cancer patients with palpable axillary lymph nodes. Eur. J. Radiol. 2015, 84, 2515–2520. [Google Scholar] [CrossRef] [PubMed]
- Van Berckelaer, C.; Huizing, M.; Van Goethem, M.; Vervaecke, A.; Papadimitriou, K.; Verslegers, I.; Trinh, B.X.; Van Dam, P.; Altintas, S.; Van den Wyngaert, T.; et al. Preoperative ultrasound staging of the axilla make’s peroperative examination of the sentinel node redundant in breast cancer: saving tissue, time and money. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 206, 164–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Wely, B.J.; de Wilt, J.H.; Schout, P.J.; Kooistra, B.; Wauters, C.A.; Venderinck, D.; Strobbe, L.J. Ultrasound-guided fine-needle aspiration of suspicious nodes in breast cancer patients; selecting patients with extensive nodal involvement. Breast Cancer Res. Treat. 2013, 140, 113–118. [Google Scholar] [CrossRef]
- Zhang, F.; Zhang, J.; Meng, Q.X.; Zhang, X. Ultrasound combined with fine needle aspiration cytology for the assessment of axillary lymph nodes in patients with early stage breast cancer. Medicine 2018, 97, e9855. [Google Scholar] [CrossRef]
- Zhong, J.; Sun, D.S.; Wei, W.; Liu, X.; Liu, J.; Wu, X.; Zhang, Y.; Luo, H.; Li, Y. Contrast-enhanced ultrasound-guided fine-needle aspiration for sentinel lymph node biopsy in early-stage breast cancer. Ultrasound Med. Biol. 2018, 44, 1371–1378. [Google Scholar] [CrossRef]
- Zhu, Y.; Zhou, W.; Zhou, J.Q.; Fei, X.C.; Ye, T.J.; Huang, O.; Chen, X.S.; Zhan, W.W. Axillary staging of early-stage invasive breast cancer by ultrasound-guided fine-needle aspiration cytology: Which ultrasound criteria for classifying abnormal lymph nodes should be adopted in the Post-ACOSOG Z0011 trial era? J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 2016, 35, 885–893. [Google Scholar] [CrossRef] [Green Version]
- Ewing, D.E.; Layfield, L.J.; Joshi, C.L.; Travis, M.D. Determinants of false-negative fine-needle aspirates of axillary lymph nodes in women with breast cancer: Lymph node size, cortical thickness and hilar fat retention. Acta Cytol. 2015, 59, 311–314. [Google Scholar] [CrossRef]
- Deurloo, E.E.; Tanis, P.J.; Gilhuijs, K.G.; Muller, S.H.; Kröger, R.; Peterse, J.L.; Rutgers, E.J.; Valdés Olmos, R.; Schultze Kool, L.J. Reduction in the number of sentinel lymph node procedures by preoperative ultrasonography of the axilla in breast cancer. Eur. J. Cancer (Oxf. Engl. 1990) 2003, 39, 1068–1073. [Google Scholar] [CrossRef]
- Ertan, K.; Linsler, C.; di Liberto, A.; Ong, M.F.; Solomayer, E.; Endrikat, J. Axillary ultrasound for breast cancer staging: An attempt to identify clinical/histopathological factors impacting diagnostic performance. Breast Cancer Basic Clin. Res. 2013, 7, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Damera, A.; Evans, A.J.; Cornford, E.J.; Wilson, A.R.; Burrell, H.C.; James, J.J.; Pinder, S.E.; Ellis, I.O.; Lee, A.H.; Macmillan, R.D. Diagnosis of axillary nodal metastases by ultrasound-guided core biopsy in primary operable breast cancer. Br. J. Cancer 2003, 89, 1310–1313. [Google Scholar] [CrossRef] [PubMed]
- De Kanter, A.Y.; van Eijck, C.H.; van Geel, A.N.; Kruijt, R.H.; Henzen, S.C.; Paul, M.A.; Eggermont, A.M.; Wiggers, T. Multicentre study of ultrasonographically guided axillary node biopsy in patients with breast cancer. Br. J. Surg. 1999, 86, 1459–1462. [Google Scholar] [CrossRef]
- Van Rijk, M.C.; Deurloo, E.E.; Nieweg, O.E.; Gilhuijs, K.G.; Peterse, J.L.; Rutgers, E.J.; Kröger, R.; Kroon, B.B. Ultrasonography and fine-needle aspiration cytology can spare breast cancer patients unnecessary sentinel lymph node biopsy. Ann. Surg. Oncol. 2006, 13, 31–35. [Google Scholar] [CrossRef]
- Vassallo, P.; Wernecke, K.; Roos, N.; Peters, P.E. Differentiation of benign from malignant superficial lymphadenopathy: The role of high-resolution US. Radiology 1992, 183, 215–220. [Google Scholar] [CrossRef]
- Del Bianco, P.; Zavagno, G.; Burelli, P.; Scalco, G.; Barutta, L.; Carraro, P.; Pietrarota, P.; Meneghini, G.; Morbin, T.; Tacchetti, G.; et al. Morbidity comparison of sentinel lymph node biopsy versus conventional axillary lymph node dissection for breast cancer patients: Results of the sentinella-GIVOM Italian randomised clinical trial. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2008, 34, 508–513. [Google Scholar] [CrossRef]
- Stachs, A.; Göde, K.; Hartmann, S.; Stengel, B.; Nierling, U.; Dieterich, M.; Reimer, T.; Gerber, B. Accuracy of axillary ultrasound in preoperative nodal staging of breast cancer-size of metastases as limiting factor. SpringerPlus 2013, 2, 350. [Google Scholar] [CrossRef] [Green Version]
- Akıncı, M.; Bulut, S.P.; Erözgen, F.; Gürbüzel, M.; Gülşen, G.; Kocakuşak, A.; Gülen, M.; Kaplan, R. Predictive value of fine needle aspiration biopsy of axillary lymph nodes in preoperative breast cancer staging. Ulus. Cerrahi Derg. 2016, 32, 191–196. [Google Scholar] [CrossRef] [Green Version]
- Gilani, S.M.; Fathallah, L.; Al-Khafaji, B.M. Preoperative fine needle aspiration of axillary lymph nodes in breast cancer: Clinical utility, diagnostic accuracy and potential pitfalls. Acta Cytol. 2014, 58, 248–254. [Google Scholar] [CrossRef]
- Mustonen, P.; Farin, P.; Kosunen, O. Ultrasonographic detection of metastatic axillary lymph nodes in breast cancer. Ann. Chir. Gynaecol. 1990, 79, 15–18. [Google Scholar] [PubMed]
- Yang, W.T.; Ahuja, A.; Tang, A.; Suen, M.; King, W.; Metreweli, C. High resolution sonographic detection of axillary lymph node metastases in breast cancer. J. Ultrasound Med. Off. J. Am. Inst. Ultrasound Med. 1996, 15, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Luparia, A.; Campanino, P.; Cotti, R.; Lucarelli, D.; Durando, M.; Mariscotti, G.; Gandini, G. Role of axillary ultrasound in the preoperative diagnosis of lymph node metastases in patients affected by breast carcinoma. Radiol. Med. 2010, 115, 225–237. [Google Scholar] [CrossRef]
- Balasubramanian, I.; Fleming, C.A.; Corrigan, M.A.; Redmond, H.P.; Kerin, M.J.; Lowery, A.J. Meta-analysis of the diagnostic accuracy of ultrasound-guided fine-needle aspiration and core needle biopsy in diagnosing axillary lymph node metastasis. Br. J. Surg. 2018, 105, 1244–1253. [Google Scholar] [CrossRef] [PubMed]
- Topps, A.R.; Barr, S.P.; Pikoulas, P.; Pritchard, S.A.; Maxwell, A.J. Pre-operative axillary ultrasound-guided needle sampling in breast cancer: Comparing the sensitivity of fine needle aspiration cytology and core needle biopsy. Ann. Surg. Oncol. 2018, 25, 148–153. [Google Scholar] [CrossRef] [PubMed]
- Vidya, R.; Iqbal, F.M.; Bickley, B. Pre-operative axillary staging: Should core biopsy be preferred to fine needle aspiration cytology? Ecancermedicalscience 2017, 11, 724. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Reference | Location | Method | Number of Patients | Reference | Location | Method | Number of Patients | ||
|---|---|---|---|---|---|---|---|---|---|
| Accurate | Total | Accurate | Total | ||||||
| Abe 2009 [3] | USA | CNB (ND) | 78 | 88 | Koelliker 2008 [37] | Island | FNAC (LBP) | 60 | 72 |
| Ahn 2013 [4] | Korea | FNAC (CS) | 41 | 48 | Kramer 2016 [38] | Netherlands | FNAC (ND) | 430 | 543 |
| CNB-Stericut | 42 | 48 | Krishnamurthy 2002 [39] | USA | FNAC (CS) | 75 | 103 | ||
| Attieh 2019 [5] | Lebanon | FNAC (ND) | 89 | 101 | Kuenen 2003 [40] | Netherlands | FNAC (CS) | 103 | 134 |
| Barco 2017 [6] | Spain | FNAC (ND) | 320 | 390 | Leenders 2012 [41] | Netherlands | FNAC (ND) | 215 | 274 |
| Bedrosian 2003 [7] | USA | FNAC (ND) | 13 | 22 | Leenders 2013 [42] | Netherlands | FNAC (ND) | 363 | 530 |
| Bonnema 1997 [8] | Netherlands | FNAC (CS) | 71 | 81 | Liang 2017 [43] | China | FNAC (ND) | 237 | 263 |
| Boughey 2007 [9] | USA | FNAC (ND) | 60 | 76 | Machida 2013 [44] | Japan | FNAC (CS) | 33 | 41 |
| Breitbach 2019 [10] | Germany | FNAC (ND) | 46 | 60 | MacNeill 2011 [45] | UK | FNAC (ND) | 74 | 93 |
| CNB-BARD® | 10 | 10 | Marti 2012 [46] | USA | FNAC (CS) | 78 | 86 | ||
| Britton 2009 [11] | UK | CNB-BARD® | 91 | 116 | Maxwell 2016 [47] | UK | CNB-Achieve® | 33 | 37 |
| Bruzzone 2018 [12] | Italy | FNAC (ND) | 363 | 439 | Moorman 2015 [48] | Netherlands | FNAC (LBP) | 148 | 202 |
| Caretta-Weyer 2012 [13] | USA | CNB (ND) | 24 | 26 | Motomura 2001 [49] | Japan | FNAC (CS) | 25 | 29 |
| Castellano 2014 [14] | Italy | FNAC (CS) | 134 | 146 | Nakamura 2018 [50] | Japan | CNB-BARD® | 260 | 272 |
| Choi 2015 [15] | Korea | FNAC (CS) | 334 | 373 | FNAC (CS) | 650 | 744 | ||
| Ciatto 2007 [16] | Italy | FNAC (CS) | 337 | 418 | O’Leary 2012 [51] | Ireland | FNAC (CS) | 108 | 129 |
| Cools 2013 [17] | Canada | FNAC (ND) | 31 | 53 | Park 2011 [52] | Korea | FNAC (CS) | 293 | 382 |
| de Coninck 2016 [18] | Belgium | FNAC (CB) | 42 | 49 | Park 2013 [53] | Korea | FNAC (CS) | 127 | 145 |
| de Kanter 2006 [19] | Netherlands | FNAC (ND) | 113 | 161 | Podkrajsek 2005 [54] | Slovenia | FNAC (CS) | 39 | 44 |
| Devaraj 2011 [20] | UK | FNAC (ND) | 44 | 45 | Popli 2006 [55] | India | FNAC (CS) | 20 | 24 |
| Engohan 2011 [21] | Belgium | FNAC (CB) | 19 | 22 | Rao 2009 [56] | USA | FNAC (ND) | 18 | 22 |
| Fayyaz 2019 [22] | Pakistan | FNAC (CS) | 136 | 160 | CNB (ND) | 21 | 25 | ||
| Feng 2015 [23] | China | FNAC (LBP) | 1056 | 1152 | Rattay 2012 [57] | UK | FNAC (CS) | 49 | 56 |
| Fung 2014 [24] | USA | FNAC (LBP) | 106 | 130 | Rautiainen 2013 [58] | Finland | FNAC (CS) | 52 | 66 |
| García 2011 [25] | Spain | FNAC (CS) | 88 | 96 | CNB (ND) | 60 | 66 | ||
| Genta 2007 [26] | Italy | FNAC (CS) | 74 | 97 | Sapino 2003 [59] | Italy | FNAC (CS) | 79 | 85 |
| Gipponi 2016 [27] | Italy | FNAC (ND) | 329 | 400 | Schiettecatte 2011 [60] | Belgium | FNAC (LBP) | 48 | 58 |
| Hayes 2011 [28] | Ireland | FNAC (CS) | 131 | 161 | Swinson 2009 [61] | UK | FNAC (ND) | 87 | 96 |
| Hyun 2015 [29] | Korea | FNAC (CS) | 161 | 176 | Topal 2005 [62] | Turkey | CNB-BARD® | 36 | 39 |
| Imai 2018 [30] | Japan | FNAC (CS) | 140 | 162 | Tsai 2013 [63] | Taiwan | FNAC (ND) | 61 | 66 |
| Iwamoto 2019 [31] | Japan | FNAC (CS) | 140 | 174 | Usmani 2015 [64] | Kuwait | FNAC (LBP) | 47 | 53 |
| Jain 2008 [32] | USA | FNAC (CS) | 57 | 69 | Van Berckelaer 2016 [65] | Belgium | FNAC (LBP) | 291 | 317 |
| Jung 2010 [33] | Korea | FNAC (CS) | 37 | 39 | Van Wely 2013 [66] | Netherlands | FNAC (CS) | 179 | 198 |
| Kane 2019 [34] | Ireland | FNAC (ND) | 480 | 589 | Zhang 2018 [67] | China | FNAC (LBP) | 110 | 124 |
| Kim 2010 [35] | Korea | FNAC (CS) | 123 | 134 | Zhong 2018 [68] | China | FNAC (CS) | 120 | 126 |
| Kim 2016 [36] | Korea | FNAC (ND) | 24 | 32 | Zhu 2016 [69] | China | FNAC (CS) | 235 | 263 |
| Comparison | Number of Subsets | Heterogeneity (p-Value) | Random Effect (95% CI) | Egger’s Test (p-Value) | MRT * (p-Value) |
|---|---|---|---|---|---|
| Preoperative evaluation of ALNs | 72 | <0.001 | 0.850 (0.833, 0.866) | 0.005 | |
| Fine-needle aspiration cytology | 62 | <0.001 | 0.844 (0.825, 0.862) | 0.024 | 0.044 |
| CS | 32 | <0.001 | 0.860 (0.839, 0.879) | 0.029 | 0.145 |
| LBP | 8 | <0.001 | 0.861 (0.797, 0.908) | 0.460 | 0.332 |
| CB | 2 | 0.942 | 0.859 (0.758, 0.922) | - | 0.544 |
| Core needle biopsy | 10 | 0.002 | 0.896 (0.844, 0.932) | 0.344 |
| Comparison | Included Studies | Sensitivity (%) (95% CI) | Specificity (%) (95% CI) | Diagnostic OR (95% CI) | AUC on SROC |
|---|---|---|---|---|---|
| Fine-needle aspiration cytology | 62 | 0.760 (0.723, 0.794) | 0.997 (0.990, 0.999) | 113.256 (71.292, 179, 922) | 0.922 |
| CS | 32 | 0.791 (0.750, 0.827) | 0.996 (0.982, 0.999) | 122.599 (68.009, 221.008) | 0.934 |
| LBP | 8 | 0.784 (0.717, 0.839) | 1.000 (0.000, 1.000) | 217.586 (49.755, 951.541) | 0.917 |
| CB | 2 | 0.643 (0.454, 0.796) | - | 72.146 (8.546, 609.058) | 0.934 |
| Core needle biopsy | 10 | 0.849 (0.776, 0.901) | 1.000 (0.002, 1.000) | 119.486 (53.021, 269.271) | 0.951 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pyo, J.-S.; Jung, J.; Lee, S.G.; Kim, N.-Y.; Kang, D.-W. Diagnostic Accuracy of Fine-Needle Aspiration Cytology and Core-Needle Biopsy in the Assessment of the Axillary Lymph Nodes in Breast Cancer—A Meta-Analysis. Diagnostics 2020, 10, 717. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10090717
Pyo J-S, Jung J, Lee SG, Kim N-Y, Kang D-W. Diagnostic Accuracy of Fine-Needle Aspiration Cytology and Core-Needle Biopsy in the Assessment of the Axillary Lymph Nodes in Breast Cancer—A Meta-Analysis. Diagnostics. 2020; 10(9):717. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10090717
Chicago/Turabian StylePyo, Jung-Soo, Jaehag Jung, Seul Gi Lee, Nae-Yu Kim, and Dong-Wook Kang. 2020. "Diagnostic Accuracy of Fine-Needle Aspiration Cytology and Core-Needle Biopsy in the Assessment of the Axillary Lymph Nodes in Breast Cancer—A Meta-Analysis" Diagnostics 10, no. 9: 717. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10090717