Increased Risk of Migraine in Patients with Temporomandibular Disorder: A Longitudinal Follow-Up Study Using a National Health Screening Cohort

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
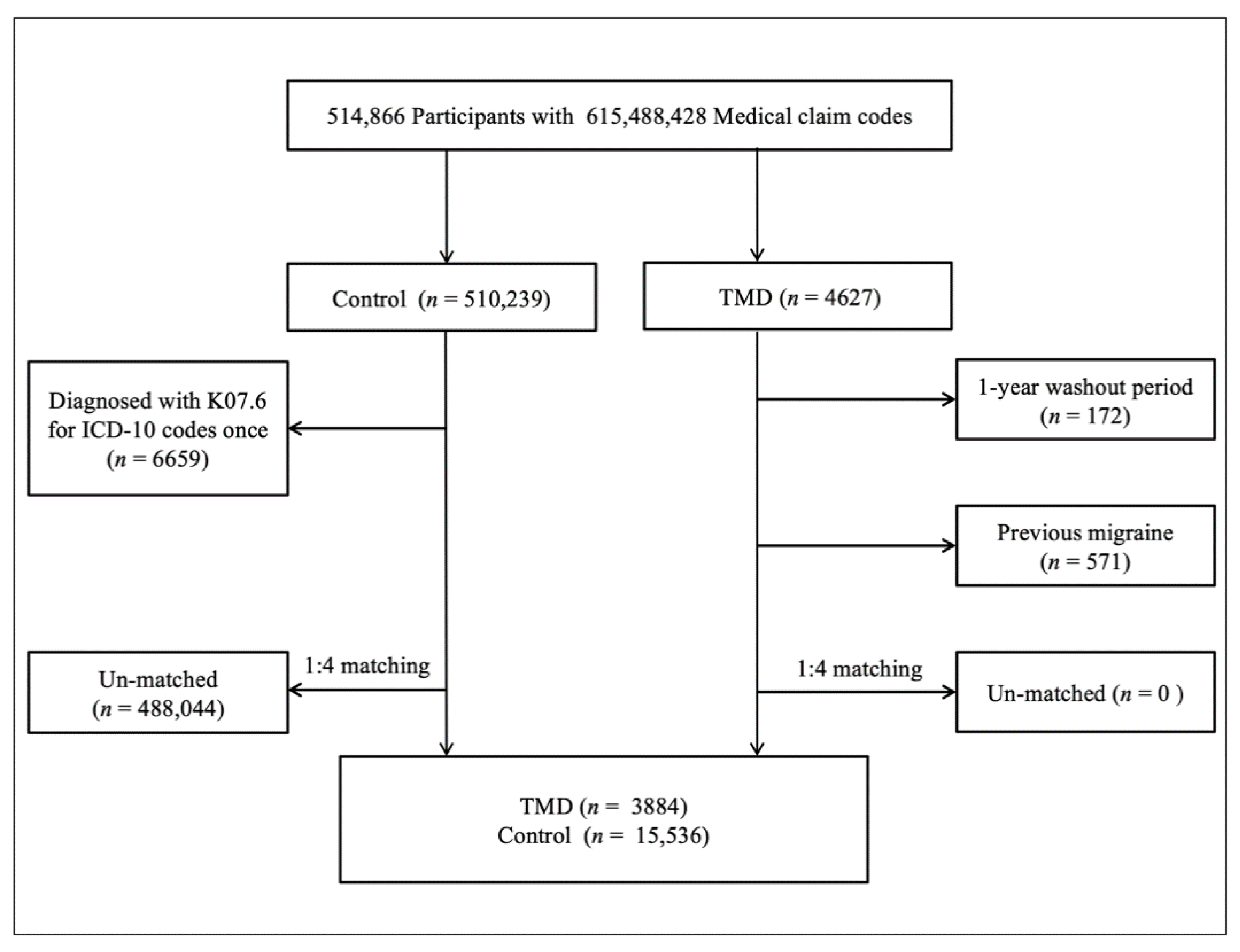
2.1. Study Population
2.2. Definition of Temporomandibular Disorder
2.3. Definition of Migraine
2.4. Participant Selection
2.5. Covariates
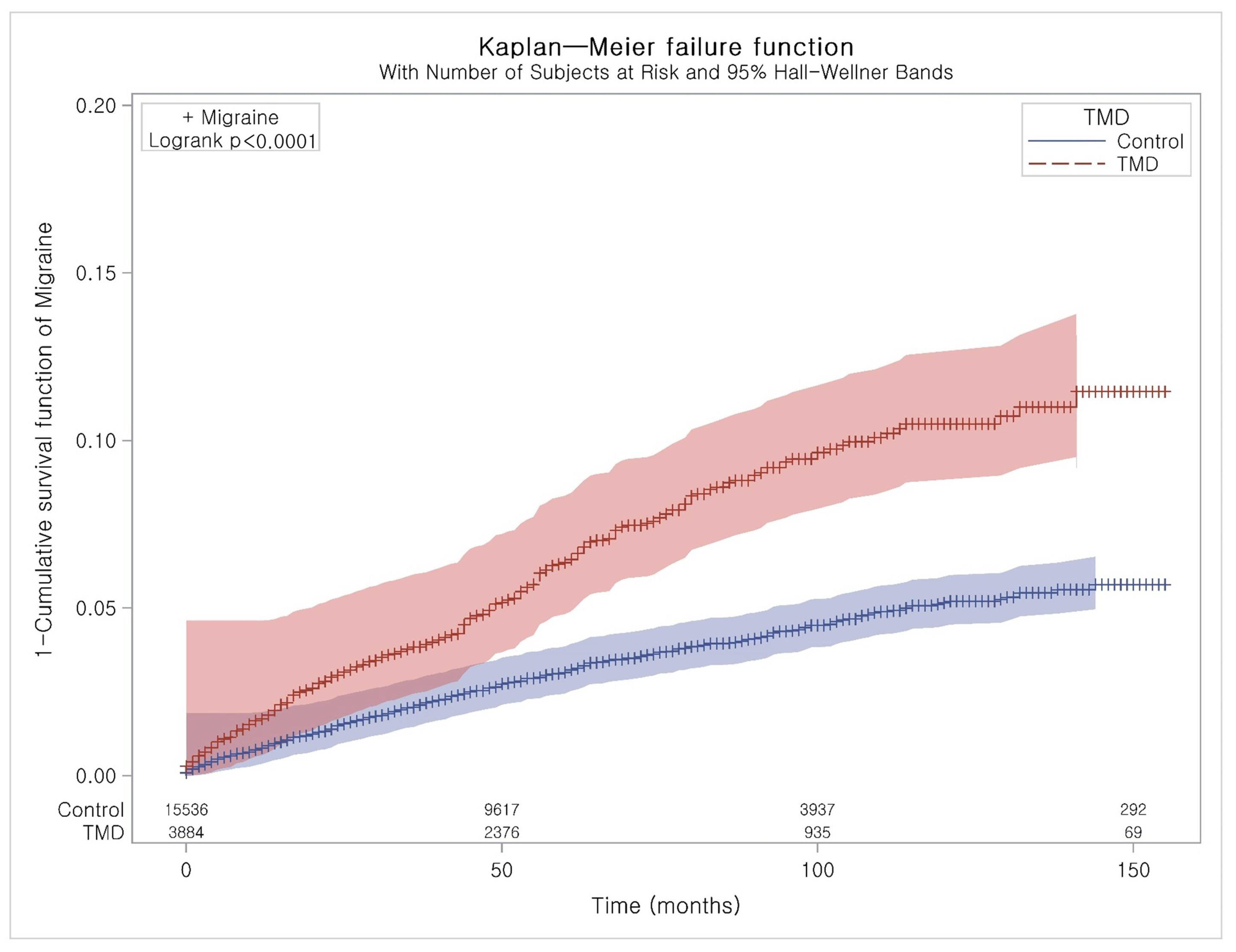
2.6. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Fernandes, G.; Franco, A.L.; Siqueira, J.T.T.; Gonçalves, D.A.D.G.; Camparis, C.M. Sleep bruxism increases the risk for painful temporomandibular disorder, depression and non-specific physical symptoms. J. Oral Rehabil. 2012, 39, 538–544. [Google Scholar] [CrossRef] [PubMed]
- Ramírez, L.M.; Ballesteros, L.E.; Sandoval, G.P. [Otological symptoms among patients with temporomandibular joint disorders]. Rev. Médica Chile 2008, 135, 1582–1590. [Google Scholar]
- Kang, J.-H. Effects on migraine, neck pain, and head and neck posture, of temporomandibular disorder treatment: Study of a retrospective cohort. Arch. Oral Boil. 2020, 114, 104718. [Google Scholar] [CrossRef] [PubMed]
- Motghare, V.; Kumar, J.; Kamate, S.; Kushwaha, S.; Anand, R.; Gupta, N.; Gupta, B.; Singh, I. Association Between Harmful Oral Habits and Sign and Symptoms of Temporomandibular Joint Disorders Among Adolescents. J. Clin. Diagn. Res. 2015, 9, ZC45–ZC48. [Google Scholar] [CrossRef]
- Chaudhari, P.K.; Verma, S.K.; Maheshwari, S. Etiological factors of temporomandibular joint disorders. Natl. J. Maxillofac. Surg. 2012, 3, 238–239. [Google Scholar] [CrossRef] [Green Version]
- Okeson, J.P. Temporomandibular disorders in children. Pediatr. Dent. 1989, 11, 325–329. [Google Scholar]
- Christidis, N.; Ndanshau, E.L.; Sandberg, A.; Tsilingaridis, G. Prevalence and treatment strategies regarding temporomandibular disorders in children and adolescents—A systematic review. J. Oral Rehabil. 2019, 46, 291–301. [Google Scholar] [CrossRef]
- Graff-Radford, S.B. Temporomandibular Disorders and Headache. Dent. Clin. North Am. 2007, 51, 129–144. [Google Scholar] [CrossRef]
- Vgontzas, A.; Burch, R. Episodic Migraine With and Without Aura: Key Differences and Implications for Pathophysiology, Management, and Assessing Risks. Curr. Pain Headache Rep. 2018, 22, 78. [Google Scholar] [CrossRef]
- Olesen, J.D. International Classification of Headache Disorders. Lancet Neurol. 2018, 17, 396–397. [Google Scholar] [CrossRef] [Green Version]
- Buse, D.C.; Loder, E.W.; Gorman, J.A.; Stewart, W.F.; Reed, M.L.; Fanning, K.M.; Serrano, D.; Lipton, R.B. Sex Differences in the Prevalence, Symptoms, and Associated Features of Migraine, Probable Migraine and Other Severe Headache: Results of the American Migraine Prevalence and Prevention (AMPP) Study. Headache J. Head Face Pain 2013, 53, 1278–1299. [Google Scholar] [CrossRef] [PubMed]
- Krivánek, J. Spreading cortical depression and acetylcholinesterase activity in rat cerebral cortex. Physiol. Bohemoslov. 1972, 21, 163–169. [Google Scholar] [PubMed]
- Sugaya, E.; Takato, M.; Noda, Y. Neuronal and glial activity during spreading depression in cerebral cortex of cat. J. Neurophysiol. 1975, 38, 822–841. [Google Scholar] [CrossRef] [PubMed]
- Shinohara, M.; Dollinger, B.; Brown, G.; Rapoport, S.; Sokoloff, L. Cerebral glucose utilization: Local changes during and after recovery from spreading cortical depression. Science 1979, 203, 188–190. [Google Scholar] [CrossRef] [PubMed]
- Hansen, J.M.; Charles, A.C. Differences in treatment response between migraine with aura and migraine without aura: Lessons from clinical practice and RCTs. J. Headache Pain 2019, 20, 96. [Google Scholar] [CrossRef] [Green Version]
- Giordano, J.; Schatman, M.E. A crisis in chronic pain care: An ethical analysis. Part three: Toward an integrative, multi-disciplinary pain medicine built around the needs of the patient. Pain Physician 2008, 11, 775–784. [Google Scholar]
- De Leeuw, R.; Klasser, G.D.; Albuquerque, R.J. Are female patients with orofacial pain medically compromised? J. Am. Dent. Assoc. 2005, 136, 459–468. [Google Scholar] [CrossRef]
- Lim, P.F.; Maixner, W.; Khan, A.A. Temporomandibular disorder and comorbid pain conditions. J. Am. Dent. Assoc. 2011, 142, 1365–1367. [Google Scholar] [CrossRef] [Green Version]
- Fernández-De-Las-Peñas, C.; Galán-Del-Río, F.; Fernández-Carnero, J.; Pesquera, J.; Arendt-Nielsen, L.; Svensson, P. Bilateral Widespread Mechanical Pain Sensitivity in Women with Myofascial Temporomandibular Disorder: Evidence of Impairment in Central Nociceptive Processing. J. Pain 2009, 10, 1170–1178. [Google Scholar] [CrossRef]
- Popescu, A.; LeResche, L.; Truelove, E.L.; Drangsholt, M.T. Gender differences in pain modulation by diffuse noxious inhibitory controls: A systematic review. Pain 2010, 150, 309–318. [Google Scholar] [CrossRef]
- Velly, A.M.; Look, J.O.; Carlson, C.; Lenton, P.A.; Kang, W.; Holcroft, C.A.; Fricton, J.R. The effect of catastrophizing and depression on chronic pain—A prospective cohort study of temporomandibular muscle and joint pain disorders. Pain 2011, 152, 2377–2383. [Google Scholar] [CrossRef] [PubMed]
- Mercuri, L.G. Temporomandibular Joint Disorder Management in Oral and Maxillofacial Surgery. J. Oral Maxillofac. Surg. 2017, 75, 927–930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonçalves, D.A.D.G.; Camparis, C.M.; Speciali, J.G.; Franco, A.L.; Castanharo, S.M.; Bigal, M.E. Temporomandibular Disorders Are Differentially Associated with Headache Diagnoses. Clin. J. Pain 2011, 27, 611–615. [Google Scholar] [CrossRef] [PubMed]
- Speciali, J.G.; Dach, F. Temporomandibular Dysfunction and Headache Disorder. Headache J. Head Face Pain 2015, 55, 72–83. [Google Scholar] [CrossRef] [PubMed]
- Gil-Martínez, C.C.-L.A.; Navarro-Fernández, G.; Mangas-Guijarro, M.Á.; Lara-Lara, M.; López-López, A.; Fernández-Carnero, J.; La Touche, R. Comparison Between Chronic Migraine and Temporomandibular Disorders in Pain-Related Disability and Fear-Avoidance Behaviors. Pain Med. 2017, 18, 2214–2223. [Google Scholar] [CrossRef] [Green Version]
- Florencio, L.L.; Oliveira, A.S.; Carvalho, G.F.; Dach, F.; Bigal, M.E.; Fernández-De-Las-Peñas, C.; Grossi, D.B. Association between Severity of Temporomandibular Disorders and the Frequency of Headache Attacks in Women with Migraine: A Cross-Sectional Study. J. Manip. Physiol. Ther. 2017, 40, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Cady, R.; Schreiber, C.; Farmer, K.; Sheftell, F. Primary Headaches: A Convergence Hypothesis. Headache J. Head Face Pain 2002, 42, 204–216. [Google Scholar] [CrossRef]
- Graff-Radford, S.B. Headache problems that can present as toothache. Dent. Clin. North. Am. 1991, 35, 155–170. [Google Scholar]
- Kaniecki, R.G. Migraine and tension-type headache: An assessment of challenges in diagnosis. Neurology 2002, 58, S15–S20. [Google Scholar] [CrossRef]
- Gonçalves, D.A.D.G.; Bigal, M.E.; Jales, L.C.; Camparis, C.M.; Speciali, J.G. Headache and Symptoms of Temporomandibular Disorder: An Epidemiological Study. Headache J. Head Face Pain 2010, 50, 231–241. [Google Scholar] [CrossRef]
- Kim, S.Y.; Min, C.; Oh, D.J.; Choi, H.-G. Tobacco Smoking and Alcohol Consumption Are Related to Benign Parotid Tumor: A Nested Case-Control Study Using a National Health Screening Cohort. Clin. Exp. Otorhinolaryngol. 2019, 12, 412–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, J.L.; Cho, J.J.; Park, K.M.; Noh, H.-M.; Park, Y. Diagnostic Performance of Body Mass Index Using the Western Pacific Regional Office of World Health Organization Reference Standards for Body Fat Percentage. J. Korean Med. Sci. 2015, 30, 162–166. [Google Scholar] [CrossRef] [PubMed]
- Anuurad, E.; Shiwaku, K.; Nogi, A.; Kitajima, K.; Enkhmaa, B.; Shimono, K.; Yamane, Y. The New BMI Criteria for Asians by the Regional Office for the Western Pacific Region of WHO are Suitable for Screening of Overweight to Prevent Metabolic Syndrome in Elder Japanese Workers. J. Occup. Health 2003, 45, 335–343. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.G.; Min, C.; Lee, C.H.; Kim, S.Y. The Relation of Sudden Sensorineural Hearing Loss in Pediatric Patients With Recurrent Otitis Media. Otol. Neurotol. 2020, 41, 836. [Google Scholar] [CrossRef]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.-M.; Sundararajan, V. Updating and Validating the Charlson Comorbidity Index and Score for Risk Adjustment in Hospital Discharge Abstracts Using Data From 6 Countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Marklund, S.; Wiesinger, B.; Wänman, A. Reciprocal influence on the incidence of symptoms in trigeminally and spinally innervated areas. Eur. J. Pain 2010, 14, 366–371. [Google Scholar] [CrossRef]
- Lim, P.F.; Smith, S.B.; Bhalang, K.; Slade, G.D.; Maixner, W. Development of Temporomandibular Disorders Is Associated With Greater Bodily Pain Experience. Clin. J. Pain 2010, 26, 116–120. [Google Scholar] [CrossRef] [Green Version]
- Grossi, D.B.; Lipton, R.; Napchan, U.; Grosberg, B.; Ashina, S.; Bigal, M. Temporomandibular disorders and cutaneous allodynia are associated in individuals with migraine. Cephalalgia 2009, 30, 425–432. [Google Scholar] [CrossRef]
- Manfredini, D.; Winocur, E.; Guarda-Nardini, L.; Paesani, D.; Lobbezoo, F. Epidemiology of bruxism in adults: A systematic review of the literature. J. Orofac. Pain 2013, 27, 99–110. [Google Scholar] [CrossRef] [Green Version]
- Didier, H.A.; Marchetti, A.; Giannì, A.B.; Tullo, V.; Di Fiore, P.; Peccarisi, C.; D’Amico, D.; Bussone, G.; Marchetti, C. Study of parafunctions in patients with chronic migraine. Neurol. Sci. 2014, 35, 199–202. [Google Scholar] [CrossRef]
- Boening, K.; Wieckiewicz, M.; Paradowska-Stolarz, A.; Wiland, P.; Shiau, Y.-Y. Temporomandibular Disorders and Oral Parafunctions: Mechanism, Diagnostics, and Therapy. BioMed Res. Int. 2015, 2015, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Paparo, F.; Fatone, F.M.G.; Ramieri, V.; Cascone, P. Anatomic relationship between trigeminal nerve and temporomandibular joint. Eur. Rev. Med. Pharmacol. Sci. 2008, 12, 15–18. [Google Scholar] [PubMed]
- Olesen, J.D. Clinical and pathophysiological observations in migraine and tension-type headache explained by integration of vascular, supraspinal and myofascial inputs. Pain 1991, 46, 125–132. [Google Scholar] [CrossRef]
- Plesh, O.; Noonan, C.; Buchwald, D.; Goldberg, J.; Afari, N. Temporomandibular disorder-type pain and migraine headache in women: A preliminary twin study. J. Orofac. Pain 2012, 26, 91–98. [Google Scholar] [PubMed]
- Gupta, S.; McCarson, K.E.; Welch, K.; Berman, N.E. Mechanisms of Pain Modulation by Sex Hormones in Migraine. Headache J. Head Face Pain 2011, 51, 905–922. [Google Scholar] [CrossRef] [PubMed]
- Sauro, K.M.; Becker, W.J. The Stress and Migraine Interaction. Headache J. Head Face Pain 2009, 49, 1378–1386. [Google Scholar] [CrossRef]
- Wright, E.F.; Clark, E.G.; Paunovich, E.D.; Hart, R.G. Headache Improvement through TMD Stabilization Appliance and Self-management Therapies. CRANIO® 2006, 24, 104–111. [Google Scholar] [CrossRef]
- Ekberg, E.; Vallon, D.; Nilner, M. Treatment outcome of headache after occlusal appliance therapy in a randomised controlled trial among patients with temporomandibular disorders of mainly arthrogenous origin. Swed. Dent. J. 2002, 26, 115–124. [Google Scholar]
- Fernandes, G.; Arruda, M.A.; Bigal, M.E.; Camparis, C.M.; Gonçalves, D.A.D.G. Painful Temporomandibular Disorder Is Associated With Migraine in Adolescents: A Case-Control Study. J. Pain 2019, 20, 1155–1163. [Google Scholar] [CrossRef]
- Monticone, M.; Rocca, B.; Abelli, P.; Tecco, S.; Geri, T.; Gherlone, E.F.; Luzzi, D.; Testa, M. Cross-cultural adaptation, reliability and validity of the Italian version of the craniofacial pain and disability inventory in patients with chronic temporomandibular joint disorders. BMC Oral Health 2019, 19, 244. [Google Scholar] [CrossRef] [Green Version]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.-P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group†. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Total Participants | ||
|---|---|---|---|
| TMD (n, %) | Control (n, %) | p-Value | |
| Age (years old) | 1.000 | ||
| 40–44 | 128 (3.3) | 512 (3.3) | |
| 45–49 | 403 (10.4) | 1612 (10.4) | |
| 50–54 | 626 (16.1) | 2504 (16.1) | |
| 55–59 | 629 (16.2) | 2516 (16.2) | |
| 60–64 | 538 (13.9) | 2152 (13.9) | |
| 65–69 | 595 (15.3) | 2380 (15.3) | |
| 70–74 | 512 (13.2) | 2048 (13.2) | |
| 75–79 | 319 (8.2) | 1276 (8.2) | |
| 80–84 | 107 (2.8) | 428 (2.8) | |
| 85+ | 27 (0.7) | 108 (0.7) | |
| Sex | 1.000 | ||
| Male | 1753 (45.1) | 7012 (45.1) | |
| Female | 2131 (54.9) | 8524 (54.9) | |
| Income | 1.000 | ||
| 1 (lowest) | 598 (15.4) | 2392 (15.4) | |
| 2 | 505 (13.0) | 2020 (13.0) | |
| 3 | 626 (16.1) | 2504 (16.1) | |
| 4 | 800 (20.6) | 3200 (20.6) | |
| 5 (highest) | 1355 (34.9) | 5420 (34.9) | |
| Region of residence | 1.000 | ||
| Urban | 1908 (40.1) | 7632 (40.1) | |
| Rural | 2850 (59.9) | 11,400 (59.9) | |
| Obesity † | |||
| Underweight | 112 (2.9) | 385 (2.5) | <0.001 * |
| Normal | 1530 (39.4) | 5601 (36.1) | |
| Overweight | 1104 (28.4) | 4171 (26.9) | |
| Obese I | 1056 (27.2) | 4885 (31.4) | |
| Obese II | 82 (2.1) | 494 (3.2) | |
| Smoking status | <0.001 * | ||
| Non-smoker | 2923 (75.3) | 11443 (73.7) | |
| Past smoker | 485 (12.5) | 1738 (11.2) | |
| Current smoker | 476 (12.3) | 2355 (15.2) | |
| Alcohol consumption | 0.754 | ||
| <1 time a week | 2733 (70.4) | 10,892 (70.1) | |
| ≥1 time a week | 1151 (29.6) | 4644 (29.9) | |
| Systolic blood pressure | <0.001 * | ||
| <120 mmHg | 1292 (33.3) | 4704 (30.3) | |
| 120–139 mmHg | 1882 (48.5) | 7508 (48.3) | |
| ≥140 mmHg | 710 (18.3) | 3324 (21.4) | |
| Diastolic blood pressure | <0.001 * | ||
| <80 mmHg | 1964 (50.6) | 7306 (47.0) | |
| 80–89 mmHg | 1355 (34.9) | 5540 (35.7) | |
| ≥90 mmHg | 565 (14.6) | 2690 (17.3) | |
| Fasting blood glucose | 0.001 * | ||
| <100 mg/dL | 2540 (65.4) | 9787 (63.0) | |
| 100–125 mg/dL | 1044 (26.9) | 4297 (27.7) | |
| ≥126 mg/dL | 300 (7.7) | 1452 (9.4) | |
| Total cholesterol | 0.097 | ||
| <200 mg/dL | 2108 (54.3) | 8288 (53.4) | |
| 200–239 mg/dL | 1294 (33.3) | 5115 (32.9) | |
| ≥240 mg/dL | 482 (12.4) | 2133 (13.7) | |
| CCI score | 0.138 | ||
| 0 | 2630 (67.7) | 10,594 (68.2) | |
| 1 | 582 (15.0) | 2254 (14.5) | |
| 2 | 337 (8.7) | 1206 (7.8) | |
| 3 | 149 (3.8) | 633 (4.1) | |
| ≥4 | 186 (4.8) | 849 (5.5) | |
| Migraine with/without aura | 263 (6.8) | 507 (3.3) | <0.001 * |
| Migraine without aura | 253 (6.5) | 476 (3.1) | <0.001 * |
| Migraine with aura | 10 (0.3) | 31 (0.2) | 0.482 |
| Characteristics | Hazard Ratios for Migraine | |||
|---|---|---|---|---|
| Crude † | p-Value | Adjusted †,‡ | p-Value | |
| Total participants (n = 19,420) | ||||
| TMD | 2.12 (1.83–2.46) | <0.001 * | 2.10 (1.81–2.44) | <0.001 * |
| Control | 1.00 | 1.00 | ||
| Age < 60 years old, men (n = 4040) | ||||
| TMD | 2.07 (1.34–3.19) | 0.001 * | 2.03 (1.31–3.14) | 0.002 * |
| Control | 1.00 | 1.00 | ||
| Age < 60 years old, women (n = 4890) | ||||
| TMD | 1.92 (1.49–2.48) | <0.001 * | 1.88 (1.46–2.44) | <0.001 * |
| Control | 1.00 | 1.00 | ||
| Age ≥ 60 years old, men (n = 4725) | ||||
| TMD | 2.24 (1.55–3.22) | <0.001 * | 2.29 (1.58–3.31) | <0.001 * |
| Control | 1.00 | 1.00 | ||
| Age ≥ 60 years old, women (n = 5765) | ||||
| TMD | 2.30 (1.80–2.93) | <0.001 * | 2.28 (1.78–2.91) | <0.001 * |
| Control | 1.00 | 1.00 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Byun, S.-H.; Min, C.; Yoo, D.-M.; Yang, B.-E.; Choi, H.-G. Increased Risk of Migraine in Patients with Temporomandibular Disorder: A Longitudinal Follow-Up Study Using a National Health Screening Cohort. Diagnostics 2020, 10, 724. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10090724
Byun S-H, Min C, Yoo D-M, Yang B-E, Choi H-G. Increased Risk of Migraine in Patients with Temporomandibular Disorder: A Longitudinal Follow-Up Study Using a National Health Screening Cohort. Diagnostics. 2020; 10(9):724. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10090724
Chicago/Turabian StyleByun, Soo-Hwan, Chanyang Min, Dae-Myoung Yoo, Byoung-Eun Yang, and Hyo-Geun Choi. 2020. "Increased Risk of Migraine in Patients with Temporomandibular Disorder: A Longitudinal Follow-Up Study Using a National Health Screening Cohort" Diagnostics 10, no. 9: 724. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10090724