Asphericity of Somatostatin Receptor Expression in Neuroendocrine Tumors: An Innovative Predictor of Outcome in Everolimus Treatment?

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. Everolimus
2.3. SPECT/CT Imaging
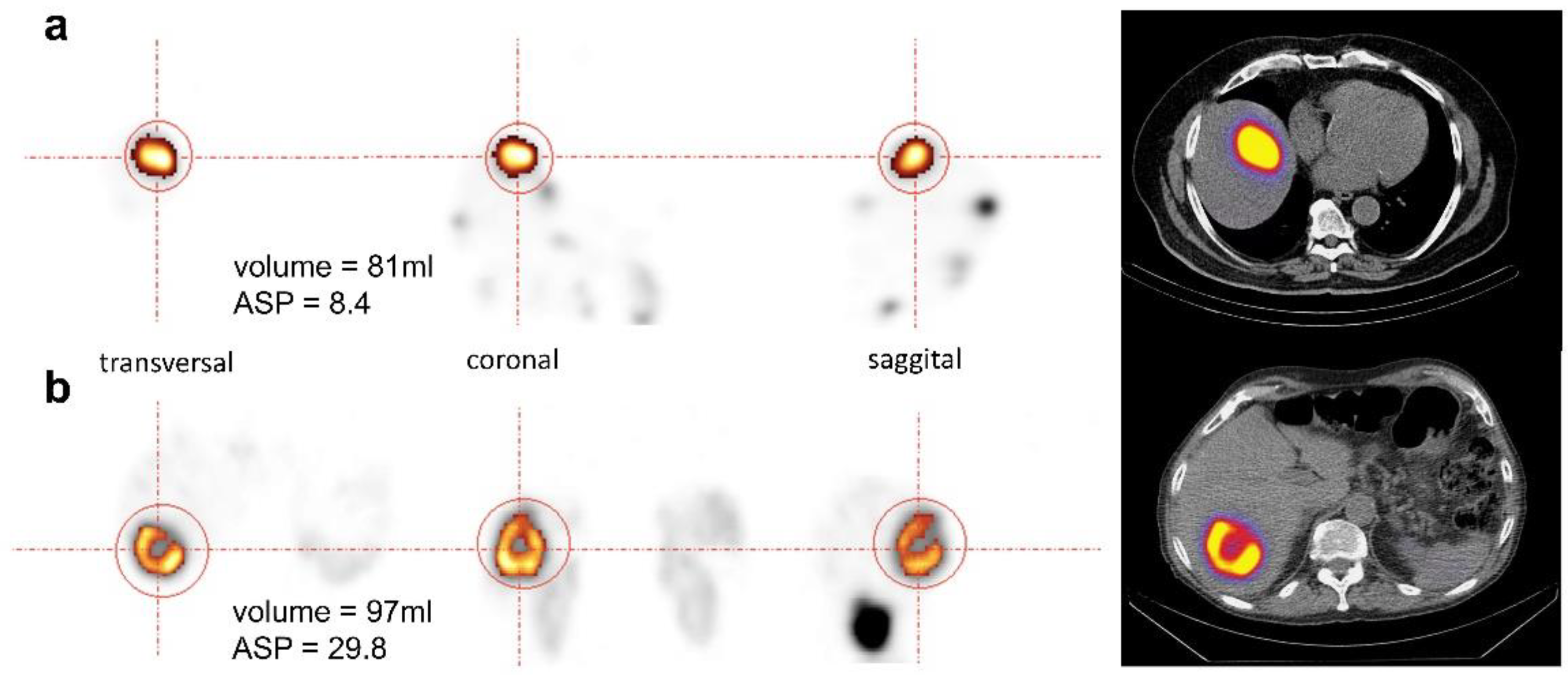
2.4. Image Analysis
2.5. Statistical Analysis
3. Results
3.1. Patient and Tumor Characteristics
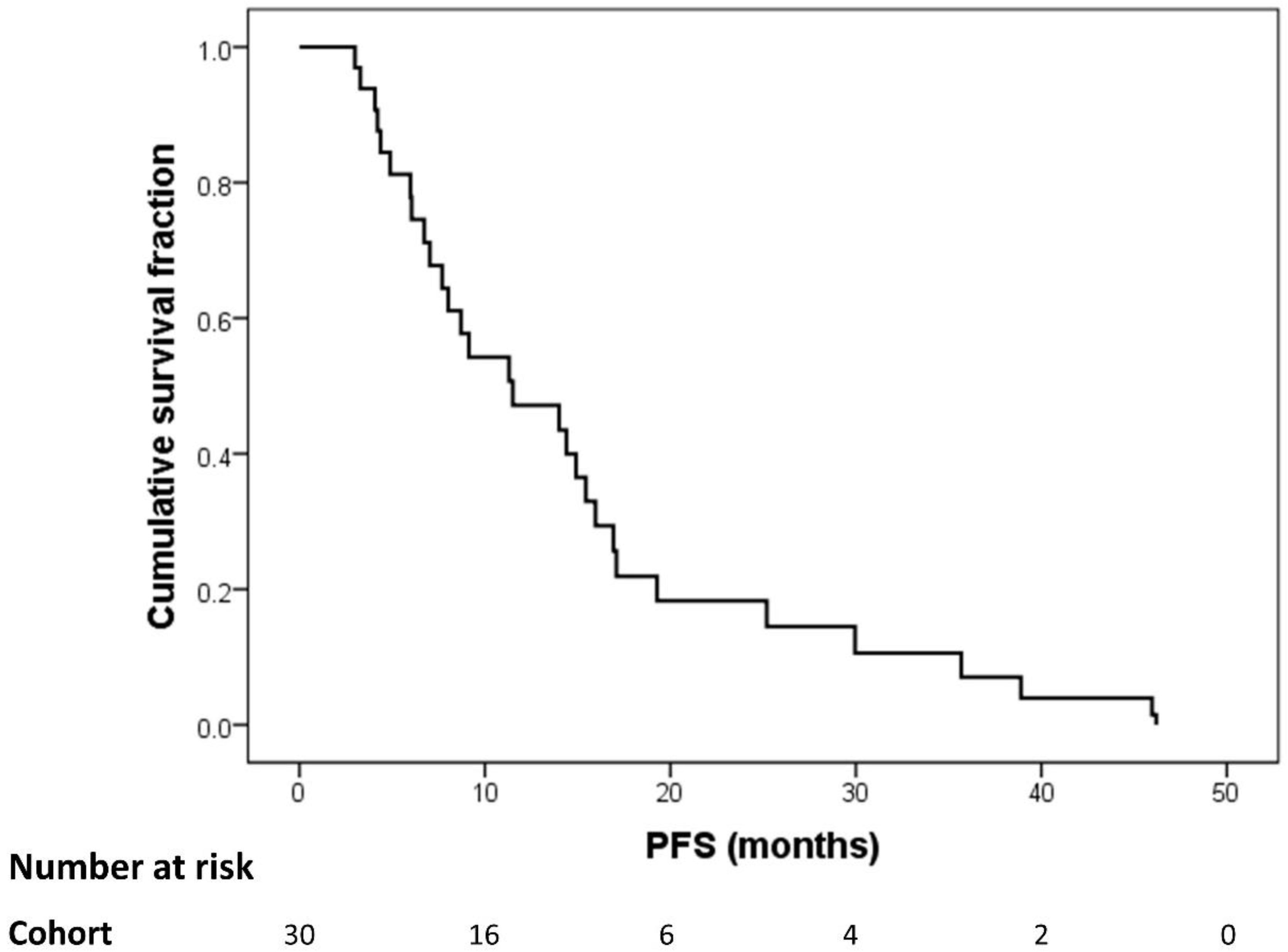
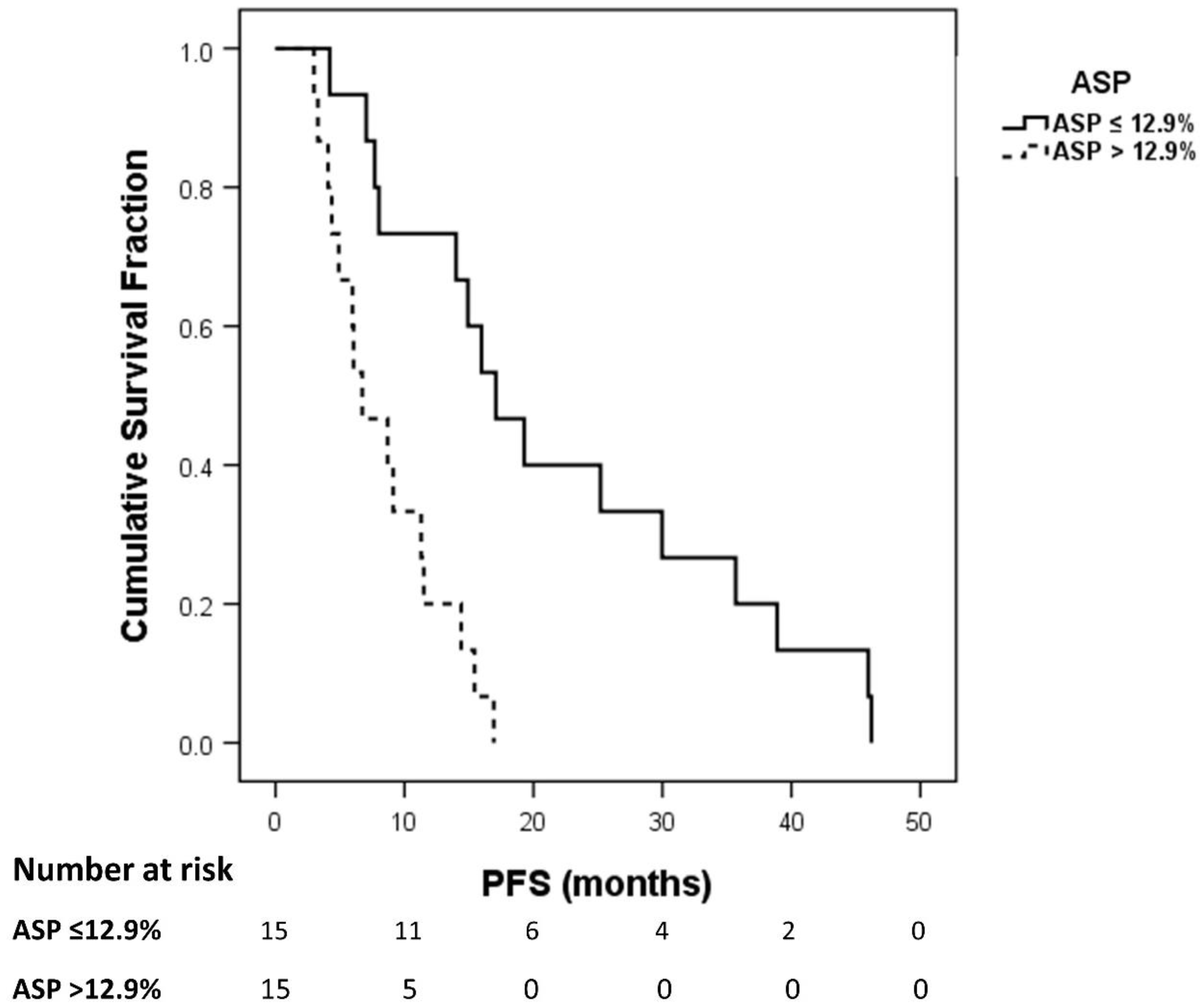
3.2. Progression-Free Survival Analysis
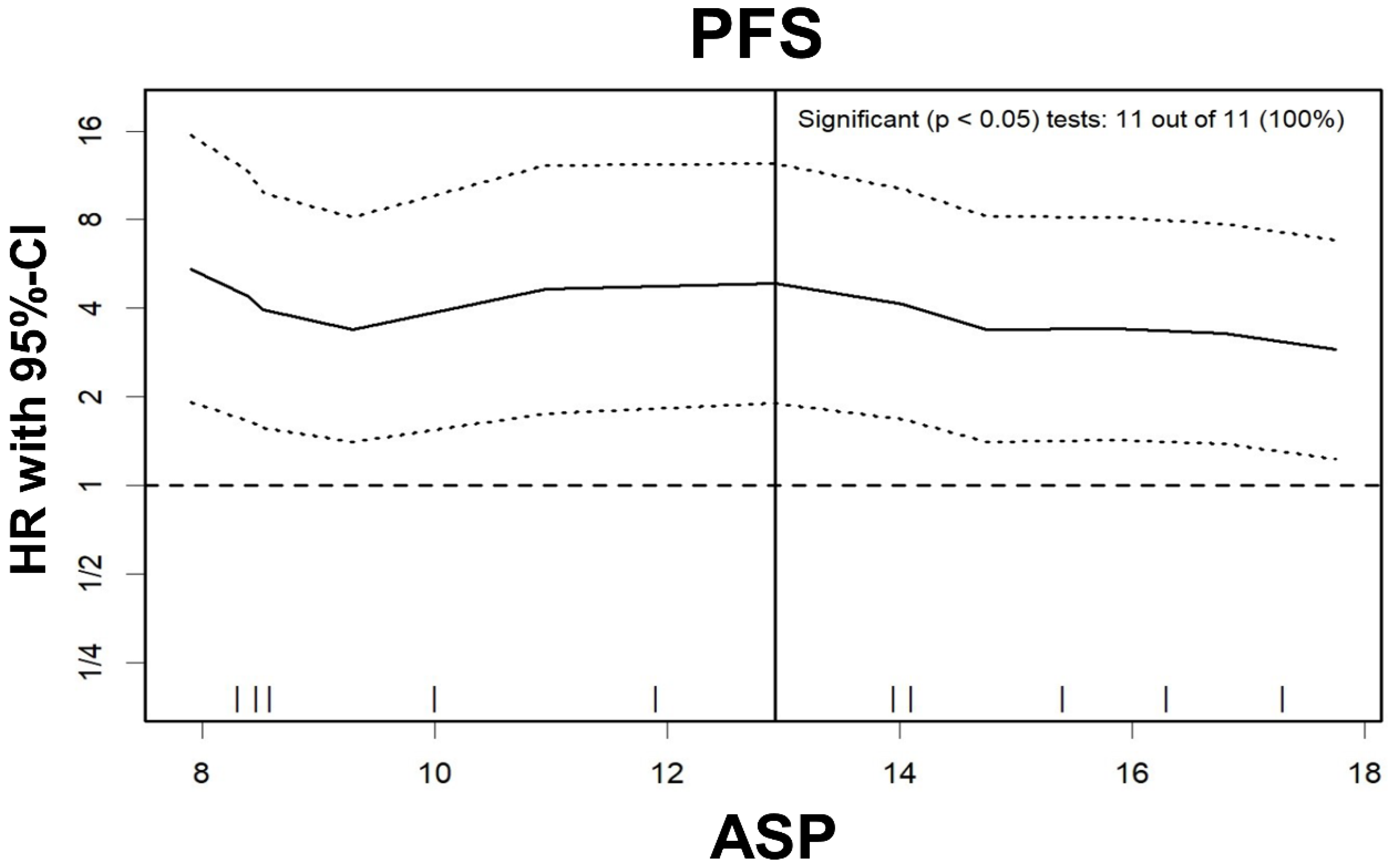
3.3. Cox Regression for PFS
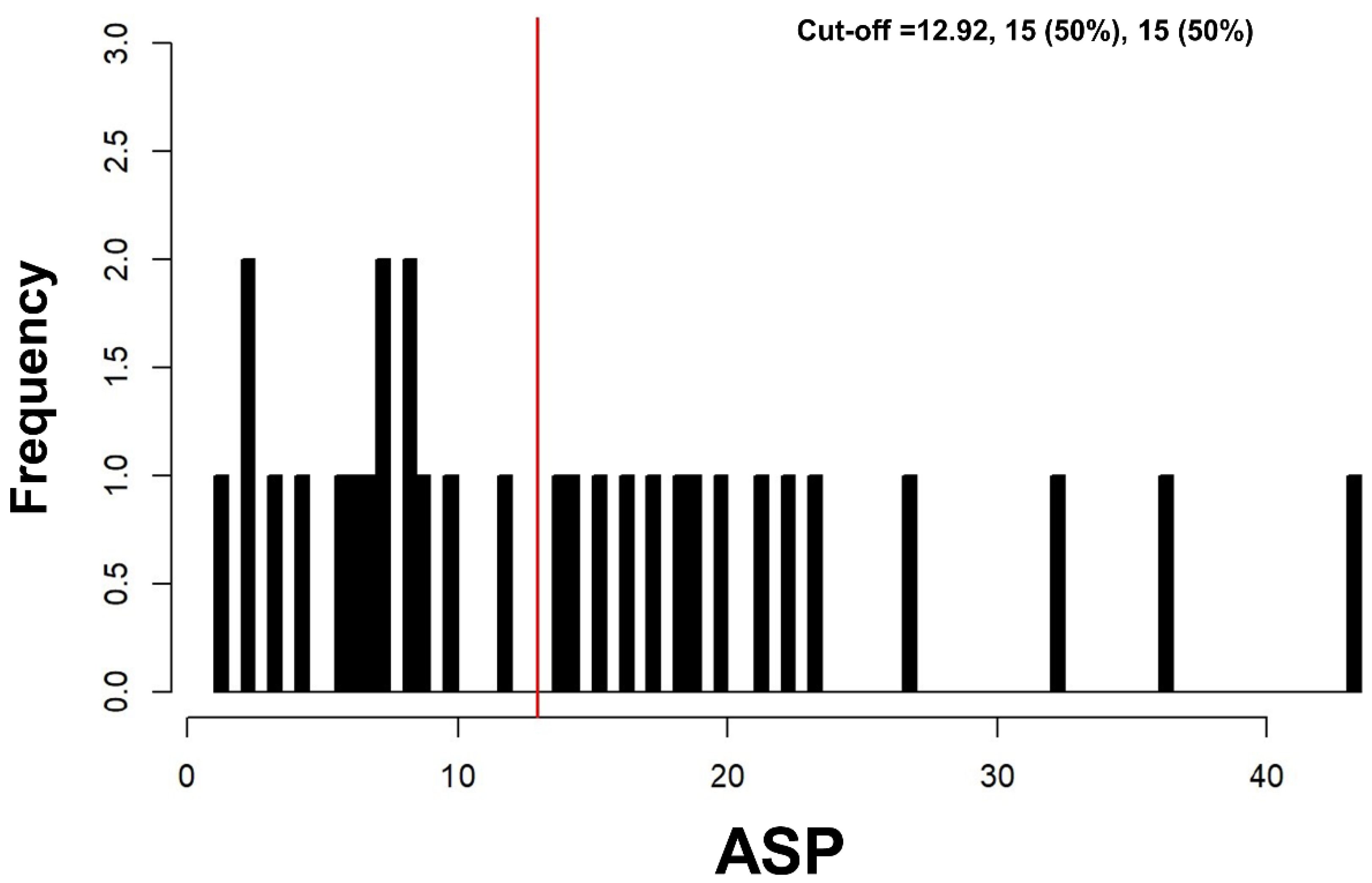
3.4. Prediction of PFS
4. Discussion
5. Conclusion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hallet, J.; Law, C.H.L.; Cukier, M.; Saskin, R.; Liu, N.; Singh, S. Exploring the rising incidence of neuroendocrine tumors: A population-based analysis of epidemiology, metastatic presentation, and outcomes. Cancer 2015, 121, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Dasari, A.; Shen, C.; Halperin, D.; Zhao, B.; Zhou, S.; Xu, Y.; Shih, T.; Yao, J.C. Trends in the Incidence, Prevalence, and Survival Outcomes in Patients With Neuroendocrine Tumors in the United States. JAMA Oncol. 2017, 3, 1335–1342. [Google Scholar] [CrossRef] [PubMed]
- Pavel, M.E.; Hainsworth, J.D.; Baudin, E.; Peeters, M.; Hörsch, D.; Winkler, R.E.; Klimovsky, J.; Lebwohl, D.; Jehl, V.; Wolin, E.M. Everolimus plus octreotide long-acting repeatable for the treatment of advanced neuroendocrine tumours associated with carcinoid syndrome (RADIANT-2): A randomised, placebo-controlled, phase 3 study. Lancet 2011, 378, 2005–2012. [Google Scholar] [CrossRef]
- Yao, J.C.; Shah, M.H.; Ito, T.; Bohas, C.L.; Wolin, E.M.; Van Cutsem, E.; Hobday, T.J.; Okusaka, T.; Capdevila, J.; De Vries, E.G. Everolimus for advanced pancreatic neuroendocrine tumors. N. Engl. J. Med. 2011, 364, 514–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, J.C.; Fazio, N.; Singh, S.; Buzzoni, R.; Carnaghi, C.; Wolin, E.; Tomasek, J.; Raderer, M.; Lahner, H.; Voi, M. Everolimus for the treatment of advanced, non-functional neuroendocrine tumours of the lung or gastrointestinal tract (RADIANT-4): A randomised, placebo-controlled, phase 3 study. Lancet 2016, 387, 968–977. [Google Scholar] [CrossRef]
- Yao, J.C.; Lombard-Bohas, C.; Baudin, E.; Kvols, L.K.; Rougier, P.; Ruszniewski, P.; Hoosen, S.; Peter, J.S.; Haas, T.; Lebwohl, D. Daily oral everolimus activity in patients with metastatic pancreatic neuroendocrine tumors after failure of cytotoxic chemotherapy: A phase II trial. J. Clin. Oncol. 2010, 28, 69. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.C.; Phan, A.T.; Chang, D.Z.; Wolff, R.A.; Hess, K.; Gupta, S.; Jacobs, C.; Mares, J.E.; Landgraf, A.N.; Rashid, A. Efficacy of RAD001 (everolimus) and octreotide LAR in advanced low-to intermediate-grade neuroendocrine tumors: Results of a phase II study. J. Clin. Oncol. 2008, 26, 4311–4318. [Google Scholar] [CrossRef]
- Pavel, M.; O’’Toole, D.; Costa, F.; Capdevila, J.; Gross, D.; Kianmanesh, R.; Krenning, E.; Knigge, U.; Salazar, R.; Pape, U.F.; et al. ENETS Consensus Guidelines Update for the Management of Distant Metastatic Disease of Intestinal, Pancreatic, Bronchial Neuroendocrine Neoplasms (NEN) and NEN of Unknown Primary Site. Neuroendocrinology 2016, 103, 172–185. [Google Scholar] [CrossRef]
- Wetz, C.; Apostolova, I.; Steffen, I.; Hofheinz, F.; Furth, C.; Kupitz, D.; Ruf, J.; Venerito, M.; Klose, S.; Amthauer, H. Predictive Value of Asphericity in Pretherapeutic [111In] DTPA-Octreotide SPECT/CT for Response to Peptide Receptor Radionuclide Therapy with [177Lu] DOTATATE. Mol. Imaging Biol. 2017, 19, 437–445. [Google Scholar] [CrossRef]
- Wetz, C.; Genseke, P.; Apostolova, I.; Furth, C.; Ghazzawi, S.; Rogasch, J.M.; Schatka, I.; Kreissl, M.C.; Hofheinz, F.; Grosser, O.S. The association of intra-therapeutic heterogeneity of somatostatin receptor expression with morphological treatment response in patients undergoing PRRT with [177Lu]-DOTATATE. PLoS ONE 2019, 14, e0216781. [Google Scholar] [CrossRef]
- Faes, S.; Santoro, T.; Demartines, N.; Dormond, O. Evolving Significance and Future Relevance of Anti-Angiogenic Activity of mTOR Inhibitors in Cancer Therapy. Cancers 2017, 9, 152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwekkeboom, D.J.; Teunissen, J.J.; Bakker, W.H.; Kooij, P.P.; de Herder, W.W.; Feelders, R.A.; van Eijck, C.H.; Esser, J.-P.; Kam, B.L.; Krenning, E.P. Radiolabeled somatostatin analog [177Lu-DOTA0, Tyr3] octreotate in patients with endocrine gastroenteropancreatic tumors. J. Clin. Oncol. 2005, 23, 2754–2762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hofheinz, F.; Langner, J.; Petr, J.; Beuthien-Baumann, B.; Steinbach, J.; Kotzerke, J.; van den Hoff, J. An automatic method for accurate volume delineation of heterogeneous tumors in PET. Med. Phys. 2013, 40, 082503. [Google Scholar] [CrossRef] [PubMed]
- Hofheinz, F.; Pötzsch, C.; Oehme, L.; Beuthien-Baumann, B.; Steinbach, J.; Kotzerke, J.; van den Hoff, J. Automatic volume delineation in oncological PET. Nuklearmedizin 2012, 51, 9–16. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Budczies, J.; Klauschen, F.; Sinn, B.V.; Győrffy, B.; Schmitt, W.D.; Darb-Esfahani, S.; Denkert, C. Cutoff Finder: A comprehensive and straightforward Web application enabling rapid biomarker cutoff optimization. PLoS ONE 2012, 7, e51862. [Google Scholar] [CrossRef] [Green Version]
- Van Asselt, S.J.; Oosting, S.F.; Brouwers, A.H.; Bongaerts, A.H.; de Jong, J.R.; Lub-de Hooge, M.N.; Munnink, T.H.O.; Fiebrich, H.-B.; Sluiter, W.J.; Links, T.P. Everolimus reduces 89Zr-bevacizumab tumor uptake in patients with neuroendocrine tumors. J. Nucl. Med. 2014, 55, 1087–1092. [Google Scholar] [CrossRef] [Green Version]
- Martins, D.; Spada, F.; Lambrescu, I.; Rubino, M.; Cella, C.; Gibelli, B.; Grana, C.; Ribero, D.; Bertani, E.; Ravizza, D.; et al. Predictive Markers of Response to Everolimus and Sunitinib in Neuroendocrine Tumors. Target. Oncol. 2017, 12, 611–622. [Google Scholar] [CrossRef]
- Yao, J.C.; Pavel, M.; Phan, A.T.; Kulke, M.H.; Hoosen, S.; St. Peter, J.; Cherfi, A.; Öberg, K.E. Chromogranin A and neuron-specific enolase as prognostic markers in patients with advanced pNET treated with everolimus. J. Clin. Endocrinol. Metab. 2011, 96, 3741–3749. [Google Scholar] [CrossRef] [Green Version]
- Benslama, N.; Bollard, J.; Vercherat, C.; Massoma, P.; Roche, C.; Hervieu, V.; Peron, J.; Lombard-Bohas, C.; Scoazec, J.-Y.; Walter, T. Prediction of response to everolimus in neuroendocrine tumors: Evaluation of clinical, biological and histological factors. Investig. New Drugs 2016, 34, 654–662. [Google Scholar] [CrossRef]
- Owonikoko, T.K.; Khuri, F.R. Targeting the PI3K/AKT/mTOR pathway: Biomarkers of success and tribulation. Am. Soc. Clin. Oncol. Educ. Book 2013, 33, e395–e401. [Google Scholar] [CrossRef] [PubMed]
- Azar, R.; Najib, S.; Lahlou, H.; Susini, C.; Pyronnet, S. Phosphatidylinositol 3-kinase-dependent transcriptional silencing of the translational repressor 4E-BP1. Cell. Mol. Life Sci. 2008, 65, 3110–3117. [Google Scholar] [CrossRef] [PubMed]
- Bousquet, C.; Lasfargues, C.; Chalabi, M.; Billah, S.M.; Susini, C.; Vezzosi, D.; Caron, P.; Pyronnet, S. Clinical review: Current scientific rationale for the use of somatostatin analogs and mTOR inhibitors in neuroendocrine tumor therapy. J. Clin. Endocrinol. Metab. 2012, 97, 727–737. [Google Scholar] [CrossRef]
- Proskuryakov, S.Y.; Konoplyannikov, A.G.; Gabai, V.L. Necrosis: A specific form of programmed cell death? Exp. Cell Res. 2003, 283, 1–16. [Google Scholar] [CrossRef]
- Lee, L.; Ito, T.; Jensen, R.T. Everolimus in the treatment of neuroendocrine tumors: Efficacy, side-effects, resistance, and factors affecting its place in the treatment sequence. Expert Opin. Pharmacother. 2018, 19, 909–928. [Google Scholar] [CrossRef]
- Berardi, R.; Torniai, M.; Pusceddu, S.; Spada, F.; Ibrahim, T.; Brizzi, M.P.; Antonuzzo, L.; Ferolla, P.; Panzuto, F.; Silvestris, N.; et al. Prognostic impact of the cumulative dose and dose intensity of everolimus in patients with pancreatic neuroendocrine tumors. Cancer Med. 2017, 6, 1493–1499. [Google Scholar] [CrossRef]
- Singh, S.; Poon, R.; Wong, R.; Metser, U. 68Ga PET imaging in patients with neuroendocrine tumors: A systematic review and meta-analysis. Clin. Nucl. Med. 2018, 43, 802–810. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Variable | Value (%) |
|---|---|---|
| Total | 30 (100) | |
| Sex | female male | 13/30 (43) 17/30 (57) |
| Age in years | median (range) | 67 (48–81) |
| Primary | ||
| pancreatic | 17/30 (57) | |
| duodenum/ileum/jejunum | 9/30 (30) | |
| CUP-NET | 4/30 (13) | |
| Previous treatment | surgery of the primary | 19/30 (63) |
| Liver-directed treatment a | 8/30 (27) | |
| SSA | 27/30 (90) | |
| PRRT | 6/30 (20) | |
| chemotherapy | 7/30 (23) | |
| Number of evaluated liver metastases per patient | ||
| n = 1 (% of patients) | 3 (10) | |
| n = 2 (% of patients) | 10 (33) | |
| n = 3 (% of patients) | 17 (57) | |
| Administered activity, MBq (OctreoScan®) | Median (range) | 222 (181.3–265.5) |
| Ki-67 (%) | Median (range) | 5 (1–25) |
| Grade | ||
| G1 | 9/30 (30) | |
| G2 | 19/30 (63) | |
| G3 | 2/30 (7) | |
| Chromogranin A (µg/L) | Median (range) | 482 (47–45,800) |
| ASP (%) | Median (range) | 12.1 (1.1–43.5) |
| ASP (%) < 12.9 | 6.9 (1.1–11.9) | |
| ASP (%) > 12.9 | 20.0 (14.0–43.5) |
| Variable | HR | 95%-CI | p Value |
|---|---|---|---|
| Patient Variables | |||
| Male sex | 2.03 | 0.91 to 4.5 | 0.082 |
| Age in years (continuous) | 1.0 | 0.96 to 1.04 | 0.93 |
| Primary Tumor Site | |||
| Pancreas | Reference | 0.084 | |
| Small bowel | 0.34 | 0.13 to 0.89 | 0.028 |
| CUP | 0.46 | 0.16 to 1.35 | 0.158 |
| Biological Variables | |||
| Baseline CgA ≥ 2 ULN | 0.9 | 0.38 to 2.14 | 0.811 |
| Ki-67 in % (continuous) | 0.98 | 0.92 to 1.05 | 0.575 |
| ASP in % (continuous) | 1.06 | 1.03 to 1.10 | 0.001 |
| Ki-67 Grading | |||
| G1 | Reference | 0.327 | |
| G2 | 1.06 | 0.48 to 2.33 | 0.887 |
| G3 | 3.22 | 0.67 to 15.5 | 0.144 |
| Clinical Parameters | |||
| Bone metastases | 3.72 | 1.57 to 8.83 | 0.003 |
| Lymph node metastases | 1.29 | 0.54 to 3.05 | 0.568 |
| Number of metastatic sites ≥ 2 | 2.37 | 1.09 to 5.15 | 0.03 |
| Prior Treatment | |||
| Primary tumor surgery | 1.64 | 0.70 to 3.82 | 0.251 |
| Liver-directed treatment | 0.79 | 0.65 to 3.19 | 0.579 |
| SSA | 2.18 | 1.08 to 7.35 | 0.21 |
| PRRT | 0.32 | 0.12 to 0.87 | 0.025 |
| Chemotherapy | 1.86 | 0.77 to 4.48 | 0.167 |
| Variable | HR | 95%-CI | p Value |
|---|---|---|---|
| ASP (>12.9 vs. ≤12.9%) | 3.33 | 1.17 to 9.47 | 0.024 |
| Bone metastases | 1.89 | 0.67 to 5.34 | 0.231 |
| Prior PRRT | 0.35 | 0.12 to 0.97 | 0.043 |
| Primary tumor site | |||
| Pancreas | Reference | 0.855 | |
| Small bowel | 0.79 | 0.27 to 2.30 | 0.664 |
| CUP | 1.03 | 0.34 to 3.12 | 0.954 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wetz, C.; Rogasch, J.; Genseke, P.; Schatka, I.; Furth, C.; Kreissl, M.; Jann, H.; Venerito, M.; Amthauer, H. Asphericity of Somatostatin Receptor Expression in Neuroendocrine Tumors: An Innovative Predictor of Outcome in Everolimus Treatment? Diagnostics 2020, 10, 732. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10090732
Wetz C, Rogasch J, Genseke P, Schatka I, Furth C, Kreissl M, Jann H, Venerito M, Amthauer H. Asphericity of Somatostatin Receptor Expression in Neuroendocrine Tumors: An Innovative Predictor of Outcome in Everolimus Treatment? Diagnostics. 2020; 10(9):732. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10090732
Chicago/Turabian StyleWetz, Christoph, Julian Rogasch, Philipp Genseke, Imke Schatka, Christian Furth, Michael Kreissl, Henning Jann, Marino Venerito, and Holger Amthauer. 2020. "Asphericity of Somatostatin Receptor Expression in Neuroendocrine Tumors: An Innovative Predictor of Outcome in Everolimus Treatment?" Diagnostics 10, no. 9: 732. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10090732