Tear Film Osmolarity Measurement in Japanese Dry Eye Patients Using a Handheld Osmolarity System


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Profile of Study Subjects
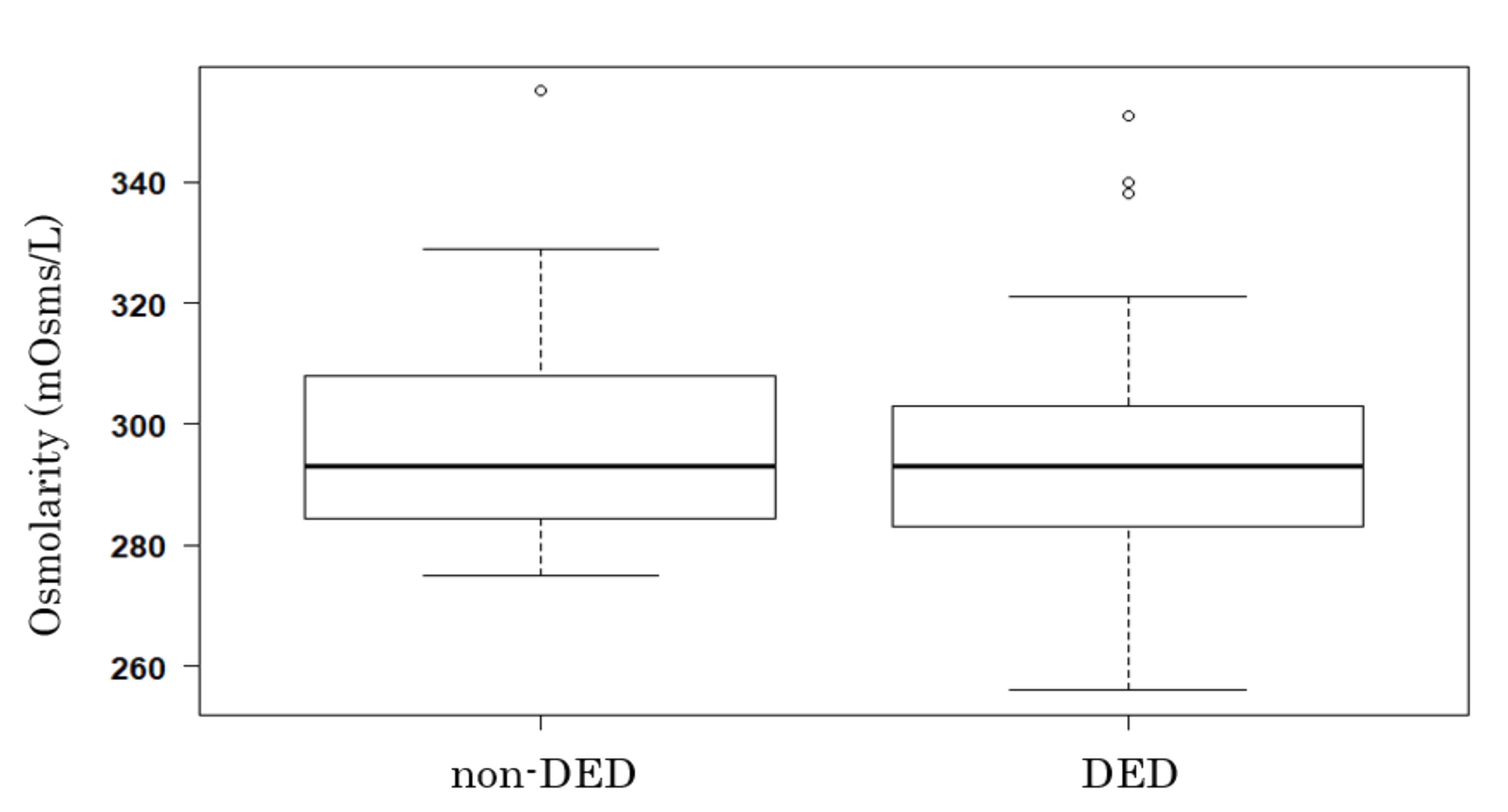
3.2. Tear Film Osmolarity and DED
3.3. Tear Film Osmolarity and Other Parameters
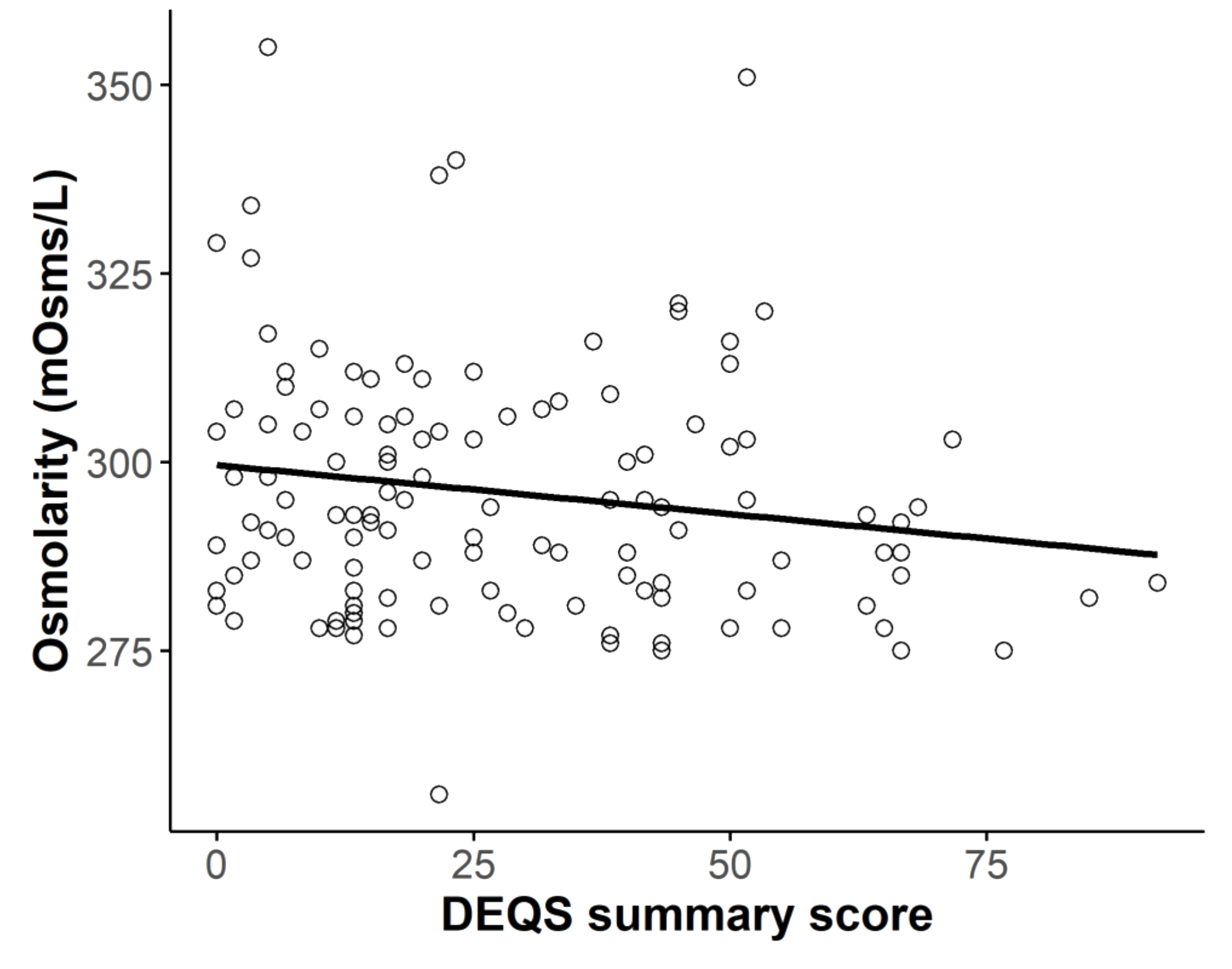
3.3.1. Osmolarity and Subjective Symptoms
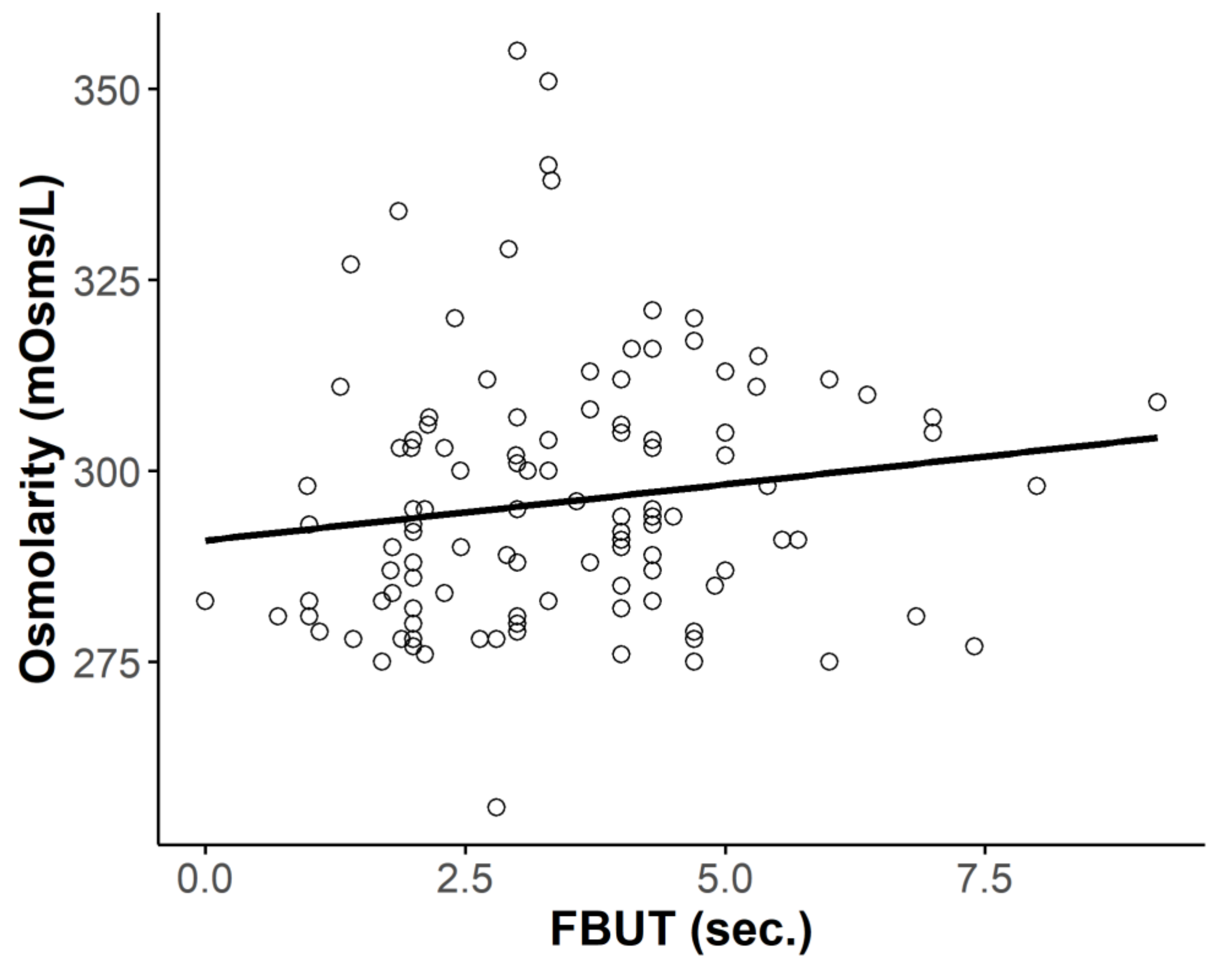
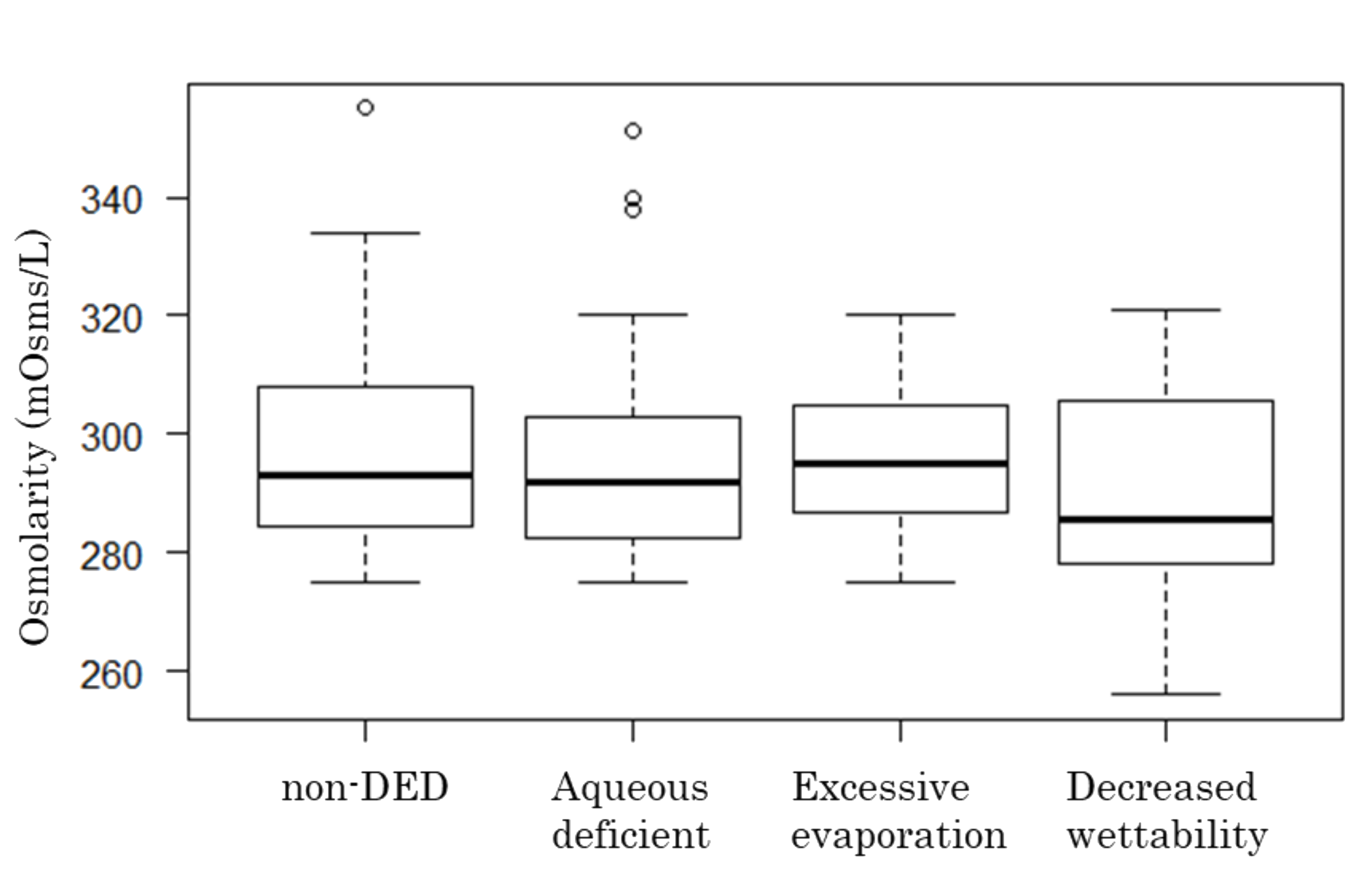
3.3.2. Osmolarity and FBUT or TBUP
3.3.3. Osmolarity and Schirmer Test Score
3.3.4. Osmolarity and Fluorescein Score
3.4. I-PEN Measurement Failures and Patient Discomfort
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- The epidemiology of dry eye disease: Report of the Epidemiology Subcommittee of the International Dry Eye WorkShop. Ocul. Surf. 2007, 5, 93–107. [CrossRef]
- Uchino, M.; Nishiwaki, Y.; Michikawa, T.; Shirakawa, K.; Kuwahara, E.; Yamada, M.; Dogru, M.; Schaumberg, D.A.; Kawakita, T.; Takebayashi, T.; et al. Prevalence and risk factors of dry eye disease in Japan: Koumi study. Ophthalmology 2011, 118, 2361–2367. [Google Scholar] [CrossRef] [PubMed]
- Bron, A.J.; Tiffany, J.M.; Yokoi, N.; Gouveia, S.M. Using osmolarity to diagnose dry eye: A compartmental hypothesis and review of our assumptions. Adv. Exp. Med. Biol. 2002, 506, 1087–1095. [Google Scholar] [PubMed]
- Murube, J. Tear osmolarity. Ocul. Surf. 2006, 4, 62–73. [Google Scholar] [CrossRef]
- Tomlinson, A.; Khanal, S.; Ramaesh, K.; Diaper, C.; McFadyen, A. Tear film osmolarity: Determination of a referent for dry eye diagnosis. Invest Ophthalmol. Vis. Sci. 2006, 47, 4309–4315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, J.P.; Nichols, K.K.; Akpek, E.K.; Caffery, B.; Dua, H.S.; Joo, C.K.; Liu, Z.; Nelson, J.D.; Nichols, J.J.; Tsubota, K.; et al. TFOS DEWS II Definition and Classification Report. Ocul. Surf. 2017, 15, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Li, D.Q.; Chen, Z.; Song, X.J.; Luo, L.; Pflugfelder, S.C. Stimulation of matrix metalloproteinases by hyperosmolarity via a JNK pathway in human corneal epithelial cells. Investig. Ophthalmol. Vis. Sci. 2004, 45, 4302–4311. [Google Scholar] [CrossRef]
- Luo, L.; Li, D.Q.; Corrales, R.M.; Pflugfelder, S.C. Hyperosmolar saline is a proinflammatory stress on the mouse ocular surface. Eye Contact Lens 2005, 31, 186–193. [Google Scholar] [CrossRef]
- Amparo, F.; Jin, Y.; Hamrah, P.; Schaumberg, D.A.; Dana, R. What is the value of incorporating tear osmolarity measurement in assessing patient response to therapy in dry eye disease? Am. J. Ophthalmol. 2014, 157, 69–77.e62. [Google Scholar] [CrossRef] [Green Version]
- Tashbayev, B.; Utheim, T.P.; Utheim, O.A.; Raeder, S.; Jensen, J.L.; Yazdani, M.; Lagali, N.; Vitelli, V.; Dartt, D.A.; Chen, X. Utility of Tear Osmolarity Measurement in Diagnosis of Dry Eye Disease. Sci. Rep. 2020, 10, 5542. [Google Scholar] [CrossRef] [Green Version]
- Sakane, Y.; Yamaguchi, M.; Yokoi, N.; Uchino, M.; Dogru, M.; Oishi, T.; Ohashi, Y.; Ohashi, Y. Development and validation of the Dry Eye-Related Quality-of-Life Score questionnaire. JAMA Ophthalmol. 2013, 131, 1331–1338. [Google Scholar] [CrossRef] [PubMed]
- Van Bijsterveld, O.P. Diagnostic tests in the Sicca syndrome. Arch Ophthalmol. 1969, 82, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Yokoi, N.; Georgiev, G.A.; Kato, H.; Komuro, A.; Sonomura, Y.; Sotozono, C.; Tsubota, K.; Kinoshita, S. Classification of Fluorescein Breakup Patterns: A Novel Method of Differential Diagnosis for Dry Eye. Am. J. Ophthalmol. 2017, 180, 72–85. [Google Scholar] [CrossRef]
- Tsubota, K.; Yokoi, N.; Watanabe, H.; Dogru, M.; Kojima, T.; Yamada, M.; Kinoshita, S.; Kim, H.M.; Tchah, H.W.; Hyon, J.Y.; et al. A New Perspective on Dry Eye Classification: Proposal by the Asia Dry Eye Society. Eye Contact Lens 2020, 46 (Suppl. 1), S2–S13. [Google Scholar] [CrossRef] [PubMed]
- Tsubota, K.; Yokoi, N.; Shimazaki, J.; Watanabe, H.; Dogru, M.; Yamada, M.; Kinoshita, S.; Kim, H.M.; Tchah, H.W.; Hyon, J.Y.; et al. New Perspectives on Dry Eye Definition and Diagnosis: A Consensus Report by the Asia Dry Eye Society. Ocul. Surf. 2016, 15, 65–76. [Google Scholar] [CrossRef]
- Utsunomiya, T.; Kawahara, A.; Hanada, K.; Yoshida, A. Effects of Diquafosol Ophthalmic Solution on Quality of Life in Dry Eye Assessed Using the Dry Eye-Related Quality-of-Life Score Questionnaire: Effectiveness in Patients While Reading and Using Visual Display Terminals. Cornea 2017, 36, 908–914. [Google Scholar] [CrossRef]
- Huang, J.F.; Zhang, Y.; Rittenhouse, K.D.; Pickering, E.H.; McDowell, M.T. Evaluations of tear protein markers in dry eye disease: Repeatability of measurement and correlation with disease. Investig. Ophthalmol. Vis. Sci. 2012, 53, 4556–4564. [Google Scholar] [CrossRef] [Green Version]
- Massingale, M.L.; Li, X.; Vallabhajosyula, M.; Chen, D.; Wei, Y.; Asbell, P.A. Analysis of inflammatory cytokines in the tears of dry eye patients. Cornea 2009, 28, 1023–1027. [Google Scholar] [CrossRef]
- VanDerMeid, K.R.; Su, S.P.; Ward, K.W.; Zhang, J.Z. Correlation of tear inflammatory cytokines and matrix metalloproteinases with four dry eye diagnostic tests. Invest Ophthalmol. Vis. Sci. 2012, 53, 1512–1518. [Google Scholar] [CrossRef]
- Szczesna-Iskander, D.H. Measurement variability of the TearLab Osmolarity System. Cont. Lens Anterior Eye 2016, 39, 353–358. [Google Scholar] [CrossRef]
- Bron, A.J.; Tomlinson, A.; Foulks, G.N.; Pepose, J.S.; Baudouin, C.; Geerling, G.; Nichols, K.K.; Lemp, M.A. Rethinking dry eye disease: A perspective on clinical implications. Ocul. Surf. 2014, 12, S1–S31. [Google Scholar] [CrossRef] [PubMed]
- McMonnies, C.W. An examination of the relationship between ocular surface tear osmolarity compartments and epitheliopathy. Ocul. Surf. 2015, 13, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.C.; Borovik, A.; Hofmann, I.; Gulliver, E.; Rocha, G. Validity and Reliability of a Novel Handheld Osmolarity System for Measurement of a National Institute of Standards Traceable Solution. Cornea 2018, 37, 1169–1174. [Google Scholar] [CrossRef] [PubMed]
- Nolfi, J.; Caffery, B. Randomized comparison of in vivo performance of two point-of-care tear film osmometers. Clin. Ophthalmol. 2017, 11, 945–950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rocha, G.; Gulliver, E.; Borovik, A.; Chan, C.C. Randomized, masked, in vitro comparison of three commercially available tear film osmometers. Clin. Ophthalmol. 2017, 11, 243–248. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Profile of the Subjects | DED 1 (Mean ± SD 2) | Non-DED (Mean ± SD) | Total (Mean ± SD) |
|---|---|---|---|
| Sex (male:female) | 18:53 | 10:41 | 28:94 |
| Age (years) | 45.39 ± 13.88 | 44.82 ± 18.73 | 44.74 ± 16.03 |
| DEQS 3 summary score | 40.45 ± 18.43 | 11.92 ± 12.63 | 28.52 ± 21.49 |
| FBUT 4 (s) | 3.12 ± 1.15 | 3.82 ± 2.04 | 3.41 ± 1.61 |
| FBUT by TBUP 5 subgroup(s) | |||
| Aqueous-deficient | 2.64 ± 0.89 (n = 36) | 2.97 ± 2.1 (n = 22) | 2.77 ± 1.48 (n = 58) |
| Decreased wettability | 2.59 ± 1.17 (n = 8) | 3.37 ± 2.06 (n = 5) | 2.89 ± 1.54 (n = 13) |
| Excessive evaporation | 4.08 ± 0.85 (n = 25) | 4.83 ± 1.50 (n = 23) | 4.44 ± 1.25 (n = 48) |
| Osmolarity by TBUP subgroup (mOsms/L) | 294.76 ± 16.39 | 297.76 ± 16.72 | 296.02 ± 16.52 |
| Aqueous-deficient | 295.89 ± 18.12 (n = 36) | 299.73 ± 16.17 (n = 22) | 297.35 ± 17.36 (n = 58) |
| Decreased wettability | 289.38 ± 21.33 (n = 8) | 292.60 ± 17.27 (n = 5) | 290.62 ± 19.17 (n = 13) |
| Excessive evaporation | 295.76 ± 12.22 (n = 25) | 297.35 ± 17.86 (n = 23) | 296.52 ± 15.04 (n = 48) |
| Schirmer test score (mm/5 min) | 15.04 ± 10.05 | 19.51 ± 12.24 | 16.91 ± 11.19 |
| Parameters | Correlation Coefficient | p-Value |
|---|---|---|
| Fluorescein score | 0.011 | 0.902 |
| FBUT 1 | 0.142 | 0.118 |
| Schirmer’s value | 0.036 | 0.696 |
| DEQS 2 Summary score | −0.168 | 0.064 |
| Adverse Event | Numbers of Adverse Event and Discomfort Level |
|---|---|
| Number of measurements failures | 18 |
| Succeeded on second attempt | 5 |
| Succeeded after multiple attempts | 6 |
| Failed (no data) | 7 |
| Discomfort level | |
| 1: No pain | 78 |
| 2: Slight pain | 55 |
| 3: Moderate pain | 7 |
| 4: Severe pain | 3 |
| 5: Extremely severe pain | 0 |
| No response | 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shimazaki, J.; Sakata, M.; Den, S.; Iwasaki, M.; Toda, I. Tear Film Osmolarity Measurement in Japanese Dry Eye Patients Using a Handheld Osmolarity System. Diagnostics 2020, 10, 789. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10100789
Shimazaki J, Sakata M, Den S, Iwasaki M, Toda I. Tear Film Osmolarity Measurement in Japanese Dry Eye Patients Using a Handheld Osmolarity System. Diagnostics. 2020; 10(10):789. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10100789
Chicago/Turabian StyleShimazaki, Jun, Miki Sakata, Seika Den, Miki Iwasaki, and Ikuko Toda. 2020. "Tear Film Osmolarity Measurement in Japanese Dry Eye Patients Using a Handheld Osmolarity System" Diagnostics 10, no. 10: 789. https://0-doi-org.brum.beds.ac.uk/10.3390/diagnostics10100789